
Abstract
Background
Alcohol consumption and oxidative stress are well-known risk factors for developing atrial fibrillation (AF). Single nucleotide polymorphisms (SNPs) of alcohol dehydrogenase (ADH1B) and aldehyde dehydrogenase 2 (ALDH2) genes encoding enzymes of alcohol and reactive aldehyde metabolism, respectively, are prevalent among East Asians. Here, we examined whether these SNPs were associated with AF in Japanese patients.
Methods and results
Five hundred seventy-seven Japanese patients with AF undergoing catheter ablation and 1935 controls at Hiroshima University Hospital were studied. Alcohol consumption habits, medical history, electrocardiogram (EKG), electrophysiology and cardiac echocardiography were reviewed. Patients were also genotyped for ALDH2 (rs671) and ADH1B (rs1229984). A significant linear correlation was found between ALDH2 genotype and mean alcohol intake (P = 1.7 × 10−6). Further, ALDH2 (rs671) was associated with AF (P = 7.6 × 10−4, odds ratio [OR] = 0.6). Frequency of the ALDH2 SNP allele A which limits acetaldehyde metabolism was lower in patients with AF (18.8%) than in controls (23.5%). In contrast, we found that the frequencies of the ADH1B SNP genotypes were similar in patients with AF and in controls. Subset analysis among the 182 patients with lone AF and 914 controls (control II) (<60 years of age and without hypertension), both ALDH2 and ADH1B SNPs were significantly associated with AF (P = 0.013, OR = 0.7; P = 0.0007, OR = 1.4, respectively). The frequency of the dysfunctional allele A of ALDH2 was significantly lower and the dysfunctional allele G of ADH1B was significantly higher in patients with lone AF than in control II (ALDH2 A allele frequency = 0.176 vs 0.235, OR = 1.3, P = 0.013, ADH1B SNP G allele frequency = 0.286 vs 0.220, OR = 1.4, P = 0.0007).
Conclusions
When considering all patients enrolled, the dysfunctional ALDH2 allele was negatively associated with AF. When examining a subset of patients with lone AF, the dysfunctional ALDH2 allele was negatively associated with AF and the slower metabolizing ADH1B allele was positively associated with AF. Hence, prolonged metabolic conversion of alcohol to acetaldehyde may be associated with the occurrence of AF in the Japanese and other East Asian populations.
Similar content being viewed by others

Background
Atrial fibrillation (AF) is the most common arrhythmia, with many risk factors being reported, including aging, male sex, hypertension, valvular diseases, left ventricular dysfunction, obesity, sleep apnea, and alcohol consumption [1]. High alcohol consumption is associated with the occurrence of AF. Some meta-analyses have identified a dose–response relationship between alcohol consumption and AF risk, and other recent studies have reported that even moderate alcohol consumption is a risk factor for AF [2, 3].
Two enzymes are mainly involved in alcohol metabolism. Alcohol is first metabolized to acetaldehyde by alcohol dehydrogenase 1B (ADH1B), and then to acetic acid by aldehyde dehydrogenase 2 (ALDH2) [4]. ALDH2 is an enzyme not only for alcohol metabolism but also for catalyzing the oxidation of an aldehyde that is a lipid peroxidation product, such as 4-hydroxy-2-nonenal (4-HNE), and other aldehydes. Thus, ALDH2 besides alcohol metabolism, reduces the damage of reactive oxygen species (ROS) and protects against oxidative stress [5, 6]. Amino acid coding single nucleotide polymorphisms (SNPs) of ADH1B (G/A, rs1229984) and ALDH2 (G/A, rs671) are widely known, and the ADH1B G and ALDH2 A alleles of these SNPs have notably decreased enzymatic activities. The dysfunctional G allele of ADH1B results in slower conversion of alcohol to acetaldehyde and the dysfunctional A allele of ALDH2 SNP is associated with deficiency in the conversion of acetaldehyde to acetic acid, hence the accumulation of toxic acetaldehyde because of their low metabolic activities [7, 8]. The ALDH2 deficiency has been known to be the underlying cause of “Alcohol Flushing Syndrome” [9]. The ADH1B and ALDH2 SNPs are especially common in East Asians [10]. People with the dysfunctional A allele of the ALDH2 SNP are at risk for many types of systemic disease because of its reduced capacity on both acetaldehyde metabolism and protection against oxidative stress [11]. Importantly, excess amounts of ROS has been known to be associated with AF by their effects on ion channels, cell coupling, and molecular mechanisms [12].
