
Abstract
Background
Point-of-care diagnosis of malaria is currently based on microscopy and rapid diagnostic tests. However, both techniques have their constraints, including poor sensitivity for low parasitaemias. Hence, more accurate diagnostic tests for field use and routine clinical settings are warranted. The miniature direct-on-blood PCR nucleic acid lateral flow immunoassay (mini-dbPCR-NALFIA) is an innovative, easy-to-use molecular assay for diagnosis of malaria in resource-limited settings. Unlike traditional molecular methods, mini-dbPCR-NALFIA does not require DNA extraction and makes use of a handheld, portable thermal cycler that can run on a solar-charged power pack. Result read-out is done using a rapid lateral flow strip enabling differentiation of Plasmodium falciparum and non-falciparum malaria infections. A laboratory evaluation was performed to assess the performance of the mini-dbPCR-NALFIA for diagnosis of pan-Plasmodium and P. falciparum infections in whole blood.
Methods
Diagnostic accuracy of the mini-dbPCR-NALFIA was determined by testing a set of Plasmodium-positive blood samples from returned travellers (n = 29), and Plasmodium-negative blood samples from travellers with suspected malaria (n = 23), the Dutch Blood Bank (n = 19) and intensive care patients at the Amsterdam University Medical Centers (n = 16). Alethia Malaria (LAMP) with microscopy for species differentiation were used as reference. Limit of detection for P. falciparum was determined by 23 measurements of a dilution series of a P. falciparum culture. A fixed sample set was tested three times by the same operator to evaluate the repeatability, and once by five different operators to assess the reproducibility.
Results
Overall sensitivity and specificity of the mini-dbPCR-NALFIA were 96.6% (95% CI, 82.2%–99.9%) and 98.3% (95% CI, 90.8%–100%). Limit of detection for P. falciparum was 10 parasites per microlitre of blood. The repeatability of the assay was 93.7% (95% CI, 89.5%–97.8%) and reproducibility was 84.6% (95% CI, 79.5%–89.6%).
Conclusions
Mini-dbPCR-NALFIA is a sensitive, specific and robust method for molecular diagnosis of Plasmodium infections in whole blood and differentiation of P. falciparum. Incorporation of a miniature thermal cycler makes the assay well-adapted to resource-limited settings. A phase-3 field trial is currently being conducted to evaluate the potential implementation of this tool in different malaria transmission areas.
Similar content being viewed by others


Background
Correct and timely diagnosis of malaria is key in the management and control of this disease. Traditionally, microscopy of Giemsa-stained thick and thin blood film has been the standard diagnostic technique applied in endemic settings. Although it is able to differentiate the causative Plasmodium species, its sensitivity for low parasite densities is limited and adequate slide reading requires extensive training and experience [1,2,3,4]. The development of rapid diagnostic tests (RDTs) has brought a fast and easy-to-use alternative for malaria diagnosis. Since their introduction, RDTs have proven to be an essential tool for malaria control in remote endemic regions [5]. However, they usually do not detect < 100 parasites per microliter of blood, which makes them of limited use in near-elimination areas where such low parasite counts are often prevalent [6,7,8]. False-negative RDT results can also arise for P. falciparum strains with a genetic deletion for the antigen targeted by RDTs, histidine-rich protein 2 (HRP2). Over the past decade, this genotype has become widespread in South America, and increasing prevalence has now been reported for African and Asian countries as well [9,10,11,12]. Conversely, residual parasite antigen in the blood after treatment and complete parasite clearance is frequently observed and may result in false-positive RDT diagnosis [13, 14].
The limitations of microscopy and RDTs can be overcome by the use of nucleic acid amplification techniques (NAATs) [15]. Examples are endpoint polymerase chain reaction (PCR) and real-time quantitative PCR (qPCR), techniques that are commonly applied for malaria diagnosis and research in high-resource settings [16,17,18,19]. However, the requirement of well-trained laboratory personnel as well as expensive PCR machines that rely on a stable power source, restrict the use of NAATs in malaria-endemic countries. An alternative to PCR is loop-mediated isothermal amplification (LAMP), a simplified molecular assay with an easy readout that makes use of isothermal DNA amplification [20]. Nevertheless, current LAMP formats are generally unsuited for multiplex amplification, hampering Plasmodium species differentiation [21].
