
Abstract
Rationale
Bronchodilator responsiveness (BDR) is a common but variable phenomenon in COPD. The CT characteristics of airway dimensions that differentiate COPD subjects with BDR from those without BDR have not been well described. We aimed to assess airway dimensions in COPD subjects with and without BDR.
Methods
We analyzed subjects with GOLD 1–4 disease in the COPDGene® study who had CT airway analysis. We divided patients into two groups: BDR + (post bronchodilator ΔFEV1 ≥ 10%) and BDR-(post bronchodilator ΔFEV1 < 10%). The mean wall area percent (WA%) of six segmental bronchi in each subject was quantified using VIDA. Using 3D SLICER, airway wall thickness was also expressed as the square root wall area of an airway of 10 mm (Pi10) and 15 mm (Pi15) diameter. %Emphysema and %gas trapping were also calculated.
Results
2355 subjects in the BDR-group and 1306 in the BDR + group formed our analysis. The BDR + group had a greater Pi10, Pi15, and mean segmental WA% compared to the BDR-group. In multivariate logistic regression using gender, race, current smoking, history of asthma, %emphysema, %gas trapping, %predicted FEV1, and %predicted FVC, airway wall measures remained independent predictors of BDR. Using a threshold change in FEV1 ≥ 15% and FEV1 ≥ 12% and 200 mL to divide patients into groups, the results were similar.
Conclusion
BDR in COPD is independently associated with CT evidence of airway pathology. This study provides us with greater evidence of changes in lung structure that correlate with physiologic manifestations of airflow obstruction in COPD.
Similar content being viewed by others

Introduction
COPD is classically associated with irreversible or poorly reversible airflow obstruction [1], which helps to distinguish it from asthma. However, the concept that asthma and COPD have a similar pathogenesis was initially described by Orie et al. in 1961 [2]. This concept, known as the “Dutch Hypothesis,” sparked tremendous debate, with many researchers arguing that COPD and asthma are distinct entities [3],[4]. Nevertheless, bronchodilator responsiveness (BDR) is present in 54-83% of COPD patients [5]–[7]. To complicate matters, this phenomenon in COPD is not a consistent one; BDR is present on some occasions but not others during serial lung function testing of the same subject [7],[8]. BDR may have significant clinical importance in COPD; some studies showed that BDR is associated with a faster rate of lung function decline [9],[10], mortality [11],[12], and the development of airflow obstruction [13], whereas others have not [14].
It is currently unclear why some patients with COPD demonstrate BDR. A crucial pathologic feature of COPD is airway inflammation, which results in epithelial remodeling, smooth muscle hypertrophy, subepithelial fibrosis, and mucous cell metaplasia [15]. Several investigators have correlated airway remodeling and degree of airflow obstruction in COPD [16]–[18]. Similarly, airway wall thickness on CT scan correlates with degree of airflow obstruction in several studies [19]–[21]. However, CT correlates of BDR in COPD have not been well described.
Given that BDR is characteristic of asthma and that asthma airway pathology is dominated by smooth muscle hypertrophy, it is reasonable to hypothesize that COPD patients with BDR have a greater degree of airway smooth muscle mass, and therefore thicker airways on CT imaging. We analyzed the 3661 subjects with COPD with quantified airway measurements in the Genetic Epidemiology of COPD Study (COPDGene®). We hypothesized that patients with BDR would have greater CT measures of airway pathology and less emphysema compared to those without BDR.
Methods
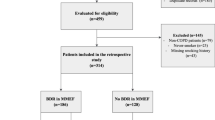
The Genetic Epidemiology of COPD (COPDGene®) Study is a multicenter observational study to analyze genetic susceptibility for the development of COPD. This study was IRB approved at all institutions (Temple IRB #11369). Inclusion and exclusion criteria were described previously [22]. Briefly, enrollees are African-American or non-Hispanic Caucasian between the ages of 45 and 80 with at least a 10 pack-year smoking history. Exclusion criteria include pregnancy, history of other lung diseases except asthma, prior lobectomy or lung volume reduction, active cancer undergoing treatment, known or suspected lung cancer.
Lung function testing and group assignment
We included patients with GOLD 1 through 4 disease severity in our analysis as defined by an FEV1/FVC ratio < 70. Each subject underwent pre- and post-bronchodilator spirometry using an EasyOne™ spirometer (Zurich, Switzerland) before and after the administration of 2 puffs of albuterol with spacer device. Bronchodilators were held prior to spirometry in usual fashion. Predicted values were obtained using NHANES III data [23]. BDR was assessed as an FEV1 % change after bronchodilator [(FEV1postBD – FEV1preBD)/FEV1preBD] × 100. 10% was used as a threshold of BDR. The patients were divided into two groups: BDR+, defined as ≥10% change in FEV1 [BDR + (10%)], and BDR-, defined as <10% change in FEV1 [BDR-(10%)]. Thresholds of ≥15% change and ≥12% and 200 mL in FEV1(American Thoracic Society criteria for BDR) were also analyzed separately as dividing points between groups [BDR + (15%) and BDR-(15%), BDR + (ATS) and BDR-(ATS)].
