
Abstract
Background
Short stature is a common human trait. More severe and/or associated short stature is usually part of the presentation of a syndrome and may be a monogenic disease. The present study aimed to identify the genetic etiology of children with short stature of unknown origin.
Methods
A total of 232 children with short stature of unknown origin from March 2013 to May 2020 were enrolled in this study. Whole exome sequencing (WES) was performed for the enrolled patients to determine the underlying genetic etiology.
Results
We identified pathogenic or likely pathogenic genetic variants in 18 (7.8%) patients. All of these variants were located in genes known to be associated with growth disorders. Five of the genes are associated with paracrine signaling or cartilage extracellular matrix in the growth plate, including NPR2 (N = 1), ACAN (N = 1), CASR (N = 1), COMP (N = 1) and FBN1 (N = 1). Two of the genes are involved in the RAS/MAPK pathway, namely, PTPN11 (N = 6) and NF1 (N = 1). Two genes are associated with the abnormal growth hormone-insulin-like growth factor 1 (GH-IGF1) axis, including GH1 (N = 1) and IGF1R (N = 1). Two mutations are located in PROKR2, which is associated with gonadotropin-releasing hormone deficiency. Mutations were found in the remaining two patients in genes with miscellaneous mechanisms: ANKRD11 (N = 1) and ARID1A (N = 1).
Conclusions
The present study identified pathogenic or likely pathogenic genetic variants in eighteen of the 232 patients (7.8%) with short stature of unknown origin. Our findings suggest that in the absence of prominent malformation, genetic defects in hormones, paracrine factors, and matrix molecules may be the causal factors for this group of patients. Early genetic testing is necessary for accurate diagnosis and precision treatment.
Similar content being viewed by others


Background
Short stature is one of the most common reasons for attendance at pediatric endocrinology clinics, and it is defined as a height that is more than 2 standard deviations (SDS) below the mean for the same age, sex and population [1]. Linear growth in childhood is a process regulated and influenced by many factors involving many genes and influenced by genetics, hormones, nutrition and the environment [2, 3]. These factors influence the proliferation and differentiation of cells and/or the development and growth of bones, which are the main determinants of height. It is widely accepted that height is strongly regulated by genetic factors. Genetic factors account for 80% of human height outcomes and are suspected to be the main cause of individual growth differences [4]. Therefore, traditional assessments based on clinical findings, supplemented by laboratory and imaging studies, have not been able to determine the cause of growth disorders in these children.
The etiology of short stature may vary depending on the degree and type of growth retardation, alongside other accompanying clinical indications. In cases where a genetic mutation is suspected to be responsible for an individual’s short stature, it is recommended to use genetic testing as a means of obtaining an accurate diagnosis. This approach typically allows clinicians to identify any relevant genetic factors that may contribute to the individual’s condition. However, most patients with short stature are nonsyndromic, and the clinical symptoms associated with short stature are diverse and vary with age. Some of these patients showed a mild phenotype of well-characterized monogenic disorders, such as Noonan syndrome [5] and Leri-Weill dyschondrosteosis (SHOX gene defect) [6]. Another group of patients had alleles in genes that led to nonspecific phenotypes, such as those with heterozygous pathogenic alleles in the ACAN [7], NPR2 [8], NPPC [9], and IHH [10] genes. This becomes a real challenge when these patients have no clear phenotype and no obvious signs or symptoms. Alternatively, these studies may support the hypothesis that rare allelic variants, many of which are unique to single families, may have a greater influence on height determination and lead to short stature without significant effects from other systems. Thus, although the diagnostic role of clinical genetic testing for short stature has been established, the genes and rare variant alleles that contribute to short stature in patient populations have not been fully elucidated.
Whole exome sequencing (WES) has been successfully used to discover gene variations as monogenic causes of growth disorders. Approximately 25–40% of short stature children with previously unknown etiology can receive a molecular diagnosis using appropriate genetic testing techniques [3]. After appropriate modern genetic diagnostic procedures, these patients should be excluded from the diagnosis of short stature of unknown origin. This extreme heterogeneity in a population of unexplained short stature inevitably affects the choice of therapy with recombinant human growth hormone (rhGH). In addition, molecular diagnosis is important because it may guide treatment decisions, facilitate tailored management, and provide adequate genetic counseling. Therefore, the purpose of this study is to apply the WES method to evaluate the genetic etiology of growth disorders in children with short stature of unknown origin and to describe their clinical characteristics and response to rhGH therapy.
