
Abstract
Background
The triglyceride-glucose (TyG) index and its combination with obesity indicators can predict cardiovascular diseases (CVD). However, there is limited research on the relationship between changes in the triglyceride glucose-waist height ratio (TyG-WHtR) and CVD. Our study aims to investigate the relationship between the change in the TyG-WHtR and the risk of CVD.
Methods
Participants were from the China Health and Retirement Longitudinal Study (CHARLS). CVD was defined as self-reporting heart disease and stroke. Participants were divided into three groups based on changes in TyG-WHtR using K-means cluster analysis. Multivariable binary logistic regression analysis was used to examine the association between different groups (based on the change of TyG-WHtR) and CVD. A restricted cubic spline (RCS) regression model was used to explore the potential nonlinear association of the cumulative TyG-WHtR and CVD events.
Results
During follow-up between 2015 and 2020, 623 (18.8%) of 3312 participants developed CVD. After adjusting for various potential confounders, compared to the participants with consistently low and stable TyG-WHtR, the risk of CVD was significantly higher in participants with moderate and increasing TyG-WHtR (OR 1.28, 95%CI 1.01–1.63) and participants with high TyG-WHtR with a slowly increasing trend (OR 1.58, 95%CI 1.16–2.15). Higher levels of cumulative TyG-WHtR were independently associated with a higher risk of CVD events (per SD, OR 1.27, 95%CI 1.12–1.43).
Conclusions
For middle-aged and older adults, changes in the TyG-WHtR are independently associated with the risk of CVD. Maintaining a favorable TyG index, effective weight management, and a reasonable waist circumference contribute to preventing CVD.
Similar content being viewed by others


Introduction
Cardiovascular diseases (CVD) are the leading cause of global mortality. Although global age-standardized CVD mortality decreased by 34.9% from 1990 to 2022, the actual number of CVD deaths has increased significantly [1, 2]. 2022 alone, CVD caused an estimated 19.8 million deaths worldwide, corresponding to 396 million years of life lost and another 44.9 million years lived with disability (YLD) [1, 2]. Early identification of high-risk groups for CVD and timely intervention to control CVD risk factors contribute to preventing the disease progression.
Insulin resistance (IR) is associated with asymptomatic atherosclerosis and coronary artery disease and is considered as predictor of CVD [3, 4]. The triglyceride-glucose index has high sensitivity and specificity in assessing IR in individuals [5]. Recent studies showed that, as a valuable biomarker of IR, triglyceride-glucose index(TyG) could be used to predict the occurrence of CVD [6, 7]. Furthermore, TyG also performed excellently in predicting the outcomes of CVD patients [8, 9].
Obesity is closely associated with various health risks, and increased abdominal fat is linked to CVD via multiple direct and indirect pathophysiological mechanisms [10]. Some studies proved that TyG combined with adiposity indices performs better than only the TyG index in assessing IR and cardiovascular risk [11]. Two previous studies used the TyG index at baseline combined with different obesity indicators to form new indicators, including TyG-BMI, TyG-WC, and TyG-WhtR, to analyze the association of these new indicators and CVD events [11, 13]. These studies were from the National Health and Nutrition Examination Survey (NHANES) [11] and the Kailuan study [13]. TyG-WHtR performed the best in identifying high-risk populations for CVD events and CVD mortality. WHtR is a standardized waist circumference measurement method that is more objective than simple waist circumference measurement. Previous studies were primarily based on the TyG index and related indicators at a single time point. However, the TyG index is a dynamic state that changes over time. We hypothesized that the dynamic change of TyG-WHtR can better predict CVD. Our study aims to investigate the relationship between the change of TyG-WHtR and the risk of CVD.
Methods
Study design and population
Our study is based on data from the China Health and Retirement Longitudinal Study (CHARLS), a national population-based cohort study. The study design has been previously described [14]. The CHARLS national baseline survey (Wave 1) spanned from June 2011 to March 2012, encompassing 17,708 individual participants. A multistage probability sampling technique selected participants from 150 counties or regions and 450 villages or urban communities in China. Up to date, four subsequent follow-up surveys were conducted every 2 years (Wave 2 in 2013, Wave 3 in 2015, Wave 4 in 2018, and Wave 5 in 2020).
