
Abstract
Background
Malaria is a critical public health concern in Ethiopia, with significant socioeconomic consequences. Malaria data trend analysis is essential for understanding transmission patterns and adopting evidence-based malaria control measures. The purpose of this study was to determine the 5 year distribution of malaria in North Shewa zone, Amhara region, Ethiopia, in 2023.
Methods
A descriptive cross-sectional study design was employed to analyse the 5 year trend of malaria surveillance data in the North Shewa zone of the Amhara regional, Ethiopia, spanning from July 2018 to June 2023. The malaria indicator data were gathered from the zone’s public health emergency management database. Malaria data from the previous 5 years was collected, compiled, processed, and analysed using Microsoft Excel 2019.
Results
Among a total of 434,110 suspected cases 47,889 (11.03%) cases were confirmed as malaria, with an average annual malaria incidence rate of 4.4 per 1000 population in the Zone. Malaria cases exhibited an increase from Epidemiological Week (Epi week) 37 to Epi week 49 (September to November) and again from Epi week 22 to week 30 (May to July). Individuals aged 15 and above, and all districts in the Zone except Angolela were notably affected by malaria.
Conclusion
Despite implementing various measures to reduce malaria incidence, the disease continues to persist in the zone. Therefore, the Zone Health Department should intensify its preventive and control efforts.
Similar content being viewed by others

Background
Globally, Malaria prevention and treatment programs have saved over 11 million lives since 2000, and malaria deaths in Africa have been decreased by 36% between 2000 and 2021 [1].
Despite this, malaria remains a major public health and life-threatening parasite illness [2]. In 2021, 3.2 billion people—almost half the world’s population—are at risk, 619,000 people died from malaria [1]. Globally there were an estimated 249million malaria cases in 2022, up from 5 million in 2021 [3]. The African continent is responsible for 95% of all malaria cases and 96% of all malaria deaths [4]. Furthermore, the survey revealed that 80% of all malaria deaths in the African region occurred among the next adult generation (children under the age of five) [5], and that malaria costs Africa nearly $12 billion per year [1].
Malaria cases spread more broadly during normal monsoon years than during drought years, owing to a more favourable environment for mosquito breeding [6, 7]. The unpredictable and seasonal transmission pattern of malaria is influenced by altitude and rainfall. In Ethiopia, the majority of regions have peak malaria transmission from September to December, following the primary wet season (June to August), and the second minor transmission occurs from April to June, following a brief rainy season (February to March) [8, 9]. It is estimated that 75% of Ethiopia’s landmass is malarial, and 68% of its population is at risk of getting the illness. The most severe form of malaria is caused by Plasmodium falciparum, responsible for 60–70% of malaria cases in the country [10].
Ethiopia has embarked on a malaria prevention and control programme with the ambitious goal of eliminating the disease by 2030 [11, 12]. Despite the implementation of various prevention and control strategies, malaria remains a significant public health challenge in the country [13].
Recent findings have indicated the emergence of a newly imported Anopheles species, Anopheles stephensi, along with increasing trends in malaria cases. Factors such as disruptions to malaria services during the COVID-19 pandemic in 2020, and ongoing conflicts in the country have contributed to the region’s malaria burden [14]. Malaria is closely monitored as an epidemic-prone disease through the Public Health Emergency Management (PHEM) surveillance system. Continuous data analysis is crucial for early outbreak detection, tracking trends, and evaluating control programme effectiveness [15]. The North Shewa zone is one of a high malaria endemic area within the region [16, 17]. Therefore, this study aims to assess the 5 year distribution of malaria cases in the zone: from July 2018 to June 2023.
Methods
Study setting, period and design
A descriptive cross-sectional study design was employed to analyse the 5 year trend (from July 2018 to June 2023) of malaria surveillance data in the North Shewa zone, located within the Amhara region. Ethiopia. The zone spans an area of 15,936.13 square kilometres with a population density of 115.3 people per square kilometre [18]. It encompasses all three broad agro-ecological zones: Kolla (hot lowlands below 1000 m altitude), Weyna-Dega (midlands between 1000- and 1500 m altitude), and Dega (cool temperate highlands 1500 m above sea level). Within the North Shewa zone, there are twenty-three districts, eleven hospitals, ninety-two health centres, and more than 380 health posts. The zone includes three general hospitals and one referral hospital, all of which directly report surveillance data to the North Shewa zone’s PHEM) directorate.
