
Abstract
Background
Malaria is the most deadly parasitic disease and continues to claim more than a half million of deaths across the world each year, mainly those of under-fives children in sub-Saharan Africa. The aim of this study was to determine the epidemiological, clinical and laboratory features of patients with severe malaria at the Centre Hospitalier Régional Amissa Bongo (CHRAB), a referral hospital in Franceville.
Methods
It was an observational descriptive study conducted at CHRAB over 10 months. All admitted patients at the emergency ward of all ages presenting with positive test to falciparum malaria diagnosed by microscopy and rapid test with clinical signs of severe illness describe by World Health Organization were enrolled.
Results
During this study, 1065 patients were tested positive for malaria, of them 220 had severe malaria. Three quarters (75.0%) were less than 5 years of age. The mean time to consultation was 3.5 ± 1 days. The most frequent signs of severity on admission were dominated by neurological disorders 92.27% (prostration 58.6% and convulsion 24.1%), followed by severe anemia 72.7%, hyperlactatemia 54.6%, jaundice 25% and respiratory distress 21.82%.The other forms such as hypoglycemia, haemoglobinuria, renal failure were found in low proportions < 10%. Twenty-one patients died, coma (aOR = 15.54, CI 5.43–44.41, p < 0.01), hypoglycemia (aOR = 15.37, CI 2.17–65.3, p < 0.01), respiratory distress (aOR = 3.85, CI 1.53–9.73, p = 0.004) and abnormal bleeding (aOR = 16.42, CI 3.57–104.73, p = 0.003) were identified as independent predictors of a fatal outcome. Anemia was associated with decreased mortality.
Conclusion
Severe malaria remains a public health problem affecting mostly children under 5 years. Classification of malaria helps identify the most severely ill patients and aids early and appropriate management of the severe malaria cases.
Similar content being viewed by others


Background
In 2020, malaria remains a devastating health problem and the deadliest parasitic disease for humans. Nearly 241 million cases of malaria occurred worldwide in 2020, most of which were in the WHO African Region. The same year, 627,000 malaria-related deaths were recorded [1]. Children under 5 years old are the most vulnerable group affected by malaria; in 2019, children accounted for 67% of all malaria deaths worldwide. Plasmodium infections result in a spectrum of clinical effects, including asymptomatic parasitemia, uncomplicated malaria, severe malaria, and death [2]. Of the five different species of Plasmodium which can infect humans, Plasmodium falciparum is the most pathogenic species and accounts for the majority of severe and fatal malaria in Africa and particularly in Gabon [3, 4], principally due to endothelial cytoadherence causing sequestration of mature-staged infected red blood cells in vital organs [5, 6]. In endemic areas, young children and pregnant women are the most vulnerable to severe malaria while older children and adults develop partial immunity after repeated infections and thus have lower risk of severe disease [7].
Severe falciparum malaria definition (SFM) has evolved these last two decades. In 1990, the World Health Organization (WHO) established criteria for the diagnosis of severe malaria [8]. In 2000, the WHO revised these criteria to include other clinical manifestations and laboratory values that portend a poor prognosis based on clinical experience in semi‑immune patients. The last update of SFM definition established that SFM is defined by the detection of P. falciparum by microscopy or a rapid diagnostic test and at least one criterion for severe disease (impaired consciousness, respiratory distress, multiple convulsions, prostration, shock, pulmonary oedema, abnormal bleeding, jaundice, severe anemia, hypoglycaemia, acidosis, hyperlactataemia, renal impairment, or hyperparasitaemia) [8].
Malaria transmission in Gabon is stable and perennial [3]. There is limited data describing severe falciparum malaria in Gabon and no study has yet been done in Franceville. Furthermore studies conducted on the topic did not take into account the last updates of SFM definition. This is the first study in Gabon that takes account of the last updates of WHO severe malaria criterions. The new WHO updates of severe malaria can help to better characterize malaria signs and symptoms, help clinicians avoid delays in diagnosis, identify patients who are more likely to die and thus improve their management.
Methods
Study site
This study was conducted at the emergency ward of Centre Hospitalier Régional Amissa Bongo (CHRAB). The CHRAB is located in the town of Franceville and it is the most important public healthcare facility in the Haut-Ogooué province. Franceville is an urban region of south-east Gabon (1° 37′ 15″ S, 13° 34′ 58″ E), the capital city of Haut-Ogooué, it is the third main town of Gabon in terms of population (pop. 110, 568 hab) [4]. Malaria prevalence is around 20% [5].