In this study, we investigated the association of ADH1B and ALDH2 SNPs with AF in Japanese populations because of their involvement with alcohol metabolism and for metabolizing reactive aldehydes produced during ROS production.
Methods
Participants
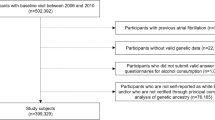
We enrolled 577 patients with AF (427 males and 130 females, mean age 61 ± 10 years) who were undergoing catheter ablation in Hiroshima University Hospital. We also enrolled 1935 non-AF controls (1563 male, mean age 55 ± 13 years) from Hiroshima University Hospital. The Institutional Ethics Committee of the Graduate School of Biomedical Science at Hiroshima University approved all procedures involving human genome usage. Written informed consent was obtained from all participants.
We genotyped SNPs rs671 of ALDH2 and rs1229984 of ADH1B and compared allele frequencies of these SNPs between AF subjects and non-AF controls. The lone AF was defined as AF diagnosed before the age of 60 years in the absence of hypertension and structural heart disease. We also examined the relationships between genotypes of the 2 SNPs in subgroup of 182 patients with lone AF and 914 controls without hypertension or structural heart disease (Control II).
All subjects underwent polysomnography (Somuno Screen, Fukuda Denshi) on the day before admission, and the apnea hypopnea index was calculated.
We interviewed the 332 out 577 enrolled patients with AF about their daily and weekly alcohol intakes. We converted daily and weekly alcohol intakes into ethanol consumption (g/day) = volume of alcohol intake × (alcohol degree/100) × 0.8 for each patient.
Genotyping of ALDH2 (rs671) and ADH1B (rs1229984)
Blood samples were obtained from all participants. Genomic DNA was extracted from leukocytes using a QIAamp DNA Blood Mini Kit (QIAGEN, Hilden, Germany) according to the standard protocol. Subsequently, we genotyped SNPs rs671 of ALDH2 and rs1229984 of ADH1B in all participants using the Invader assay, as previously described [13, 14].
For typing the SNP of ALDH2 (rs671), we used the forward primer: GATGTGTTTGGAGCCCAGTC, reverse primer: CCCAACAGACCCCAATCC, Invader oligo: GCGAGTACGGGCTGCAGGCATACACTT, signal prove-G: CGCGCCGAGGgAAGTGAAAACTGTGAGTGTGG, and signal prove-A: ATGACGTGGCAGACaAAGTGAAAACTGTGAGTGTG. For typing the SNP of ADH1B (rs1229984), we used forward primer: CAATTTCAGGAATTTGGGTATG, reverse primer: CACACGTGTTCCCTGAGTGT and Invader oligo: CAGGTTGCCACTAACCACGTGGTCATCTGTGA, signal prove-G: CGCGCCGAGGcGACAGATTCCTACAGCC and signal prove-A: ATGACGTGGCAGACtGACAGATTCCTACAGC.
Echocardiographic measurements
Transthoracic echocardiographic examinations were performed in all patients with an iE33 ultrasound (Philips Medical Systems, Best, the Netherlands) equipped with a 3.5-MHz transducer at a depth of 16 cm with the patient in the left lateral decubitus position. The left atrial volume index was calculated by dividing the maximal left atrial volume by the body surface area. Left ventricular diameter and wall thickness were measured by two-dimensional echocardiography. Echocardiographic measurements were taken in accordance with the recommendations of the American Society of Echocardiography [15].
Electrophysiological study
The patients underwent electrophysiological study after pulmonary vein isolation. Three 5-French quadripolar electrode catheters, each with a 5-mm interelectrode distance, were positioned at the high right atrium, His bundle, and right ventricle. Right atria to His (AH) and His to right ventricle (HV) intervals were measured on the baseline electrocardiogram. Sinus node recovery time and atrioventricular node effective refractory period were also determined.