Computed tomography
Volumetric CT acquisitions were obtained at full inspiration and at the end of normal expiration. Thin-slice collimation with slice thickness and intervals of < lmm was used to enhance spatial resolution. Quantitative image analysis to calculate lung volumes, percent emphysema, and percent gas-trapping was performed using 3D SLICER (http://www.slicer.org/). Percent emphysema was defined as the total percentage of both lungs with attenuation values < −950 Hounsfield units on inspiratory images, and percent gas trapping was defined as the total percentage of both lungs with attenuation values < −856 Hounsfield units on expiratory images. Total lung capacity and functional residual capacity were calculated based on inspiratory and expiratory CT images, respectively. Airway disease was quantified using VIDA Diagnostics Inc.’s PW workstation software (http://www.vidadiagnostics.com) as wall area percent (WA%: (wall area/total bronchial area)×100) [9]. The mean WA% was calculated as the average of six segmental bronchi in each subject. Using 3D SLICER, airway wall thickness was also expressed as the square root wall area of a 10 mm diameter airway (Pi10) and 15 mm diameter airway (Pi15) as previously described [21].
Statistical analysis
Analysis was performed using SPSS v21.0. Categorical variables were compared between groups using Chi squared test. Continuous variables were evaluated using 2-tailed unpaired t test. Wilcoxon rank sum test was used for non-normally distributed data. A p value <0.05 was considered statistically significant. Pearson correlations were performed between the measures of airway wall thickness and percent change in FEV1. Multivariate logistic regressions were performed to assess the independent effects of airway dimensions on BDR, using the 10%, 15%, and ATS dividing points in separate models with current smoking, history of asthma, %emphysema, %gas trapping, FEV1 %predicted, and FVC %predicted as covariates. FEV1/FVC ratio was excluded due to significant co-linearity with spirometric parameters. In addition, a multivariate linear regression was performed for SGRQ scores, mMRC dyspnea scores, total and severe exacerbations as outcomes of interest with lung function and BDR as covariates.
Results
There were 1306 subjects in the BDR + (10%) group (35.7% of total) and 2355 subjects in the BDR-(10%) group. Baseline subject characteristics are summarized in Table 1. The BDR + (10%) group was older, was less likely to be currently smoking, had a greater history of asthma, worse lung function, higher BODE indices, worse health related quality of life (SGRQ scores), greater dyspnea, and greater total and severe exacerbation frequency compared to the BDR-(10%) group. There were no differences in gender, race, BMI, or 6-min walk distance. Similarly, the BDR + (15%) (n = 798, 21.8% of total) group had a greater smoking history, history of asthma, higher BODE indices, worse SGRQ scores, greater dyspnea, worse lung function, and greater total exacerbation history compared to the BDR-(15%) group (n = 2863). However, unlike the differences between the BDR + (10%) and BDR-(10%) groups, the BDR + (15%) group had a lower 6-minute walk distance, and did not have a greater history of severe exacerbations (defined as an exacerbation requiring an emergency room visit or hospitalization) compared to the BDR-(15%) group. Similar to the BDR + (10%) and BDR + (15%) groups, the BDR + (ATS) group (n = 1276, 34.9% total) had worse lung function, higher SGRQ scores, BODE scores, and mMRC dyspnea scores, but there were no differences in total and severe exacerbations. In all groups, percent change in FVC was greater in the BDR + groups.
When a multivariate linear regression was performed for SGRQ scores, mMRC dyspnea scores, total and severe exacerbations as outcomes of interest with FEV1 %predicted, FVC %predicted, and BDR by either 10%, 15%, or ATS criteria as covariates, BDR was not a significant predictor for these outcomes. This indicates that the differences in dyspnea, health related quality of life, and exacerbations were more likely a consequence of the differences in lung function in the BDR + groups.
Quantitative CT measurements are summarized in Table 2. The BDR + (10%) group had slightly more %emphysema, had more %gas trapping, and a higher functional residual capacity compared to the BDR-(10%) group. Total lung capacity was not different between groups. Pi10, Pi15, and WA% were significantly greater in the BDR + (10%) group compared to the BDR-(10%) group. The results were similar with the BDR + (15%) and BDR-(15%) groups, but the differences was slightly greater compared to the differences between the BDR + (10%) and BDR-(10%) groups. The BDR + (ATS) group had greater Pi10, Pi15, and WA% compared to the BDR-(ATS) group. In contrast to the other two groups, the BDR + (ATS) group had similar %emphysema and a lower FRC compared to the BDR-(ATS) group.