Methods
Subjects
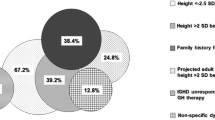
The subjects of this study were children with short stature of unknown origin who visited the Department of Endocrinology, Genetics and Metabolism, Affiliated Hospital of Jining Medical University from March 2013 to May 2020. The hospital is a comprehensive tertiary hospital with multiple disciplines, and all patients were evaluated by geneticists. Of the 1,165 children and adolescents with short stature, 90 patients were not evaluated by the two growth hormone stimulation tests and were excluded, the cause of short stature could be identified in 741 patients and there was no clear origin in 334 subjects. Among the 334 subjects with unknown origin of short stature, 102 DNA samples were not available, and thus, 232 short stature children and adolescents were finally included in the study. The participant selection process is shown as a flow chart in Fig. 1. The 232 children and adolescents with short stature were unrelated individuals. In total, there were 154 males and 78 females, and the average age was 10.4 ± 3.6 years. All subjects were selected based on the following inclusion criteria: the height of the participants was more than two SDS below the average height for the same race, age and sex; an appropriate birth weight for gestational age; and adequacy of GH was confirmed by at least two GH stimulation tests with concentrations > 10 ng/mL. We excluded patients with preterm birth, small for gestational age, and significant signs of malformation, including severe malformation, microcephaly, neurodevelopmental delay, intellectual disability, or skeletal dysplasia [11]. We did not exclude patients with minor malformations, defined as unusual morphological features found in the general population that have no serious medical or cosmetic significance for the affected individual [12]. In addition, participants with identified causes of short stature or chromosomal abnormalities or those for which DNA samples were not available were excluded from this study Figs. 2 and 3.

Flowchart of study subjects

Change in height of the study population after rhGH treatment. rhGH: recombinant human growth hormone

Height SDS of the study population after rhGH treatment. Height SDS: height standard deviation scores; rhGH: recombinant human growth hormone
Clinical evaluation
Clinical evaluations included anthropomorphic measurements, laboratory examinations and imaging evaluations. The height and weight of the anthropometric index were measured by a stadiometer (accuracy of 0.1 cm) and an electronic scale (accuracy of 0.1 kg). Height SDS was calculated according to the normal range of Chinese children [13]. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters and expressed as SDS based on the growth curve of Chinese children as a reference [14]. Puberty was assessed by physical examination based on Tanner stages. Participants with testicular volume less than 4 ml and no pubic hair in boys and no breasts and no pubic hair in girls were considered prepubertal [15]. Two GH stimulation tests (levodopa stimulation test and insulin hypoglycemia stimulation test) were performed to determine GH peaks. The serum GH concentration was determined by chemiluminescence (Access 2, Beckman Coulter, USA) with a sensitivity of 0.010 µg/L. Serum IGF-1 and insulin-like growth factor binding protein 3 (IGFBP-3) levels were measured by the chemiluminescence immunometric method (DPC IMMULITE 1000 analyzer, SIEMENS, Germany) with intra- and interassay CVs for IGF-1 of 3.0% and 6.2%, respectively, and intra- and interassay CVs for IGFBP-3 of 4.4% and 6.6%, respectively. IGF-1 SDS were calculated based on IGF-1 levels matched to healthy children and adolescents of the same age and sex [16]. Left hand and wrist X-ray bone age (BA) determination (Ysio SIEMENS, Germany) was conducted using the Greulich and Pyle method [17].
Genetic examination
Genomic DNA was extracted from peripheral blood using the Blood DNA Midi Kit (D3494-04, Omega Bio-Tek, GA, USA). WES was performed using an Agilent SureSelect V6 capture kit for enrichment of coding exonic sequences (Agilent Technologies, CA, USA), and the indexed DNA fragments were sequenced by BGISEQ-500 (BGI, Shenzhen, China) to achieve 100× average coverage with paired-end sequencing.
After the sequencing data were filtered and quality controlled, all clean reads were aligned to the GRCh37/hg19 assembly of the human genome with Burrows‒Wheeler Aligner software (BWA, version 0.7.15). Variant calling included single nucleotide polymorphisms (SNPs) and small insertions and deletions (InDels), which were detected using HaplotypeCaller of GATK (version 3.7). The resulting data (in variant call format –VCF) were annotated with ANNOVAR. The median average of the target bases was 147x, with 99% of the target bases having ≥ 10x coverage.