Population
The source population for this study comprised individuals seeking healthcare services at facilities within the North Shewa zone between July 2018 and June 2023. The study population specifically included all reported cases of malaria diagnosed within health facilities in the North Shewa zone during the same time frame.
Eligibility criteria
The study included confirmed and clinically treated cases of malaria over a 5 year period, while incomplete data were excluded from the analysis.
Study variable
The dependent variable was number of malaria cases, whereas the independent variable were years, age, pregnancy status, woreda/hospitals, Epi-weeks.
Operational definition
Suspected case: any person with fever or fever with headache, back pain, chills, rigor, sweating, muscle pain, nausea and vomiting were considered as suspected cases for malaria [17].
Confirmed case: suspected case confirmed by rapid diagnostic test (RDT) or microscopy for Plasmodium species [17].
Data collection tools and procedure
First, written permission was obtained from the North Shewa zone’s health department. Subsequently, 5 years of secondary data spanning from July 2018 to June 2023 were acquired from the zone’s health department’s PHEM directorate. Following this, an Excel extraction sheet was prepared, and the required data were retrieved and compiled from the reporting database using pivot tables.
Data quality control, processing and analysis
Descriptive data analysis was done by using Microsoft office excel-2019. Before analysis the data were checked for completeness and consistency. And also, during analysis a team of data analysts to review and validate data at different stages of the analysis process were done. The data were summarized and displayed by using table and different graphs.
Results
Malaria surveillance data analysis by time
Five-year malaria incidence in North Shewa zone
Out of a total of 434,110 probable fever cases examined through rapid diagnostic test (RDT), microscopy, and clinical assessment, 47,889 cases (11.03%) were confirmed as malaria. The proportion of malaria admissions (inpatient malaria cases) rose from 0.015% in 2018 to 0.35% in 2023. Throughout this reporting period, one death was recorded in Epi week 46 of 2020 in the Merhabete district, resulting in a case fatality rate of 0.002% in the zone. On average, 8978 malaria cases were reported annually to the PHEM, with numbers ranging from 6710 in 2019 to 12,790 in 2020. Over the same timeframe, the zone’s average annual malaria incidence rate stood at 4.4 cases per 1000 inhabitants (Table 1).
Trends of malaria species
According to PHEM data from the previous 5 years, from a total 47, 889 confirmed malaria cases, 27010 (56.4%) of confirmed malaria patients had P. falciparum and 43.6% had Plasmodium vivax. Plasmodium falciparum increased dramatically from July 2019 to June 2021, then decreased. Throughout a 5 year period, the trends in P. vivax malaria cases were nearly stable (Fig. 1).

The five years trends of malaria by Plasmodium species in North Shewa zone, Ethiopia, July 2018–June 2023
Trends of malaria by epidemiologic weeks
The systematically gathered and analysed malaria surveillance data confirmed that the trend of malaria cases began to grow from Epi week 37 to 49 (September to November). Then again from Epi week 23 to 29 (May to July) (Fig. 2). A higher/peak of incidence of malaria were observed from July 2020 to June 2021 (Fig. 3).

Trend of five year aggregated total malaria cases with similar WHO weeks of the past five years of North Shewa Zone/July 2018–June 2023

Each year of total malaria cases with WHO Epi-weeks of the past 5 years of North Shewa Zone/July 2018–June 2023
Malaria surveillance data analysis by person
Analysis by age
Among all confirmed cases, 79% were individuals aged 15 years or older, while 16% and 5% were children aged 5–14 and 5 years, respectively. Additionally, as mentioned earlier, one death occurred within the age range of 5 to 15 years (Fig. 4).

Malaria distribution by age in North Shewa zone, Ethiopia, July 2018–June 2023
Analysis by pregnancy status
Over the past 5 years, 224 cases (0.47%) out of the total malaria cases (47,889) were identified as pregnant women. From July 2018 to June 2021, there was a notable increase in the proportion of pregnant women diagnosed with malaria (Fig. 5).

Proportion of pregnant women malaria cases in of North Shewa zone, July 2018–June 2023
Malaria surveillance data analysis by place
Total malaria distributions by districts
The analysis revealed malaria presence in all of the Zone’s woredas except Angolela. Over the past 5 years, three districts accounted for 60% of malaria cases in the zone: Shewarobit with 11,467 cases (23.9%), Mida-Woremo with 10,720 cases (22.4%), and Merhabete with 6,764 cases (14.1%). Conversely, the lowest number of malaria cases were reported from Basona Werna with 24 cases (0.05%), Menz Lalo with 37 cases (0.07%), and Asagrt with 56 cases (0.12%) (Fig. 6). Data from Debre Berhan town, Debre Berhan hospital, and Ataye hospital were unavailable for the Ethiopian fiscal year 2015 (July 2022 to June 2023) due to changes in reporting sites and a conflict situation at Ataye hospital.