Table 3 summarizes airway dimensions according to BDR + (10%) or BDR-(10%) by GOLD stage. In each GOLD stage, Pi10, Pi15, and WA% is greater in the BDR + (10%) group, with the exception of Pi10 in GOLD 3 subjects. This is depicted in Figure 1. The three variables for airway thickness were weakly related to percent change in FEV1 as a continuous variable. The correlation coefficients for Pi10, Pi15, and WA% are 0.148, 0.145, and 0.167, respectively, p < 0.0001 for all relationships. Figure 2 demonstrates the relationship between WA% and BDR.

Airway dimensions in those that are BDR + (10%) and BDR-(10%) according to GOLD stage. Data presented as mean ± SD. A) Pi10, B) Pi15, and C) WA%. *p < 0.05. †p < 0.0001.

Relationship between WA% and percent change in FEV 1 .
Table 4 summarizes the odds ratios and 95% confidence intervals for the multivariate logistic regressions for the three measures of bronchodilator responsiveness (BDR ≥ 10%, BDR ≥ 15%, BDR + by ATS criteria) as the outcomes of interest with using the three measures of airway wall thickness as predictors of interest in separate models. All three measures of airway wall measures had significant odds ratios for bronchodilator responsiveness. The most significant odds ratios were for Pi15 (4.60 [95% CI 3.13, 6.75], 5.35 [95% CI 3.48, 8.24], and 5.13 [95% CI 3.46, 7.61] for BDR + (10%), (15%), and (ATS), respectively). Asthma history was not a significant predictor of BDR in these multivariate models (1.07 [95% CI 0.99, 1.15], 0.99 [95% CI 0.91, 1.08], and 0.97 [95% CI 0.81, 1.16] for BDR + (10%), (15%), and (ATS), respectively).
Discussion
We have demonstrated that subjects with BDR have CT evidence of thicker airways than non BDR subjects using three different thresholds for change in FEV1. We also showed that the two groups divided by changes in FEV1 were similar in terms of race and gender distribution, but had higher BODE indices, worse lung function, worse health related quality of life and dyspnea, and greater exacerbation frequency. To our knowledge, this is the most comprehensive clinical and CT description of subjects with and without BDR.
We chose FEV1 to determine BDR using several cutoff values based on prior studies [24],[25] because of the notion that changes in FEV1 may be more reflective of airway disease. In addition to percent changes, we also analyzed an absolute change in FEV1 to divide subjects into groups. Indeed, many patients with COPD, particularly those with worse disease, demonstrate responsiveness to bronchodilator by an increase in FVC as opposed to FEV1[26]. This may represent decreases in air trapping and dynamic airway collapse during forced expiratory maneuvers [27]. In our study, we found that those with BDR by FEV1 criteria also had significantly greater increases in FVC, and thus could also be labeled “volume responders” in addition to “flow responders” [14].
Studies have shown conflicting results in clinical outcomes of BDR in COPD. There are some studies that show an accelerated decline in lung function in reversible patients, whereas other studies have not [9],[14],[28]. In the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE), a three year prospective observational study, patients with BDR had a 17 ± 4 ml per year greater rate of decline in FEV1 compared to those without BDR [9], but no differences in mortality, hospitalizations, or exacerbations were found [29]. Bronchial hyper-responsiveness was found to accelerate lung function decline in over 7,000 individuals and conferred an odds ratio of 4.5 for the development of COPD [13]. However, Nishimura et al. categorized GOLD 1–4 COPD patients into rapid decliners, slow decliners, and sustainers of lung function and found no difference in the presence of BDR among these three groups [14]. Similarly, there was no relationship between BDR and rate of lung function decline in the Inhaled Steroids in Obstructive Lung Disease in Europe trial (ISOLDE) or the Understanding Potential Long-term Improvements in Function with Tiotropium trial (UPLIFT) [24],[28]. In addition, acute bronchodilator responsiveness did not predict improvements in lung function with tiotropium [24]. Therefore, it is unclear if BDR in COPD has any clinical significance.
Part of the problem lies in the variability in the definition of BDR across studies and the inconsistency of BDR in COPD subjects over time. Calverley et al. found that 52% of 660 patients with serial lung function testing switched responder status to bronchodilator [8]. In the National Intermittent Positive Pressure Breathing Trial, 65% of patients had at least 1 visit with 15% improvement in lung function with administration of isoproterenol over a period of 2 years [30]. Another complicating matter is that using American Thoracic Society criteria of a change in FEV1 of 12% and 200 cc may be too restrictive for subjects with very severe airflow obstruction [31]. For someone with an FEV1 of 800 cc, for example, a change of 200 cc would translate into a change of 25%, a change much greater than 12%. In addition, many patients with severe COPD demonstrate a change in FVC acutely, not necessarily FEV1, in response to bronchodilator [26]. Thus, a practical, consistent definition of BDR is needed in order to understand the importance of this physiologic phenomenon.