Evaluation of the genetic results
Based on data from the 1000 Genomes Project (http://www.ncbi.nlm.nih.gov/variation/tools/1000 genomes), Genome Aggregation Database (gnomAD: http://gnomad.broadinstitute.org/) and Exome Aggregation Consortium (http://exac.broadinstitute.org), rare nonsynonymous variants were selected, and common polymorphisms with a minor allele frequency (MAF) of 0.1% or above in the general population were excluded. The functional consequence of each variant was predicted by several in silico programs (SIFT, PolyPhen-2, Mutation Taster, LRT Prediction, CADD and M-CAP). Sanger sequencing was performed to validate the candidate variant identified. The pathogenicity of the variants identified during genetic analysis was classified according to the American College of Medical Genetics and Genomics/Association for Molecular Pathology (ACMG/AMP) guidelines [18].
Statistical analysis
Continuous variables are presented as the mean ± standard deviation or median (interquartile range). Categorical variables are displayed as numbers and percentages. To compare differences between two groups, Student’s t-test was used for normally distributed variables, the Kruskal-Wallis test was used for nonnormally distributed variables, and the chi-square test were used for categorical variables. Statistical analysis was performed with R 4.0.2 (https://www.R-project.org).
Results
The patient cohort
The clinical characteristics of this cohort are described in Table 1. WES was performed for a total of 232 children with short stature of unknown origin, of which of 154 (66.38%) were male and 78 (33.62%) were female. The average age and bone age of the selected participants were 10.4 ± 3.6 years and 8.8 ± 4.1 years, respectively. The mean height SDS of patients was − 2.76 ± 0.73. The height SDS of the patients with the gene variant was significantly lower than that of the patients without the gene variant (P = 0.023). All individuals showed sufficient GH, and the peak GH was 14.99 ± 4.50 ng/mL. The median IGF-1 SDS and IGFBP-3 levels were − 0.68 (-1.53-0.34) and 4.61 (3.66–5.63) µg/mL, respectively. The IGF-1 SDS of patients carrying the genetic variant was significantly lower than that of patients without the genetic variant (P = 0.038). Therefore, genetic testing is more suitable for patients with severe short stature and lower levels of IGF-1.
Genetic variants identified
For 7.8% of children in this cohort (18/232), pathogenic or likely pathogenic variants with potential clinical significance in genes with a known impact on growth were identified. Of these variants, seven were classified as pathogenic, and 11 were classified as likely pathogenic. All these variants were identified in genes already associated with growth disorders (Table 2): PROKR2 (N = 2), PTPN11 (N = 6), ANKRD11 (N = 1), NPR2 (N = 1), NF1 (N = 1), ACAN (N = 1), GH1 (N = 1), FBN1 (N = 1), COMP (N = 1), IGF1R (N = 1), ARID1A (N = 1), and CASR (N = 1). Only one of these mutations was a frameshift mutation. All other mutations were missense and predicted to be pathogenic by a variety of silico tools.
Clinical phenotypes
The phenotypic characteristics of the patients carrying a pathogenic or likely pathogenic mutation are shown in Table 3. In total, eighteen pathogenic or likely pathogenic variants from unrelated individuals were identified. Their height SDS ranged from − 2.03 SD to -3.94 SD. Nine of the eighteen patients had familial short stature (FSS), with the height of a father or mother below 160 cm or 150 cm, respectively. However, blood samples were obtained from the parents of only 5 patients. Parental testing using Sanger sequencing revealed that for 3 patients, the variants were inherited from their affected mother. For 1 patient, the variant was inherited from his affected father, and for 1 patient, the variant was a de novo mutation (Table 3). Additionally, one patient had a slightly advanced bone age at prepubertal age (chronological age was 3 years old and bone age was 4 years old for a patient with ACAN), whereas the majority of the patients had a markedly delayed bone age.
Five patients had rare genetic variants in genes (NPR2, ACAN, CASR, COMP, and FBN1) directly involved in paracrine signaling or the cartilage extracellular matrix in the growth plate. Patient #133 carried a heterozygous FBN1 mutation and presented with severely delayed bone age (BA-CA: -4 years) and additional phenotypic features, including viral encephalitis, sinus arrhythmia, and high arched palate. Patient #144 carried a heterozygous mutation in COMP (c.949G > T) and presented with short stature accompanied by skeletal dysplasia. His height SDS was − 3.05 SD. The height of his mother was 132 cm, and she presented with additional phenotypic features, such as limited knee mobility, lumbar spine tilted forward significantly, forearm flexion and metaphyseal dysplasia. These patients showed only a mild clinical phenotype and were within the normal range of body proportions, including the sit height/height and arm span/height (Table 3). The bone age x-ray evaluation for these patients showed no abnormalities, except for minor metaphyseal chondrodysplasia in patient #144, and further lumbar spine radiographs showed unnatural morphology, which indicated minor dysplasia.
