
Abstract
Background and objectives
Evidence on the associations between baseline stromal cell-derived factor (SDF)-1 and clinical outcomes in acute ischemic stroke patients is lacking. The present study aimed to examine the relationship between plasma SDF-1 levels and clinical outcomes based on a large multicenter study of the China Antihypertensive Trial in Acute Ischemic Stroke (CATIS).
Methods
Secondary analysis was conducted among 3,255 participants from the CATIS trial with a baseline measurement of plasma SDF-1 levels. We evaluated the associations between plasma SDF-1 levels and one-year recurrent stroke, cardiovascular events, and all-cause mortality using Cox regression models. We further investigated the prognostic effect of SDF-1 on clinical outcomes in patients with different characteristics.
Results
Higher plasma SDF-1 levels were not associated with recurrent stroke, cardiovascular events, and all-cause mortality at one-year after ischemic stroke (all P trend ≥ 0.05). There were significant interactions between plasma SDF-1 levels and history of diabetes mellitus on recurrent stroke (P = 0.005), cardiovascular events (P = 0.007) and all-cause mortality (P = 0.04) at one year. In patients with diabetes mellitus, plasma SDF-1 was significantly associated with an increased risk of recurrent stroke and cardiovascular events after adjustment for confounders. For example, 1-SD higher log–SDF-1 was associated with a hazard ratio (95% confidence interval) of 1.65 (1.18–2.32) for recurrent stroke and 1.47 (1.08–1.99) for the cardiovascular events, but not all-cause mortality 1.36 (0.96–1.93) at one year. However, there were no associations between plasma SDF-1 and clinical outcomes in patients without diabetes mellitus (all P > 0.05). The addition of plasma SDF-1 to the conventional risk factors model significantly improved the risk prediction of all outcomes. Similarly, findings between elevated SDF-1 levels and two-year outcomes were found only in patients with diabetes mellitus.
Conclusions
Elevated plasma SDF-1 was significantly associated with an increased risk of recurrent stroke and cardiovascular events only in ischemic patients with diabetes mellitus.
Similar content being viewed by others


Introduction
Identifying novel biomarkers of recurrent stroke and cardiovascular events after stroke could increase our understanding of its pathogenesis and suggest novel therapeutic targets. The stromal cell-derived factor (SDF)-1, also known as CXC chemokine ligand-12 (CXCL-12), is a member of the CXC chemokine subfamily and regulates cellular activity by binding to CXC chemokine receptor 4 (CXCR4) or CXCR7 [1,2,3].
Experimental studies indicated that increased SDF-1 could induce neointimal hyperplasia and angiogenesis, triggers vascular inflammatory response, aggravates insulin resistance, and is associated with atherosclerosis and cardiovascular events [1,2,3,4,5,6,7]. Several population studies have proven the positive association of serum SDF-1 with the risk of cardiovascular disease, including ischemic stroke [1, 4,5,6,7]. Moreover, some studies also indicated that a high level of serum SDF-1 was associated with an increased risk of poor functional outcome and animal studies reported that the SDF-1 antagonist AMD3100 significantly improved functional recovery after stroke [8,9,10]. However, epidemiological evidence with sufficient statistical power on the association between serum SDF-1 and recurrent stroke and cardiovascular events after acute ischemic stroke is limited [11].
Interestingly, several studies have noted a strong association between serum SDF-1 and diabetes mellitus [12,13,14,15]. These studies demonstrated that the levels of serum SDF-1 were increased in patients with diabetes mellitus, and increased SDF-1 can aggravate insulin resistance, and promote chronic inflammation and immune responses, which are the main mechanisms of diabetes mellitus progression and diabetes-associated cardiovascular events [12,13,14,15].
We hypothesized that having higher level of SDF-1 may be associated with an increased risk of recurrent stroke and cardiovascular events after ischemic stroke and the effect of SDF-1 on ischemic stroke prognosis may be different in patients with and without diabetes mellitus. To test this hypothesis, we conducted a prospective study to investigate the association between plasma SDF-1 levels and recurrent stroke, cardiovascular events, and all-cause mortality in ischemic stroke patients based on a large prospective multicenter study of the China Antihypertensive Trial in Acute Ischemic Stroke (CATIS).