Regardless of its clinical consequences, BDR is associated with thicker airways based on quantitative CT imaging. The reason for these observed differences is not clear, but our results are hypothesis generating. It is possible that genetic influences have bearing on BDR in COPD, accounting for both the physiologic and CT differences between those with and without BDR. Indeed, one study revealed greater BDR in smokers of first degree relatives with early onset COPD [32], and another identified several genomic regions that could contain loci regulating BDR [33]. If that is the case, then this could mean there are different potential therapeutic targets for those with BDR. This would have to be confirmed with more extensive genetic analysis. In addition, we have shown that advanced emphysema patients with greater airway smooth muscle mass were more likely to demonstrate BDR on lung function testing [34]. Other investigators have found direct correlations with the degree of smooth muscle mass and airflow obstruction in COPD [16],[17]. The increased CT airway thickness in the BDR groups may represent a greater degree of smooth muscle hypertrophy, which is thought to be the pathologic correlate in asthma responsible for bronchodilator responsiveness and airway hyper-responsiveness. These findings, however, must be confirmed in studies that also obtain surgical lung tissue or autopsy obtained tissue to confirm our results pathologically. Finally, it has been proposed that gas trapping may be a surrogate marker for airway disease in COPD; the association between BDR and gas trapping in our cohort is consistent with this notion.
Of interest was the finding that percent emphysema and percent gas trapping were greater in those in the BDR + (10%) and BDR + (15%) groups, but there was no difference in emphysema in the BDR + (ATS) group. This most likely reflects the differences in lung function between the groups; FEV1 and FVC %predicted were lower in the BDR + (10%) and BDR + (15%) groups and higher in the BDR + (ATS) group. This phenomenon likely is a result of greater ease in achieving an absolute change of 200 mL with bronchodilator in those with better lung function. In addition, in the multivariate models for BDR + presented in Table 4, %emphysema had slightly but significantly reduced odds ratios for BDR, and %gas trapping had slightly but significantly greater odds ratios for BDR. This is consistent with prior studies that have found lower percent emphysema is associated with BDR [35].
This study has some noteworthy limitations. Firstly, lung function testing was only performed once, leading to the possibility of inconsistency and lack of repeatability of the response to bronchodilator during serial testing. Some subjects that were not reversible may demonstrate reversibility on their next measure of airflow by spirometry [8]. Secondly, outcomes such as exacerbation and asthma history were by subject self-report, lending to recall bias. In addition, the inclusion of subjects with asthma, whether or not the diagnosis was made by a physician, is a limitation of the study. Thirdly, the differences in airway measurements were small between groups, making the significance of the data questionable. However, the multivariate analyses clearly show BDR, using various definitions, to increase the odds of having thicker airways. Finally, many of the clinical phenotypic differences are most likely the result of differences in lung function between the two groups.
Conclusions
We show that quantitative CT measures of airway thickness are greater in those with bronchodilator responsiveness. This is one more step towards bridging the gap between radiological and pathological correlations. How these differences in airway thickness translates to airway pathology remains to be determined.
Abbreviations
- BDR:
-
Bronchodilator responsiveness
- BDR + (10%):
-
Bronchodilator responsiveness as defined by increase in FEV1 by 10%
- BDR + (15%):
-
Bronchodilator responsiveness as defined by increase in FEV1 by 15%
- BDR + (ATS):
-
Bronchodilator responsiveness as defined by increase in FEV1 by 12% and 200 mL
- BODE:
-
Body mass index, airflow obstruction, dyspnea, exercise capacity
- COPD:
-
Chronic obstructive pulmonary disease
- CT:
-
Computed tomography
- FEV1:
-
Forced expiratory volume in 1 second
- FRC:
-
Functional residual capacity
- FVC:
-
Forced vital capacity
- mMRC:
-
Modified Medical Research Council
- Pi10:
-
Airway of 10 mm internal perimeter
- Pi15:
-
Airway of 15 mm internal perimeter
- SGRQ:
-
St. George’s Respiratory Questionaire
- TLC:
-
Total lung capacity
- WA%:
-
Wall area percent
References
Global Initiative for Chronic Obstructive Pulmonary Disease: Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease, executive summary 2005. 2005, ., [www.goldcopd.com]
Orie NG: The dutch hypothesis. Chest. 2000, 117 (5 Suppl 1): 299S-
Barnes PJ: Mechanisms in COPD: differences from asthma. Chest. 2000, 117 (2 Suppl): 10S-14S.
Vermeire PA, Pride NB: A “splitting” look at chronic nonspecific lung disease (CNSLD): common features but diverse pathogenesis. Eur Respir J. 1991, 4 (4): 490-496.