Two patients, including one boy and one girl, carried the PROKR2 gene variant. The 14-year-old boy exhibited delayed development of secondary sex characteristics, a mid-parental height (MPH) of 176 cm, and a bone age delay of 1.5 years. The 5-years-old girl was still being followed up. She presented a MPH of 163 cm, and exhibited a significant delay in bone age (BA-CA: -2.5 years).
Seven patients had pathogenic variants in two genes involved in the RAS-MAPK pathway: PTPN11 (N = 6) and NF1 (N = 1). At the first evaluation, their clinical presentation was not sufficient to allow the diagnosis of Noonan syndrome (OMIM #163,950) or neurofibromatosis type 1 (OMIM #162,200). Patient #108 carried a heterozygous NF1 mutation and presented with 15 milk coffee spots with a diameter greater than 5 mm on the chest and underarms. His head circumference was in the normal range of 48.5 cm, and his academic performance was acceptable. However, he is now only 4 years old and needs follow-up monitoring. Patient #56, patient #68, patient #79, patient #91, patient #202 and patient #214 all carried mutations in PTPN11; these patients demonstrated different specific facial features, congenital heart anomalies or cryptorchidism.
Patient #77 carried a mutation in the ANKRD11 gene, which encodes an ankyrin repeat domain-containing protein, corresponding to the phenotype of KBG syndrome (OMIM#148,050) with an autosomal dominant inheritance pattern. Her height SDS was − 3.31 SD, BMI SDS was − 0.51 SD, peak GH concentration was 18.88 ng/mL, IGF-1 SDS showed a low level of -0.43 SD, and additional phenotypic characteristics included congenital heart disease and delayed bone age.
Patient #87 and patient #123 carried IGF1R and GH1 gene mutations, respectively; these genes are related to the abnormal growth hormone/insulin-like growth factor 1 (GH/IGF-1) axis. Patient #87 showed adequate IGF-1 and GH levels. The IGF-1 SDS was 0.57, and peak GH was 17.37 ng/mL. Short stature may be associated with IGF-1 insensitivity, and the clinical phenotype was high arched palate. Patient #123 carried the GH1 gene variant. This patient had sufficient GH with a peak GH of 24.23 ng/mL. The level of IGF-1 was low, and IGF-1 SDS was − 1.30. Partial GH insensitivity may be present in this patient.
Growth response to rhGH treatment
Of the 18 patients with a pathogenic or likely pathogenic variant, 4 received rhGH for 0.5 to 3.5 years (Figs. 2 and 3). The age range of these patients at rhGH treatment ranged from 4 to 12 years, and these patients showed varying degrees of catch-up growth during treatment with rhGH (Δ height SDS range: 0.07 SD to 0.34 SD). Among these four patients, one patient was treated for half a year, one patient was treated for 3.5 years, and two patients were treated for 2 years. Patient #133 carried the FBN1 gene variation, and after 0.5 years of treatment with rhGH, the SDS of height improved by 0.34 SD. rhGH treatment had been used for only 0.5 years in this patient; thus, conclusions about the efficacy of rhGH treatment could not be reached. Patient #68 and Patient #214 both carried the PTPN11 gene variant, and the rhGH treatment duration was 3.5 years and 2 years, respectively. For these patients, the height SDS only improved by 0.27 SD and 0.21 SD, respectively. In addition, during 2 years of rhGH treatment, there was no significant improvement in the height SDS (Δ height SDS: 0.07 SD) of patient #181, who carried the ARID1A variant.
Discussion
The present study evaluated the complex genetic etiology of short stature in a population of unrelated individuals using the WES method. From our cohort of 232 children with short stature of unknown origin at the time of diagnosis, 18 pathogenic or likely pathogenic mutations that were associated with growth disorders were identified. These genetic variants affect diverse pathways involved in growth, including the endocrine system, paracrine growth factors, extracellular matrix, and intracellular signaling molecules in the growth plate. Patients with different genetic variants showed significant differences in response to rhGH treatment. Early genetic diagnosis may lead to better clinical management and treatment choices.
Many children with short stature of unknown origin show mild clinical features that can be observed in some syndromes. However, these features are not sufficient to diagnose a specific syndrome. Therefore, some special syndromes with a wide range of clinical phenotypes, especially for patients with mild clinical features, may be misdiagnosed as idiopathic short stature. The final diagnosis may not be clear until molecular genetic and/or biochemical markers are identified. Recognizing the etiology of short stature and elucidating the gene-specific response to rhGH therapy is one of the major challenges facing pediatric endocrinology. Pathogenic or likely pathogenic variants were revealed in 7.8% of children with short stature in our study (18/232). This finding is similar to that of our previous study in which WES was performed for 93 patients with growth hormone deficiency (GHD); this study yielded a molecular diagnostic rate of 7.5% [19]. A recent review mentioned that genetic testing for short stature children of unknown etiology yielded a diagnosis rate of between 4% and 16%, which increased with the severity of short stature and the fact that the child had additional characteristics, such as deformations or intellectual disabilities [20].