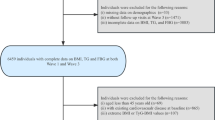
In this study, we included 11,847 participants who participated in blood tests. We excluded participants for reasons including (1) lack of fasting blood glucose (FBG) or triglycerides (TG) at Wave 1 or Wave 3. (2) Missing or abnormal height and waist measurements. (3) under 45 years of age. (4) People who had CVD events before Wave 3 (2015) or lacked information about CVD. The detailed inclusion and exclusion process is shown in Fig. 1.

Flow chart of the study population
The Biomedical Ethics Review Board of Peking University gave its ethical approval for gathering CHARLS data (IRB00001052-11015), and all participants signed an informed consent form.
Assessment of the change in TyG-WHtR
Fasting status, blood glucose, and triglyceride levels were obtained from the blood sample examinations at Wave 1 and Wave 3. Any height variation exceeding 10 cm between measurements taken at Wave 1 and Wave 3 was deemed an abnormal height measurement. Any waist measurement that deviates from the overall mean waist measurement by more than three standard deviations (either above or below) was classified as an abnormal waist measurement. TyG, WHtR, TyG-WHtR, and cumulative TyG-WHtR were calculated according to the following formulas [11, 15]: (1) TyG = ln [triglycerides (mg/dl) × glucose (mg/dl)/2]; (2) WHtR = waist circumference/height; (3) TyG-WHtR = TyG × WHtR; (3) Cumulative TyG-WHtR = (TyG-WHtR2012 + TyG-WHtR2015)/2 × time(2015–2012).
Assessment of CVD
The presence of heart disease was determined by the question, “Have you been diagnosed with heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems by a doctor?” Similarly, the occurrence of stroke was ascertained through the question, “Have you been diagnosed with stroke by a doctor?” CVD was defined as self-reporting heart disease and stroke. Participants were required to reaffirm CVD in the subsequent wave if they reported heart disease or stroke in the previous wave. When participants denied their previous self-reported diagnoses of heart disease or stroke, these inconsistencies were rectified retrospectively. Our CVD ascertainment was consistent with previous studies using the CHARLS [16].
Covariates
The covariates included sociodemographic characters (age, sex, marital status, hukou status, education, smoking status, and drinking status), health conditions (systolic blood pressure, diastolic blood pressure, hypertension, diabetes, dyslipidemia, and cancer), and laboratory examination total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and glycosylated hemoglobin (HbA1c)). Hypertension was defined as systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg or self-reported diagnosis history of hypertension or use of any antihypertensive treatment. Diabetes was defined as fasting glucose ≥ 7.0 mmol/L or self-reported diagnosis history of diabetes or use of any hypoglycemic medication. Dyslipidemia was defined as TC ≥ 240 mg/dl, triglycerides ≥ 150 mg/dl, LDL-C ≥ 160 mg/dl, HDL-C < 40 mg/dl, self-reported dyslipidemia or use of lipid-lowering treatment [15].
Statistical analyses
K-means clustering analysis is a type of unsupervised machine learning method. We use the elbow method to identify the appropriate number of clusters (Additional file 1: Figure S1). Based on measurements of TyG-WHtR in 2012 and 2015, We classify the participants into three groups: for Class 1 (n = 1141), the TyG-WHtR ranged from 3.96 ± 0.33 in 2012 to 3.97 ± 0.36 in 2015, and the cumulative TyG-WHtR was 11.90 ± 0.82, representing a consistently low and stable TyG-WHtR; for Class 2 (n = 1392), the TyG-WHtR ranged from 4.74 ± 0.34 in 2012 to 4.84 ± 0.34 in 2015, and the cumulative TyG-WHtR was 14.36 ± 0.72, representing a moderate and increasing TyG-WHtR; for Class 3 (n = 779), the TyG-WHtR ranged from 5.72 ± 0.49 in 2012 to 5.78 ± 0.47 in 2015, and the cumulative TyG-WHtR was 17.24 ± 1.18, representing a high TyG-WHtR with a slowly increasing trend (Fig. 2).