Dorinsky PM, Reisner C, Ferguson GT, Menjoge SS, Serby CW, Witek TJ: The combination of ipratropium and albuterol optimizes pulmonary function reversibility testing in patients with COPD. Chest. 1999, 115 (4): 966-971.
Mahler DA, Wire P, Horstman D, Chang CN, Yates J, Fischer T, Dorinsky PM, Reisner C, Ferguson GT, Menjoge SS, Serby CW, Witek TJ: Effectiveness of fluticasone propionate and salmeterol combination delivered via the diskus device in the treatment of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002, 166 (8): 1084-1091.
Tashkin DP, Celli B, Senn S, Burkhart D, Kesten S, Menjoge S, Decramer D: A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008, 359 (15): 1543-1554.
Calverley PM, Burge PS, Spencer S, Anderson JA, Jones PW: Bronchodilator reversibility testing in chronic obstructive pulmonary disease. Thorax. 2003, 58 (8): 659-664.
Vestbo J, Edwards LD, Scanlon PD, Yates JC, Agusti A, Bakke P, Calverley PM, Celli B, Coxson HO, Crim C, Lomas DA, Macnee W, Miller BE, Silverman EK, Tal-Singer R, Wouters E, Rennard SI: Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011, 365 (13): 1184-1192.
Vollmer WM, Johnson LR, Buist AS: Relationship of response to a bronchodilator and decline in forced expiratory volume in one second in population studies. Am Rev Respir Dis. 1985, 132 (6): 1186-1193.
Postma DS, Gimeno F, van der Weele LT, Sluiter HJ: Assessment of ventilatory variables in survival prediction of patients with chronic airflow obstruction: the importance of reversibility. Eur J Respir Dis. 1985, 67 (5): 360-368.
Postma DS, De Vries K, Koeter GH, Sluiter HJ: Independent influence of reversibility of air-flow obstruction and nonspecific hyperreactivity on the long-term course of lung function in chronic air-flow obstruction. Am Rev Respir Dis. 1986, 134 (2): 276-280.
Brutsche MH, Downs SH, Schindler C, Gerbase MW, Schwartz J, Frey M, Russi EW, Ackermann-Liebrich U, Leuenberger P: Bronchial hyperresponsiveness and the development of asthma and COPD in asymptomatic individuals: SAPALDIA cohort study. Thorax. 2006, 61 (8): 671-677.
Nishimura M, Makita H, Nagai K, Konno S, Nasuhara Y, Hasegawa M, Shimizu K, Betsuyaku T, Ito YM, Fuke S, Igarashi T, Akiyama Y, Ogura S: Annual change in pulmonary function and clinical phenotype in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012, 185 (1): 44-52.
Kim V, Rogers TJ, Criner GJ: New concepts in the pathobiology of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008, 5 (4): 478-485.
Finkelstein R, Fraser RS, Ghezzo H, Cosio MG: Alveolar inflammation and its relation to emphysema in smokers. Am J Respir Crit Care Med. 1995, 152 (5 Pt 1): 1666-1672.
Hogg JC, Chu F, Utokaparch S, Woods R, Elliott WM, Buzatu L, Cherniack RM, Rogers RM, Sciurba FC, Coxson HO, Pare PD: The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004, 350 (26): 2645-2653.
Kim V, Kelemen SE, Abuel-Haija M, Gaughan J, Sharafkhaneh A, Evans CM, Dickey BF, Solomides CC, Rogers TJ, Criner GJ: Small airway mucous metaplasia and inflammation in chronic obstructive pulmonary disease. J COPD. 2008, 5 (6): 329-338.
Nakano Y, Muro S, Sakai H, Hirai T, Chin K, Tsukino M, Nishimura K, Itoh H, Pare PD, Hogg JC, Mishima M: Computed tomographic measurements of airway dimensions and emphysema in smokers. correlation with lung function. Am J Respir Crit Care Med. 2000, 162 (3 Pt 1): 1102-1108.
Hasegawa M, Nasuhara Y, Onodera Y, Makita H, Nagai K, Fuke S, Ito Y, Betsuyaku T, Nishimura M: Airflow limitation and airway dimensions in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2006, 173 (12): 1309-1315.
Patel BD, Coxson HO, Pillai SG, Agusti AG, Calverley PM, Donner CF, Make BJ, Muller NL, Rennard SI, Vestbo J, Wouters EF, Hiorns MP, Nakano Y, Camp PG, Nasute Fauerbach PV, Screaton NJ, Campbell EJ, Anderson WH, Pare PD, Levy RD, Lake SL, Silverman EK, Lomas DA: Airway wall thickening and emphysema show independent familial aggregation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2008, 178 (5): 500-505.
Regan EA, Hokanson JE, Murphy JR, Make B, Lynch DA, Beaty TH, Curran-Everett D, Silverman EK, Crapo JD: Genetic epidemiology of COPD (COPDGene) study design. COPD. 2010, 7 (1): 32-43.