The genetic variants we identified in this study were all heterozygous variants with an autosomal dominant pattern of inheritance. This finding is similar to that of a previously reported study by Ahn J et al., in which 14 of 144 patients with short stature were identified as carrying pathogenic or likely pathogenic variants, and all patients showed a dominant inheritance pattern [21]. In addition, autosomal recessive genetic disorders are also causes of short stature and may account for a relatively small proportion of short stature patients, especially for those with nonsyndromic short stature. A recent study of the genetics of short stature in China showed that the genetic diagnosis rate of patients with idiopathic short stature was 11.3%. Of these patients, 72% carried monoallelic variants consistent with the underlying autosomal dominant (AD) condition or disease feature, and 10% carried biallelic variants consistent with Mendelian expectations for an autosomal recessive (AR) condition [22]. In addition, in the above study, dual diagnosis of short stature was present in 0.5% of patients with syndromic short stature, while no dual diagnosis was found in patients with idiopathic short stature [22]. The lack of identification of genetic causes of short stature due to autosomal recessive disorders and dual diagnosis in the present study may be related to regional differences and the inclusion criteria for the patient population. In our previous genetic testing of GHD patients, no dual diagnosis or autosomal recessive genetic disease of short stature was identified [19].
The genetic causes of linear growth disorders identified in previous reports are highly heterogeneous, affecting a variety of cellular pathways. Furthermore, any regulatory mechanism that alters growth plate chondrogenesis may be a genetic cause of growth disorders [23]. A notable aspect of this study was the frequency of heterozygous mutations detected in genes previously associated with skeletal dysplasia (NPR2, ACAN, CASR, COMP, and FBN1), confirming the dose effect of cartilage matrix proteins in growth and development. In patients with short stature disorder of unknown origin in the present study, these gene variants showed a mild clinical phenotype, causing difficulties for accurate diagnosis. Among these gene variants, NPR2 and ACAN are more common in patients initially diagnosed with idiopathic short stature [24, 25]. In the present study, one case of a NPR2 gene variant and one case of a ACAN gene variant were identified. Patient #87 carried heterozygous frameshift mutations of NPR2 (c.2629_2630delAG); however, no significant skeletal phenotype was observed. Previous studies have shown that heterozygous mutations in NPR2 appear to be associated with mild and variable growth disorders without a distinct skeletal phenotype compared with homozygous or compound heterozygous mutations in NPR2 that cause severe short stature and body disproportion [26]. Patient #119 carried a heterozygous frameshift mutation in the ACAN gene, and the clinical characteristics showed slightly advanced bone age. A recent study noted that 47.4% of patients with ACAN variants in the Chinese population showed advanced bone age [27]. Functional aggregative proteoglycan haploid deficiency leads to premature maturation of hypertrophic chondrocytes and premature invasion of vascular cells and osteoblasts in the growth plate, which has been suggested as a potential mechanism for advanced bone age, premature growth cessation, and early epiphyseal fusion in patients with ACAN mutations [28, 29].
In this study, we separately identified two patients with rare variants p.Gly229Arg and p.Arg353Cys in PROKR2 who showed delayed development of secondary sexual characteristics. In addition, we also identified four patients with a common PROKR2 (p.Trp178Ser) variant. This variation was classified as pathogenic, including in other previous studies involving short stature [21]. However, we did not include the p.Trp178Ser in PROKR2 as a possible cause of short stature, since it has been described in several others clinical exomes with no mention to this phenotype. PROKR2 is traditionally known as a gene implicated in hypogonadism hypogonadotropic, involved in pituitary ontogenesis [30]. Additionally, some investigators have also suggested that the PROKR2 is associated with hypothalamic pituitary development and that children carrying this variant may present with short stature [31]. In addition, a PROKR2 variant was identified in patients born small for gestational age, without any facial deformity, with not catching up on growth [32]. In a previous study, an idiopathic short stature patient with a PROKR2 missense mutation was identified [21].