Clustering of the change in the TyG-WHtR from 2012 to 2015. A Three clusters were found using the K-means method with Euclidean distance: the x- and y-axes are principal components of the change in the TyG-WHtR; B The change of TyG-WHtR from 2012 to 2015
Continuous variables were described as mean (standard deviation, SD) or median (interquartile range, IQR), while categorical variables were expressed as frequency (proportion). We used multivariable binary logistic regression analysis to examine the association between different clusters (based on measurements of TyG-WHtR) and CVD. The results were shown as odds ratio(ORs) and 95% confidence intervals (CIs). Four models were estimated: Model 1 adjusted for age and gender. Model 2 adjusted for age, gender, marital status, hukou status, educational level, smoking status, and drinking status. Model 3 adjusted for variables in Model 2 and history of hypertension, diabetes, dyslipidemia, and cancer. Model 4 adjusted for variables in Model 3 and systolic blood pressure, diastolic blood pressure, total cholesterol, HDL-C, LDL-C, and HbA1c. We divided participants into four groups based on quartiles of cumulative TyG-WHtR to examine the relationship between cumulative TyG-WHtR and CVD. P values for trend were calculated using the median TyG-WHtR in each quartile. We also used a restricted cubic spline (RCS) regression model to explore the potential nonlinear association of the cumulative TyG-WHtR and CVD events. We fit restricted cubic spline models with 3–5 nodes and then selected the model with the smallest AIC to determine the number of nodes. Additionally, we performed subgroup and interaction analyses to investigate whether the relationships between the change in TyG-WHtR or cumulative TyG-WHtR and CVD varied according to the status of the covariates (gender, marital status, education level, smoking status, drinking status, hypertension, diabetes, and dyslipidemia). Receiver operating characteristic (ROC) curves were used for diagnostic value analysis, and the area under the curve was computed to quantify the predictive power of TyG, WHtR, TyG-WHtR, and cumulative TyG-WHtR for cardiovascular disease. Missing covariates were imputed by multiple imputations using mice package in R. We also repeated analyses using the complete data set (3216 participants) without multiple imputations as sensitivity analysis. A two-sided P value < 0.05 was considered statistically significant. Statistical analysis was performed using R software 4.3.3 and SPSS 26.0.
Results
Baseline characteristics of participants
In this study, 3312 participants were included for analysis. The mean age at baseline was 58.30 ± 8.38 years, and 1499(45.3%) were men. The mean TyG-WHtR was 4.70 ± 0.76 in 2012 and 4.76 ± 0.78 in 2015, and the mean cumulative TyG-WHtR was 14.19 ± 2.19. Based on the cluster analysis, the baseline characteristics of participants in each group are presented in Table 1. Additionally, we described the baseline characteristics of participants in each group based on the cumulative TyG-WHtR (Additional file 1: Table S1).
Odds ratios for incident CVD
During follow-up between 2015 and 2020, 623 participants (18.8%) developed CVD.
The results of logistic regression analyses for the association between the change of TyG-WHtR and CVD are shown in Table 2. After adjustment for all potential confounders in Model 4, compared with Class 1, the risk of CVD was significantly higher in Class 2 (OR 1.28, 95%CI 1.01–1.63) and Class 3 (OR 1.58, 95%CI 1.16–2.15). The RCS regression model showed a linearly increasing relationship between the cumulative TyG-WHtR and the risk of CVD (P for nonlinearity = 0.964). (Fig. 3) In the fully adjusted model, higher levels of cumulative TyG-WHtR were independently associated with a greater risk of CVD event (per SD, OR 1.27, 95%CI 1.12–1.43). Results were similar when we categorized participants by cumulative TyG-WHtR quartiles. In the final model, compared with the first quartile, the adjusted ORs (95%CI) for CVD were 1.28 (0.96–1.71) for the second quartile, 1.52 (1.13–2.06) for the third quartile, and 1.67 (1.19–2.34) for the fourth quartile. Additional file 1: Table S2 provided the results of logistic regression analyses for heart disease and stroke.

Cubic model of the association between cumulative TyG-WHtR index and (A) CVD; (B) heart disease; (C)stroke
The ROC curve indicated that cumulative TyG-WHtR (AUC 0.596, 95%CI 0.572–0.621) had the highest diagnostic efficacy for CVD, followed by TyG-WHtR at baseline (AUC 0.596, 95%CI 0.572–0.621), WHtR at baseline (AUC 0.584, 95%CI 0.559–0.609), and TyG at baseline (AUC 0.568, 95%CI 0.544–0.593).(Fig. 4) Cumulative TyG-WHtR also had the highest diagnostic efficacy for heart disease and stroke. (Additional file 1: Figures S2, S3).

Receiver operating characteristic curves for baseline TyG, WHtR, and TyG-WHtR predicting CVD (A) and cumulative TyG-WHtR predicting CVD (B)
Subgroup analyses and sensitivity analyses
Tables 3, 4 show the association of the change of TyG-WHtR with CVD risk and cumulative TyG-WHtR with CVD risk stratified by different factors, respectively. Except for marital status, subgroups did not have significant interactions. Sensitivity analyses yielded congruent results when performing complete data analyses. (Additional file 1: Table S3).