Consequently, there is still a need for a highly sensitive, user-friendly and field-deployable diagnostic test for malaria that can discriminate Plasmodium species. An innovative assay has recently been developed to meet these requirements: the miniature direct-on-blood PCR nucleic acid lateral flow immunoassay (mini-dbPCR-NALFIA, Fig. 1). This platform combines three techniques to overcome the issues encountered when attempting to implement traditional PCR methods in limited-resource settings. First of all, the direct-on-blood PCR (dbPCR) uses a specialized reagent mix that eliminates the need of DNA extraction prior to amplification [22, 23]. Instead, the PCR can be performed directly on a template of EDTA-anticoagulated whole blood. The dbPCR also has a duplex format which can detect all (pan) Plasmodium species infecting humans and differentiate P. falciparum infections. The second innovative element is the use of a miniature thermal cycler to run the dbPCR, called miniPCR (miniPCR bio, Massachusetts, USA). It is a hand-held, portable device that can be programmed with a smartphone or laptop application, either through USB cable or Bluetooth connection. The latest model, mini16, has an affordable price of approximately 800 USD (compared to 3000–5000 USD for a conventional PCR thermal cycler) and can process 16 samples per run. The mini16 can run on mains power, but also on a portable and solar-chargeable power pack, making the system completely autonomous and suitable for rural or emergency settings with unstable or no electricity supply. Finally, the result of the dbPCR is easily and rapidly read out with NALFIA, an immunochromatographic flow strip that can detect labelled PCR amplicons [22,23,24,25]. A NALFIA strip is placed in a mixture of dbPCR product and running buffer, after which the dbPCR amplicons will flow over the strip. Neutravidin-labelled carbon particles on the NALFIA strip will bind to the labelled dbPCR amplicons, and this complex is visualized within 10 min when it is captured by the two amplicon-specific antibody lines on the NALFIA strip.

Workflow of the mini-dbPCR-NALFIA
Earlier prototypes of the dbPCR-NALFIA assay have shown promising results in field evaluations, with sensitivity and specificity results up to 97.2% and 95.5%, respectively, using light microscopy as reference standard, and a detection limit for P. falciparum infections of 1 parasite per microlitre (p/μL) of blood [22, 23]. In these studies, the dbPCR was still run on a conventional thermal cycler. By optimizing the dbPCR protocol, the mini-dbPCR-NALFIA can now be run on a miniPCR device, making the method better adapted to field settings with limited resources. This article describes the laboratory evaluation of the optimized mini-dbPCR-NALFIA as a multiplex assay for the detection of pan-Plasmodium and P. falciparum infections in blood.
Methods
Direct-on-blood PCR reagent mix
The dbPCR is a duplex reaction targeting two regions in the Plasmodium 18S rRNA gene: one that is highly conserved in the genus Plasmodium (the pan-Plasmodium target), and a second that is specific for P. falciparum [26, 27]. By using 5’-labelled primer pairs (Eurogentec, Liège, Belgium) previously described in literature, both target amplicons will carry a biotin label and a target-specific label (Table 1) [23]. The dbPCR reagent mix consists of 10 μL of 2× Phusion Blood PCR buffer (Thermo Fisher Scientific, Waltham, MA, USA), 0.1 μL of Phire Hot Start II DNA polymerase (Thermo Fisher Scientific), labelled primers and sterile water to make a total volume of 22.5 μL per sample.
Direct-on-blood PCR on miniature thermal cycler
The template format for the dbPCR is 2.5 μL of EDTA-anticoagulated blood. Every mini-dbPCR-NALFIA run includes controls, which are a P. falciparum-infected EDTA blood sample and a Plasmodium-negative EDTA blood sample. As a first step, the samples were lysed at 98 °C for 10 min on the mini16 thermal cycler (miniPCR bio, Massachusetts, USA), a miniature endpoint PCR device (dimensions: 5 × 13 × 10 cm, weight: 0.5 kg) which can also be used for heat block protocols. The miniPCR smartphone application was used to programme the lysis protocol on the mini16 device through Bluetooth connection. After the lysis of the EDTA blood templates, 22.5 μL of the dbPCR reagent mix was added to each (total reaction volume 25 μL). The dbPCR was also run on the mini16 thermal cycler. Its protocol consisted of an initial activation step of 1 min at 98 °C, followed by 10 cycles of 5 s at 98 °C, 15 s at 61 °C and 30 s at 72 °C; next, 28 cycles of 5 s at 98 °C, 15 s at 58 °C and 30 s at 72 °C; and a final extension step of 72 °C for 2 min.
Read-out with NALFIA
Read-out of the results was done with NALFIA (Abingdon Health, York, UK). The test strip consists of a sample absorption pad, a conjugate pad with neutravidin-labelled carbon binding to the amplicons’ biotin label, and a nitrocellulose membrane coated with anti-digoxigenin (Dig) and anti-fluorescein isothiocyanate (FITC) antibody lines detecting and visualizing the amplicon-carbon complex. A third line on the membrane functions as a flow control (Fig. 2). After completion of the dbPCR run on the mini16, a NALFIA strip was placed in a tube with 10 μL of dbPCR product and 140 μL running buffer. After a 10 min incubation, the NALFIA results were read out. When the first line directed against the Dig-labelled pan-Plasmodium amplicon was positive, it indicated the presence of Plasmodium infection. If the second anti-FITC test line for the fluorescein amidite (FAM)-labelled P. falciparum amplicon was also positive, the sample was infected specifically with P. falciparum (or a mixed infection including P. falciparum). A sample with a positive pan-Plasmodium line and an absent P. falciparum line was classified positive for a non-falciparum malaria species, i.e. Plasmodium vivax, Plasmodium malariae, Plasmodium ovale or Plasmodium knowlesi. When only the P. falciparum line was visible, this result was interpreted to be positive for this species. A NALFIA test was considered invalid when the flow control line was absent.