Study period
The study was carried out from June 2019 to April 2020 (03 June 2019–09 April 2020).
Patients and procedures
All febrile (or those with history of fever in the last 48 h) participants admitted at the emergency ward and pediatric emergency ward of all ages were referred to the study team and seen on admission by a clinical staff of the study. Summary data were recorded on a pro-forma sheet. Only patients presenting with positive falciparum malaria test with clinical signs of severe illness (as described above, according to the WHO criteria [8]) were enrolled. These patients were examined by a physician and their data captured on a standardized form. The study was authorized by the Director of the hospital and approved by the Gabonese National Ethics Committee (PROTN°23/2019/PR/SG/CNER). Only children whose parents gave informed written consent were enrolled in the study. The rainfall dataset for this study was obtained from the Agence pour la sécurité de la navigation aérienne en Afrique et à Madagascar (ASECNA).Venous blood was collected for all enrolled patients for the following medical exam.
Laboratory procedures
Laboratory analysis were performed at the CHRAB’s laboratory and the Centre International de Recherches Médicales de Franceville (CIRMF). Malaria was confirmed by thick blood film under the light microscope. The investigations were performed within 30 min of blood collection at the CHRAB’s laboratory. Thick blood films were stained with 3% Giemsa and parasite load was determined using the Lambarene method [6]. All thick blood were read by two independent qualified microscopists and quality control was done in 10% of slides by a third reader. The Optimal-IT® rapid diagnostic test detecting P. falciparum was also used according to the manufacturers’ instructions [7]. A previous study led in Gabon evaluated this RDT and showed that it is a good tool for malaria diagnosis [9]. Measurement of haemoglobin concentration and white cell count were carried out using an automate ABX Micros® (Horiba, Japan) from EDTA blood samples. Capillary blood glucose was measured with an ACCU-CHEK® Active blood glucose meter (Roche, South Africa). Biochemical analyses were carried out by an ABX PENTRA device (Horiba, Japan) on plasma samples. Macroscopic haemoglobinuria was measured using SD UroColor® Urine Test Strip (SD, South Korea).
Chest radiography
The chest X-ray was performed when clinical examination is suggestive of lung damage at the CHRAB radiography department.
Case definitions
Severe malaria was defined by the detection of P. falciparum by microscopy or a rapid diagnostic test and at least one WHO criterion for severe disease (see above). Fever was defined as axillary temperature ≥ 37.5 °C or reported history of fever in the past 48 h.
Statistical analysis
Data of patients were recorded in Excel 2013 spreadsheets. Statistical analysis was performed using the Epi-Info 6 and R version 4.0.5 (2021-03-31) software. Simple proportion were calculated for qualitative variables and quantitative variables by mean, standard deviation (SD), median with inter-quartile range (IQR). The qualitative variables were compared using the Chi-square test or Fisher’s exact test for numbers below 5. Binary logistic regression model was used to compute the adjusted odds ratios (aOR) of independent risk factors. The confidence interval was set at 95% (95% CI). Statistical significance was set at α = 5%.
Results
Demographic and clinical data of patients included
From June 2019 to March 2020, a total of 5642 patients were admitted to the CHRAB emergency department. One thousand sixty-five (1065) of them were tested positive for malaria and the 4575 other patients were admitted for another pathology. Of 1065 patients with malaria, 847 (79.4%) had simple or moderate malaria and 220 (20.6%) had severe malaria (Fig. 1).

Flowchart of the screening of severe malaria cases in the CHRAB’s emergency ward. *According to the WHO criterions
Demographic data and individual factor for patients are represented in Table 1. Patients included in this study ranged in age from 3 to 1128 months (94 years) with a sex ratio (M/F) of 1.09. Three quarters (165/220, 75.0%) of the patients were less than 5 years of age.
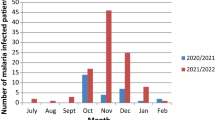
Seasonal distribution of severe malaria case
The monthly distribution of severe malaria cases was analyzed in relation to rainfall (Fig. 2). The prevalence of severe malaria cases differs by month (p = 0.007). The majority of severe malaria cases were observed during the months of September 2019 to November 2019 (short rainy season). Mars 2020 had the lowest proportion of severe malaria cases.