Discussion
In this study, we observed the relationship between TyG-WHtR changes and CVD. A chronically higher TyG-WHtR or a higher cumulative TyG-WHtR is associated with a higher incidence of CVD events. The ability of TyG-WHtR to assess CVD risk is superior to that of TyG alone and WHtR alone, and cumulative TyG-WHtR, an indicator of dynamic change of TyG-WHtR, has the best performance. However, TyG-WHtR may not assess CVD risks in unmarried population.
Initially, the TyG index alone was used to predict CVD events. In 2016, a groundbreaking study revealed a significant positive correlation between the TyG index and CVD events [6]. Their analysis, which involved 5014 patients from the Vascular Metabolic CUN cohort, spanned a median follow-up period of 10 years. According to the quintiles of the TyG index, they divided the patients into five groups. The risk of CVD in the group with the highest TyG index was 2.32 times that in the group with the lowest TyG index. They also found that the TyG index can improve the accuracy of Framingham model predicting the occurrence of coronary heart disease [6]. Since obesity and cardiovascular disease are closely related, some studies gradually used the TyG index combined with anthropometric and adiposity indicators to predict CVD events. Several studies reported the role of the TyG-BMI index in predicting the incidence of CVD events [15, 17]. A systematic review and meta-analysis suggested the WHtR index was better than BMI and waist circumference at predicting CVD risk [18]. As a good indicator of central (visceral) adipose tissue and a marker of ‘early health risk’ [19], WHtR was recommended to replace BMI in the evaluation of adiposit [20]. A recent study included 11,937 adults from the National Health and Nutrition Examination Survey (NHANES), and they found that the TyG-WHtR index had the highest predictive power for CVD mortality rather than the TyG index [11]. These results suggested that TyG-WHtR will become a more helpful tool for risk stratification and identifying groups at early risk of cardiovascular disease.
Considering that the TyG index changes dynamically over time, researchers began to study the impact of changes on CVD events. Recently, Cui et al. demonstrated that cumulative TyG index was associated with an increased risk of CVD [7]. Huo et al. also found that changes in the TyG-BMI may help identify individuals at higher risk of stroke [15]. However, few studies have investigated the association between changes in TyG-WHtR and CVD.
Our study used K-means clustering analysis to classify individuals into three groups by the change of TyG-WHtR and cumulative TyG-WHtR. Compared to the first group of participants who have consistently low and stable TyG-WHtR, both the second group with moderate and increasing TyG-WHtR and the third group with high TyG-WHtR and slowly increasing trends have higher risks of CVD. Similarly, results grouped according to cumulative TyG-WHtR quartiles had similar findings. Patients with higher cumulative TyG-WHtR have higher CVD risk.
As a reliable biomarker of IR, the TyG index is consistent with the gold standard, the euglycemic-hyperinsulinemic clamp test, and has superior sensitivity and specificity [5]. Compared with the homeostasis model assessment estimated insulin resistance index, the TyG index performs better in evaluating IR [21]. IR can exacerbate both the initiation and progression of atherosclerosis, and the mechanisms involve systemic factors, particularly dyslipidemia, hypertension, and a pro-inflammatory state [22]. IR is independently associated with elevated cardiovascular risk [23].
The evidence from the UK Biobank demonstrated that WHtR was linearly associated with ischemic CVD, myocardial infarction, and ischemic stroke [24]. Raele et al. suggested that WHtR was positively associated with Coronary Artery Calcium and could be regarded as a promising biomarker for subclinical atherosclerosis [25]. Central adiposity is associated with CVD, and WHtR is a good indicator of assessing central adiposity. Obesity leads to adipose tissue dysfunction, and an imbalance in adipokine levels contributes to a chronic systemic inflammatory response, which is fundamental to the development and progression of cardiovascular complications [26]. Our study also showed that TyG-WHtR had better diagnostic performance than TyG alone and WHtR alone in CVD. The indicator cumulative TyG-WHtR, which takes the time span into consideration, has the highest AUC. Similarly, another study also showed that the utilization of the change in TyG-BMI is valuable in assessing the risk for stroke [15]. These results remind us to pay more attention to the value of dynamic monitoring of CVD risk factors.
To verify whether our findings were applicable in different populations, we performed subgroup analyses. Subgroup analyses were consistent with the major findings except in the subgroups of unmarried individuals. Similarly, Huo et al. found that marital status moderates the association of cumulative TyG-BMI with stroke [15]. A previous meta-analysis, including 34 studies and more than two million participants, found that unmarried status was associated with increased odds of CVD [27]. A large prospective cohort study also demonstrated that living singly was associated with a higher risk of CVD [28]. These results suggest that the unmarried population is associated with a higher cardiovascular risk, and the TyG-WHtR index may not predict high-risk CVD individuals in this group.
Our study also has some limitations. Firstly, our participants were all from the Chinese elderly population, so these findings may not be generalizable to other countries or other age groups. Secondly, while the rate of lost follow-up in this study is acceptable, the occurrence of competing events, such as death due to cardiovascular diseases, may underestimate the relationship between TyG and CVD. Last, in our study, CVD is defined as self-reporting heart disease and stroke, which might lead to a misclassification bias. However, previous studies shown that self-reported was basically consistent with medical records and misreporting was nonsystematic, which means the potential misclassification bias was minor [16, 29, 30].
Conclusion
In our study, we discovered that changes in TyG-WHtR are associated with a higher incidence of CVD events. For individuals with a persistently high and increasing trend in TyG-WHtR over the long term, measures such as exercising, losing weight, or modifying lifestyle habits should be taken to reduce the risk of CVD.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- TyG index:
-
Triglyceride-glucose index
- CVD:
-
Cardiovascular diseases
- TyG-WHtR:
-
Triglyceride glucose-waist height ratio
- CHARLS:
-
China Health and Retirement Longitudinal Study
- RCS:
-
Restricted cubic spline
- SD:
-
Standard deviation
- IQR:
-
Interquartile range
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- HbA1c:
-
Glycosylated hemoglobin
References
Mensah GA, Fuster V, Roth GA. A heart-healthy and stroke-free world: using data to inform global action. J Am Coll Cardiol. 2023;82(25):2343–9.
Abbasian M, Adderley NJ, Agasthi P, et al. Global Burden of Cardiovascular Diseases and Risks, 1990–2022. J Am Coll Cardiol. 2023;82(25):2350–473.
Tao LC, Xu JN, Wang TT, Hua F, Li JJ. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc Diabetol. 2022;21(1):68.
Laakso M, Kuusisto J. Insulin resistance and hyperglycaemia in cardiovascular disease development. Nat Rev Endocrinol. 2014;10(5):293–302.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, et al. The product of triglycerides and glucose a simple measure of insulin sensitivity comparison with the euglycemic hyperinsulinemic clamp. J Clini Endocrinol Metab. 2010;95:3347–51.
Sánchez Íñigo L, Navarro González D, Fernández Montero A, Pastrana Delgado J, Martínez JA. The TyG index may predict the development of cardiovascular events. Eur J Clin Invest. 2016;46(2):189–97.
Cui H, Liu Q, Wu Y, Cao L. Cumulative triglyceride-glucose index is a risk for CVD: a prospective cohort study. Cardiovasc Diabetol. 2022;21(1):22.
Wu Z, Liu L, Wang W, et al. Triglyceride-glucose index in the prediction of adverse cardiovascular events in patients with premature coronary artery disease: a retrospective cohort study. Cardiovasc Diabetol. 2022;21(1):142.
Zhang Q, Xiao S, Jiao X, Shen Y. The triglyceride-glucose index is a predictor for cardiovascular and all-cause mortality in CVD patients with diabetes or pre-diabetes: evidence from NHANES 2001–2018. Cardiovasc Diabetol. 2023;22(1):1–279.
Lopez-Jimenez F, Almahmeed W, Bays H, et al. Obesity and cardiovascular disease: mechanistic insights and management strategies a joint position paper by the world heart federation and world obesity federation. Eur J Prev Cardiol. 2022;29(17):2218–37.
Dang K, Wang X, Hu J, et al. The association between triglyceride-glucose index and its combination with obesity indicators and cardiovascular disease: NHANES 2003–2018. Cardiovasc Diabetol. 2024;23(1):8.
Er L, Wu S, Chou H, et al. Triglyceride Glucose-Body Mass Index Is a Simple and Clinically Useful Surrogate Marker for Insulin Resistance in Nondiabetic Individuals. PLoS ONE. 2016;11(3): e0149731.
Xia X, Chen S, Tian X, et al. Association of triglyceride-glucose index and its related parameters with atherosclerotic cardiovascular disease: evidence from a 15-year follow-up of Kailuan cohort. Cardiovasc Diabetol. 2024;23(1):208.
Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: The China health and retirement longitudinal study (CHARLS). Int J Epidemiol. 2014;43(1):61–8.
Huo R, Zhai L, Liao Q, You X. Changes in the triglyceride glucose-body mass index estimate the risk of stroke in middle-aged and older Chinese adults: a nationwide prospective cohort study. Cardiovasc Diabetol. 2023;2(1):28.
He D, Wang Z, Li J, et al. Changes in frailty and incident cardiovascular disease in three prospective cohorts. Eur Heart J. 2024;23(1):28.
Cheng Y, Fang Z, Zhang X, et al. Association between triglyceride glucose-body mass index and cardiovascular outcomes in patients undergoing percutaneous coronary intervention: a retrospective study. Cardiovasc Diabetol. 2023;22(1):75.
Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. 2012;13(3):275–86.
Ashwell M, Gibson S. Waist-to-height ratio as an indicator of ‘early health risk’: simpler and more predictive than using a ‘matrix’ based on BMI and waist circumference. BMJ Open. 2016;6(3): e010159.
Butt JH, Petrie MC, Jhund PS, et al. Anthropometric measures and adverse outcomes in heart failure with reduced ejection fraction: revisiting the obesity paradox. Eur Heart J. 2023;44(13):1136–53.
Vasques ACJ, Novaes FS, de Oliveira MDS, et al. TyG index performs better than HOMA in a Brazilian population: a hyperglycemic clamp validated study. Diabetes Res Clin Pract. 2011;93(3):e98–100.
Bornfeldt KE, Tabas I. Insulin Resistance, Hyperglycemia, and Atherosclerosis. Cell Metab. 2011;14(5):575–85.
Adeva-Andany MM, Martínez-Rodríguez J, González-Lucán M, Fernández-Fernández C, Castro-Quintela E. Insulin resistance is a cardiovascular risk factor in humans. Diabetes Metab Syndr. 2019;13(2):1449–55.
Feng Q, Bešević J, Conroy M, et al. Waist-to-height ratio and body fat percentage as risk factors for ischemic cardiovascular disease: a prospective cohort study from UK Biobank. Am J Clin Nutr. 2024;119(6):1386–96.
Raele R, Lotufo PA, Bittencourt MS, et al. The association of waist-to-height ratio and other anthropometric measurements with subclinical atherosclerosis: Results from the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Nutr Metab Cardiovasc Dis. 2020;30(11):1989–98.
Fuster JJ, Ouchi N, Gokce N, Walsh K. Obesity-induced changes in adipose tissue microenvironment and their impact on cardiovascular disease. Circ Res. 2016;118(11):1786–807.
Wong CW, Kwok CS, Narain A, et al. Marital status and risk of cardiovascular diseases: a systematic review and meta-analysis. Heart (British Cardiac Society). 2018;104(23):1937–48.
Chen R, Zhan Y, Pedersen N, et al. Marital status, telomere length and cardiovascular disease risk in a Swedish prospective cohort. Heart. 2020;106(4):267–72.
Glymour MM, Avendano M. Can self-reported strokes be used to study stroke incidence and risk factors? Stroke. 2009;40(3):873–9.
Xie W, Zheng F, Yan L, Zhong B. Cognitive decline before and after incident coronary events. J Am Coll Cardiol. 2019;73(24):3041–50.
Acknowledgements
The authors thank the National School of Development of Peking University and the Chinese Social Science Survey Center of Peking University for providing CHARLS data.
Funding
This work was supported by the National Key R&D Program of China (2023YFC2706200), National Science Foundation of China (82370271,82070297), National Key Research and Development Program of Guangzhou (202103000014).
Author information
Authors and Affiliations
Contributions
QR, YH and QL conceived the study. QR and CT prepared and analyzed the data. GL carried out literature search. QR, YH and QL drafted the manuscript. ZW revised the manuscript. All authors have approved the final draft of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The CHARLS study was performed in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Peking University. All participants provided written informed consent before participating in the CHARLS study.
Competing interests
The authors declare no potential competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary lnformation
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ren, Q., Huang, Y., Liu, Q. et al. Association between triglyceride glucose-waist height ratio index and cardiovascular disease in middle-aged and older Chinese individuals: a nationwide cohort study. Cardiovasc Diabetol 23, 247 (2024). https://doi.org/10.1186/s12933-024-02336-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-024-02336-6