Total 5 years malaria distribution by place (districts) of North Shewa zone, July2018–June 2023
Distribution of Plasmodium species by districts
Regarding the distribution of parasite species in relation to woreda of the zone, Mida Woremo, Ensaro and Efratana Gidm woredas were more affected by P. falciparum than P. vivax. On the other hand, P. falciparum and P. vivax were evenly distributed in other woredas of the zone (Fig. 7).

Malaria plasmodium species distribution by Woreda of the North Shewa zone, 2023
Discussion
Malaria is one of the major serious public health and life-threatening parasitic disease caused by Plasmodium species [35]. The peak malaria transmission season in the country is from September to December, following the main rainy season from June/July to early September [19, 20]. The result of this surveillance data analysis is in line with results from Kombolch town, Bahir Dar city, Adama, Mojo, Dembia, Northwest Tigray, Ataye, Jimma, and Harari [8, 9, 20,21,22,23,24,25,26]. The similarity could be explained by, these areas have similar raining season and following this the environment is comfortable for Anopheles mosquito breeding [10, 27].
This surveillance analysis result showed that, from the suspected fever cases 11.03% were malaria cases. Which is comparable with surveillance analysis result of East Shewa zone in Oromia region, 13.4% [28]. It is much lower than study in Guba district in Benshangul Gumuz, (51.04%) [29], Dembia (21.8%) [9], Sibu Sire (20.1%) [30], Harari (46.9%) [25], Abeshge (33.8%) [31] and Bale Zone (17.6%) [32]. This difference could be explained by most of the above are known malaria endemic areas and need further investigation climatic factors and the status of malaria interventions in the region [33] might have greatly contributed. Additionally, this can be explained by the fact that most of the aforementioned studies were conducted in single districts, such as Guba district in Benishangul Gumiz, which is known for its high prevalence of malaria. In contrast, the study site for the current research encompasses a broader area that includes all three agro-ecological zones. However, the results of this study were higher than the confirmed malaria cases reported in other similar retrospective studies conducted in Bahir Dar city (5.0%), Kombolcha town (7.52%), and Mojo town (4.2%) in Ethiopia [20, 26, 34]. The difference may be all Kombolcha, Bahir Dar and Mojo are urban and most of the population living in the area may have a good awareness on preventive practice of malaria than our study area population, most of them are rural.
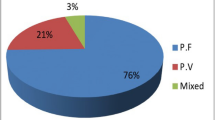
Plasmodium falciparum is responsible for 60–70% of malaria cases in Ethiopia, with P. vivax causing the remainder [10]. A 5 years surveillance analysis in East Shewa zone showed that, from a total of confirmed malaria cases, 61% P. falciparum and 39% were P. vivax [28]. From confirmed malaria cases in Central, North and West Gondar zones; P. falciparum species were 73.4% and P. vivax were 26.6% [36]. In this surveillance analysis, P. falciparum were lower than those reported, that is 56.4% P. falciparum and 43.6% P. vivax. Whereas study in Mojo, Ethiopia, P. vivax was the predominant species accounting for 76.2% [26].
As the surveillance result showed in North Shewa zone within 5 years period > 15 years of age were more affected by malaria. Out of total confirmed and clinical malaria cases obtaining outpatient and inpatient service, 79% were age of 15 years and above, and the remaining 16 and 5% were children of age 5–14 and < 5 years, respectively. This is in line with finding from Gondar which showed that > 15 years of age accounts 71.89% followed by 5–14 years of age [36]. Another study in Adama also showed that 60% of all malaria positive cases were individuals with ≥ 15 years of age, followed by 5–14 age groups (28%), while children below the age of 5 were least affected [21]. This similarity may be explained by, adults are actively engaged in an agricultural activity that might expose them to an Anopheles mosquito bite. In addition, they travel far for schooling which also exposes them to infection [37].
Conclusion and recommendation
According to 5 year PHEM data, the average annual malaria incidence rate in the Zone stood at 4.4 per 1000 population, indicating a high burden that makes achieving a malaria-free nation by 2030 challenging. Plasmodium falciparum malaria emerged as the predominant malaria parasite species in the zone. Malaria transmission typically begins in September and extends through December, and disproportionately affecting individuals aged 15 and above. In light of these findings, it is imperative to intensify malaria prevention and control efforts to reduce the malaria burden. Public Health Emergency Management officials at the Zone, Districts, and health facility levels should prioritize strengthening malaria data documentation and handling across all districts within the zone. This data should be rigorously analysed to promptly identify and respond to outbreaks, particularly during peak transmission seasons.