Distribution of the severe malaria cases according to the pluviometry
Self-medication and patient consultation
The most commonly used antimalarial drug for self-medication was artemisinin-based combination therapy 171/220 (77.7%) as show in Table 2.
Patient consultation time and death
No patient with severe malaria went to the hospital at the start of symptoms. The mean time to consultation was 3.5 ± 1 days (extremes 1–7 days). Patients with severe malaria usually had a delay in consultation of more than 48 h (53.64%). Time to consultation from symptoms onset was not associated with death (p = 0.13). A total of 21 (9.54%) patients died during study. Sixteen (76.19%) patients died less than 24 h after their hospitalization (Table 3).
Clinical and biological description of severe malaria
All severe clinical forms of severe P. falciparum malaria are shown in Table 4. The neurological disorders accounted for 92.27% of cases (prostration (58.6%; n = 129), repeated convulsions (24.1%; n = 53) and coma (9.5%; n = 21)). Pulmonary oedema, macroscopic haemoglobinuria and abnormal bleeding were rarely observed. The laboratory features observed in the patients were dominated by severe anaemia (72.7%; 160/220), hyperlactataemia (54.6; 59/108) and hyperparasitaemia (5.45%; 12/220). The other laboratory features observed in the patients included hyperbilirubinaemia (9.3%; 8/86), rarely hypoglycaemia and hypercreatinaemia. Of 220 patients, 21 died, giving an overall case fatality rate of 9.5%. The full clinical and laboratory features are shown in Table 4.
Individual characteristics data of patients in relation to death
Table 5 presents the social characteristics of the patients in relation to death. The number of deaths related to severe malaria differed according to age group (p = 0.019). The highest number of deaths was observed in the age group of 0–5 years.
Association of severe malaria cases with death
Table 6 shows a multiple logistic regression model identifying coma (aOR = 15.54, CI 5.43–44.41, p < 0.01), hypoglycaemia (aOR = 15.37, CI 0.96–0.99, p < 0.01), respiratory distress (aOR = 3.85, CI 1.53–9.73, p = 0.004) and abnormal bleeding (aOR = 16.42, CI 3.57–104.73, p = 0.003) as independent predictors of a fatal outcome.
Discussion
Malaria is one of the world’s leading parasitic diseases and affects a considerably large number of people especially children under 5 years old. This study was designed to describe the epidemiology, clinical and laboratory presentations of severe falciparum malaria according to the last WHO updates [2] in patients at the emergency ward of the CHRAB hospital, in order to improve the diagnosis, classification and appropriate management of malaria.
Malaria prevalence was 18.9%, this prevalence has remained stable in Franceville since 2011 [5, 10, 11]. Of the 1065 patients with malaria, 220 cases of severe malaria were admitted for hospitalization corresponding to 20.6% of overall malaria cases. A similar finding has been noted in Gabon (Libreville) and Cameroon [12, 13]. Other studies in West Africa [14, 15] showed lower values than those of this study (4.4% and 6.4%, respectively). This difference could be explained by the difference in epidemiological pattern. Indeed the central African countries have a hyperendemic or holendemic facies while West African countries have a seasonal pattern. Higher incidences have also been reported in other studies done in Cameroon and Central Africa Republic [16–18]. Despite the fact that these studies were carried out in central Africa, the study settings differed, as well as methodologies and sample sizes, which could explain the variations in the incidences.
In this study, the most represented age group was 0–5 years i.e. three quarters (75.0%) of population. This finding is in accordance with other studies, which states that children less than 5 years are most vulnerable to malaria [12, 19, 20, 21, 22]. Most of the participants (77.7%) used self-medication. This findings can result in delayed treatment of uncomplicated P. falciparum malaria with further progression to severe malaria. In this study the mean time between the onset of the disease and admission was 3.5 ± 1 days (extremes 1–7 days). Indeed, several studies in other African settings have reported an increased risk of severe malaria with delay [23–25] in presentation.
The frequency of severe falciparum malaria cases was associated with pluviometry, with most cases seen in the months of September to November (rainy season in Gabon). This result is in accordance with another study performed by Maghendji-Nzondo et al. [5]. This observation was also noted in Cameroon by Chiabi et al. [17]. This result could be explained by the fact that vector of the malaria parasite in man, is a mosquito species (Anopheles gambiae species complex.) which develops during the rainy season. Rains create a moist climate, resulting in a rapid parasitic cycle in the mosquito, thus increasing malaria transmission during this period.
