
Abstract
Background
Although coffee consumption is increasing rapidly, the results of previous studies regarding the association between coffee consumption and stroke risk have been conflicting. This was a multi-center cross-sectional study that aimed to evaluate the relationship between coffee consumption and stroke risk in Korean population.
Methods
Data were obtained from the Health Examinees (HEXA) Study, which involved 146,830 individuals aged 40–69 years. Coffee consumption was categorized as none, < 1 cup/day, 1 to < 3 cups/day, and ≥ 3 cups/day. We used logistic regression models to examine the association between coffee consumption and the risk of stroke while controlling for potential confounders and performed subgroup analyses.
Results
After adjusting for age and various possible confounders, high coffee consumption was associated with a 38% lower odds ratio for stroke in women (none vs. ≥ 3 cups/day: OR, 0.62; 95% CI 0.47-0.81; P for trend < 0.0001). No significant association was found in men (none vs. ≥ 3 cups/day: OR, 0.84; 95% CI, 0.66-1.07; P for trend = 0.1515). In analyses stratified by covariates, an inverse association between coffee consumption and stroke risk was most evident among healthy women who were younger, non-obese, non-hypertensive, non-diabetic, non-smokers, and non-alcohol drinkers.
Conclusion
Our results suggest that higher coffee consumption may have protective benefits with regards to stroke risk in middle-aged Korean women.
Similar content being viewed by others


Background
Coffee is one of the most popular beverages consumed worldwide [1]. According to a report issued by the Ministry of Agriculture, Food and Rural Affairs, Korea’s per capita coffee consumption was 3.38 kg in 2011, representing a 17% increase from 2.91 kg in 2008; this rate of increase is greater than that in most other countries [2]. The Korea Health Statistics 2014 report, published by the Ministry of Health and Welfare and the Korea Centers for Disease Control and Prevention, estimates Korean per capita coffee consumption at 11.99 cups/week [3]. As coffee has become more popular, the importance of coffee consumption to public health has received increasing attention.
Caffeine and polyphenol, the rich bioactive compounds in coffee, may play important roles in reducing the risk of stroke through several complex mechanisms, including increased antioxidant activity, insulin sensitivity, hypocholesterolemia, and vascular endothelial function [4, 5]. Several epidemiological studies have suggested that high coffee consumption has protective effects on the risks of Parkinson’s disease, Alzheimer’s disease, cardiovascular disease, and diabetes mellitus [6, 7]. In 2014, cerebrovascular disease was the third leading cause of death in Korea, and the general public became more aware of the dangers of stroke, including its high mortality rate and serious side effects [8].
Data on the association between high coffee consumption and the risk of stroke has been inconsistent [9–11]. A meta-analysis of 11 cohort studies conducted in Japan (n = 2), the U.S (n = 7) and Europe (n = 7) yielded a U-shaped curve, which showed that low and high coffee consumption are both associated with an increased risk of stroke [12]. This distribution may be due to differences in study populations and designs. The type and pattern of coffee intake in Korea may differ considerably from those in other countries. For instance, filtered or brewed coffee is the most popular form of coffee consumed in the U.S and Europe [7],whereas Koreans tend to consume more soluble types of coffees (usually an instant mix containing non-dairy creamer and sugar) rather than brewed coffee [13]. Thus, results from studies done in other countries may not be fully applicable to the Koreans population. In addition, no large population-based study has investigated the association between coffee consumption and risk of stroke in Korea. The aim of this study was to examine the relationship between coffee consumption and the risk of stroke in a large Korean population using data from the Health Examinees (HEXA) baseline Study. The results may be useful in developing daily coffee consumption recommendations for stroke prevention.
Methods
Study population
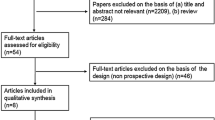
We used data from the HEXA study, a large-scale community-based prospective cohort study involving 173,357 subjects that is part of a larger Korean Genome and Epidemiology Study (KoGES). Only base line information from the HEXA study was used in the present study. Briefly, the study was conducted in Korea from 2004 through 2013 by the K-CDC with the main objective of identifying general characteristics of public health with regard to major chronic diseases. According to standardized study criteria, subjects were recruited from 35 major hospitals and local health examination centers. All of the participants received a detailed description of the study beforehand and voluntarily signed an agreement form. The enrolled subjects included men and women who ranged in age from 40 to 69 years and who participated in a clinical health check-up program. Eligible subjects were required to reply to a structured questionnaire, which was consistently conducted in a consistent manner by trained staff. The questionnaire provided information regarding the general characteristics, medical history, medication usage, family history, lifestyle factors, diet (food frequency questionnaire), and physical activity of each subject. For women, the questionnaire also included a section regarding reproductive factors. Detailed information about the HEXA Study has been reported elsewhere [14].
At baseline, 173,357 subjects were included in the HEXA Study. We excluded individuals who did not respond about stroke diagnosis (n = 667), those with a family history of stroke (n = 23,715), and individuals for whom information on habitual coffee consumption was missing (n = 2,145). After these exclusions, 146,830 individuals (50,439 men and 96,391 women) were included in the final analysis. All participants provided written informed consent at the time they took the baseline HEXA survey. The protocol of the current study was approved by the Institutional Review Board of the Ewha Womans University, in Seoul, Korea (IRB no. 109–2).
Baseline data collection
Trained interviewers conducted the survey using a strictly structured questionnaire [15]. Data on participants’ age, education level, marital status, household income, body mass index (BMI), smoking status, alcohol consumption habits, exercise habits, and history of chronic diseases, including hypertension, diabetes mellitus, and hyperlipidemia, were collected. BMI was categorized according to the guidelines of the Steering Committee of the Regional Office for the Western Pacific Region of the World Health Organization [16]. Obesity was defined as a BMI ≥ 25.0 kg/m2. Diabetes was defined as a fasting blood glucose level ≥ 126 mg/dL or according to diagnosis by a doctor. Hypertension was defined as a systolic blood pressure ≥ 140 mmHg or a diastolic blood pressure ≥ 90 mmHg [17], or according to diagnosis by a doctor. Stroke was evaluated by a questionnaire question that asked participants whether they had ever been diagnosed with a stroke by a doctor. Stroke subtype (e.g., ischemic, hemorrhagic) was not specified in the questionnaire.
Assessment of coffee consumption
Subjects’ coffee consumption was estimated using data from a 106-item semi-quantitative food frequency questionnaire developed for the Korean population. The reliability and validity of this questionnaire were established in a prior Korean population-based study [15]. Participants were asked to indicate how many cups of coffee they drank per day, per week, or per month, and the average volume per drink (1/2 cup, 1 cup, 2 cups), during the last year. The questionnaire did not solicit information on the type of coffee consumed (e.g. instant, drip, or filtered) or caffeine content. Subjects were grouped subjects based on their average coffee consumption as follows: none, < 1 cup a day, 1 to < 3 cups/ day, and ≥ 3 cups a day.
Statistical analysis
All analyses were stratified by sex, and SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA) was used for the main analyses. The cutoff for statistical significance was set at P < 0.05. The chi-squared test was used to compare subjects’ general characteristics according to frequency of coffee consumption. We used regression models to assess the association between coffee consumption and stroke risk. Binary logistic regression was used to calculate the odds ratios (OR) and the associated 95% confidence intervals (CI) for each coffee consumption category, and tests to assess trends were performed. The analyses were adjusted for the following potential confounders, based on the literature [10, 12, 18–20] and participants’ demographic and clinical characteristics: age, education level, alcohol consumption, regular exercise, BMI, smoking, caloric consumption, and diagnosed hypertension, diabetes, and hyperlipidemia (Table 1). In addition, stratified analyses according to alcohol consumption, hypertension, BMI, smoking status, diabetes, and age were performed to further investigate the interactions between coffee consumption and these variables in the association with stroke.
Results
Table 1 describes the participants’ basic demographic characteristics according to sex and daily coffee consumption (none, n = 24,505; < 1 cup/day, n = 33,156; 1 to < 3 cups/day, n = 59,719; ≥ 3 cups/day, n = 29,450). The prevalence of stroke in the study population as a whole was 1.3%, the prevalence for men was 1.54%, and that for women was 1.14% (data not shown). In men and women, several variables (age group, marital status, educational level, household income, BMI, alcohol consumption, smoking status, regular exercise, hypertension, diabetes, and hyperlipidemia) differed significantly according to coffee consumption. Men and women with higher frequencies of coffee consumption tended to be younger and to have more education, higher incomes, and higher BMIs. They were also somewhat more likely to be current smokers and current drinkers and to perform less regular exercise (P for all < 0.0001). Subjects with higher frequencies of coffee consumption tended to have a lower prevalence of hypertension, diabetes mellitus, and hyperlipidemia.
The ORs and 95% CIs for stroke prevalence according to coffee consumption are presented in Table 2. Among men, no significant association was found between coffee consumption and the risk of stroke. However, among women, inverse associations were found between all coffee consumption groups and stroke prevalence. Although further adjustment attenuated this association, the odds ratio for stroke was 38% lower among women who consumed ≥ 3 cups of coffee per day than among non-coffee drinkers (OR, 0.62; 95% CI, 0.47-0.81).
The results of covariate-stratified analyses of the association between stroke prevalence and coffee consumption are presented in Table 3. Among men, no significant association was found between coffee consumption and stratified covariates. Among women, significant associations were found according to the strata of age, BMI, hypertension, diabetes, smoking, and alcohol consumption. The inverse association of coffee consumption with stroke prevalence was most evident among healthy individuals who were younger (OR, 0.56; 95% CI, 0.42 – 0.76), non-obese (OR, 0.53; 95% CI, 0.36 – 0.77), non-hypertensive (OR, 0.52; 95% CI, 0.34 – 0.80), non-smokers (OR, 0.58; 95% CI, 0.43 – 0.77), and non-drinkers (OR, 0.61; 95% CI, 0.44 – 0.84).
Discussion
In the present study, higher coffee consumption was found to be inversely associated with the prevalence of stroke in women. No dose–response relationship was found between coffee consumption and the prevalence of stroke. After adjustment for other risk factors, high coffee consumption was associated with a significantly lower prevalence of stroke in women.
According to the American Heart Association (AHA) and the American Stroke Association (ASA) in 2015, risk factors for stroke include age, heredity, race, sex, transient ischemic attacks (TIAs), high blood pressure, diabetes mellitus, high blood cholesterol, other heart diseases, physical inactivity and obesity, and poor diet [21, 22]. Green tea, oolong tea, and black teas are the most consumed teas in Asia and several Western countries and have been reported to be associated with a lower risk of cardiovascular disease and stroke [23–25]. Coffee contains a complex mixture of bioactive substances, and reported associations of coffee consumption with cardiovascular diseases and diabetes have been inconsistent [12, 26, 27].
A meta-analysis of epidemiological studies showed that coffee consumption (≥4 cups/day) was inversely associated with the risk of stroke [28]. Another meta-analysis [12] found that the association between the two was U-shaped. In cohort studies of women in the US [10] and Sweden [9], moderate consumption of coffee reduced the risk of stroke by approximately 20%. In a cohort study conducted in the Japan, subjects aged ≥ 45 years who consumed coffee (≥4 cups per day) showed a reduced stroke risk compared with non-coffee drinkers. An American cross-sectional study suggested that heavier daily coffee consumption had a beneficial effect on stroke prevalence [29], whereas other studies have shown either no association or an increase in stroke risk according to high or low coffee consumption [30–32]. The variance in these findings may be partly due to differences in the amount of caffeine that was consumed and the different methods of coffee preparation. It is also important to note that these findings must be interpreted relative to the cultural aspects of coffee consumption, which can vary greatly.
The findings from a cohort study of Swedish women and the Nurses’ Health Study are consistent with our results [9, 10]. In addition, the Health Professionals Follow-up Study showed no significant association between coffee consumption and stroke in men. However, a Japanese cohort study found a significant inverse relationship between coffee consumption and stroke risk in men who drank 3 cups of coffee per day [25]. Although the underlying mechanism for the difference in the results between sexes is unknown, Nagata et al. [33] and Ferrini et al. [34] reported that caffeine intake may be beneficially associated beneficially with plasma estrogen, plasma estradiol, and sex hormone-binding globulin levels, as it is inversely related to testosterone level in postmenopausal women. Physical, physiological, hormonal, and lifestyle differences between the sexes may influence the relationship between coffee intake and stroke risk. Surprisingly, the odds ratio for stroke risk was 0.29 (95% CI, 0.11 - 0.74) among diabetic women who consumed ≥ 3 cups of coffee per day as compared to non-coffee drinkers. That is lower than the odds ratio among non-diabetic women (OR, 0,66; 95% CI, 0.49 – 0.88).
The anti-diabetic and anti-stroke effects of coffee may be explained by the bioactive compounds or nutrients contained in coffee. Coffee contains chlorogenic acids, which may contribute to its anti-diabetic effect by reducing cholesterol levels, blood glucose levels, and insulin resistance [35]. In addition, caffeine, a major ingredient in coffee, increases peripheral vascular resistance and blood pressure [36], but a large prospective study revealed an inverse U-shaped association between coffee consumption and the incidence of hypertension [37]. In a meta-analysis of randomized controlled trials, chronic coffee intake was associated beneficially with hypertension, an important main risk factor for stroke [38]. Other phenolic compounds in coffee, including chlorogenic acid, ferulic acid, quinides, and p-coumaric acid, possess high antioxidant abilities, which may help reduce not only endothelial dysfunction [39, 40], but also low-density lipoprotein oxidation [41]. Furthermore, the magnesium, potassium, trigonelline, and niacin in coffee have been associated with enhanced insulin sensitivity, which may prevent the progression of diabetes mellitus [42, 43]. More precise anti-diabetic mechanisms of coffee require further investigation
The present study has several limitations. First, because it was cross-sectional in nature, the cause and effect relationship between coffee consumption and the stroke risk could not be investigated. These results may not reflect long-term coffee consumption patterns, as the study was cross-sectional. To increase the methodological strength of the analyses, adjustments for several known confounding factors, sex stratification, and subgroup analyses were performed. Second, information about stroke types (ischemic, hemorrhage) was not collected, and it is possible that different stroke types may be affected differently by coffee consumption. Third, different types of coffee (caffeinated vs. decaffeinated) and preparation (e.g., filtered, boiled, espresso, and instant), as well as the addition of sugar, milk, and/or powdered creamer, were not considered in the analyses. This heterogeneity may partly explain the differences between studies. Lastly, because the original study did not account for these variables, we could not consider other stroke risk factors deemed important by the AHA and the ASA.
The major strength of this study is its inclusion of a large number of subjects and stroke cases, which provided high statistical power for the analysis of the association between coffee consumption and stroke prevalence. The present study is the first to explore the association between coffee consumption and the prevalence of stroke in a Korean population. Although it was cross-sectional, these results have value as the coffee consumption patterns of Koreans particularly intake level and preparation method – differ from those of other populations. Koreans do not drink decaffeinated coffee, and they often drink instant coffee with sugar and powdered creamer. A previous study suggested that consumption of coffee prepared in this manner is associated with an increased risk of metabolic syndrome risk in Koreans [44]. Although the coffee consumption data in the present study included coffee prepared in this manner, coffee intake was inversely associated with the risk of stroke. Further research is needed to investigate whether this association is attributable to coffee alone. Some evidence suggests that the rate of caffeine metabolism differs between races [45, 46].
Conclusion
Results from this cross-sectional study imply that high coffee consumption, as currently practiced by Koreans, may confer a protective relationship with regards to the development of stroke in this population. This association should be investigated further in validated long-term cohort studies with large numbers of subjects from different ethnic groups.
Abbreviations
- AHA:
-
American heart association
- ASA:
-
American stroke association
- BMI:
-
Body mass index
- HEXA:
-
The health examinees
- K-CDC:
-
Korean centers for disease control and prevention
- TIAs:
-
Transient ischemic attacks
References
Grigg D. The worlds of tea and coffee: Patterns of consumption. GeoJournal. 2002;57:283–94.
Processed food subdivision marketplace report. The ministry of Agriculture, Food and Rural Affairs 2015.
Korea health statistics: Korea national health and nutrition examination survey. Ministry of health and welfare and Korea Centers for Disease Control and Prevention 2014.
Larsson SC. Coffee, tea, and cocoa and risk of stroke. Stroke. 2014;45:309–14.
Butt MS, Sultan MT. Coffee and its consumption: benefits and risks. Crit Rev Food Sci Nutr. 2011;51:363–73.
Higdon JV, Frei B. Coffee and health: a review of recent human research. Crit Rev Food Sci Nutr. 2006;46:101–23.
van Dam RM, Hu FB. Coffee consumption and risk of type 2 diabetes: a systematic review. JAMA. 2005;294:97–104.
Cause of death statistics. Statistics Korea 2014.
Larsson SC, Virtamo J, Wolk A. Coffee consumption and risk of stroke in women. Stroke. 2011;42:908–12.
Lopez-Garcia E, Rodriguez-Artalejo F, Rexrode KM, Logroscino G, Hu FB, van Dam RM. Coffee consumption and risk of stroke in women. Circulation. 2009;119:1116–23.
Shaikh QN, Memon AA, Kamal AK. The impact of green tea and coffee consumption on risk of stroke in Japanese population. J Pak Med Assoc. 2014;64:1094.
Larsson SC, Orsini N. Coffee consumption and risk of stroke: a dose-response meta-analysis of prospective studies. Am J Epidemiol. 2011;74:993–1001.
Je Y, Jeong S, Park T. Coffee consumption patterns in Korean adults: the Korean National Health and Nutrition Examination Survey (2001-2011). Asia Pac J Clin Nutr. 2014;23:691–702.
Health Examinees Study G. The Health Examinees (HEXA) study: rationale, study design and baseline characteristics. Asian Pac J Cancer Prev. 2015;16:1591–7.
Ahn Y, Kwon E, Shim JE, Park MK, Joo Y, Kimm K, Park C, Kim DH. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur J Clin Nutr. 2007;61:1435–41.
World Health Organization: Obesity: preventing and managing the global epidemic. WHO technical report series no 894, Geneva, Switzerland. WHO 2000.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr JL, Jones DW, Materson BJ, Oparil S, Wright Jr JT. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289:2560–71.
O'Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, Rangarajan S, Islam S, Pais P, McQueen MJ, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. 2010;376:112–23.
Lambert M. AHA/ASA guidelines on prevention of recurrent stroke. Am Fam Physician. 2011;83.
Kokubo Y, Iso H, Saito I, Yamagishi K, Yatsuya H, Ishihara J, Inoue M, Tsugane S. The impact of green tea and coffee consumption on the reduced risk of stroke incidence in Japanese population: the Japan public health center-based study cohort. Stroke. 2013;44:1369–74.
risk factors for stroke. American Heart Association, American Stroke Association 2015.
Sacco RL, Benjamin EJ, Broderick JP, Dyken M, Easton JD, Feinberg WM, Goldstein LB, Gorelick PB, Howard G, Kittner SJ, et al. American Heart Association Prevention Conference. IV. Prevention and Rehabilitation of Stroke. Risk factors. Stroke. 1997;28:1507–17.
Arab L, Liu W, Elashoff D. Green and black tea consumption and risk of stroke: a meta-analysis. Stroke. 2009;40:1786–92.
Liang W, Lee AH, Binns CW, Huang R, Hu D, Zhou Q. Tea consumption and ischemic stroke risk: a case-control study in southern China. Stroke. 2009;40:2480–5.
Mineharu Y, Koizumi A, Wada Y, Iso H, Watanabe Y, Date C, Yamamoto A, Kikuchi S, Inaba Y, Toyoshima H, et al. Coffee, green tea, black tea and oolong tea consumption and risk of mortality from cardiovascular disease in Japanese men and women. J Epidemiol Community Health. 2011;65:230–40.
Cornelis MC, El-Sohemy A. Coffee, caffeine, and coronary heart disease. Curr Opin Lipidol. 2007;18:13–9.
Greenberg JA, Boozer CN, Geliebter A. Coffee, diabetes, and weight control. Am J Clin Nutr. 2006;84:682–93.
Kim B, Nam Y, Kim J, Choi H, Won C. Coffee Consumption and Stroke Risk: A Meta-analysis of Epidemiologic Studies. Korean J Fam Med. 2012;33:356–65.
Liebeskind DS, Sanossian N, Fu KA, Wang H-J, Arab L. The coffee paradox in stroke: Increased consumption linked with fewer strokes. Nutr Neurosci. 2016;19:406–13.
Sugiyama K, Kuriyama S, Akhter M, Kakizaki M, Nakaya N, Ohmori-Matsuda K, Shimazu T, Nagai M, Sugawara Y, Hozawa A, et al. Coffee consumption and mortality due to all causes, cardiovascular disease, and cancer in Japanese women. J Nutr. 2010;140:1007–13.
de Koning Gans JM, Uiterwaal CS, van der Schouw YT, Boer JM, Grobbee DE, Verschuren WM, Beulens JW. Tea and coffee consumption and cardiovascular morbidity and mortality. Arterioscler Thromb Vasc Biol. 2010;30:1665–71.