Methods
Study participants
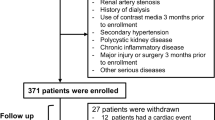
The present study is a secondary analysis of the CATIS trial, a multicenter, single-blind, blinded endpoints, randomized clinical trial conducted in 26 hospitals across China from August 2009 to May 2013, and the purpose of CATIS was to evaluate whether immediate blood pressure (BP) reduction in patients with acute ischemic stroke could reduce death and major disability at 14 days or hospital discharge [16]. The CATIS trial was registered on clinicaltrials.gov (NCT01840072). Details of the rationale, design, and major results of CATIS had been reported previously. Briefly, 4071 patients aged ≥ 22 years with a first-ever ischemic stroke, confirmed by computed tomography or magnetic resonance imaging of the brain within 48 h of symptom onset, and with elevated systolic blood pressure (BP) between 140 to < 220 mmHg were recruited. Patients with a BP ≥ 220/120 mmHg, severe heart failure, acute myocardial infarction or unstable angina, atrial fibrillation, aortic dissection, severe cerebrovascular stenosis (≥ 70%), or resistant hypertension, in a deep coma, or treated with intravenous thrombolytic therapy were excluded from the CATIS trial [16]. Patients were randomly assigned to receive antihypertensive treatment (aimed at lowering systolic blood pressure by 10–25% within the first 24 h after randomization, achieving blood pressure less than 140/90 mm Hg within seven days, and maintaining this level during hospitalization) or to discontinue all antihypertensive medications (control) during hospitalization.
The current study excluded 632 patients without available blood samples for plasma SDF-1 measurements and 184 patients lost to follow-up. Finally, 3,255 ischemic stroke patients from CATIS were included for analysis (Supplementary Fig. 1).
Data collection
Baseline data on demographic characteristics, lifestyle risk factors, medical history, and medication use history were collected upon hospital admission using a standard questionnaire. Information on baseline characteristics was obtained through face-to-face interviews with trained interviewers. Stroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS) by trained neurologists at admission. Ischemic stroke was classified as large-artery atherosclerosis (embolus/thrombosis), cardiac embolism (embolic), and small-artery occlusion (lacunar) according to the symptoms and imaging data of the patients. Three blood pressure (BP) measurements were also obtained at admission by trained nurses using a standard mercury sphygmomanometer according to a standard protocol adapted from procedures recommended by the American Heart Association [17]. Additionally, serum lipids, plasma glucose, and other clinical laboratory measurements were obtained at the participating hospitals at admission.
Blood samples were collected after at least eight hours of fasting within 24 h of hospital admission. Plasma samples were separated at the clinical laboratories of the participating hospitals and immediately frozen at − 80 °C. Plasma SDF-1 concentrations were measured centrally in the Central Laboratory of the School of Public Health at Soochow University with a commercially available ELISA kit (Catalog: DY350; R&D Systems, Minneapolis, Minnesota). Intra- and inter-assay coefficients of variation were 5.8% and 8.6%, respectively. Laboratory technicians who measured plasma SDF-1 levels were blinded to baseline characteristics and study clinical outcomes of participants.
Study outcomes
Participants were followed up in person two years after stroke onset by trained neurologists and research nurses blinded to treatment assignment. The primary outcome was a recurrent stroke one year after stroke onset. The secondary outcomes were: (1) composite of cardiovascular events after ischemic stroke, including vascular death, nonfatal stroke, nonfatal myocardial infarction, angina hospitalization, congestive heart failure hospitalization, peripheral arterial disease at one year; (2) all-cause mortality at one year after stroke onset. Death certificates were obtained for deceased participants, and hospital data were abstracted for all vascular events. The study outcomes assessment committee blinded to treatment assignment reviewed and adjudicated outcomes based on the criteria established in the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial.
Statistical analysis
We grouped all study participants by quartiles of plasma SDF-1 levels. Cox proportional hazards models were used to assess the associations between plasma SDF-1 and recurrent stroke, cardiovascular events, and all-cause mortality in all study participants and key subgroups by age (≥ 62 vs. <62 years), sex, current smoking, alcohol consumption, baseline NIHSS score, history of hypertension, randomization treatment and history of diabetes mellitus. The interaction between subgroup valuables and SDF-1 on study outcome was tested by the likelihood ratio test of models with interaction terms, adjusting for the covariates.