In our study, we also identified seven patients with pathogenic or likely pathogenic variants affecting the RAS-MAPK pathway. Six of the patients carried missense mutations in the PTPN11 gene, which is the most commonly mutated gene associated with Noonan syndrome (OMIM #163,950). Noonan syndrome is usually diagnosed by specific clinical criteria [33]. Facial features and/or typical heart malformations often raise doubts about the diagnosis. However, the phenotype of the patients analyzed in this study was mild, with only 2 patients having congenital heart disease, which is often associated with the clinical phenotype of Noonan syndrome. The characteristic facial appearance of Noonan syndrome varies somewhat across ages. However, with increasing age, the facial features of affected children become increasingly atypical. Mutations in the PTPN11 gene cause large clinical phenotypic variability, so milder mutations in the PTPN11 gene may result in less severe cases that are insufficient to meet the clinical diagnostic criteria for Noonan syndrome. If a patient has a mild or atypical presentation, genotyping could establish the diagnosis [33]. In addition, a previous study revealed atypical faces of Chinese Noonan syndrome patients and the lack of genetics training in China, which may have led to missed diagnoses in the past without next-generation sequencing [34].
Although most short stature patients can receive rhGH treatment to improve adult height, not all short stature patients are eligible or suitable for rhGH treatment. Clear molecular diagnosis of patients is crucial for deciding to continue/stop growth hormone therapy [35]. Individuals with growth hormone receptor (GHR) deficiency have a poor response to rhGH treatment. The short stature caused by abnormal growth plate-related genes makes it difficult to achieve a good therapeutic effect with rhGH treatment. For Bloom syndrome, rhGH treatment is contraindicated. For children who can be treated with rhGH, identifying genetic mutations can help determine the therapeutic effect of rhGH. If children homozygous for GH1 gene deletions are treated with rhGH, growth hormone antibodies are easily produced, leading to poor efficacy. After rhGH treatment, the levels of IGF-1 in children with IGFR deficiency can be significantly increased, but sensitivity decreases [31]. In this study, 4 out of 18 patients with pathogenic gene variants received rhGH treatment. However, one of the patients had only been using rhGH for 0.5 years. Thus, there is not enough evidence to draw any conclusions about the efficacy of the treatment. Two patients with Noonan syndrome were treated for 2 and 3.5 years, and only limited growth catch-up was observed. Several previous studies have reported a correlation between rhGH treatment response and genotype in Noonan syndrome, with patients carrying the PTPN11 pathogenic variant having a poor response to rhGH treatment [36, 37]. However, rhGH treatment has been reported to improve the height and growth rate in patients with Noonan syndrome, but there was no significant difference in rhGH treatment response in Noonan syndrome patients carrying the PTPN11 gene variant compared with those not carrying the PTPN11 gene variant [38]. In addition, a study by E-M Seok et al. showed that in rhGH-treated Noonan syndrome patients, the improvement in growth rate was significantly higher in patients carrying the PTPN11 gene variant than in those not carrying the PTPN11 gene variant [39]. This suggests that the response to rhGH treatment in Noonan syndrome patients carrying the PTPN11 gene variant is currently controversial. Further confirmation is needed with large samples and long-term follow-up cohort studies. However, most of the current research evidence supports a reduced rhGH treatment response in patients carrying the PTPN11 pathogenic gene variant [40]. The mechanism by which the PTPN11 gene variant leads to a reduced rhGH treatment response has not been elucidated but may be due to the role of SHP-2 as a negative regulator of GH receptor signaling [41, 42].
Several potential limitations of the present study should also be considered. Parental samples were not available for all patients; thus, some patients lacked trio testing, which should be performed in the future to improve the diagnostic rate. In addition, functional studies of pathogenic variants have not been conducted and can be added in future studies. Finally, in addition to the variants reported in this study, we cannot confirm the presence of other candidate variants in any patient. Even though we conducted WES for each patient, it is possible that some rare or private variants were missed due to the current limitations of sequencing technology. Furthermore, the interpretation of genetic variants is an ongoing and complex process, and new tools and information may become available in the future that can reclassify variants previously considered benign or of uncertain significance.
Conclusion
We performed genetic analysis of WES in Chinese children with short stature of unknown origin. Pathogenic or likely pathogenic genetic variants were identified in 18 of the 232 patients (7.8%). Genetic testing may help determine the underlying cause of short stature, helping to make an accurate diagnosis and treatment decisions. Even in the absence of malformation features, short stature may be caused by genetic defects in hormones, paracrine factors, matrix molecules, intracellular pathways, and fundamental cellular processes. Further studies should be conducted to test gene-specific GH reactivity as a necessary first step toward better personalization of short stature management.
Availability of data and materials
The data that support the findings of this study are not publicly available due to restrictions by General Data Protection Regulation (GDPR), but are available from the corresponding author on reasonable request.