The recent definition of severe malaria requires additional investigations that are difficult to carry out sub-Saharan countries, especially in an emergency situation. In this context, the study was unable to diagnose metabolic acidosis. This difficulty is reported by Camara et al. [15] in Senegal, by Ndoyo et al. [26] in Central Africa Republic, and by Sanou et al. [27] in Ouagadougou [27].
The most frequent clinical feature of severe malaria on admission was neurological disorders, particularly prostration and convulsion, followed by severe anaemia, hyperlactataemia and respiratory distress. Similar results were also observed by other authors [13, 19, 21, 28, 29, 30]. Hypoglycaemia, haemoglobinuria and renal failure were less common in this study. Other studies led in Senegal, Central Africa and Burkina-Faso have confirmed their rarity [15, 26, 27].
The independent prognostic factors associated with mortality in this study were coma, respiratory distress, hypoglycaemia and abnormal bleeding. These observations are entirely consistent with other studies [31]. The severity of impaired consciousness was measured using the Blantyre or Glasgow coma scale. Several studies have shown that impaired consciousness and seizures are associated with a higher risk of mortality in malaria patients, especially in children [19, 32]. The results of this study showed that respiratory distress was associated with mortality. In childhood malaria, respiratory distress is largely attributed to metabolic acidosis [33], unfortunately in the present study measure the metabolic acidosis could not be realized. A previous study revealed that the incidence of pulmonary dysfunction is 3% to 10% in patients with P. falciparum infections, and the mortality rate is approximately 70% [34] that confirming findings obtained in the present study. Many studies have also demonstrated hypoglycaemia as an important risk factor for death [15, 19, 35] and the present study have made the similar observation. Imbert and Camara, noted the very poor prognosis of hypoglycaemia because its clinical expression can be masked by possible neurological disorders and it aggravates the latter [15, 36]. Hypoglycaemia is often undervalued by clinicians that could explain the rarity of cases [15].
This study highlight only 5 cases of abnormal bleeding but this feature was associated with mortality. It is also rare in other studies. Severe anaemia was the second most frequent clinical feature of severe malaria in this study but was associated with decreased mortality. A similar observation in other studies showed a better outcome in children with severe anaemia [19, 30]. This result could be explain by the fact that the patients with severe anaemia were rapidly transfused and thus correcting their anaemia.
Conclusion
At the CHRAB hospital, severe malaria is one of the main cause of hospitalization and its related mortality is high The most common clinical features of severe malaria in this study were neurological disorders, severe anaemia and respiratory distress and coma, respiratory distress, hypoglycaemia and abnormal bleeding were independent prognostic factors associated with mortality in this study.
Availability of data and materials
Not applicable.
Abbreviations
- ACT:
-
Artemisinin-based combination therapy
- ASECNA:
-
Agence pour la sécurité de la navigation aérienne en Afrique et à Madagascar
- CANTAM:
-
Central Africa network on tuberculosis, HIV/AIDS and malaria
- CIRMF:
-
Centre International de Recherches Médicales de Franceville
- CHRAB:
-
Centre Hospitalier Régional Amissa Bongo
- EDCTP:
-
European and Developing Countries Clinical Trials Partnership
- RDT:
-
Rapid diagnostic test
- WHO:
-
World Health Organization
References
WHO. World Malaria report 2021. Geneva: World Health Organization; 2021.
WHO. Guidelines for the treatment of malaria. 3rd ed. Geneva: World Health Organization; 2015.
Elissa N, Migot-Nabias F, Luty A, Renaut A, Toure F, Vaillant M, et al. Relationship between entomological inoculation rate, Plasmodium falciparum prevalence rate, and incidence of malaria attack in rural Gabon. Acta Trop. 2003;85:355–61.
Direction générale de la statistique. Résultats globaux du recensement général de la population et des logements de 2013 du Gabon (RGPL-2013). Libreville, Gabon, 2015: p. 11, Table 19.
Maghendji-Nzondo S, Nzoughe H, Lemamy GJ, Kouna LC, Pegha-Moukandja I, Lekoulou F, et al. Prevalence of malaria, prevention measures, and main clinical features in febrile children admitted to the Franceville Regional Hospital. Gabon Parasite. 2016;23:32.