Possible NALFIA results after dbPCR for pan-Plasmodium and P. falciparum. The strip has 3 potential lines that can appear: a pan-Plasmodium test line (1), a P. falciparum test line (2) and a flow control line (FC). A Positive pan-Plasmodium and P. falciparum test lines, thus a P. falciparum infection or a mixed infection including P. falciparum; B Pan-Plasmodium positive test line, but negative for the P. falciparum test line. This is a Plasmodium infection with a non-falciparum species (e.g. P. vivax); C Pan-Plasmodium negative, but a positive P. falciparum line. This result is also considered positive for P. falciparum; D The NALFIA has a flow control line but the pan-Plasmodium and P. falciparum test lines are absent. This is a Plasmodium-negative test result; E Pan-Plasmodium and P. falciparum negative, but also negative for the flow control line. This NALFIA test is invalid
Laboratory evaluation
Limit of detection
The limit of detection (LoD) for the pan-Plasmodium and P. falciparum targets was determined by testing 23 aliquots of a tenfold dilution series of a FCR3 ring-stage P. falciparum culture. The parasite density of the culture was determined by light microscopy. Dilutions were made in Plasmodium-negative EDTA blood from the Dutch blood bank. Tested parasite densities ranged from 1000 to 0.1 p/μL. LoD was defined as the lowest parasite density that was detected with 90% confidence (≥ 21 of 23 runs).
Sensitivity and specificity
To determine the laboratory sensitivity and specificity of the mini-dbPCR-NALFIA, a set of 87 blood specimen was tested, including samples from returned Dutch travellers with suspected malaria infection, Dutch blood donors, and intensive care unit patients from the Academic Medical Centre (Amsterdam, the Netherlands). All samples were derived from a pre-established Biobank at the Laboratory for Experimental Parasitology at the Academic Medical Centre. Both blood donors and intensive care unit patients did not travel to malaria-endemic areas in the 6 months before blood collection. The malaria status of all samples had been determined previously using the Alethia Malaria assay (Meridian Bioscience, Cincinnati, USA), a highly sensitive LAMP-based method for diagnosing malaria in non-endemic settings with a detection limit of 2 p/µL for P. falciparum and 0.1 p/µL for P. vivax [28, 29]. For samples with a positive Alethia result (n = 29, all returned travellers), the infecting Plasmodium species had been determined with expert microscopy. This set included 23 P. falciparum, 3 P. vivax, 2 P. ovale and 1 P. malariae infections. The P. falciparum samples had been quantified microscopically and ranged from 106 to 102 p/μL; the parasite counts of the non-falciparum malaria samples had not been determined at the time of microscopic examination. The 58 Plasmodium-negative samples comprised 19 samples from the Dutch blood donors, 16 samples from intensive care unit patients and 23 samples from malaria-suspected returned travellers with a negative Alethia diagnosis. The operator that tested all samples with mini-dbPCR-NALFIA was blinded to the reference test outcomes.
Accordance and concordance
Accordance and concordance are measures to express, respectively, the repeatability (intra-operator variability) and reproducibility (inter-operator variability) of qualitative tests [30, 31]. To evaluate the accordance and concordance of the mini-dbPCR-NALFIA, a single individual prepared 8 aliquots of a dilution series of FCR3 ring-stage P. falciparum culture and five Plasmodium-negative blood samples. For the accordance assessment, one operator tested three sets of aliquots with mini-dbPCR-NALFIA on three consecutive days, using the same equipment and dbPCR reagent batch numbers. To determine the concordance of the mini-dbPCR-NALFIA, five different operators from the same laboratory each tested a set of sample aliquots once. All five operators were blinded to the nature of the samples and used the same equipment and dbPCR reagent batch numbers.
Statistical analysis
Sensitivity and specificity were calculated for the pan-Plasmodium target, the P. falciparum target and the overall assay. The Clopper-Pearson Exact method was used to calculate the 95% confidence interval (CI) of the sensitivity and specificity. Accordance and concordance were calculated in random framework, using the formulae proposed by Van der Voet and Van Raamsdonk (2004): \({ACC}_{random}=\frac{1}{L}{\sum }_{i}({{p}_{0,i}}^{2}+{{p}_{1,i}}^{2}+{{p}_{2,i}}^{2}{+{p}_{3,i}}^{2})\), where L represents the number of tested samples, p0 the proportion of negative results, p1 the proportion of pan-Plasmodium single positive results (i.e. only the pan line), p2 the proportion of P. falciparum single positive results (i.e. only the P. falciparum line) and p3 the proportion of double positive results (i.e. both pan and P. falciparum lines), for a particular sample i. For the random concordance, the following formula was used: \({CON}_{random}={{P}_{0,i}}^{2}+{{P}_{1,i}}^{2}+{{P}_{2,i}}^{2}+{{P}_{3,i}}^{2}\), where \({P}_{0,i}=\frac{1}{L}{\sum }_{i}^{L}{p}_{0,i}\),\({P}_{1,i}=\frac{1}{L}{\sum }_{i}^{L}{p}_{1,i}\), \({P}_{2,i}=\frac{1}{L}{\sum }_{i}^{L}{p}_{2,i}\) and\({P}_{3,i}=\frac{1}{L}{\sum }_{i}^{L}{p}_{3,i}\). Here, L represents the number of different operators, and p0,i, p1,i, p2,i and p3,i represent the proportion of negative, pan single positive, P. falciparum single positive and double positive results for a particular operator i [31]. The 95% CI of the accordance and concordance estimates was calculated by means of bootstrapping [30, 32].