Hankinson JL, Odencrantz JR, Fedan KB: Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999, 159 (1): 179-187.
Hanania NA, Sharafkhaneh A, Celli B, Decramer M, Lystig T, Kesten S, Tashkin D: Acute bronchodilator responsiveness and health outcomes in COPD patients in the UPLIFT trial. Respir Res. 2011, 12: 6-
Tashkin DP, Celli B, Senn S, Burkhart D, Kesten S, Menjoge S, Decramer M: Bronchodilator responsiveness in patients with COPD. Eur Respir J. 2008, 31 (4): 742-750.
Walker PP, Calverley PM: The volumetric response to bronchodilators in stable chronic obstructive pulmonary disease. COPD. 2008, 5 (3): 147-152.
Cerveri I, Pellegrino R, Dore R, Corsico A, Fulgoni P, Van De Woestijne KP, Brusasco V: Mechanisms for isolated volume response to a bronchodilator in patients with COPD. J Appl Physiol. 2000, 88 (6): 1989-1995.
Anthonisen NR, Lindgren PG, Tashkin DP, Kanner RE, Scanlon PD, Connett JE: Bronchodilator response in the lung health study over 11 yrs. Eur Respir J. 2005, 26 (1): 45-51.
Albert P, Agusti A, Edwards L, Tal-Singer R, Yates J, Bakke P, Celli BR, Coxson HO, Crim C, Lomas DA, Macnee W, Miller B, Rennard S, Silverman EK, Vestbo J, Wouters E, Calverley P: Bronchodilator responsiveness as a phenotypic characteristic of established chronic obstructive pulmonary disease. Thorax. 2012, 67 (8): 701-708.
Nagai A, West WW, Thurlbeck WM: The national institutes of health intermittent positive-pressure breathing trial: pathology studies. II. Correlation between morphologic findings, clinical findings, and evidence of expiratory air-flow obstruction. Am Rev Respir Dis. 1985, 132 (5): 946-953.
Hansen JE: Assessment of bronchoreversibility in severe emphysema. Eur Respir J. 2010, 36 (4): 972-author reply 973
Celedon JC, Speizer FE, Drazen JM, Weiss ST, Campbell EJ, Carey VJ, Reilly JJ, Ginns L, Silverman EK: Bronchodilator responsiveness and serum total IgE levels in families of probands with severe early-onset COPD. Eur Respir J. 1999, 14 (5): 1009-1014.
Palmer LJ, Celedon JC, Chapman HA, Speizer FE, Weiss ST, Silverman EK: Genome-wide linkage analysis of bronchodilator responsiveness and post-bronchodilator spirometric phenotypes in chronic obstructive pulmonary disease. Hum Mol Genet. 2003, 12 (10): 1199-1210.
Kim V, Pechulis RM, Abuel-Haija M, Solomides CC, Gaughan JP, Criner GJ: Small airway pathology and bronchoreversibility in advanced emphysema. COPD. 2010, 7 (2): 93-101.
Han MK, Wise R, Mumford J, Sciurba F, Criner GJ, Curtis JL, Han MK, Wise R, Mumford J, Sciurba F, Criner GJ, Curtis JL, Murray S, Sternberg A, Weinman G, Kazerooni E, Fishman AP, Make B, Hoffman EA, Mosenifar Z, Martinez FJ: Prevalence and clinical correlates of bronchoreversibility in severe emphysema. Eur Respir J. 2010, 35 (5): 1048-1056.