Planche T, Krishna S, Kombila M, Engel K, Faucher JF, Ngou-Milama E, et al. Comparison of methods for the rapid laboratory assessment of children with malaria. Am J Trop Med Hyg. 2001;65:599–602.
Moody AH, Chiodini PL. Non-microscopic method for malaria diagnosis using OptiMAL IT, a second-generation dipstick for malaria pLDH antigen detection. Br J Biomed Sci. 2002;59:228–31.
WHO. Management of severe malaria. A practical handbook. 3rd ed. Geneva: World Health Organization; 2012.
Mawili-Mboumba DP, Bouyou Akotet MK, Ngoungou EB, Kombila M. Evaluation of rapid diagnostic tests for malaria case management in Gabon. Diagn Microbiol Infect Dis. 2010;66:162–8.
Lekana-Douki JB, Pontarollo J, Zatra R, Toure-Ndouo FS. Paludisme au Gabon: résultats d’une étude bioclinique à l’hôpital de l’amitié sino-gabonaise de Franceville. Cahier Sante. 2011;21:193–8.
Maghendji-Nzondo S, Kouna LC, Mourembou G, Boundenga L, Imboumy-Limoukou RK, Matsiegui PB, et al. Malaria in urban, semi-urban and rural areas of southern of Gabon: comparison of the Pfmdr 1 and Pfcrt genotypes from symptomatic children. Malar J. 2016;15:420.
Koko J, Dufillot D, Zima-Ebeyard A, Duong T, Gahouma D, Kombila M. Aspects cliniques et approche épidémiologique du paludisme de l’enfant à Libreville. Gabon Med Afr Noire. 1999;46:10–4.
Chiabi A, Takou V, Tchokoteu P-F, Ngo S, Essoh L. Initial treatment of severe malaria in children is inadequate–a study from a referral hospital in Cameroon. S Afr J Child Health. 2009;3:9–11.
Giha H, Elghazali G, A-Elgadir T, A-Elbasit I, Eltahir E, Baraka O, et al. Clinical pattern of severe Plasmodium falciparum malaria in Sudan in an area characterized by seasonal and unstable malaria transmission. Trans R Soc Trop Med Hyg. 2005;99:243–51.
Camara B, Diagne N, Faye P, Fall M, Ndiaye J, Ba M, et al. Critères de gravité et facteurs pronostiques du paludisme chez l’enfant à Dakar. Med Mal Infect. 2011;41:63–7.
Tchokoteu P, Bitchong-Ekono C, Tietche F, Tapko J, Ekobo AS, Douala-Mouteng V, et al. Les formes graves du paludisme de l’enfant dans un service de pédiatrie générale à Yaoundé, Cameroun. Bull Soc Pathol Exot. 1999;92:153–6.
Chiabi A, Djimafo ANM, Nguefack S, Mah E, Dongmo FN, Angwafo IF. Severe malaria in Cameroon: pattern of disease in children at the Yaounde Gynaeco-Obstetric and Pediatric hospital. J Infect Public Health. 2020;13:1469–72.
Serengbe GB, Ndoyo J, Gaudeuille A, Longo J, Bezzo M, Ouilibona S, et al. Les aspects actuels du paludisme grave de l’enfant en milieu hospitalier pédiatrique centrafricain. Med Mal Infect. 2004;34:86–91.
Dzeing-Ella A, Nze Obiang PC, Tchoua R, Planche T, Mboza B, Mbounja M, et al. Severe falciparum malaria in Gabonese children: clinical and laboratory features. Malar J. 2005;4:1.
Bouyou-Akotet MK, Mawili-Mboumba DP, Kendjo E, Eyang Ekouma A, Abdou Raouf O, Engohang Allogho E, et al. Complicated malaria and other severe febrile illness in a pediatric ward in Libreville. Gabon BMC Infect Dis. 2012;12:216.
Edelu BO, Ndu IK, Igbokwe OO, Iloh ON. Severe falciparum malaria in children in Enugu, South East Nigeria. Niger J Clin Pract. 2018;21:1349–55.
Chiabi A, Tchokoteu PF, Toupouri A, Mbeng TB, Wefuan J. The clinical spectrum of severe malaria in children in the east provincial hospital of Bertoua, Cameroon. Bull Soc Pathol Exot. 2004;97:239–43.