Statistical analysis
Normally distributed continuous variables are presented as means ± standard deviation. The differences between the three genotypes were analyzed by a linear regression for continuous data. Odds ratios (ORs) and 95% confidence intervals (CIs) are stated as appropriate. To test the genetic association between cases and controls, we used the chi-square test and the Cochran–Armitage trend test. Deviation from the Hardy–Weinberg equilibrium was tested among the cases and controls with an ordinary chi-square test, where a P-value of <0.05 was considered to indicate statistical significance.
Results
ALDH2 (rs671) was significantly negatively associated with AF (P = 7.6 × 10−4, OR = 1.3). In control group, the GG, GA and AA genotypes were 58.2, 36.7 and 5.1% as compared with 66.0, 30.6 and 3.5% respectively in the AF group (Fig. 1). We found that both the GA and AA genotype of ALDH2 were less common in the AF patient group. The frequency of the dysfunctional allele A was significantly lower in patients with AF than in controls (0.188 vs 0.235 P = 0.0007, Table 1). Table 2 shows the relationships between ALDH2 genotypes and clinical manifestations in patients with AF. We noticed that the frequency of ischemic heart disease was higher in AF patients with AA and GA genotypes than those with GG genotypes. The other clinical characteristics, echocardiographic findings, and electrophysiological study (EPS) findings were all similar for each ALDH2 genotype.

ALDH2 Polymorphism (rs671) in AF Patients and Controls. The frequency of the dysfunctional genotypes with allele A was significantly lower in patients with AF than in controls (P = 0.0007)
Among AF subjects whose alcohol consumption was available, the mean ethanol consumption was 30.6 ± 27.8 g/day in AF patients with GG genotype (N = 219), 17.6 ± 24.6 g/day in those with GA genotype (N = 98) and 0 g/day in those with AA genotype (N = 13). A significant linear correlation was found between ALDH2 genotype and mean alcohol intake (P = 1.7 × 10−6) (Fig. 2). In contrast, we found that the frequencies of the ADH1B genotypes were similar in patients with AF and in controls.

ALDH2 variant (rs671) genotypes and amounts of alcohol intake. A significant linear correlation was found between ALDH2 genotype and mean alcohol intake (P = 1.7 × 10−6)
A subgroup analysis of 182 patients with lone AF and 914 control subjects (control II), revealed that both ALDH2 (rs671) and ADH1B (rs1229984) were significantly associated with lone AF. The frequency of the dysfunctional allele A of ALDH2 SNP was significantly lower and the frequency of the dysfunctional allele G of ADH1B SNP was significantly higher in patients with lone AF than in control II (ALDH2 A allele frequency = 0.176 vs 0.235, OR = 1.3, P = 0.013, Fig. 3 and Table 3, ADH1B SNP G allele frequency = 0.286 vs 0.220, OR = 1.4, P = 0.0007, Fig. 4 and Table 4). For the ALDH2 SNP, the GG, GA and AA genotypes were 56.9, 36.2 and 3.9% in control II group as compared to 67.6, 39.2 and 2.7%, respectively, in the lone AF group for ALDH2. As for ADH1B, the GG, GA and AA genotypes were 4.7, 34.7 and 60.6% in control II group, as compared to 6.6, 44.0 and 49.5%, respectively, in the lone AF group. It is noteworthy that the frequency of the slower alcohol metabolizing allele G in ADH1B (rs1229984) was higher in patients with lone AF than in control II subjects. The characteristics of patients with lone AF and ADH1B genotypes are shown in Table 5. Among lone AF subjects whose alcohol consumption was available, mean ethanol consumption was 45.1 ± 33.5 g/day in lone AF patients with GG genotype (N = 6), 27.8 ± 27.6 g/day in those with GA genotype (N = 32) and 22.7 ± 24.3 g/day in those with AA genotype (N = 60). Alcohol intake tended to be higher in those with the GG genotype. A significant linear correlation was found between ADH1B genotype and the refractory period of the right atrium, indicating atrial conduction disturbance (P = 0.0453).