Results
Limit of detection
The results of the P. falciparum culture dilution series testing are displayed in Table 2. At a confidence level of 90%, LoD was determined to be 100 p/µL for the pan-Plasmodium test line and 10 p/µL for the P. falciparum line.
Sensitivity and specificity
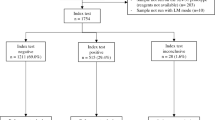
Of the 29 Plasmodium samples, 28 tested positive for the pan-Plasmodium line in the mini-dbPCR-NALFIA, while 1 P. vivax sample was false-negative for this line. All 23 P. falciparum samples also showed the P. falciparum test line. 57 Plasmodium-negative blood samples were negative for both test lines with mini-dbPCR-NALFIA; 1 sample from a Dutch blood donor was false-positive for the P. falciparum line. None of the test samples had an invalid NALFIA result.
This resulted in a sensitivity of 96.6% (95% CI, 82.2%–99.9%) and a specificity of 100% (95% CI, 93.8%–100%) for the pan-Plasmodium line. The sensitivity of the P. falciparum test line was calculated to be 100% (95% CI, 85.2%–100%), and its specificity 98.4% (95% CI, 91.6%–100%). When the results of the two NALFIA test lines were combined, there were three possible outcomes: a non-falciparum infection, a P. falciparum infection and Plasmodium-negative. This approach resulted in an overall sensitivity of 96.6% (95% CI, 82.2%–99.9%) and specificity of 98.3% (95% CI, 90.8%–100%) of the mini-dbPCR-NALFIA.
Accordance and concordance
An overview of the accordance test results for the mini-dbPCR-NALFIA is shown in Table 3. The overall accordance of all tested samples in a random framework was 93.7% (95% CI, 89.5%–97.8%).
Table 4 summarizes the test results for the five different operators of the mini-dbPCR-NALFIA. Based on these data, the random concordance was calculated to be 84.6% (95% CI, 79.5%–89.6%).
Discussion
This study demonstrates that the mini-dbPCR-NALFIA is a robust, highly sensitive and specific tool for molecular diagnosis of malaria. It has a simpler workflow than traditional NAATs and requires much less resources. By incorporating the mini16 as portable, battery-powered thermal cycler, the mini-dbPCR-NALFIA can be used even in remote healthcare settings without an extensive laboratory infrastructure or stable power supply.
With an excellent overall sensitivity of 96.6% and specificity of 98.3%, the diagnostic accuracy of the mini-dbPCR-NALFIA is similar to that of traditional molecular techniques for malaria diagnosis, such as conventional PCR, qPCR and nested PCR [15]. One P. vivax sample gave a false-negative result. This may have been due to a low parasite density, which is common in P. vivax infections [33]. Unfortunately, whether this was indeed the case for this sample was unknown, as its parasitaemia had not been determined with microscopy at the time of diagnosis. Also, this particular sample had been in − 20 °C storage for 2 years, which may have affected the DNA integrity. The occasional false-positive result in one Plasmodium-negative sample could have been the result of carry-over contamination from a Plasmodium-positive sample during the preparation of the dbPCR or NALFIA.
The LoDs of 100 p/μL for the pan-Plasmodium line and 10 p/μL for the P. falciparum line demonstrate the high sensitivity of the mini-dbPCR-NALFIA for low falciparum parasite densities. Although the LoD of extremely sensitive nested and qPCR techniques can go as low as 0.1 p/μL [34,35,36,37], most importantly, the mini-dbPCR-NALFIA is still significantly more sensitive for low falciparum parasitaemias than light microscopy and RDTs, which generally fail to detect infections below 50 to 200 p/µL [38]. As such, the assay will be able to diagnose the majority of symptomatic malaria patients in an endemic setting, who often present with a parasitaemia above 1000 p/μL [39,40,41]. On top of that, mini-dbPCR-NALFIA could potentially be used for screening and detection of asymptomatic falciparum cases with sub-microscopic infections [7, 42]. As no quantified non-falciparum samples were available for this study, additional evaluation of the LoD of the mini-dbPCR-NALFIA for these other Plasmodium species is warranted.