Abbreviations
- WES:
-
Whole exome sequencing
- GH/IGF-1:
-
Growth hormone/insulin-like growth factor-1
- rhGH:
-
Recombinant human growth hormone
- IGFBP-3:
-
Insulin-like growth factor binding protein 3
- BA:
-
Bone age
- SNPs:
-
Single nucleotide polymorphisms
- InDels:
-
Insertions and deletions
- FSS:
-
Familial short stature
- MPH:
-
Mid-parental height
- NF1:
-
Type 1 neurofibromatosis
References
Polidori N, Castorani V, Mohn A, Chiarelli F. Deciphering short stature in children. Ann Pediatr Endocrinol Metab. 2020;25(2):69–79.
Inzaghi E, Reiter E, Cianfarani S. The challenge of defining and investigating the causes of idiopathic short stature and finding an effective therapy. Horm Res Paediatr. 2019;92(2):71–83.
Murray PG, Clayton PE, Chernausek SD. A genetic approach to evaluation of short stature of undetermined cause. Lancet Diabetes Endocrinol. 2018;6(7):564–74.
Vinkhuyzen AA, Wray NR, Yang J, Goddard ME, Visscher PM. Estimation and partition of heritability in human populations using whole-genome analysis methods. Annu Rev Genet. 2013;47:75–95.
Pannone L, Bocchinfuso G, Flex E, Rossi C, Baldassarre G, Lissewski C, Pantaleoni F, Consoli F, Lepri F, Magliozzi M, et al. Structural, functional, and clinical characterization of a novel PTPN11 mutation cluster underlying Noonan Syndrome. Hum Mutat. 2017;38(4):451–9.
Malaquias AC, Scalco RC, Fontenele EG, Costalonga EF, Baldin AD, Braz AF, Funari MF, Nishi MY, Guerra-Junior G, Mendonca BB, et al. The sitting height/height ratio for age in healthy and short individuals and its potential role in selecting short children for SHOX analysis. Horm Res Paediatr. 2013;80(6):449–56.
Gkourogianni A, Andrew M, Tyzinski L, Crocker M, Douglas J, Dunbar N, Fairchild J, Funari MF, Heath KE, Jorge AA, et al. Clinical characterization of patients with autosomal Dominant Short stature due to aggrecan mutations. J Clin Endocrinol Metab. 2017;102(2):460–9.
Vasques GA, Arnhold IJ, Jorge AA. Role of the natriuretic peptide system in normal growth and growth disorders. Horm Res Paediatr. 2014;82(4):222–9.
Hisado-Oliva A, Ruzafa-Martin A, Sentchordi L, Funari M, Bezanilla-López C, Alonso-Bernáldez M, Barraza-García J, Rodriguez-Zabala M, Lerario AM, Benito-Sanz S, et al. Mutations in C-natriuretic peptide (NPPC): a novel cause of autosomal dominant short stature. Genet Med. 2018;20(1):91–7.
Vasques GA, Funari M, Ferreira FM, Aza-Carmona M, Sentchordi-Montané L, Barraza-García J, Lerario AM, Yamamoto GL, Naslavsky MS, Duarte Y, et al. IHH gene mutations causing short stature with nonspecific skeletal abnormalities and response to growth hormone therapy. J Clin Endocrinol Metab. 2018;103(2):604–14.
Collett-Solberg PF, Ambler G, Backeljauw PF, Bidlingmaier M, Biller B, Boguszewski M, Cheung PT, Choong C, Cohen LE, Cohen P, et al. Diagnosis, Genetics, and therapy of short stature in children: a growth hormone Research Society International Perspective. Horm Res Paediatr. 2019;92(1):1–14.
Hoyme HE. Minor malformations. Significant or insignificant? Am J Dis Child. 1987;141(9):947.
Li H, Ji CY, Zong XN, Zhang YQ. Height and weight standardized growth charts for chinese children and adolescents aged 0 to 18 years. Chin J Pediatr. 2009;47(7):487–92.
Li H, Ji CY, Zong XN, Zhang YQ. Body mass index growth curves for chinese children and adolescents aged 0–18 years. Chin J Pediatr. 2009;47(7):493–8.
Wright C, Ahmed L, Dunger D, Preece M, Cole T, Butler G. Can we characterise growth in puberty more accurately? Validation of a new Puberty Phase Specific (PPS) growth chart. Arch Dis Child. 2012;97(Suppl 1):A100.
Xu S, Gu X, Pan H, Zhu H, Gong F, Li Y, Xing Y. Reference ranges for serum IGF-1 and IGFBP-3 levels in chinese children during childhood and adolescence. Endocr J. 2010;57(3):221–8.