ALDH2 Polymorphism (rs671) in Lone AF Patients and Control II. The dysfunctional genotypes with allele A of ALDH2 SNP rs671 significantly decreased also in Lone AF patients (P = 0.01)

ADH1B Polymorphism (rs1229984) in Lone AF Patients and Control II. The dysfunctional genotypes with allele G of ADH1B SNP rs1229984 significantly increased in lone AF patients (P = 7.0x10-4)
Discussion
ADH1B (rs1229984) and ALDH2 (rs671) are common functional SNPs of alcohol and acetaldehyde-metabolizing enzymes that are prevalent in East Asians [10]. More than 90% of Japanese people, but under 20% of Caucasians, have the A allele of ADH1B SNP (rs1229984), which is associated with high metabolic activity in the conversion of alcohol to acetaldehyde. Whereas, about half of Japanese people, but less than 1% of Caucasians, have the dysfunctional A allele of ALDH2 SNP (rs671), which is associated with deficient metabolic activity in the conversion of acetaldehyde to acetic acid. Few Japanese people have the slower ADH1B G allele [8, 16]. Thus, people with the combination of high ADH1B activity and low ALDH2 activity are very common in Japan.
ALDH2 is a key enzyme not only for acetaldehyde metabolism, but also for the removal of toxic aldehydes, such as lipid peroxidation-derived 4-HNEand protection against ROS [5, 6]. The dysfunctional A allele of ALDH2 has been associated with risks for many diseases, including esophageal cancer, coronary artery diseases, Alzheimer’s disease, diabetes, stroke, and others [11, 17].
AF is the most common arrhythmia, and its frequency increases with age. Many risk factors for AF have been reported, including aging, male sex, hypertension, valve disease, left ventricular dysfunction, obesity, sleep apnea, and alcohol consumption [1]. Meta-analyses and prospective studies have established a relationship between alcohol consumption and AF. [2, 3] Several mechanisms for this relationship have been suggested, including hyper adrenergic state [18], impairment of vagal tone [19], a direct effect on myocardial structure [20], and an increase in intra-atrial conduction time [21]. However, no definitive mechanism has been completely elucidated.
We investigated the association of ADH1B and ALDH2 SNPs with AF in Japanese patients undergoing AF ablation. The frequency of the dysfunctional A allele of ALDH2 was lower in patients with AF than in controls. We also extracted the data from patients with lone AF to eliminate other confounding factors and re-analyzed the data. The frequency of the dysfunctional A allele of ALDH2 was also lower and the frequency of the slower alcohol metabolizing G alleles of ADH1B was higher in patients with AF than in non-AF controls. Contrary to our expectation based on the function of ALDH2 in reducing oxidative stress, the low frequency of the dysfunctional A allele of ALDH2 in patients with AF was an unexpected result. This is in contrast with the reports that the ALDH2 dysfunctional A allele was associated with coronary spastic angina and ischemic stroke in Ease Asian populations [22, 23]. We also noticed that in our study, frequency of ischemic heart diseases was higher in AF patients with AA and GA genotypes than those with the GG genotype-.
Considering that alcohol consumption can cause AF, it stands to reason that patients with the dysfunctional A allele of ALDH2, who have a low tolerance for alcohol consumption, were less likely to develop AF. Whereas people with the slower alcohol metabolizing G allele of ADH1B were more prone to be heavy drinkers which could lead to a higher risk of AF.
One of the limitations of this study is that quantitative information on alcohol consumption was not fully available for all patients with AF and controls Therefore, we could not determine whether the results were due to ALDH2 and ADH1B SNPs themselves or due to different amounts of alcohol intake. However, in patients with AF, when all the other physiological parameters were similar, we found that there was a significant linear correlation between ALDH2 genotype and mean alcohol intake. Liu J reported that ADH1B and ALDH2 SNPs were significantly associated with pathogenesis of hepatocellular carcinoma medicated through alcohol drinking [24]. Our limitation was that we were not able to analyze relationship between pathogenesis of AF and these 2 SNPs in stratified with amount of alcohol drinking.
From perspectives that mitochondrial ALDH2 reduce oxidative stress and the ROS is an important risk factor for AF, low dysfunctional allele of ALDH2 SNP in AF patients came as an unexpected result. The 4-HNE, accumulated in people with minor allele of ALDH2 SNP reported to be suppress protein kinase C (PKC) [25]. The mitochondrial ROS causes a reduction of sodium channel and the effect was prevented by inhibition of PKC [26]. The suppression of PKC in people with minor allele of ALDH2 SNP may work protective for AF occurrence. However, the precise mechanism, of different frequencies of ALDH2 SNP in AF or non-AF patients have not been elucidated. Future studies will be needed to clarify whether ALDH2 SNP by itself or alcohol consumption contributes to the occurrence of AF.