Mousa A, Al-Taiar A, Anstey NM, Badaut C, Barber BE, Bassat Q, et al. The impact of delayed treatment of uncomplicated P. falciparum malaria on progression to severe malaria: a systematic review and a pooled multicentre individual-patient meta-analysis. PLoS Med. 2020;17:e1003359.
Ossou-Nguiet P, Okoko A, Oko A, Mabiala-Babela J, Moyen G. Determinants of cerebral malaria in Congolese children (in French). Rev Neurol (Paris). 2013;169:510–4.
Mpimbaza A, Ndeezi G, Katahoire A, Rosenthal PJ, Karamagi C. Demographic, socioeconomic, and geographic factors leading to severe malaria and delayed care seeking in Ugandan children: a case–control study. Am J Trop Med Hyg. 2017;97:1513–23.
Ndoyo J, Gaudeuille A, Longo J, Bezzo M, Ouilibona S, Ayivi B. An update on severe pediatric malaria in Central Africa hospital units. Med Mal Infect. 2004;34:86–91.
Sanou I, Pare J, Traoré S, Modiano D, Kam K, Kaboré J, et al. Formes cliniques du paludisme grave en milieu hospitalier pédiatrique a Ouagadougou. Cah Sante. 1997;7:13–7.
Geleta G, Ketema T. Severe malaria associated with Plasmodium falciparum and P. vivax among children in Pawe Hospital, Northwest Ethiopia. Malar Res Treat. 2016;2016:1240962.
Garba B, Muhammad A, Edem B, Adeniji A, Aghadueki S, Kolawole T, et al. Prevalence and pattern of severe malaria seen in children at a specialist hospital in Gusau, Nigeria. Int J Biomed Res. 2014;5:351–4.
Mockenhaupt FP, Ehrhardt S, Burkhardt J, Bosomtwe SY, Laryea S, Anemana SD, et al. Manifestation and outcome of severe malaria in children in northern Ghana. Am J Trop Med Hyg. 2004;71:167–72.
Sypniewska P, Duda JF, Locatelli I, Althaus CR, Althaus F, Genton B. Clinical and laboratory predictors of death in African children with features of severe malaria: a systematic review and meta-analysis. BMC Med. 2017;15:147.
Kremsner PG, Valim C, Missinou MA, Olola C, Krishna S, Issifou S, et al. Prognostic value of circulating pigmented cells in African children with malaria. J Infect Dis. 2009;199:142–50.
English M, Murphy S, Mwangi I, Crawley J, Peshu N, Marsh K. Interobserver variation in respiratory signs of severe malaria. Arch Dis Child. 1995;72:334–6.
Boulos M, Costa JM, Tosta CE. Comprometimento pulmonar na malária (revisão). Rev Instit MedTrop São Paulo. 1993;35:93–102.
Kendjo E, Agbenyega T, Bojang K, Newton CR, Bouyou-Akotet M, Pedross F, et al. Mortality patterns and site heterogeneity of severe malaria in African children. PLoS ONE. 2013;8:e58686.
Imbert P, Gérardin P, Rogier C, Jouvencel P, Brousse V, Guyon P, et al. Pertinence des critères OMS 2000 de paludisme grave chez l’enfant non immun à Dakar, Sénégal. Bull Soc Pathol Exot. 2003;96:156–60.
Acknowledgements
The authors would like to acknowledge all the participants in this study. We also acknowledge the CHRAB’s staff and the CIRMF’s staff especially Alain Prince Okouga.
Funding
This study was funded by CIRMF. CIRMF is member of the Central Africa Clinical Research Network, CANTAM funded by EDCTP and the European Union.
Author information
Authors and Affiliations
Contributions
RKIL and JBLD: conception and design of the study; AFNA and JBLW: collected biological samples and data and carried out clinical and biological examinations; EBN, JCBBE and FM acquisition, analysis and interpretation of data; RKIL and JCBBE: drafting the article; RKIL, LSOL and JBLD: revising it critically for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Gabonese National Ethics Committee (PROTN 23/2019/PR/SG/CNER).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Imboumy-Limoukou, R.K., Lendongo-Wombo, J.B., Nguimbyangue-Apangome, A.F. et al. Severe malaria in Gabon: epidemiological, clinical and laboratory features in Amissa Bongo Hospital of Franceville. Malar J 22, 88 (2023). https://doi.org/10.1186/s12936-023-04512-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-023-04512-7