When analysing a P. falciparum blood dilution series and five malaria-negative blood samples, the mini-PCR-NALFIA showed a high accordance of 93.7%, demonstrating the robustness of the method. Discordant results were mainly observed for parasite densities < 10 p/μL, which are close to the LoD of the test. At such low Plasmodium DNA concentrations, stochastic variations tend to have a more prominent influence on the assay’s outcome. This phenomenon was also believed to be the main reason for the concordance being 84.6%. The laboratory experience of the different operators in the concordance evaluation ranged from basic to proficient. They were only given written and oral instructions, which was sufficient for them to correctly perform the mini-dbPCR-NALFIA. This observation underlined its simplicity and user-friendliness.
Compared to other molecular methods for malaria diagnosis, mini-dbPCR-NALFIA shares some characteristics with LAMP, which also has a simplified protocol with easy read-out and high accuracy for diagnosing malaria, including low density falciparum infections [43, 44]. However, LAMP currently has no multiplex capability and, therefore, cannot differentiate Plasmodium species in one reaction. This issue is not encountered with mini-dbPCR-NALFIA, a duplex assay that can distinguish falciparum malaria from infections with other Plasmodium species. To further evaluate the performance of the mini-dbPCR-NALFIA for diagnosis of (submicroscopic) infections with P. vivax, P. malariae and P. ovale., additional research is required, since this study tested only a limited number of non-falciparum malaria blood samples.
The adaptation of the assay described by Roth et al. [23] to operate on a portable, battery-powered mini16 thermal cycler has made it possible to run the dbPCR in harsh, resource-limited conditions of sub-Saharan Africa. Implementation in such settings is also supported by the stability of the dbPCR reagents, which did not show loss of performance after storage at 4 °C for 9 months [23]. Another strength of the mini-dbPCR-NALFIA is its affordability: the testing costs per sample are economical (0.30 USD for the dbPCR reagents, 2.80 USD per NALFIA test) and introduction of the mini16 greatly reduces the cost of the required equipment (800 USD per device). A planned economic evaluation will assess the cost-effectiveness of the mini-dbPCR-NALFIA in different endemic areas, compared to currently implemented malaria point-of-care diagnostics.
A limitation of the current mini-dbPCR-NALFIA is its inability to differentiate between the non-falciparum malaria species and identify mixed infections. Although the vast majority of malaria cases in Africa is caused by P. falciparum, the relative contribution of P. vivax, P. malariae and P. ovale infections in this region appears to be increasing [45,46,47,48]. Fortunately, the mini-dbPCR-NALFIA has a flexible design: an alternative format is currently under development, which will have a P. falciparum and a P. vivax test line. In the same way, the mini-dbPCR-NALFIA also has the potential to be modified to detect other blood-borne pathogens.
In areas with high malaria transmission, the mini-dbPCR-NALFIA could be a valuable alternative to RDTs, which are likely to suffer from false-positive results due to P. falciparum HRP2 antigen persistence in the blood after clearance of the parasites [13, 14, 49, 50]. Nevertheless, it is possible that a similar issue may arise for molecular diagnostic techniques: there have been a number of studies showing that PCR-based detection of Plasmodium DNA in blood can remain positive up to seven weeks after curative malaria treatment [51, 52]. This could either be caused by residual circulating DNA fragments or by a small subset of parasites with extended survival. Although this phenomenon could have its implications for the specificity of the mini-dbPCR-NALFIA, its relevance for the application of the assay as a field diagnostic remains a subject of further study.
Conclusion
The mini-dbPCR-NALFIA is an easy-to-use method for sensitive and specific diagnosis of malaria. Compared to other simplified molecular diagnostics, it has the advantages that there is no need of prior sample processing and that differentiation of P. falciparum and non-falciparum infections is possible thanks to its duplex format. A handheld miniature thermal cycler makes the assay well-adapted to resource-poor conditions in malaria endemic regions. The high diagnostic accuracy and low LoD of the mini-dbPCR-NALFIA could make it a valuable tool in many malaria control programmes, especially for detection of asymptomatic and low-density cases in near-elimination areas. A phase-3 field trial is currently being conducted to evaluate the potential of the mini-dbPCR-NALFIA in different epidemiological settings.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ACC:
-
Accordance
- CI:
-
Confidence interval
- CON:
-
Concordance
- dbPCR:
-
Direct-on-blood PCR
- Dig:
-
Digoxigenin
- DNA:
-
Deoxyribonucleic acid
- EDTA:
-
Ethylenediaminetetraacetic acid
- FAM:
-
Fluorescein amidite
- FITC:
-
Fluorescein isothiocyanate
- HRP2:
-
Histidine-rich protein 2
- LAMP:
-
Loop-mediated isothermal amplification
- LoD:
-
Limit of detection
- NAAT:
-
Nucleic acid amplification technique
- NALFIA:
-
Nucleic acid lateral flow immunoassay
- p/μL:
-
Parasites per microlitre
- PCR:
-
Polymerase chain reaction
- qPCR:
-
Real-time quantitative PCR
- RDT:
-
Rapid diagnostic test
- rRNA:
-
Ribosomal ribonucleic acid
- USD:
-
United States dollars
References
Ngasala B, Bushukatale S. Evaluation of malaria microscopy diagnostic performance at private health facilities in Tanzania. Malar J. 2019;18:375.