In the subgroup analysis, we found significant interactions between plasma SDF-1 levels and the status of diabetes mellitus on the study outcomes at one year. Then, the participants were divided into two subgroups according to diabetes mellitus status. In each subgroup, the participants were further divided into four groups by quartiles of plasma SDF-1 levels. Baseline characteristics were compared and tested for trends across the SDF-1 quartiles using a generalized linear model in patients with and without diabetes mellitus. The associations between plasma SDF-1 and recurrent stroke, cardiovascular events, and all-cause mortality were assessed using Cox proportional hazards models in patients with and without diabetes. The covariates included in the multivariable models were selected based on prior knowledge, including age, sex, current smoking, alcohol consumption, estimated glomerular filtration rate (eGFR), baseline NIHSS score, medical history (hypertension, hyperlipidemia), ischemic stroke subtype, and randomized treatment. The proportional hazards assumption of the Cox models was tested using Schoenfeld residuals, which showed no significant departure from proportionality (P > 0.05). Hazard ratios (HRs) and 95% confidence intervals (CIs) for SDF-1 quartiles and per one standard deviation (SD) increment of log-transformed plasma SDF-1 levels were calculated. Tests for linear trends in HRs across plasma SDF-1 quartiles were conducted using the median value of each quartile as the predictor. In addition, restricted cubic splines were used to generate more precise estimates and to assess the shape of associations between SDF-1 and clinical outcomes (with four knots at the 5th, 35th, 65th, and 95th percentiles) [18]. The Fine-Gray model was performed as a sensitivity analysis to robustly assess the association between SDF-1 levels and recurrent stroke and cardiovascular events (excluding vascular death) by regarding death as a competing risk [19].
We further assessed the predictive performance of plasma SDF-1 for clinical outcomes in the basic model with conventional risk factors. The Hosmer Lemeshow χ2 statistic was first conducted to evaluate the calibration of models with SDF-1. Furthermore, the net reclassification index (NRI) and integrated discrimination improvement (IDI) were used for assessing improvements in risk reclassification when adding plasma SDF-1 to the conventional model [20, 21]. Multiple imputations for missing covariate values were performed using the Markov chain Monte Carlo method. To assess the robustness of the predicted effect of plasma SDF-1 after stroke, we also analyzed the association between plasma SDF-1 levels and recurrent stroke, cardiovascular events, and all-cause mortality at two years as sensitivity analysis. All P values were 2-tailed, and a significance level of 0.05 was used. Statistical analysis was conducted using SAS statistical software (version 9.2, Cary, North Carolina, USA).
Results
Baseline characteristics
A total of 3,255 ischemic stroke patients (mean [SD] age 61.9 [10.8] years, 2103 [64.6%] male) were included in the present analyses. The median plasma SDF-1 concentration was 639.4 pg/mL (interquartile range 436.9-855.3 pg/mL). The level of plasma SDF-1 in patients with diabetes mellitus was lower than in those without diabetes mellitus (624.5 pg/mL vs. 673.7 pg/mL). The baseline characteristics of participants with and without diabetes mellitus are shown in Supplementary Table 1. Compared with participants without diabetes mellitus, patients with diabetes mellitus were less often male, smokers, and drinkers, had lower diastolic BP, higher levels of triglycerides, total cholesterol, low-density lipoprotein cholesterol and fasting plasma glucose and lower levels of high-density lipoprotein cholesterol. Patients with diabetes mellitus also had a greater frequency of history of hypertension, hyperlipidemia, and coronary heart disease, prior antihypertensive and lipid-lowing treatment. The frequency of recurrent stroke, cardiovascular events, and all-cause mortality in patients with diabetes mellitus was higher than those without diabetes mellitus, although no statistically significant difference was observed between the two groups (Supplementary Table 2).
Among 567 patients with diabetes mellitus, compared with participants with lower plasma SDF-1 levels, those with higher SDF-1 were older, had lower levels of eGFR, more likely with lacunar stroke, and less likely with thrombosis (Table 1). In 2688 patients without diabetes mellitus, compared with participants with lower plasma SDF-1 levels, those with higher SDF-1 were older and female, non-smoking, non-alcohol drinking, and more likely to have a lacunar stroke and less likely to have thrombosis. Patients with higher SDF-1 levels also had lower levels of total cholesterol, eGFR and a longer time from onset to hospitalization (Table 1).
Plasma SDF-1 levels and clinical outcomes after acute ischemic stroke
During one year of follow-up, there were 150 recurrent strokes (4.6%), 196 cardiovascular events (6.0%), and 204 all-cause mortalities (6.3%) in the whole population. We found that plasma SDF-1 levels were not associated with recurrent stroke, cardiovascular events, and all-cause mortality one year after stroke onset Supplementary Table 3). There were significant interactions between plasma SDF-1 levels and history of diabetes mellitus on recurrent stroke (P = 0.005 for interaction), cardiovascular events (P = 0.007 for interaction) and, all-cause mortality (P = 0.04 for interaction) at one year. However, no significant interaction between plasm SDF-1 and age, sex, current smoking, alcohol consumption, baseline NIHSS score, history of hypertension, and randomization treatment on outcomes were observed (all P for interaction > 0.05).