Acknowledgements
We acknowledge and thank the COPDGene Core Teams:
Administrative Core: James D. Crapo, MD (PI); Edwin K. Silverman, MD, PhD (PI); Barry J. Make, MD; Elizabeth A. Regan, MD, PhD; Stephanie Bratschie, MPH; Rochelle Lantz; Sandra Melanson, MSW, LCSW; Lori Stepp
Executive Committee: Terri Beaty, PhD; Russell P. Bowler, MD, PhD; James D. Crapo, MD; Jeffrey L. Curtis, MD; Douglas Everett, PhD; MeiLan K. Han, MD, MS; John E. Hokanson, MPH, PhD; David Lynch, MB; Barry J. Make, MD; Elizabeth A. Regan, MD, PhD; Edwin K. Silverman, MD, PhD; E. Rand Sutherland, MD
External Advisory Committee: Eugene R. Bleecker, MD; Harvey O. Coxson, PhD; Ronald G. Crystal, MD; James C. Hogg, MD; Michael A. Province, PhD; Stephen I. Rennard, MD; Duncan C. Thomas, PhD
NHLBI: Thomas Croxton, MD, PhD; Weiniu Gan, PhD; Lisa Postow, PhD
COPD Foundation: John W. Walsh; Randel Plant; Delia Prieto
Data Coordinating Center: Douglas Everett, PhD; Andre Williams, PhD; Ruthie Knowles; Carla Wilson, MS
Epidemiology Core: John Hokanson, MPH, PhD; Jennifer Black-Shinn, MPH; Gregory Kinney, MPH
Genetic Analysis Core: Terri Beaty, PhD; Peter J. Castaldi, MD, MSc; Michael Cho, MD; Dawn L. DeMeo, MD, MPH; Marilyn G. Foreman, MD, MS; Nadia N. Hansel, MD, MPH; Megan E. Hardin, MD; Craig Hersh, MD, MPH; Jacqueline Hetmanski, MS; John E. Hokanson, MPH, PhD; Nan Laird, PhD; Christoph Lange, PhD; Sharon M. Lutz, MPH, PhD; Manuel Mattheisen, MD; Merry-Lynn McDonald, MSc, PhD; Margaret M. Parker, MHS; Elizabeth A. Regan, MD, PhD; Stephanie Santorico, PhD; Edwin K. Silverman, MD, PhD; Emily S. Wan, MD; Jin Zhou, PhD
Genotyping Cores: Genome-Wide Core: Terri Beaty, PhD; Candidate Genotyping Core: Craig P. Hersh, MD, MPH; Edwin K. Silverman, MD, PhD
Imaging Core: David Lynch, MB; Mustafa Al Qaisi, MD; Jaleh Akhavan; Christian W. Cox, MD; Harvey O. Coxson, PhD; Deanna Cusick; Jennifer G. Dy, PhD; Shoshana Ginsburg, MS; Eric A. Hoffman, PhD; Philip F. Judy, PhD; Alex Kluiber; Alexander McKenzie; John D. Newell, Jr., MD; John J. Reilly, Jr., MD; James Ross, MSc; Raul San Jose Estepar, PhD; Joyce D. Schroeder, MD; Jered Sieren; Arkadiusz Sitek, PhD; Douglas Stinson; Edwin van Beek, MD, PhD, MEd; George R. Washko, MD; Jordan Zach
PFT QA Core: Robert Jensen, PhD; E. Rand Sutherland, MD
Biological Repository, Johns Hopkins University, Baltimore, MD: Homayoon Farzadegan, PhD: Samantha Bragan; Stacey Cayetano
We further wish to acknowledge the COPDGene Investigators from the participating Clinical Centers:
Ann Arbor VA: Jeffrey Curtis, MD, Ella Kazerooni, MD
Baylor College of Medicine, Houston, TX: Nicola Hanania, MD, MS, Philip Alapat, MD, Venkata Bandi, MD, Kalpalatha Guntupalli, MD, Elizabeth Guy, MD, Antara Mallampalli, MD, Charles Trinh, MD, Mustafa Atik, MD, Hasan Al-Azzawi, MD, Marc Willis, DO, Susan Pinero, MD, Linda Fahr, MD, Arun Nachiappan, MD, Collin Bray, MD, L. Alexander Frigini, MD, Carlos Farinas, MD, David Katz, MD, Jose Freytes, MD, Anne Marie Marciel, MD
Brigham and Women’s Hospital, Boston, MA: Dawn DeMeo, MD, MPH, Craig Hersh, MD, MPH, George Washko, MD, Francine Jacobson, MD, MPH, Hiroto Hatabu, MD, PhD, Peter Clarke, MD, Ritu Gill, MD, Andetta Hunsaker, MD, Beatrice Trotman-Dickenson, MBBS, Rachna Madan, MD
Columbia University, New York, NY: R. Graham Barr, MD, DrPH, Byron Thomashow, MD, John Austin, MD, Belinda D’Souza, MD
Duke University Medical Center, Durham, NC: Neil MacIntyre, Jr., MD, Lacey Washington, MD, H Page McAdams, MD
Richard Rosiello, MD, Timothy Bresnahan, MD, Joseph Bradley, MD, Sharon Kuong, MD, Steven Meller, MD, Suzanne Roland, MD
Health Partners Research Foundation, Minneapolis, MN: Charlene McEvoy, MD, MPH, Joseph Tashjian, MD
Johns Hopkins University, Baltimore, MD: Robert Wise, MD, Nadia Hansel, MD, MPH, Robert Brown, MD, Gregory Diette, MD, Karen Horton, MD
Los Angeles Biomedical Research Institute at Harbor UCLA Medical Center, Los Angeles, CA: Richard Casaburi, MD, Janos Porszasz, MD, PhD, Hans Fischer, MD, PhD, Matt Budoff, MD, Mehdi Rambod, MD
Michael E. DeBakey VAMC, Houston, TX: Amir Sharafkhaneh, MD, Charles Trinh, MD, Hirani Kamal, MD, Roham Darvishi, MD, Marc Willis, DO, Susan Pinero, MD, Linda Fahr, MD, Arun Nachiappan, MD, Collin Bray, MD, L. Alexander Frigini, MD, Carlos Farinas, MD, David Katz, MD, Jose Freytes, MD, Anne Marie Marciel, MD