Ouedraogo AL, Bousema T, Schneider P, de Vlas SJ, Ilboudo-Sanogo E, Cuzin-Ouattara N, et al. Substantial contribution of submicroscopical Plasmodium falciparum gametocyte carriage to the infectious reservoir in an area of seasonal transmission. PLoS ONE. 2009;4: e8410.
Payne D. Use and limitations of light-microscopy for diagnosing malaria at the primary health-care level. Bull World Health Organ. 1988;66:621–6.
WHO. Malaria microscopy quality assurance manual. 2nd Edn. Geneva: World Health Organization; 2016.
Aidoo M, Incardona S. Ten years of universal testing: how the rapid diagnostic test became a game changer for malaria case management and improved disease reporting. Am J Trop Med and Hyg. 2022;106:29–32.
Okell LC, Ghani AC, Lyons E, Drakeley CJ. Submicroscopic infection in Plasmodium falciparum-endemic populations: a systematic review and meta-analysis. J Infect Dis. 2009;200:1509–17.
Bousema T, Okell L, Felger I, Drakeley C. Asymptomatic malaria infections: detectability, transmissibility and public health relevance. Nat Rev Microbiol. 2014;12:833–40.
Wu L, van den Hoogen LL, Slater H, Walker PG, Ghani AC, Drakeley CJ, et al. Comparison of diagnostics for the detection of asymptomatic Plasmodium falciparum infections to inform control and elimination strategies. Nature. 2015;528:S86-93.
Kojom LP, Singh V. Prevalence of Plasmodium falciparum field isolates with deletions in histidine-rich protein 2 and 3 genes in context with sub-Saharan Africa and India: a systematic review and meta-analysis. Malar J. 2020;19:46.
Gamboa D, Ho MF, Bendezu J, Torres K, Chiodini PL, Barnwell JW, et al. A large proportion of P. falciparum isolates in the Amazon region of Peru lack pfhrp2 and pfhrp3: implications for malaria rapid diagnostic tests. PLoS One. 2010;5:e8091.
Jejaw Zeleke A, Hailu A, Bayih AG, Kefale M, Amare AT, Tegegne Y, et al. Plasmodium falciparum histidine-rich protein 2 and 3 genes deletion in global settings (2010–2021): a systematic review and meta-analysis. Malar J. 2022;21:26.
Rogier E, McCaffery JN, Nace D, Svigel SS, Assefa A, Hwang J, et al. Plasmodium falciparum pfhrp2 and pfhrp3 gene deletions from persons with symptomatic malaria infection in Ethiopia, Kenya, Madagascar, and Rwanda. Emerg Infect Dis. 2022;28:608–16.
Kattenberg JH, Tahita CM, Versteeg IA, Tinto H, Traore-Coulibaly M, Schallig HD, et al. Antigen persistence of rapid diagnostic tests in pregnant women in Nanoro, Burkina Faso, and the implications for the diagnosis of malaria in pregnancy. Trop Med Int Health. 2012;17:550–7.
Kiemde F, Bonko MDA, Tahita MC, Lompo P, Rouamba T, Tinto H, et al. Accuracy of a Plasmodium falciparum specific histidine-rich protein 2 rapid diagnostic test in the context of the presence of non-malaria fevers, prior anti-malarial use and seasonal malaria transmission. Malar J. 2017;16:294.
Roth JM, Korevaar DA, Leeflang MM, Mens PF. Molecular malaria diagnostics: a systematic review and meta-analysis. Crit Rev Clin Lab Sci. 2016;53:87–105.
Snounou G, Viriyakosol S, Zhu XP, Jarra W, Pinheiro L, Rosario VE, et al. High sensitivity of detection of human malaria parasites by the use of nested polymerase chain reaction. Mol Biochem Parasitol. 1993;61:315–20.
Rougemont M, Van Saanen M, Sahli R, Hinrikson HP, Bille J, Jaton K. Detection of four Plasmodium species in blood from humans by 18S rRNA gene subunit-based and species-specific real-time PCR assays. J Clin Microbiol. 2004;42:5636–43.
Shokoples SE, Ndao M, Kowalewska-Grochowska K, Yanow SK. Multiplexed real-time PCR assay for discrimination of Plasmodium species with improved sensitivity for mixed infections. J Clin Microbiol. 2009;47:975–80.
Calderaro A, Montecchini S, Buttrini M, Piccolo G, Rossi S, Arcangeletti MC, et al. Malaria diagnosis in non-endemic settings: the European experience in the last 22 years. Microorganisms. 2021;9:2265.
Selvarajah D, Naing C, Htet NH, Mak JW. Loop-mediated isothermal amplification (LAMP) test for diagnosis of uncomplicated malaria in endemic areas: a meta-analysis of diagnostic test accuracy. Malar J. 2020;19:211.