Limitation of the study
The study uses the secondary data/surveillance data which lacks some important variables, like gender and other sociodemographic variables.
Availability of data and materials
All the data are available from the corresponding author upon reasonable request. All relevant data are within the manuscript.
Abbreviations
- PHEM:
-
Public Health Emergency Management
- RDT:
-
Rapid Diagnostic Test
References
Centers of disease control. CDC Malaria Program. 2023.
WHO. Technical brief for countries preparing malaria funding requests for the global fund (2020–2022). Geneva: World Health Organization; 2020.
WHO. World malaria report 2023. Geneva: World Health Organization; 2023.
Oladipo HJ, Tajudeen YA, Oladunjoye IO, Yusuff SI, Yusuf RO, Oluwaseyi EM, et al. Increasing challenges of malaria control in sub-Saharan Africa: priorities for public health research and policymakers. Ann Med Surg. 2022;81:104366.
Liu Q, Jing W, Kang L, Liu J, Liu M. Trends of the global, regional and national incidence of malaria in 204 countries from 1990 to 2019 and implications for malaria prevention. J Travel Med. 2021;28:046.
Grover-Kopec EK, Blumenthal MB, Ceccato P, Dinku T, Omumbo JA, Connor SJ. Web-based climate information resources for malaria control in Africa. Malar J. 2006;5:38.
Moise IK, Roy SS, Nkengurutse D, Ndikubagenzi J. Seasonal and geographic variation of pediatric malaria in Burundi: 2011 to 2012. Int J Environ Res Public Health. 2016;13:425.
Berhe B, Mardu F, Legese H, Negash H. Seasonal distribution and seven year trend of malaria in North West Tigrai: 2012–2018, Ethiopia; 2019. Trop Dis Travel Med Vaccines. 2019;5:15.
Addisu A, Tegegne Y, Mihiret Y, Setegn A, Zeleke AJ. A 7-year trend of malaria at primary health facilities in Northwest Ethiopia. J Parasitol Res. 2020;2020:32411421.
Federal Ministry of Health. National malaria guidelines. Ethiopia, Addis Ababa, 2018.
WHO. Global technical strategy for malaria 2016–2030. Geneva: World Health Organization; 2015.
Ewnetu Y, Lemma W. Highland malaria transmission dynamics in space and time before pre-elimination era, Northwest Ethiopia. J Epidemiol Glob Health. 2022;12:362–71.
Daba C, Atamo A, Debela SA, Kebede E, Woretaw L, Gebretsadik D, et al. A retrospective study on the burden of malaria in Northeastern Ethiopia from 2015 to 2020: implications for pandemic preparedness. Infect Drug Resist. 2023;16:821–8.
Weiss DJ, Bertozzi-Villa A, Rumisha SF, Amratia P, Arambepola R, Battle KE, et al. Indirect effects of the COVID-19 pandemic on malaria intervention coverage, morbidity, and mortality in Africa: a geospatial modelling analysis. Lancet Infect Dis. 2021;21:59–69.
Federal Ministry of Health. National Malaria Programme Monitoring and Evaluation Plan 2014–2020. Ethiopia, Addis Ababa; 2014.
Abye T, Taye B, Abera T, Hailegiorgis B. Malaria Surveillance system evaluation in Ankober woreda North Shewa, Amhara region, Ethiopia, 2022. Research Square. 2023.
Shiferawu TT, Desta AT. Five-year trend analysis of malaria prevalence in Shewarobit, Amhara regional state, North-central Ethiopia. Pan Afr Med J. 2021;40:237.
North shewa zone (Amhara) [https://dbpedia.org/page/North_Shewa_Zone_(Amhara)]
Nega D, Abera A, Gidey B, Mekasha S, Abebe A, Dillu D, et al. Baseline malaria prevalence at the targeted pre-elimination districts in Ethiopia. BMC Public Health. 2021;21:1996.
Gebretsadik D, Feleke DG, Fiseha M. Eight-year trend analysis of malaria prevalence in Kombolcha, South Wollo, north-central Ethiopia: a retrospective study. Parasit Vectors. 2018;11:55.
Hulluka TF, Chala BC. Five year trend analysis of malaria cases in Adama, Boset and Lume Districts of East Shawa, Oromia, Ethiopia. 2021.
Yenew C, Mulatu S: Trends of Malaria on Hotspot and Ivermectin Mass-drug Administration Zone of Amhara Regional State, 2020. 2020.
Feleke DG, Gebretsadik D, Gebreweld A. Analysis of the trend of malaria prevalence in Ataye, North Shoa, Ethiopia between 2013 and 2017. Malar J. 2018;17:323.
Jemal A, Ketema T. A declining pattern of malaria prevalence in Asendabo Health Center Jimma zone, Southwest Ethiopia. BMC Res Notes. 2019;12:290.
Esayas E, Tufa A, Massebo F, Ahemed A, Ibrahim I, Dillu D, et al. Malaria epidemiology and stratification of incidence in the malaria elimination setting in Harari Region, Eastern Ethiopia. Infect Dis Poverty. 2020;9:160.
Abate A, Assefa M, Golassa L. Five-year trend of malaria prevalence in Mojo town, Central Ethiopia: shifting burden of the disease and its implication for malaria elimination: a retrospective study. Infect Drug Resist. 2022;15:455–64.
Adugna T, Getu E, Yewhalaw D. Species diversity and distribution of Anopheles mosquitoes in Bure district, Northwestern Ethiopia. Heliyon. 2020;6:e05063.
File T, Chala B. Five-year trend analysis of malaria cases in East Shawa Zone, Ethiopia. Ethiop J Health Sci. 2021;31:1215–22.
Alkadir S, Gelana T, Gebresilassie A. A five year trend analysis of malaria prevalence in Guba district, Benishangul-Gumuz regional state, western Ethiopia: a retrospective study. Trop Dis Travel Med Vaccines. 2020;6:18.
Gemechu T, Samuel A, Yewhalaw D. Ten years trend analysis of malaria prevalence and its correlation with climatic variables in Sibu Sire District, east Wollega zone, Oromia regional state, Western Ethiopia: a retrospective study. Sci Technol Arts Res J. 2015;4:99–105.
Yimer F, Animut A, Erko B, Mamo H. Past five-year trend, current prevalence and household knowledge, attitude and practice of malaria in Abeshge, south-central Ethiopia. Malar J. 2015;14:230.
Sani Kalil F, Hasen Bedaso M, Kabeta WS. Trends of malaria morbidity and mortality from 2010 to 2017 in Bale Zone, Ethiopia: analysis of surveillance data. Infect Drug Resist. 2020;13:4379–87.
Weiss DJ, Mappin B, Dalrymple U, Bhatt S, Cameron E, Hay SI, et al. Re-examining environmental correlates of Plasmodium falciparum malaria endemicity: a data-intensive variable selection approach. Malar J. 2015;14:68.
Yimer M, Hailu T, Mulu W, Abera B, Ayalew W. A 5 year trend analysis of malaria prevalence with in the catchment areas of Felegehiwot referral Hospital, Bahir Dar city, northwest-Ethiopia: a retrospective study. BMC Res Notes. 2017;10:239.
White N. Plasmodium knowlesi: the fifth human malaria parasite. Clin Infect Dis. 2008;46:172–3.
Lankir D, Solomon S, Gize A. A five-year trend analysis of malaria surveillance data in selected zones of Amhara region, Northwest Ethiopia. BMC Public Health. 2020;20:1175.
Solomon A, Kahase D, Alemayehu M. Trend of malaria prevalence in Wolkite health center: an implication towards the elimination of malaria in Ethiopia by 2030. Malar J. 2020;19:112.
Acknowledgements
The author’s gratitude goes to North Shewa zone zonal health department, PHEM directorate staffs for their kind cooperation to give the data.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
TM designed the study, performed the statistical analysis, and participated in the writing of the manuscript. GB, ZAG, TL, MS, MM, MS, LD, TNK, and BTT reviewed the manuscript for intellectual content and provided technical guidance in the statistical analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Institutional Review Board (IRB) of Asrat Woldeyes health science Campus, Debre Berhan University (Ref. No IRB 01/154). The North Shewa Zone Health Department provided letters of support and permission for the use of the data for research.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Moltot, T., Bekele, G., Gebreegziabher, Z.A. et al. A five years malaria surveillance data analysis of North Shewa zone, Amhara region, Ethiopia: July 2018 to June 2023. Malar J 23, 187 (2024). https://doi.org/10.1186/s12936-024-05006-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-024-05006-w