In 567 patients with diabetes mellitus, during one year of follow-up, there were 30 recurrent strokes (5.3%), 42 cardiovascular events (7.4%), and 40 all-cause mortalities (7.1%). Compared to those with the lowest quartile of plasma SDF-1 levels, patients with the highest SDF-1 levels had a higher risk HRs (95% CIs) of recurrent stroke [4.12 (1.31–12.95)], cardiovascular events [2.80 (1.11–7.06)] but not all-cause mortality [2.09 (0.86–5.09)] at one year after adjustment for age, sex, medical history, and other covariates (Table 2). Each 1-SD increase in log-transformed SDF-1 levels was associated with a 65% increased risk (HR 1.65, 95% CI 1.18–2.32) of recurrent stroke and a 47% increased risk (HR 1.47, 95% CI 1.08–1.99) of cardiovascular events at one year after stroke (Table 2). There were 120 recurrent strokes (4.5%), 154 cardiovascular events (5.7%), and 164 all-cause mortalities (6.1%) at one year in non-diabetic patients. Patients with the highest SDF-1 levels did not have an increased risk of recurrent stroke [0.95 (0.58–1.55)], cardiovascular events [0.71 (0.45–1.12)] and all-cause mortality [0.84 (0.53–1.33)] at one year in compared to those with the lowest quartile of plasma SDF-1 levels (Table 2). In a competing risk analysis, the associations of recurrent stroke and cardiovascular events (excluding vascular death) with increased SDF-1 levels in patients with diabetes mellitus at one year were still significant treating death as a competing risk (Supplementary Table 4).
Similarly, elevated SDF-1 levels were associated with two-year recurrent stroke and cardiovascular events only in patients with diabetes mellitus, but not those without diabetes mellitus (Supplementary Table 5).
Multivariable-adjusted spline regression models showed a linear association between SDF-1 levels and recurrent stroke (Fig. 1A, P for linearity = 0.005), cardiovascular events (Fig. 1C, P for linearity = 0.02), but not all-cause mortality (Fig. 1E, P for linearity = 0.09) at one year in patients with diabetes mellitus (Fig. 1). However, no significant associations between plasma SDF-1 levels and recurrent stroke (Fig. 1B, P for linearity = 0.49), cardiovascular events (Fig. 1D, P for linearity = 0.11), all-cause mortality (Fig. 1F, P for linearity = 0.34) were detected in patients without diabetes mellitus at one year.

Relationships of SDF-1 with recurrent stroke, cardiovascular events and all-cause mortality in patients with ischemic stroke
Hazards ratios and 95% confidence intervals derived from restricted cubic spline regression, with knots placed at the 5th, 35th, 65th, and 95th percentiles of the SDF-1 levels distribution. The reference point is the midpoint of the reference group for the categorical analysis. Hazard ratios were adjusted for the same variables as Model 3. Panel A: Recurrent Stroke at 1 year in ischemic stroke with diabetes (P for linearity = 0.005); Panel B: Recurrent Stroke at 1 year in ischemic stroke without diabetes (P for linearity = 0.49); Panel C: Cardiovascular events at 1 year in ischemic stroke with diabetes (P for linearity = 0.02). Panel D: Cardiovascular events at 1 year in ischemic stroke without diabetes (P for linearity = 0.11). Panel E: All-cause mortality at 1 year in ischemic stroke with diabetes (P for linearity = 0.09). Panel F: All-cause mortality at 1 year in ischemic stroke without diabetes (P for linearity = 0.34)
Predictive performance of plasma SDF-1 levels in patients with and without diabetes mellitus
We assessed the predictive value of plasma SDF-1 beyond conventional factors for recurrent stroke, cardiovascular events, and all-cause mortality. In patients with diabetes mellitus, the Hosmer Lemeshow test indicated that model calibration was adequate after adding plasma SDF-1. Furthermore, we found that the addition of plasma SDF-1 to the basic model containing conventional risk factors also significantly improved risk reclassification for recurrent stroke (NRI: 51.77%, P = 0.006; IDI: 1.74%, P = 0.005), cardiovascular events (NRI: 42.29%, P = 0.008; IDI: 1.39%, P = 0.01), and all-cause mortality (NRI: 33.03%, P = 0.04; IDI: 0.69%, P = 0.36) at one year after stroke (Table 3). However, plasma SDF-1 did not show significance for predicting recurrent stroke, cardiovascular events, and all-cause mortality in patients without diabetes mellitus (Table 3).