Morris U, Aydin-Schmidt B. Performance and application of commercially available loop-mediated isothermal amplification (LAMP) kits in malaria endemic and non-endemic settings. Diagnostics. 2021;11:8.
Mens PF, de Bes HM, Sondo P, Laochan N, Keereecharoen L, van Amerongen A, et al. Direct blood PCR in combination with nucleic acid lateral flow immunoassay for detection of Plasmodium species in settings where malaria is endemic. J Clin Microbiol. 2012;50:3520–5.
Roth JM, de Bes L, Sawa P, Omweri G, Osoti V, Oberheitmann B, et al. Plasmodium detection and differentiation by direct-on-blood PCR nucleic acid lateral flow immunoassay: development, validation, and evaluation. J Mol Diagn. 2018;20:78–86.
Mens PF, van Amerongen A, Sawa P, Kager PA, Schallig HD. Molecular diagnosis of malaria in the field: development of a novel 1-step nucleic acid lateral flow immunoassay for the detection of all 4 human Plasmodium spp. and its evaluation in Mbita, Kenya. Diagn Microbiol Infect Dis. 2008;61:421–7.
Mens PF, Moers AP, de Bes LM, Flint J, Sak JR, Keereecharoen L, et al. Development, validation and evaluation of a rapid PCR-nucleic acid lateral flow immuno-assay for the detection of Plasmodium and the differentiation between Plasmodium falciparum and Plasmodium vivax. Malar J. 2012;11:279.
Schoone GJ, Oskam L, Kroon NC, Schallig HD, Omar SA. Detection and quantification of Plasmodium falciparum in blood samples using quantitative nucleic acid sequence-based amplification. J Clin Microbiol. 2000;38:4072–5.
Hermsen CC, Telgt DS, Linders EH, van de Locht LA, Eling WM, Mensink EJ, et al. Detection of Plasmodium falciparum malaria parasites in vivo by real-time quantitative PCR. Mol Biochem Parasitol. 2001;118:247–51.
De Koninck AS, Cnops L, Hofmans M, Jacobs J, Van den Bossche D, Philippe J. Diagnostic performance of the loop-mediated isothermal amplification (LAMP) based Illumigene® malaria assay in a non-endemic region. Malar J. 2017;16:418.
Rypien C, Chow B, Chan WW, Church DL, Pillai DR. Detection of Plasmodium infection by the Illumigene malaria assay compared to reference microscopy and real-time PCR. J Clin Microbiol. 2017;55:3037–45.
Langton SD, Chevennement R, Nagelkerke N, Lombard B. Analysing collaborative trials for qualitative microbiological methods: accordance and concordance. Int J Food Microbiol. 2002;79:175–81.
van der Voet H, van Raamsdonk LW. Estimation of accordance and concordance in inter-laboratory trials of analytical methods with qualitative results. Int J Food Microbiol. 2004;95:231–4.
Davison AC, Hinkley DV. Bootstrap methods and their application. Cambridge: Cambridge University Press; 1997.
Howes RE, Battle KE, Mendis KN, Smith DL, Cibulskis RE, Baird JK, et al. Global epidemiology of Plasmodium vivax. Am J Trop Med Hyg. 2016;95(6 Suppl):15–34.
Lau YL, Lai MY, Anthony CN, Chang PY, Palaeya V, Fong MY, et al. Comparison of three molecular methods for the detection and speciation of five human Plasmodium species. Am J Trop Med Hyg. 2015;92:28–33.
Komaki-Yasuda K, Vincent JP, Nakatsu M, Kato Y, Ohmagari N, Kano S. A novel PCR-based system for the detection of four species of human malaria parasites and Plasmodium knowlesi. PLoS ONE. 2018;13: e0191886.
Nuin NA, Tan AF, Lew YL, Piera KA, William T, Rajahram GS, et al. Comparative evaluation of two commercial real-time PCR kits (QuantiFast™ and abTES™) for the detection of Plasmodium knowlesi and other Plasmodium species in Sabah. Malaysia Malar J. 2020;19:306.
Haanshuus CG, Mohn SC, Mørch K, Langeland N, Blomberg B, Hanevik K. A novel, single-amplification PCR targeting mitochondrial genome highly sensitive and specific in diagnosing malaria among returned travellers in Bergen. Norway Malar J. 2013;12:26.
Mbanefo A, Kumar N. Evaluation of malaria diagnostic methods as a key for successful control and elimination programs. Trop Med Infect Dis. 2020;5:102.
Mmbando BP, Lusingu JP, Vestergaard LS, Lemnge MM, Theander TG, Scheike TH. Parasite threshold associated with clinical malaria in areas of different transmission intensities in north eastern Tanzania. BMC Med Res Methodol. 2009;9:75.
Goncalves BP, Huang CY, Morrison R, Holte S, Kabyemela E, Prevots DR, et al. Parasite burden and severity of malaria in Tanzanian children. N Engl J Med. 2014;370:1799–808.
Afrane YA, Zhou G, Githeko AK, Yan G. Clinical malaria case definition and malaria attributable fraction in the highlands of western Kenya. Malar J. 2014;13:405.
Prusty D, Gupta N, Upadhyay A, Dar A, Naik B, Kumar N, et al. Asymptomatic malaria infection prevailing risks for human health and malaria elimination. Infect Genet Evol. 2021;93: 104987.
Picot S, Cucherat M, Bienvenu AL. Systematic review and meta-analysis of diagnostic accuracy of loop-mediated isothermal amplification (LAMP) methods compared with microscopy, polymerase chain reaction and rapid diagnostic tests for malaria diagnosis. Int J Infect Dis. 2020;98:408–19.
Mohon AN, Getie S, Jahan N, Alam MS, Pillai DR. Ultrasensitive loop mediated isothermal amplification (US-LAMP) to detect malaria for elimination. Malar J. 2019;18:350.
Baltzell KA, Shakely D, Hsiang M, Kemere J, Ali AS, Bjorkman A, et al. Prevalence of PCR detectable malaria infection among febrile patients with a negative Plasmodium falciparum specific rapid diagnostic test in Zanzibar. Am J Trop Med Hyg. 2013;88:289–91.
Lover AA, Baird JK, Gosling R, Price RN. Malaria elimination: time to target all species. Am J Trop Med Hyg. 2018;99:17–23.
Twohig KA, Pfeffer DA, Baird JK, Price RN, Zimmerman PA, Hay SI, et al. Growing evidence of Plasmodium vivax across malaria-endemic Africa. PLoS Negl Trop Dis. 2019;13: e0007140.
Hawadak J, Dongang RR, Singh V. Global trend of Plasmodium malariae and Plasmodium ovale spp malaria infections in the last two decades (2000–2020): a systematic review and meta-analysis. Parasit Vectors. 2021;14:297.
Grandesso F, Nabasumba C, Nyehangane D, Page AL, Bastard M, De Smet M, et al. Performance and time to become negative after treatment of three malaria rapid diagnostic tests in low and high malaria transmission settings. Malar J. 2016;15:496.
Dalrymple U, Arambepola R, Gething PW, Cameron E. How long do rapid diagnostic tests remain positive after anti-malarial treatment? Malar J. 2018;17:228.
Vafa Homann M, Emami SN, Yman V, Stenstrom C, Sonden K, Ramstrom H, et al. Detection of malaria parasites after treatment in travelers: a 12-months longitudinal study and statistical modelling analysis. EBioMedicine. 2017;25:66–72.
Haanshuus CG, Morch K. Detection of remaining Plasmodium DNA and gametocytes during follow up after curative malaria treatment among returned travellers in Norway. Malar J. 2020;19:296.
Acknowledgements
We would like to thank Dr. Tom van Gool of the Amsterdam University Medical Centres for kindly providing the Plasmodium-positive and -negative blood samples from returned travellers. Our thanks go to the Sanquin Amsterdam Blood Bank for the provision of blood samples from healthy donors. We also thank Zoë Piets (Amsterdam University Medical Centres) for assisting in the sensitivity and specificity assessment, and Lieke Deckers, Merel Schrooten (both Amsterdam University Medical Centres), Japhet Kabalu Tshiongo and Flory Luzolo Khote (both University of Kinshasa, Democratic Republic of the Congo) for participating in the concordance evaluation.
Funding
This work was supported by the EU FP7-Health-2013.0-1 project “Translation of the direct-on-blood PCR-NALFIA system into an innovative near point-of-care diagnostic for malaria” (DIAGMAL) [Grant Number 601714].
Author information
Authors and Affiliations
Contributions
NvD was responsible for the assay optimization to mini16, coordinated and performed the laboratory work, drafted the protocols, analysed the data and drafted the manuscript. SM gave input during the assay optimization phase, provided technical assistance, prepared the P. falciparum culture and critically read the manuscript. EWB and PBvH provided the samples from returned travellers and performed reference testing with Alethia and expert microscopy. EW gave technical support related to the lateral flow strips. PM and HS conceived the study, provided input and feedback during the optimization and evaluation and critically read the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Anonymized clinical samples from patients or blood donors were derived from a pre-established Biobank at the Laboratory for Experimental Parasitology at the Academic Medical Centre (Amsterdam, The Netherlands) and were collected in accordance with the Dutch Medical Research involving Human Subjects Act. Informed consent was obtained from human participants for the use of anonymized specimens according to the ‘no objection’ system, hence the study was exempted from the need for ethical approval according to Dutch law.
Consent for publication
Not applicable.
Competing interests
EW is an employee of Abingdon Health, manufacturer of the NALFIA strips used in the present study. Abingdon Health was not directly involved in the design of the study or the data analysis.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
van Dijk, N.J., Menting, S., Wentink-Bonnema, E.M.S. et al. Laboratory evaluation of the miniature direct-on-blood PCR nucleic acid lateral flow immunoassay (mini-dbPCR-NALFIA), a simplified molecular diagnostic test for Plasmodium. Malar J 22, 98 (2023). https://doi.org/10.1186/s12936-023-04496-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-023-04496-4