In patients with the slow alcohol metabolizing genotype of ADH1B, alcohol consumption tended to be higher and the right atrium refractory period was longer than in those with other genotypes. Slow metabolism of blood ethanol by a reduced alcohol elimination rate have been reported in Japanese alcoholic men with the minor G allele of ADH1B [27, 28]. Horakova et al. reported that the effects of ethanol on atrial I k1 were heterogeneous, and the heterogeneity of electrical properties might increase susceptibility to AF. [29] The decreased metabolic conversion of alcohol to acetaldehyde and the low elimination rate of alcohol in patients with the slow alcohol metabolizing allele of ADH1B may therefore be related to the occurrence of AF in Japanese and other East Asian populations.
There were some limitations in this study. The study was a retrospective, single-center study, and the numbers of cases and controls were small. The main limitation was that information on alcohol consumption was not fully available for both patients with AF and controls. Therefore, we could not clarify whether the relationships between AF and ALDH2 and ADH1B SNPs were caused by SNPs themselves or by different amounts of alcohol intake. It will be necessary to compare the frequencies of ALDH2 and ADH1B SNPs in nondrinking patients with AF and nondrinking controls and stratify the analysis according to alcohol consumption.
Another limitation was that all AF patients included in this study as the AF patients were patients who undergo catheter ablation. They may not necessarily represent all patients with atrial fibrillation. The AF patient undergone AF ablation may be serious patients whose duration of AF was long and resistant for anti-arrhythmic.
The other limitation was that the patients included in this study were all Japanese, we did not consider racial differences.
The interaction of ALDH2 with ADH1B SNPs in alcohol metabolism and multiple risk factors for AF complicated the effects of these SNPs on the occurrence of AF; a precise, large-scale cohort study will be needed to clarify the mechanism.
Conclusions
ALDH2 SNP rs671 A allele was negatively associated with AF and ADH1B SNP rs1229984 G allele was positively associated with AF. The ADH1B SNP rs1229984 may be a marker for susceptibility to AF, and prolonged metabolic conversion of alcohol to acetaldehyde may be related to the occurrence of AF in Japanese and other East Asian populations. A prospective cohort study with a larger sample size for each subgroup of genotypes and alcohol consumption data will be needed to confirm our results.
Abbreviations
- 4-HNE:
-
4-hydroxy-2-nonenal
- ADH1B :
-
Alcohol dehydrogenase
- AF:
-
Atrial fibrillation
- AH:
-
Right atria to his
- ALDH2 :
-
Aldehyde dehydrogenase 2
- CIs:
-
Confidence intervals
- EKG:
-
Electrocardiogram
- HV:
-
His to right ventricule
- OR:
-
Odds ratio
- SNPs:
-
Single nucleotide polymorphisms
References
Andrade J, Khairy P, Dobrev D, Nattel S. The clinical profile and pathophysiology of atrial fibrillation relationships among clinical features, epidemiology, and mechanisms. Circ Res. 2014;114:1453–68.
Kodama S, Saito K, Tanaka S, Horikawa C, Saito A, Heianza Y, Anasako Y, Nishigaki Y, Yachi Y, Iida KT, Ohashi Y, Yamada N, Sone H. Alcohol consumption and risk of atrial fibrillation: a meta-analysis. J Am Coll Cardiol. 2011;57(4):427–36.
Larsson SC, Drca N, Wolk A. Alcohol consumption and risk of atrial fibrillation. A prospective study and dose-response meta-analysis. J Am Coll Cardiol. 2014;64:281–9.
Yoshida A, Hsu LC, Yasunami M. Genetics of human alcohol-metabolizing enzymes. Prog Nucleic Acid Res Mol Biol. 1991;40:255–87. Review.
Wenzel P, Müller J, Zurmeyer S, Schuhmacher S, Schulz E, Oelze M, Pautz A, Kawamoto T, Wojnowski L, Kleinert H, Münzel T, Daiber A. ALDH-2 deficiency increases cardiovascular oxidative stress--evidence for indirect antioxidative properties. Biochem Biophys Res Commun. 2008;367:137–43.
Choi H, Tostes RC, Webb RC. Mitochondrial aldehyde dehydrogenase prevents ROS-induced vascular contraction in angiotensin-II hypertensive mice. J Am Soc Hypertens. 2011;5:154–60.
Kitagawa K, Kawamoto T, Kunugita N, Tsukiyama T, Okamoto K, Yoshida A, Nakayama K, Nakayama K. Aldehyde dehydrogenase (ALDH) 2 associates with oxidation of methoxyacetaldehyde; in vitro analysis with liver subcellular fraction derived from human and Aldh2 gene targeting mouse. FEBS Lett. 2000;476:306–11.
Suzuki Y, Fujisawa M, Ando F, Niino N, Ohsawa I, Shimokata H, Ohta S. Alcohol dehydrogenase 2 variant is associated with cerebral infarction and lacunae. Neurology. 2004;63:1711–3.
Harada S, Agarwal DP, Goedde HW. Aldehyde dehydrogenase deficiency as cause of facial flushing reaction to alcohol in Japanese. Lancet. 1981;2(8253):982.
Li H, Borinskaya S, Yoshimura K, Kal’ina N, Marusin A, Stepanov VA, Qin Z, Khaliq S, Lee MY, Yang Y, Mohyuddin A, Gurwitz D, Mehdi SQ, Rogaev E, Jin L, Yankovsky NK, Kidd JR, Kidd KK. Refined geographic distribution of the oriental ALDH2*504Lys (nee 487Lys) variant. Ann Hum Genet. 2009;73:335–45.
Gross ER, Zambelli VO, Small BA, Ferreira JC, Chen CH, Mochly-Rosen D. A personalized medicine approach for Asian Americans with the aldehyde dehydrogenase 2*2 variant. Annu Rev Pharmacol Toxicol. 2015;55:107–27.
Sovari AA. Cellular and molecular mechanisms of arrhythmia by oxidative stress. Cardiol Res Pract. 2016;2016:9656078. doi:10.1155/2016/9656078.
Ohnishi Y, Tanaka T, Ozaki K, Yamada R, Suzuki H, Nakamura Y. A high-throughput SNP typing system for genome-wide association studies. J Hum Genet. 2001;46:471–7.
Suzuki A, Yamada R, Chang X, Tokuhiro S, Sawada T, Suzuki M, Nagasaki M, Nakayama-Hamada M, Kawaida R, Ono M, Ohtsuki M, Furukawa H, Yoshino S, Yukioka M, Tohma S, Matsubara T, Wakitani S, Teshima R, Nishioka Y, Sekine A, Iida A, Takahashi A, Tsunoda T, Nakamura Y, Yamamoto K. Functional haplotypes of PADI4, encoding citrullinating enzyme peptidylarginine deiminase 4, are associated with rheumatoid arthritis. Nat Genet. 2003;34:395–402.
Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: a report from the American society of Echocardiography’s guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the European association of echocardiography, a branch of the European society of cardiology. J Am Soc Echocardiogr. 2005;18:144063.
Higuchi S, Matsushita S, Murayama M, Takagi S, Hayashida M. Alcohol and aldehyde dehydrogenase polymorphisms and the risk for alcoholism. Am J Psychiatry. 1995;152:1219–21.
Chen CH, Ferreira JC, Gross ER, Mochly-Rosen D. Targeting aldehyde dehydrogenase 2: new therapeutic opportunities. Physiol Rev. 2014;94:1–34.
Denison H, Jern S, Jagenburg R, Wendestam C, Wallerstedt S. Influence of increased adrenergic activity and magnesium depletion on cardiac rhythm in alcohol withdrawal. Br Heart J. 1994;72:554–60.
Maki T, Toivonen L, Koskinen P, Naveri H, Harkonen M, Leinonen H. Effect of ethanol drinking, hangover, and exercise on adrenergic activity and heart rate variability in patients with a history of alcohol induced atrial fibrillation. Am J Cardiol. 1998;82:317–22.
Preedy VR, Siddiq T, Why H, Richardson PJ. The deleterious effects of alcohol on the heart: involvement of protein turnover. AlcoholAlcoholism. 1994;29:141–7.
Habuchi Y, Furukawa T, Tanaka H, Lu LL, Morikawa J, Yoshimura M. Ethanol inhibition of Ca2 and Na currents in the guinea-pig heart. Eur J Pharmacol. 1995;292:143–9.
Mizuno Y, Harada E, Morita S, Kinoshita K, Hayashida M, Shono M, Morikawa Y, Murohara T, Nakayama M, Yoshimura M, Yasue H. Response to letter regarding article, “east Asian variant of aldehyde dehydrogenase 2 is associated with coronary spastic angina: possible roles of reactive aldehydes and implications of alcohol flushing syndrome”. Circulation. 2015;131:1665–73.
Sung YF, Lu CC, Lee JT, Hung YJ, Hu CJ, Jeng JS, Chiou HY, Peng GS. Homozygous ALDH2*2 Isan Independent Risk Factor for Ischemic Stroke in TaiwaneseMen. Stroke. 2016;47(9):2174–9.
Liu J, Yang HI, Lee MH, Jen CL, Hu HH, Lu SN, Wang LY, You SL, Huang YT, Chen CJ. Polymorphisms of ADH1B and ALDH2 and hepatitis B-related hepatocellular carcinoma. Cancer Epidemiol Biomarkers Prev. 2016;25(4):693–9. doi:10.1158/1055-9965.
Suzuki Y, Taniyama M, Muramatsu T, Higuchi S, Ohta S, Atsumi Y, Matsuoka K. ALDH2/ADH2 polymorphism associated with vasculopathy and neuropathy in type 2 diabetes. Alcohol Clin Exp Res. 2004;28(8 Suppl Proceedings):111S–6S.
Liu M, Liu H, Dudley Jr SC. Reactive oxygen species originating from mitochondria regulate the cardiac sodium channel. Circ Res. 2010;107(8):967–74.
Yokoyama A, Yokoyama T, Mizukami T, Matsui T, Kimura M, Matsushita S, Higuchi S, Maruyama K. Blood ethanol levels of nonabstinent Japanese alcoholic men in the morning after drinking and their ADH1B and ALDH2 genotypes. Alcohol Alcohol. 2014;49:31–7. doi:10.1093/alcalc/agt136.
Yokoyama A, Yokoyama T, Matsui T, Mizukami T, Matsushita S, Higuchi S, Maruyama K. Alcohol dehydrogenase-1B genotype (rs1229984) is a strong determinant of the relationship between body weight and alcohol intake in Japanese alcoholic men. Clin Exp Res. 2013;37:1123–32.
Horakova Z, Matejovic P, Pasek M, Hosek J, Simurdova M, Simurda J, Bebarova M. Effect of ethanol and acetaldehyde at clinically relevant concentrations on atrial inward rectifier potassium current IK1: separate and combined effect. J Physiol Pharmacol. 2016;67(3):339–51.
Acknowledgements
We thank the members of the clerical and medical staff at Hiroshima University Hospital for their assistance.
Funding
Dr. Y. Nakano was supported by JSPS KAKENHI Grant Number 26461130. Dr. Y. Kihara was supported by JSPS KAKENHI Grant Number 15 K09084.
This work is also supported by a grant from NIH, NIAAA11147 to Dr. Daria Mochly-Rosen.
Availability of data and materials
Not applicable.
Authors’ contributions
Conception and design of the study, analysis and interpretation of data, drafting of the manuscript: YN, YK, ERG, C-HC. Critical discussion and revision of the manuscript for its intellectual content: HO, KC, C-HC, DM-R, YK. Analysis and interpretation of the data: YO, AS, TT, HM, ST, MA, NH, CM, NO. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Written informed consent for this publication was obtained from all participants.
Ethics approval and consent to participate
The Institutional Ethics Committee of the Graduate School of Biomedical Science at Hiroshima University approved all procedures involving human genome use. Written informed consent for this investigation was obtained from all participants.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Nakano, Y., Ochi, H., Onohara, Y. et al. Genetic variations of aldehyde dehydrogenase 2 and alcohol dehydrogenase 1B are associated with the etiology of atrial fibrillation in Japanese. J Biomed Sci 23, 89 (2016). https://doi.org/10.1186/s12929-016-0304-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12929-016-0304-x