Discussion
This prospective analysis of ischemic stroke patients from the CATIS trial dataset demonstrates that higher plasma SDF-1 levels were not associated with recurrent stroke and cardiovascular events after ischemic stroke. However, we found a significant modifying role of diabetes mellitus on the association between increased plasma SDF-1 levels and poor prognosis after ischemic stroke. Our findings indicated that higher plasma SDF-1 levels were associated with increased risks of recurrent stroke and cardiovascular events within one year after ischemic stroke only in the patients with diabetes mellitus. However, no evidence of an association between plasma SDF-1 levels and clinical outcomes was found after ischemic stroke in those without diabetes mellitus.
Previous experimental studies had reported that SDF-1 activated various biological signaling pathways including atherosclerosis and inflammatory response by binding to its receptor [1, 22,23,24]. Several population studies indicated elevated serum SDF-1 levels were significantly associated with an increased risk of myocardial infarction and coronary artery disease [4,5,6, 25]. Data from the Chronic Renal Insufficiency Cohort (CRIC) Study of 3687 chronic kidney disease patients found that higher plasma SDF-1 was associated with the hazard of incident myocardial infarction and death [6]. Regarding ischemic stroke, most studies suggested that elevated serum SDF-1 was related to poor functional outcomes [8, 9, 26]. For example, a study of 304 acute ischemic stroke patients indicated that having a high level of SDF-1 (≥ 12.4 ng/mL) was an independent predictor of poor functional outcome and mortality at six months after stroke [8]. To date, one study has examined the association of SDF-1 levels with recurrent stroke. This study involved 248 patients with first-ever ischemic stroke and found an association between higher baseline serum SDF-1 levels and the risk of recurrent stroke within one year [11]. The present analysis with more than 3000 acute ischemic stroke patients showed that having elevated SDF-1 levels at baseline was not associated with an increased risk of recurrent stroke as well as cardiovascular events after ischemic stroke. The discrepant prognostic effect of SDF-1 on recurrent stroke in patients with acute ischemic stroke may largely be attributed to variations in sample size and baseline characteristics.
A growing body of evidence suggested that increased SDF-1 was strongly related to diabetes mellitus and its complications. A study of 200 patients with diabetes mellitus found that the level of SDF-1 is higher than healthy controls [12]. Several basic and clinical studies indicated that elevated level of SDF-1 was reported to contribute to diabetes complications by promoting the expression of inflammatory cytokines and immune-related disorders exacerbating insulin resistance [13,14,15, 27]. Moreover, inhibited expression of SDF-1 was reported to have the effect of reversing diabetic complications [28]. Additionally, a recent experimental study demonstrated that SDF-1 impaired cardiac contractility in aged, obese, and diabetic mice, but not in mice without diabetes [29]. Considering the existing evidence, we hypothesize that diabetes mellitus may modify the prognostic value of SDF-1 in ischemic stroke patients. The present study found an interaction between plasma SDF-1 levels and a history of diabetes mellitus on recurrent stroke, cardiovascular events, and all-cause mortality. In patients with diabetes mellitus, baseline plasma SDF-1 levels were significantly associated with an increased risk of recurrent stroke and cardiovascular events at one year. Moreover, the predictive effect of SDF-1 and clinical outcomes were improved after the addition of plasma SDF-1 to the basic model containing conventional risk factors. However, no associations between plasma SDF-1 levels and clinical outcomes in those without diabetes mellitus were found. Additionally, our findings revealed that having higher plasma SDF-1 levels were associated with an increased risk of recurrent stroke and cardiovascular events at two years in patients with diabetes mellitus, although this association was not as strong as observed for outcomes at one year. The underlying reason for the predictive effect of plasma SDF-1 on outcomes at two years being less robust than at one year remains unclear and needs further studies to confirm.
Our study has important clinical implications for firstly demonstrating that the status of diabetes mellitus affects the prognostic effect of plasma SDF-1 on outcomes after acute stroke. Our findings provide evidence that inflammation by diabetes mellitus may be the underlying mechanize contributing to diabetic associated cardiovascular events and help to better understand the pathogenesis of stroke progression in patients with diabetes mellitus. The findings suggested that SDF-1 could be a potential therapeutic target in acute stroke patients with diabetes mellitus in future studies and the use of SDF-1 inhibitors in medical treatment shows promise as a potential therapeutic intervention for secondary prevention following an ischemic stroke with diabetes mellitus.
The exact mechanisms underlying the relationship between higher plasma SDF-1 levels and increased risk of recurrent stroke and cardiovascular events in acute ischemic stroke patients with diabetes mellitus are unclear. Several hypotheses have been proposed. First, a growing body of evidence suggested that increased plasma SDF-1 levels can promote insulin resistance and diabetic kidney disease [12,13,14, 27], which were reported to be significantly associated with recurrent stroke and poor functional outcomes after ischemic stroke [30, 31]. Second, increased SDF-1 through mediate Ca2+ flux affects cardiac contractility in diabetes mice [29], which is associated with heart failure, cardiovascular events, and recurrent stroke.
The strengths of these analyses included the large sample size from the multicenter of the CATIS trial with standardized protocols and strict quality control procedures in baseline data collection and outcome assessment. Moreover, multiple established cardiovascular risk factors were collected and controlled in the multivariable models. However, there are also several limitations. First, the present study is derived from the CATIS trial, thus selection bias might be unavoidable. The patients with BP ≥ 220/120 mmHg or other serious conditions such as severe heart failure, acute myocardial infarction or unstable angina, atrial fibrillation, aortic dissection, or resistant hypertension at admission were excluded, so these findings cannot be generalized to these patients. Second, the possibility of residual confounding cannot be fully eliminated in an observational study, although several important potential confounders have been controlled for in multivariable-adjusted models. Third, plasma SDF-1 levels were measured only at the acute stage, and we could not evaluate the dynamic change of SDF-1 on the clinical outcomes after acute ischemic stroke.
In conclusion, we found a modifying role of diabetes mellitus on the association between baseline plasma SDF-1 levels and clinical outcomes. Elevated plasma SDF-1 was significantly associated with an increased risk of recurrent stroke and cardiovascular events at one year only in ischemic stroke patients with diabetes mellitus, but not in those without diabetes mellitus. Future studies from other populations are needed to verify our findings and clarify the potential mechanisms.
Data Availability
The datasets used and analyzed in the current study are available from the corresponding author upon reasonable request.
Abbreviations
- BP:
-
blood pressure
- BMI:
-
body mass index
- CATIS:
-
China Antihypertensive Trial in Acute Ischemic Stroke
- CIs:
-
confidence intervals
- CXCL12:
-
CXC chemokine ligand-12
- CXCR4/7:
-
CXC chemokine receptor 4/7
- HRs:
-
Hazard ratios
- IDI:
-
integrated discrimination improvement
- NRI:
-
net reclassification improvement
- NIHSS:
-
National Institutes of Health Stroke Scale
- SDF-1:
-
stromal cell-derived factor-1
References
Yamaguchi J, Kusano KF, Masuo O, Kawamoto A, Silver M, Murasawa S, Bosch-Marce M, Masuda H, Losordo DW, Isner JM, et al. Stromal cell-derived factor-1 effects on ex vivo expanded endothelial progenitor cell recruitment for ischemic neovascularization. Circulation. 2003;107(9):1322–8.
D’Apuzzo M, Rolink A, Loetscher M, Hoxie JA, Clark-Lewis I, Melchers F, Baggiolini M, Moser B. The chemokine SDF-1, stromal cell-derived factor 1, attracts early stage B cell precursors via the chemokine receptor CXCR4. Eur J Immunol. 1997;27(7):1788–93.
Gao JH, Yu XH, Tang CK. CXC chemokine ligand 12 (CXCL12) in atherosclerosis: an underlying therapeutic target. Clin Chim Acta. 2019;495:538–44.
Rath D, Chatterjee M, Borst O, Müller K, Stellos K, Mack AF, Bongartz A, Bigalke B, Langer H, Schwab M, et al. Expression of stromal cell-derived factor-1 receptors CXCR4 and CXCR7 on circulating platelets of patients with acute coronary syndrome and association with left ventricular functional recovery. Eur Heart J. 2014;35(6):386–94.
Sjaarda J, Gerstein H, Chong M, Yusuf S, Meyre D, Anand SS, Hess S, Paré G. Blood CSF1 and CXCL12 as Causal Mediators of Coronary Artery Disease. J Am Coll Cardiol. 2018;72(3):300–10.
Mehta NN, Matthews GJ, Krishnamoorthy P, Shah R, McLaughlin C, Patel P, Budoff M, Chen J, Wolman M, Go A, et al. Higher plasma CXCL12 levels predict incident myocardial infarction and death in chronic kidney disease: findings from the chronic renal insufficiency cohort study. Eur Heart J. 2014;35(31):2115–22.
Schutt RC, Burdick MD, Strieter RM, Mehrad B, Keeley EC. Plasma CXCL12 levels as a predictor of future stroke. Stroke. 2012;43(12):3382–6.
Cheng X, Lian YJ, Ma YQ, Xie NC, Wu CJ. Elevated serum levels of CXC chemokine Ligand-12 are Associated with unfavorable functional outcome and mortality at 6-Month follow-up in chinese patients with Acute ischemic stroke. Mol Neurobiol. 2017;54(2):895–903.
Huang X, Wan M, Yang Q, Ding X, Zhou Z. The stromal cell-derived factor-1 α (SDF-1α)/cysteine-X-cysteine chemokine receptor 4 (CXCR4) axis: a possible prognostic indicator of acute ischemic stroke. J Int Med Res. 2019;47(5):1897–907.
Ruscher K, Kuric E, Liu Y, Walter HL, Issazadeh-Navikas S, Englund E, Wieloch T. Inhibition of CXCL12 signaling attenuates the postischemic immune response and improves functional recovery after stroke. J Cereb Blood Flow Metab. 2013;33(8):1225–34.
Gu XL, Liu L, Lu XD, Liu ZR. Serum CXCL12 levels as a novel predictor of future stroke recurrence in patients with Acute ischemic stroke. Mol Neurobiol. 2016;53(5):2807–14.
Derakhshan R, Arababadi MK, Ahmadi Z, Karimabad MN, Salehabadi VA, Abedinzadeh M, Khorramdelazad H, Balaei P, Kennedy D, Hassanshahi G. Increased circulating levels of SDF-1 (CXCL12) in type 2 diabetic patients are correlated to disease state but are unrelated to polymorphism of the SDF-1β gene in the iranian population. Inflammation. 2012;35(3):900–4.
Kim D, Kim J, Yoon JH, Ghim J, Yea K, Song P, Park S, Lee A, Hong CP, Jang MS, et al. CXCL12 secreted from adipose tissue recruits macrophages and induces insulin resistance in mice. Diabetologia. 2014;57(7):1456–65.
Xu H, Barnes GT, Yang Q, Tan G, Yang D, Chou CJ, Sole J, Nichols A, Ross JS, Tartaglia LA, et al. Chronic inflammation in fat plays a crucial role in the development of obesity-related insulin resistance. J Clin Invest. 2003;112(12):1821–30.
Karimabad MN, Hassanshahi G. Significance of CXCL12 in type 2 diabetes mellitus and its associated complications. Inflammation. 2015;38(2):710–7.
He J, Zhang Y, Xu T, Zhao Q, Wang D, Chen CS, Tong W, Liu C, Xu T, Ju Z, et al. Effects of immediate blood pressure reduction on death and major disability in patients with acute ischemic stroke: the CATIS randomized clinical trial. JAMA. 2014;311(5):479–89.
Kurtz TW, Griffin KA, Bidani AK, Davisson RL, Hall JE, AHA Council on High Blood Pressure Research, Professional and Public Education Subcommittee. Recommendations for blood pressure measurement in animals: summary of an AHA scientific statement from the Council on high blood pressure research, Professional and Public Education Subcommittee. Arterioscler Thromb Vasc Biol. 2005;25(3):478–9.
Durrleman S, Simon R, Durrleman S, Simon R. Flexible regression models with cubic splines. Stat Med 8, 551–561. Stat Med. 1989;8(5):551 – 61.
Barrowman MA, Peek N, Lambie M, Martin GP, Sperrin M. How unmeasured confounding in a competing risks setting can affect treatment effect estimates in observational studies. BMC Med Res Methodol. 2019;19(1):166.
Pencina MJ, D’Agostino RB, Sr, Agostino RB Jr, Vasan RS. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med. 2008;27(2):157–72. discussion 207 – 12.
Pickering JW, Endre ZH. New metrics for assessing diagnostic potential of candidate biomarkers. Clin J Am Soc Nephrol. 2012;7(8):1355–64.
Schober A, Hristov M, Kofler S, Forbrig R, Löhr B, Heussen N, Zhe Z, Akhtar S, Schumann U, Krötz F, et al. CD34 + CD140b + cells and circulating CXCL12 correlate with the angiographically assessed severity of cardiac allograft vasculopathy. Eur Heart J. 2011;32(4):476–84.
Deshane J, Chen S, Caballero S, Grochot-Przeczek A, Was H, Li Calzi S, Lach R, Hock TD, Chen B, Hill-Kapturczak N, et al. Stromal cell-derived factor 1 promotes angiogenesis via a heme oxygenase 1-dependent mechanism. J Exp Med. 2007;204(3):605–18.
Döring Y, van der Vorst EPC, Duchene J, Jansen Y, Gencer S, Bidzhekov K, Atzler D, Santovito D, Rader DJ, Saleheen D, et al. CXCL12 derived from endothelial cells promotes atherosclerosis to Drive Coronary Artery Disease. Circulation. 2019;139(10):1338–40.
Ghasemzadeh N, Hritani AW, De Staercke C, Eapen DJ, Veledar E, Al Kassem H, Khayata M, Zafari AM, Sperling L, Hooper C, et al. Plasma stromal cell-derived factor 1α/CXCL12 level predicts long-term adverse cardiovascular outcomes in patients with coronary artery disease. Atherosclerosis. 2015;238(1):113–8.
Duan XX, Zhang GP, Wang XB, Yu H, Wu JL, Liu KZ, Wang L, Long X. The diagnostic and prognostic value of serum CXCL12 levels in patients with ischemic stroke. Neurol Sci. 2015;36(12):2227–34.
Sayyed SG, Hägele H, Kulkarni OP, Endlich K, Segerer S, Eulberg D, Klussmann S, Anders HJ. Podocytes produce homeostatic chemokine stromal cell-derived factor-1/CXCL12, which contributes to glomerulosclerosis, podocyte loss and albuminuria in a mouse model of type 2 diabetes. Diabetologia. 2009;52(11):2445–54.
Darisipudi MN, Kulkarni OP, Sayyed SG, Ryu M, Migliorini A, Sagrinati C, Parente E, Vater A, Eulberg D, Klussmann S, et al. Dual blockade of the homeostatic chemokine CXCL12 and the proinflammatory chemokine CCL2 has additive protective effects on diabetic kidney disease. Am J Pathol. 2011;179(1):116–24.
Batchu SN, Thieme K, Zadeh FH, Alghamdi TA, Yerra VG, Hadden MJ, Majumder S, Kabir MG, Bowskill BB, Ladha D, et al. The Dipeptidyl peptidase 4 substrate CXCL12 has opposing Cardiac Effects in Young mice and aged Diabetic mice mediated by Ca2 + flux and phosphoinositide 3-Kinase γ. Diabetes. 2018;67(11):2443–55.
Ago T, Matsuo R, Hata J, Wakisaka Y, Kuroda J, Kitazono T, Kamouchi M. Fukuoka Stroke Registry Investigators. Insulin resistance and clinical outcomes after acute ischemic stroke. Neurology. 2018;90(17):e1470–7.
Hubbard D, Colantonio LD, Rosenson RS, Brown TM, Jackson EA, Huang L, Orroth KK, Reading S, Woodward M, Bittner V, et al. Risk for recurrent cardiovascular disease events among patients with diabetes and chronic kidney disease. Cardiovasc Diabetol. 2021;20(1):58.
Acknowledgements
We thank the study participants and their relatives, and the clinical staff for their support and contribution to this study.
Funding
This study was supported by the National Natural Science Foundation of China (grants: 82171296 and 82273706), and a Project of the Priority Academic Program Development of Jiangsu Higher Education Institutions, China; Discipline Construction Program of the Second Affiliated Hospital of Soochow University (XKTJ-XK202001and XKTJ-TD202004), Jiangsu Provincial Medical Key Discipline (ZDXK202217), Gusu Health Talents Program (GSWS2020029), and the 6th Jiangsu Province 333 High Level Talents Training Project.
Author information
Authors and Affiliations
Contributions
SJY, YJC, CKZ, CFL, JH and YHZ contributed to the concept and rationale for the study. SJY, HYC and CKZ were responsible for the first draft. CKZ, XYZ and HYC contributed statistical analyses. MYM, BZC, JGD, TX and XYZ performed the data collection. SJY, XYZ, YJC, and CKZ contributed discussion and edited manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The Institutional Review Boards or Ethical Committees approved the study at Soochow University in China, Tulane University in the US, and all participating hospitals. Written informed consent was obtained from all study participants or their immediate family members.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
You, S., Chen, H., Miao, M. et al. Prognostic significance of plasma SDF-1 in acute ischemic stroke patients with diabetes mellitus: the CATIS trial. Cardiovasc Diabetol 22, 274 (2023). https://doi.org/10.1186/s12933-023-01996-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-01996-0