Hakim AA, Ross GW, Curb JD, Rodriguez BL, Burchfiel CM, Sharp DS, Yano K, Abbott RD. Coffee consumption in hypertensive men in older middle-age and the risk of stroke: the Honolulu Heart Program. J Clin Epidemiol. 1998;51:487–94.
Nagata C, Kabuto M, Shimizu H. Association of coffee, green tea, and caffeine intakes with serum concentrations of estradiol and sex hormone-binding globulin in premenopausal Japanese women. Nutr Cancer. 1998;30:21–4.
Ferrini RL, Barrett-Connor E. Caffeine intake and endogenous sex steroid levels in postmenopausal women. The Rancho Bernardo Study. Am J Epidemiol. 1996;144:642–4.
Santos RM, Lima DR. Coffee consumption, obesity and type 2 diabetes: a mini-review. Eur J Nutr. 2016;55:1345–58.
Pincomb GA, Lovallo WR, Passey RB, Whitsett TL, Silverstein SM, Wilson MF. Effects of caffeine on vascular resistance, cardiac output and myocardial contractility in young men. Am J Cardiol. 1985;56:119–22.
Winkelmayer WC, Stampfer MJ, Willett WC, Curhan GC. Habitual caffeine intake and the risk of hypertension in women. JAMA. 2005;294:2330–5.
Noordzij M, Uiterwaal CS, Arends LR, Kok FJ, Grobbee DE, Geleijnse JM. Blood pressure response to chronic intake of coffee and caffeine: a meta-analysis of randomized controlled trials. J Hypertens. 2005;23:921–8.
Lopez-Garcia E, van Dam RM, Qi L, Hu FB. Coffee consumption and markers of inflammation and endothelial dysfunction in healthy and diabetic women. Am J Clin Nutr. 2006;84:888–93.
Gomez-Ruiz JA, Leake DS, Ames JM. In vitro antioxidant activity of coffee compounds and their metabolites. J Agric Food Chem. 2007;55:6962–9.
Natella F, Nardini M, Belelli F, Scaccini C. Coffee drinking induces incorporation of phenolic acids into LDL and increases the resistance of LDL to ex vivo oxidation in humans. Am J Clin Nutr. 2007;86:604–9.
Arnlov J, Vessby B, Riserus U. Coffee consumption and insulin sensitivity. JAMA. 2004;291:1199–201.
Lopez-Ridaura R, Willett WC, Rimm EB, Liu S, Stampfer MJ, Manson JE, Hu FB. Magnesium intake and risk of type 2 diabetes in men and women. Diabetes Care. 2004;27:134–40.
Kim HJ, Cho S, Jacobs Jr DR, Park K. Instant coffee consumption may be associated with higher risk of metabolic syndrome in Korean adults. Diabetes Res Clin Pract. 2014;106:145–53.
Cornelis MC, El-Sohemy A, Kabagambe EK, Campos H. Coffee, CYP1A2 genotype, and risk of myocardial infarction. JAMA. 2006;295:1135–41.
Derby KS, Cuthrell K, Caberto C, Carmella SG, Franke AA, Hecht SS, Murphy SE, Le Marchand L. Nicotine metabolism in three ethnic/racial groups with different risks of lung cancer. Cancer Epidemiol Biomarkers Prev. 2008;17:3526–35.
Acknowledgments
The epidemiologic data used in this study were from the Korean Genome and Epidemiology Study (KoGES) of the Korea Centers for Disease Control & Prevention, Republic of Korea.
Funding
No specific funding was used to support this study.
Availability of data and materials
Data sharing is not applicable to this article as no novel datasets were generated or analyzed during the current study. Please contact the author for data requests.
Authors’ contributions
JL performed the statistical analyses and drafted the manuscript. JEL advised the statistical analyses and helped to draft the manuscript. YK conceived of the study and reviewed, guided, and edited the manuscript. All authors reviewed and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The study was conducted under the guidelines of the Declaration of Helsinki and the study protocol was approved by the Institutional Review Board of Ewha Womans University, Seoul, Korea (IRB no. 109–2). Written informed consent was obtained from all participants.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lee, J., Lee, JE. & Kim, Y. Relationship between coffee consumption and stroke risk in Korean population: the Health Examinees (HEXA) Study. Nutr J 16, 7 (2017). https://doi.org/10.1186/s12937-017-0232-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-017-0232-y