Minneapolis VA: Dennis Niewoehner, MD, Quentin Anderson, MD, Kathryn Rice, MD, Audrey Caine, MD
Morehouse School of Medicine, Atlanta, GA: Marilyn Foreman, MD, MS, Gloria Westney, MD, MS, Eugene Berkowitz, MD, PhD
National Jewish Health, Denver, CO: Russell Bowler, MD, PhD, David Lynch, MB, Joyce Schroeder, MD, Valerie Hale, MD, John Armstrong, II, MD, Debra Dyer, MD, Jonathan Chung, MD, Christian Cox, MD
Temple University, Philadelphia, PA: Gerard Criner, MD, Victor Kim, MD, Nathaniel Marchetti, DO, Aditi Satti, MD, A. James Mamary, MD, Robert Steiner, MD, Chandra Dass, MD, Libby Cone, MD
University of Alabama, Birmingham, AL: William Bailey, MD, Mark Dransfield, MD, Michael Wells, MD, Surya Bhatt, MD, Hrudaya Nath, MD, Satinder Singh, MD
University of California, San Diego, CA: Joe Ramsdell, MD, Paul Friedman, MD
University of Iowa, Iowa City, IA: Alejandro Cornellas, MD, John Newell, Jr., MD, Edwin JR van Beek, MD, PhD
University of Michigan, Ann Arbor, MI: Fernando Martinez, MD, MeiLan Han, MD, Ella Kazerooni, MD
University of Minnesota, Minneapolis, MN: Christine Wendt, MD, Tadashi Allen, MD
University of Pittsburgh, Pittsburgh, PA: Frank Sciurba, MD, Joel Weissfeld, MD, MPH, Carl Fuhrman, MD, Jessica Bon, MD, Danielle Hooper, MD
University of Texas Health Science Center at San Antonio, San Antonio, TX: Antonio Anzueto, MD, Sandra Adams, MD, Carlos Orozco, MD, Mario Ruiz, MD, Amy Mumbower, MD, Ariel Kruger, MD, Carlos Restrepo, MD, Michael Lane, MD
COPDGene is supported by NHLBI R01 HL089856 and R01 HL089897
Disclosures
VK has nothing to disclose in relationship to this manuscript but has served on an advisory committee for CSA and has participated in clinical trials sponsored by Boehringer Ingelheim, Glaxo-Smith-Kline, and Roche pharmaceuticals. VK is supported by NHLBI K23HL094696. JDN is a paid consultant for VIDA Diagnostics Inc and has stock options in VIDA Diagnostics Inc. JDN has funded research from Siemens Health. EKS received grant support and consulting fees from GlaxoSmithKline for studies of COPD genetics. EKS received grant support from GlaxoSmithKline for studies of COPD genetics, and he received honoraria and consulting fees from AstraZeneca, Merck, and GlaxoSmithKline. PD, SPB, and JC have nothing to disclose. GW has received grants from the NHLBI to perform quantitative image analysis and have been a paid consultant for MedImmune and Spiration, and his spouse is an employee of Merck Research Laboratories. Over the last three years, BJM has participated in advisory boards, speaker bureaus, consultations and multi-center clinical trials with funding from the National Heart Lung and Blood Institute, Abbott, Astellas, AstraZeneca, Boerhinger-Ingelheim, Coviden, Dey, Forest, GlaxoSmithKline, Merck, MedImmune, NABI, Novartis, Pfizer, Respironics, Sepracor, Sequal and Talecris. GJC has served on Advisory Committees for Boehringer Ingelheim, Ikaria, Holaira, CSA and Amirall. All of these sums are less than $2,500. GJC has received research grants from: Boehringer Ingelheim, Forest, Actelion, Glaxo-Smith-Kline, AstraZeneca, Pearl, Novartis Pharmaceuticals, Pulmonx, PneumRX and Aeris Therapeutics. All research grant monies are deposited and controlled by Temple University.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare no competing interests.
Authors’ contributions
VK, PD, GJC were involved in the conception, hypotheses delineation, and design of the study and acquisition of the data; VK, PD, GW, JDN, and GJC were involved in the analysis and interpretation of the data; VK, PD, GJC, SB, GW, BJM, JC, EKS were involved in the writing the article or substantial involvement in its revision prior to submission. VK is the guarantor of the content of the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

{kind=link}
{kind=link}
Cite this article
Kim, V., Desai, P., Newell, J.D. et al. Airway wall thickness is increased in COPD patients with bronchodilator responsiveness. Respir Res 15, 84 (2014). https://doi.org/10.1186/s12931-014-0084-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-014-0084-3