Satoh M. Bone age: assessment methods and clinical applications. Clin Pediatr Endocrinol. 2015;24(4):143–52.
Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, Grody WW, Hegde M, Lyon E, Spector E. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17(5):405–24.
He D, Li Y, Yang W, Chen S, Sun H, Li P, Zhang M, Ban B. Molecular diagnosis for growth hormone deficiency in chinese children and adolescents and evaluation of impact of rare genetic variants on treatment efficacy of growth hormone. Clin Chim Acta. 2022;524:1–10.
Perchard R, Murray PG, Clayton PE. Approach to the patient with short stature: genetic testing. J Clin Endocrinol Metab. 2023;108(4):1007–17.
Ahn J, Oh J, Suh J, Song K, Kwon A, Chae HW, Oh JS, Lee HI, Lee MS, Kim HS. Next-generation sequencing-based mutational analysis of idiopathic short stature and isolated growth hormone deficiency in korean pediatric patients. Mol Cell Endocrinol. 2022;544:111489.
Fan X, Zhao S, Yu C, Wu D, Yan Z, Fan L, Song Y, Wang Y, Li C, Ming Y, et al. Exome sequencing reveals genetic architecture in patients with isolated or syndromic short stature. J Genet Genomics. 2021;48(5):396–402.
Yue S, Whalen P, Jee YH. Genetic regulation of linear growth. Ann Pediatr Endocrinol Metab. 2019;24(1):2–14.
Hauer NN, Sticht H, Boppudi S, Büttner C, Kraus C, Trautmann U, Zenker M, Zweier C, Wiesener A, Jamra RA, et al. Genetic screening confirms heterozygous mutations in ACAN as a major cause of idiopathic short stature. Sci Rep. 2017;7(1):12225.
Vasques GA, Amano N, Docko AJ, Funari MF, Quedas EP, Nishi MY, Arnhold IJ, Hasegawa T, Jorge AA. Heterozygous mutations in natriuretic peptide receptor-B (NPR2) gene as a cause of short stature in patients initially classified as idiopathic short stature. J Clin Endocrinol Metab. 2013;98(10):E1636–44.
Wang SR, Jacobsen CM, Carmichael H, Edmund AB, Robinson JW, Olney RC, Miller TC, Moon JE, Mericq V, Potter LR, et al. Heterozygous mutations in natriuretic peptide receptor-B (NPR2) gene as a cause of short stature. Hum Mutat. 2015;36(4):474–81.
Lin L, Li M, Luo J, Li P, Zhou S, Yang Y, Chen K, Weng Y, Ge X, Mireguli M, et al. A high proportion of novel ACAN mutations and their prevalence in a large cohort of chinese short stature children. J Clin Endocrinol Metab. 2021;106(7):e2711–9.
Lauing KL, Cortes M, Domowicz MS, Henry JG, Baria AT, Schwartz NB. Aggrecan is required for growth plate cytoarchitecture and differentiation. Dev Biol. 2014;396(2):224–36.
Domowicz MS, Cortes M, Henry JG, Schwartz NB. Aggrecan modulation of growth plate morphogenesis. Dev Biol. 2009;329(2):242–57.
Zhao Y, Wu J, Jia H, Wang X, Zheng R, Jiang F, Chen DN, Chen Z, Li JD. PROKR2 mutations in idiopathic hypogonadotropic hypogonadism: selective disruption of the binding to a Gα-protein leads to biased signaling. FASEB J. 2019;33(3):4538–46.
Liang Y, Luo XP. Challenges and opportunities for genetic diagnosis of children with short stature. Chin J Pediatr. 2020;58(6):443–6.
Toni L, Plachy L, Dusatkova P, Amaratunga SA, Elblova L, Sumnik Z, Kolouskova S, Snajderova M, Obermannova B, Pruhova S et al. The genetic landscape of children born small for gestational age with persistent short stature (SGA-SS). Horm Res Paediatr. 2023 (published online ahead of print).
Roberts AE, Allanson JE, Tartaglia M, Gelb BD. Noonan syndrome. Lancet. 2013;381(9863):333–42.
Li X, Yao R, Tan X, Li N, Ding Y, Li J, Chang G, Chen Y, Ma L, Wang J, et al. Molecular and phenotypic spectrum of Noonan syndrome in chinese patients. Clin Genet. 2019;96(4):290–9.
Wit JM, Oostdijk W, Losekoot M, van Duyvenvoorde HA, Ruivenkamp CA, Kant SG. MECHANISMS IN ENDOCRINOLOGY: novel genetic causes of short stature. Eur J Endocrinol. 2016;174(4):R145–73.
Rodríguez F, