
Abstract
Background
Recently, the De Ritis (AST/ALT) ratio has been considered as a prognostic biomarker for various malignancies. We conducted this systematic review and meta-analysis to explore the prognostic value of preoperative De Ritis ratio in patients after surgery for urothelial carcinoma.
Methods
We searched the online database Embase, PubMed and Cochrane Library up to October 2019. The hazard ratio (HR) and 95% confidence interval (CI) were extracted from the studies.
Results
A total of 8 studies incorporating 3949 patients were included in the quantitative synthesis. We observed that elevated preoperative De Ritis ratio is associated with inferior OS (HR = 1.97; 95% CI 1.70–2.28; P < 0.001), CSS (HR = 2.40; 95% CI 2.02–2.86; P < 0.001), RFS (HR = 1.31; 95% CI 1.11–1.54; P = 0.001), PFS (HR = 2.07; 95% CI 1.68–2.56; P < 0.001) and MFS (HR = 2.39; 95% CI 1.16–4.91; P = 0.018). Stratified by diseases, the elevated De Ritis ratio also served as an unfavorable factor.
Conclusion
The elevated preoperative De Ritis ratio is an unfavorable factor for patients with urothelial carcinoma. In patients with BC and UTUC, the elevated preoperative De Ritis ratio is also associated with poor prognosis. But De Ritis ratio must be validated in large, independent cohorts before it can be applied widely.
Similar content being viewed by others


Background
Urothelial carcinoma (UC) is one of the most commonly diagnosed malignancies, with an estimated 80 thousand new cases and 18 thousand deaths in the United States in 2019 [1]. UC is mainly composed of upper tract urothelial carcinoma (UTUC) and bladder cancer (BC), which are situated at the upper and lower urinary tract, respectively [2]. UTUC is a rare disease that accounts for approximately 5–10% UC, while BC takes up 90–95% of UC and is the most common urinary tract malignancy [3, 4]. Although radical nephroureterectomy (RUN) with bladder cuff excision is the standard treatment for patients with non-metastatic UTUC, high incidences of postoperative disease recurrence have been reported [2, 5]. Radical cystectomy (RC) is the standard approach in patients with non-metastatic muscle-invasive bladder cancer (MIBC) and high-risk non-muscle-invasive bladder cancer (NMIBC), while the 5-year overall survival (OS) rate after RC is approximately 60% [4, 6, 7].
Thus, it is important to precisely predict clinical course after surgery during counseling to determine the suitable treatment and follow-up strategies for individual patients with UC. Pathological T stage and tumor grade are established prognostic factors, besides several prognostic favors are also presented, including lymphovascular invasion, tumor necrosis, Eastern Cooperative Oncology Group Performance Status (ECOG-PS), systemic inflammation and others [2, 4, 6,7,8].
Aminotransaminases, including aspartate aminotransaminase (AST) and alanine aminotransaminase (ALT), are enzymes released from the liver cell into the blood stream, reflecting hepatocellular damage [9]. The ratio of the serum activities of AST to ALT, firstly described by De Ritis and known as the De Ritis ratio [10]. The De Ritis ratio has been used as a predictor of several chronic liver diseases [11]. Recently, this ratio has been considered as a prognostic biomarker for various malignancies, such as renal cell carcinoma, pancreatic cancer, and breast cancer [12,13,14]. While in patients with surgically treated UC, the prognostic value of De Ritis ratio is still unclear. Nishikawa et al. found that elevated De Ritis ratio is associated with recurrence-free survival (RFS) in patients with UC, while the other study did not detect the significant association between elevated De Ritis ratio and RFS [15, 16]. As a result, we conducted this systematic review and meta-analysis to explore the prognostic value of preoperative De Ritis ratio in patients after surgery for UC.
Method
Literature search strategy
Based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement, we conducted this systematic review and meta-analysis. We searched the PubMed, Embase, the Cochrane library up to October 2019. We applied the following items: urothelial carcinoma (urothelial, bladder, tumor, cancer or carcinoma) and De Ritis ratio (aspartate aminotransferase, AST, alanine aminotransferase, ALT, AST/ALT ratio, AST to ALT ratio) as keywords or Mesh. We also screened the reference lists of all eligible studies to ensure comprehensive search. Two reviewers screened the literature independently, any disagreements were resolved by discussing or consulting another one.
Inclusion and exclusion criteria
We included articles conforming to the following inclusion criteria: (1) random-controlled studies or observational studies; (2) patients were diagnosed urothelial carcinoma and underwent surgery; (3) De Ritis ratio was obtained before surgery; (4) evaluated the prognostic value of preoperative De Ritis ratio, (5) reported available data for analyses, for example: overall survival (OS), cancer-specific survival (CSS), recurrence-free survival (RFS), progression-free survival (PFS) or metastasis-free survival (MFS). The following studies were excluded: (1) non-English language; (2) patients did not undergo surgery; (3) did not involve the De Ritis ratio, (4) no available data for analyses. We did not include conference abstracts owing to incomplete information. Regarding duplicated records, we only included the most recent and informative study.
Data extraction and quality assessment
Two reviewers extracted items from all eligible studies independently, which are as follows: the name of the first author and published year, enrollment data and location, study type, diseases, intervention, number of patients, age, the cutoff value of the De Ritis ratio, the duration of follow-up. Concerning the clinical outcome such as OS, CSS, RFS, and PFS, we extracted hazard ratio (HR) and 95% confidence interval (CI) from the studies. If the HRs and 95% CI were not revealed, we could calculate the HR and 95% CI based on the method by Tierney [17]. We used the Newcastle–Ottawa Quality Assessment Scale (NOS) to evaluate the quality of the observational studies. And studies with a score of no less than 7 were considered as good quality.
Statistical analysis
We conducted all statistical analyses by using STATA version 12 (StataCorp, College Station, TX, USA). As for the clinical outcome, we pooled the HRs and 95% CI. And we used Q and I2 statistics to evaluate the heterogeneity among studies. A random-effect model was used when we observed the significant heterogeneity (P < 0.10 or I2 > 50%); otherwise, a fixed-effect model was used [18]. We also carried out subgroup analyses based on available data. In addition, we performed sensitivity analyses to test the robustness of the final results. In terms of the publication bias, we used Egger’s test and Begg’s test. A two-sided P-value < 0.05 was considered as a statistical difference.
Results
Study search
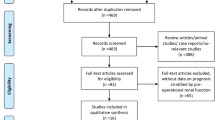
The study search strategy yield 304 studies, 5 of which were duplicated records. After screening titles and abstracts of the remaining 299 studies, 20 studies were reviewed comprehensively. Finally, a total of 8 studies incorporating 3949 patients were included in the quantitative synthesis [15, 16, 19,20,21,22,23,24]. The flow diagram of the study search and selection is presented in Fig. 1.

Flow chart of study selection
Characteristics of included studies
Of the enrolled 8 studies, all are published in recent 3 years and are retrospective. Five studies involved the patients with UTUC and underwent RUN [15, 16, 20], 3 studies involved patients with BC and treated by RC [19, 21, 22]. The median ages of patients were similar, ranging from 61 to 69. All studies defined the De Ritis ratio as a dichotomous variable, which was measured before surgery. Most studies had a relatively long follow-up, and median follow-up ranged from 33.3 months to 84 months, while one study did not report the duration of the follow-up [22]. Seven studies observed the OS and CSS, 3 studies revealed the clinical outcome of RFS and PFS, and only one study involves the MFS. Detailed characteristics of the included studies were shown in Table 1. All studies included in our meta-analysis were considered as high quality (Table 1).
Overall survival
Regarding 7 studies including 3814 patients, the pooled results demonstrated that elevated De Ritis ratio was significantly associated with worse OS, the pooled HR was 1.97 (95% CI 1.70–2.28; P < 0.001). We did not detect significant heterogeneity among studies (I2 = 0.0%, P = 0.563, Fig. 2a).

a The association between preoperative De Ritis ratio and OS in patients with UC. b The association between preoperative De Ritis ratio and CSS in patients with UC. c The association between preoperative De Ritis ratio and PFS in patients with UC. d The association between preoperative De Ritis ratio and RFS in patients with UC
Cancer-specific survival
As shown in Fig. 3, we demonstrated that the patients with elevated preoperative De Ritis ratio had an inferior CSS. The pooled HR was 2.40 (95% CI 2.02–2.86; P < 0.001). No evidence of heterogeneity was revealed (I2 = 23.7%, P = 0.248, Fig. 2b).

Sensitivity analyses for a OS. b CSS
Progression-free survival and recurrence-free survival and metastasis-free survival
In terms of 2 studies incorporating 1727 patients and 1955 patients, we found that the patients with a higher De Ritis ratio had a significantly increased risk of progression and recurrence compared with those with lower De Ritis ratio. The pooled HRs for PFS and RFS were 2.07 (95% CI 1.68–2.56; P < 0.001; Fig. 2c) and 1.31 (95% CI 1.11–1.54; P = 0.001; Fig. 2d), respectively. There was also no heterogeneity among studies. Only one study reported the MFS and higher De Ritis ratio was associated with an increased risk of metastasis (HR = 2.39; 95% CI 1.16–4.91; P = 0.018).
Publication bias and sensitivity analysis
Because of the small number of included studies, we only performed publication bias and sensitivity analysis for OS and CSS. We carried out sensitivity analyses by removing each study sequentially. After removing each study sequentially, we did not observe a relative change, which showed the stability of our results (Fig. 3). Regarding publication bias, we did not detect significant publication bias of OS and CSS according to the Begg’s test (OS: P = 0.230; CSS: P = 0.230) and Egger’s test (OS: P = 0.059; CSS: P = 0.106).
Subgroup analyses
Due to the small number of enrolled studies, we only performed subgroup analyses for OS and CSS and stratified by, the number of patients, cutoff value and diseases. For the studies that included ≤ 500 patients, the elevated De Ritis ratio was significant associated with worse OS (HR = 2.30; 95% CI 1.66–3.20; P < 0.001) and CSS (HR = 2.73; 95% CI 1.82–4.10; P < 0.001). And in the > 500 patients subgroup, higher De Ritis was also considered as an unfavorable factor for OS (HR = 1.90; 95% CI 1.61–2.23; P < 0.001) and CSS (HR = 2.34; 95% CI 1.93–2.83; P < 0.001). In cutoff value of ≤ 1.3 subgroup, the patients with elevated De Ritis ratio has a worse OS (HR = 1.88; 95% CI 1.57–2.26; P < 0.001) and CSS (HR = 2.30; 95% CI 1.84–2.88; P < 0.001). Similarly, in the cutoff value of > 1.3 subgroup, higher De Ritis ratio was associated with worse OS (HR = 2.13; 95% CI 1.67–2.71; P < 0.001) and CSS (HR = 2.57; 95% CI 1.95–3.39; P < 0.001). Furthermore, stratified by diseases, elevated De Ritis ratio could serve as an unfavorable factor for OS (HR = 2.08; 95% CI 1.73–2.51; P < 0.001) and CSS (HR = 2.59; 95% CI 2.08–3.21; P < 0.001) in the patients with UTUC. In addition, in the subgroup of BC, the elevated De Ritis ratio was significantly associated with inferior OS (HR = 1.80; 95% CI 1.43–2.27; P < 0.001) and CSS (HR = 2.71; 95% CI 1.38–5.31; P = 0.004). The detailed information was summarized in Table 2.
Discussion
Despite the development of surgical techniques and adjuvant therapies, the prognosis of patients with UC did not improve a lot. Several prognostic factors were proposed in recent years, including lymphovascular invasion, tumor necrosis, Eastern Cooperative Oncology Group Performance Status (ECOG-PS), systemic inflammation and others [2, 4, 6,7,8].
In this study, we evaluated the prognostic value of De Ritis ratio in patients with surgically treated UC. We demonstrated that a higher preoperative De Ritis ratio is associated with inferior OS, CSS, PFS, and RFS. When stratified by diseases, the elevated preoperative De Ritis ratio was also an unfavorable factor in patients with either BC or UTUC. Regarding the difference of cutoff values, we divided studies into ≤ 1.3 and > 1.3 groups and found that elevated De Ritis ratio is correlated to poor OS and CSS. In addition, we conducted sensitivity analyses and did not observe a relatively big change. There was also no evidence for publication bias, reflecting the robustness of our results.
So far, several studies have shown the prognostic value of aminotransaminases in patients with malignancies irrespective of the presence of liver-specific disease [12,13,14, 25, 26]. For example, Stocken et al. found that AST was associated with overall survival in patients with pancreatic cancer [13]. Generally, AST is widely expressed in various tissues such as the brain, muscle, kidney, but ALT is regarded as more liver-specific or enriched [11]. Pathological processes were shown to bring about tissue damage and higher proliferative status, and high tumor cell turnover tends to increase AST rather than ALT, making the De Ritis ratio an attractive potential biomarker [27].
De Ritis ratio, the ratio of the serum activities of AST to ALT, was firstly described by De Ritis [10]. The De Ritis ratio was mostly used as a predictor of several chronic liver diseases in previous studies [11]. Currently, several studies have demonstrated that the De Ritis ratio could serve as a prognostic factor in patients with several cancers. For instance, Bezan et al. enrolled 698 patients with nonmetastatic renal cell carcinoma and found that increased (≥ 1.26) preoperative AST/ALT ratio was an independent prognostic factor for metastasis-free survival (HR 1.61, 95% CI 1.25–2.07, P < 0.001) and OS (HR 1.76, 95% CI 1.34–2.32, P < 0.001). Furthermore, Lee et al. revealed that elevated AST/ALT ratio was an unfavorable factor for OS, CSS, and PFS in patients surgically treated for localized clear-cell RCC [28]. We summarized all available studies and also found that elevated De Ritis ratio is associated with poor prognosis in patients after surgery for urothelial carcinoma.
The association between the De Ritis ratio and histological tumor necrosis, pathological T stage strength this finding. Currently, tumor metabolism has gained attention concerning the carcinogenesis of malignancies. The Warburg effect is the well-known cancer metabolism, describing the abnormal anaerobic glycolysis in cancer cells for producing adenosine triphosphate (ATP) regardless of the availability of the oxygen [29]. Increased glycolysis is shown to be associated with mitochondrial dysfunction linked to nicotinamide adenine dinucleotide (NAD)-related enzymes and glucose transporters [30]. Furthermore, AST is a component of a malate-aspartate shuttle pathway that allows NADH/NAD+ conversion [31]. Therefore, the De Ritis ratio might be related to tumor metabolism in many glucose-using cancers. Reportedly, urothelial carcinoma was associated with glucose metabolism [32]. Whyard et al. researched the uptake of fluorescent glucose by bladder cancer cells using fluorescence microscopy and observed significant differences in glucose consumption between normal urothelium and malignant urothelial cells [33]. Based on these findings and our study, it is highly likely that the De Ritis ratio is associated with the prognosis of patients with urothelial carcinoma. But the detailed interaction between the De Ritis ratio and poor prognosis of patients with urothelial carcinoma remains to be explored.
The De Ritis ratio has important implications for clinical practice. The patients with a higher De Ritis ratio had an inferior survival. It may serve as a potential selection criterion for risk factor stratified management of urothelial carcinoma and adjuvant therapies. Besides, close postoperative follow-up should be emphasized for these patients. The AST/ALT ratio is easily accessible and relatively inexpensive because AST and ALT are the most commonly used serum biomarkers in our daily clinical practice.
Despite our novel findings, the present study has some limitations. Firstly, a total of 8 studies incorporating 3949 patients was included in the quantitative synthesis, which is a relatively small number and may limit the power of the final results. So more studies are needed to validate our findings. Secondly, all studies are retrospective, which may increase the risk of bias because of the retrospective data analysis. Thirdly, although included studies tried to exclude all patients with acute or chronic liver disease, they may not eliminate the undetected diseases that confounded results. As results, the De Ritis ratio must be validated in large, independent cohorts before it can be applied widely.
Conclusion
The preoperative De Ritis ratio is an unfavorable factor for patients with urothelial carcinoma. When stratified by diseases, in patients with BC and UTUC, the De Ritis ratio is also associated with poor prognosis. However, the De Ritis ratio must be validated in large, independent cohorts before it can be applied widely.
Availability of data and materials
All the data (pooled HR with 95% CI of OS, CSS, PFS, RFS, and MFS) used to support the findings of this study are included within the article.
Abbreviations
- UTUC:
-
Upper tract urothelial carcinoma
- BC:
-
Bladder cancer
- RUN:
-
Radical nephroureterectomy
- RC:
-
Radical cystectomy
- OS:
-
Overall survival
- CSS:
-
Cancer-specific survival
- PFS:
-
Progression-free survival
- RFS:
-
Recurrence-free survival
- MFS:
-
Metastasis-free survival
- NOS:
-
Newcastle–Ottawa quality assessment scale
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- MIBC:
-
Muscle-invasive bladder cancer
- NMIBC:
-
Non-muscle-invasive bladder cancer
- ECOG-PS:
-
Eastern cooperative oncology group performance status
- AST:
-
Aspartate aminotransaminase
- ALT:
-
Alanine aminotransaminase
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA: Cancer J Clin. 2019;69(1):7–34.
Roupret M, Babjuk M, Comperat E, Zigeuner R, Sylvester RJ, Burger M, Cowan NC, Bohle A, Van Rhijn BW, Kaasinen E, et al. European association of urology guidelines on upper urinary tract urothelial cell carcinoma: 2015 update. Eur Urol. 2015;68(5):868–79.
Raman JD, Messer J, Sielatycki JA, Hollenbeak CS. Incidence and survival of patients with carcinoma of the ureter and renal pelvis in the USA, 1973–2005. BJU Int. 2011;107(7):1059–64.
Babjuk M, Bohle A, Burger M, Capoun O, Cohen D, Comperat EM, Hernandez V, Kaasinen E, Palou J, Roupret M, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2016. Eur Urol. 2017;71(3):447–61.
Margulis V, Shariat SF, Matin SF, Kamat AM, Zigeuner R, Kikuchi E, Lotan Y, Weizer A, Raman JD, Wood CG. Outcomes of radical nephroureterectomy: a series from the upper tract urothelial carcinoma collaboration. Cancer. 2009;115(6):1224–33.
Alfred Witjes J, Lebret T, Comperat EM, Cowan NC, De Santis M, Bruins HM, Hernandez V, Espinos EL, Dunn J, Rouanne M, et al. Updated 2016 EAU guidelines on muscle-invasive and metastatic bladder cancer. Eur Urol. 2017;71(3):462–75.
Stein JP, Lieskovsky G, Cote R, Groshen S, Feng AC, Boyd S, Skinner E, Bochner B, Thangathurai D, Mikhail M, et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol. 2001;19(3):666–75.
Lughezzani G, Burger M, Margulis V, Matin SF, Novara G, Roupret M, Shariat SF, Wood CG, Zigeuner R. Prognostic factors in upper urinary tract urothelial carcinomas: a comprehensive review of the current literature. Eur Urol. 2012;62(1):100–14.
Ozer J, Ratner M, Shaw M, Bailey W, Schomaker S. The current state of serum biomarkers of hepatotoxicity. Toxicology. 2008;245(3):194–205.
De Ritis F, Coltorti M, Giusti G. An enzymic test for the diagnosis of viral hepatitis; the transaminase serum activities. Clin Chimi Acta. 1957;2(1):70–4.
Botros M, Sikaris KA. The De Ritis ratio: the test of time. Clin Biochem Rev. 2013;34(3):117–30.
Bezan A, Mrsic E, Krieger D, Stojakovic T, Pummer K, Zigeuner R, Hutterer GC, Pichler M. The preoperative AST/ALT (De Ritis) ratio represents a poor prognostic factor in a cohort of patients with nonmetastatic renal cell carcinoma. J Urol. 2015;194(1):30–5.
Stocken DD, Hassan AB, Altman DG, Billingham LJ, Bramhall SR, Johnson PJ, Freemantle N. Modelling prognostic factors in advanced pancreatic cancer. Br J Cancer. 2008;99(6):883–93.
Thornburg JM, Nelson KK, Clem BF, Lane AN, Arumugam S, Simmons A, Eaton JW, Telang S, Chesney J. Targeting aspartate aminotransferase in breast cancer. Breast Cancer Res. 2008;10(5):R84.
Nishikawa M, Miyake H, Kurahashi T, Fujisawa M. Significance of multiple preoperative laboratory abnormalities as prognostic indicators in patients with urothelial carcinoma of the upper urinary tract following radical nephroureterectomy. Int J Clin Oncol. 2018;23(1):151–7.
Lee H, Choi YH, Sung HH, Han DH, Jeon HG, Chang Jeong B, Seo SI, Jeon SS, Lee HM, Choi HY. De Ritis Ratio (AST/ALT) as a significant prognostic factor in patients with upper tract urothelial cancer treated with surgery. Clin Genitourin Cancer. 2017;15(3):e379–85.
Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007;8:16.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Yuk HD, Jeong CW, Kwak C, Kim HH, Ku JH. De Ritis Ratio (aspartate transaminase/alanine transaminase) as a significant prognostic factor in patients undergoing radical cystectomy with bladder urothelial carcinoma: a propensity score-matched study. Dis Markers. 2019;2019:6702964.
Li Y, Fang D, Bao Z, He A, Guan B, He S, Zhan Y, Gong Y, Li X, Zhou L. High aspartate transaminase/alanine transaminase ratio predicts poor prognosis in patients with localized upper tract urothelial cancer: a propensity score-matched study in a large Chinese center. Onco Targets Ther. 2019;12:2635–48.
Ha YS, Kim SW, Chun SY, Chung JW, Choi SH, Lee JN, Kim BS, Kim HT, Yoo ES, Kwon TG, et al. Association between De Ritis ratio (aspartate aminotransferase/alanine aminotransferase) and oncological outcomes in bladder cancer patients after radical cystectomy. BMC Urol. 2019;19(1):10.
Gorgel SN, Kose O, Koc EM, Ates E, Akin Y, Yilmaz Y. The prognostic significance of preoperatively assessed AST/ALT (De Ritis) ratio on survival in patients underwent radical cystectomy. Int Urol Nephrol. 2017;49(9):1577–83.
Gao X, Chen W, Zhang R, Wu C, Li Y, Zhu H, Deng Z, Yu Z, Wu S, Pan Y. Preoperative AST/ALT ratio predicts long-term survival after radical nephroureterectomy in patients with upper tract urothelial carcinoma. Int J Clin Exp Med. 2017;10(5):8464–71.
Cho YH, Hwang JE, Chung HS, Kim MS, Hwang EC, Jung SI, Kang TW, Kwon DD, Choi SH, Kim HT, et al. The De Ritis (aspartate transaminase/alanine transaminase) ratio as a predictor of oncological outcomes in patients after surgery for upper urinary tract urothelial carcinoma. Int Urol Nephrol. 2017;49(8):1383–90.
Tan X, Xiao K, Liu W, Chang S, Zhang T, Tang H. Prognostic factors of distal cholangiocarcinoma after curative surgery: a series of 84 cases. Hepatogastroenterology. 2013;60(128):1892–5.
Takenaka Y, Takemoto N, Yasui T, Yamamoto Y, Uno A, Miyabe H, Ashida N, Shimizu K, Nakahara S, Hanamoto A, et al. Transaminase activity predicts survival in patients with head and neck cancer. PLoS ONE. 2016;11(10):e0164057.
Conde VR, Oliveira PF, Nunes AR, Rocha CS, Ramalhosa E, Pereira JA, Alves MG, Silva BM. The progression from a lower to a higher invasive stage of bladder cancer is associated with severe alterations in glucose and pyruvate metabolism. Exp Cell Res. 2015;335(1):91–8.
Lee H, Lee SE, Byun SS, Kim HH, Kwak C, Hong SK. De Ritis ratio (aspartate transaminase/alanine transaminase ratio) as a significant prognostic factor after surgical treatment in patients with clear-cell localized renal cell carcinoma: a propensity score-matched study. BJU Int. 2017;119(2):261–7.
Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science. 2009;324(5930):1029–33.
Dorward A, Sweet S, Moorehead R, Singh G. Mitochondrial contributions to cancer cell physiology: redox balance, cell cycle, and drug resistance. J Bioenerg Biomembr. 1997;29(4):385–92.
Greenhouse WV, Lehninger AL. Occurrence of the malate-aspartate shuttle in various tumor types. Cancer Res. 1976;36(4):1392–6.
Tai YS, Chen CH, Huang CY, Tai HC, Wang SM, Pu YS. Diabetes mellitus with poor glycemic control increases bladder cancer recurrence risk in patients with upper urinary tract urothelial carcinoma. Diab/Metab Res Rev. 2015;31(3):307–14.
Whyard T, Waltzer WC, Waltzer D, Romanov V. Metabolic alterations in bladder cancer: applications for cancer imaging. Exp Cell Res. 2016;341(1):77–83.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
Conception and design: XL and XH; Collection and assembly of data: XH, YW, and W-XY; Data analysis and interpretation: XL, XH and S-CX; Manuscript writing: All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hu, X., Yang, WX., Wang, Y. et al. The prognostic value of De Ritis (AST/ALT) ratio in patients after surgery for urothelial carcinoma: a systematic review and meta-analysis. Cancer Cell Int 20, 39 (2020). https://doi.org/10.1186/s12935-020-1125-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12935-020-1125-2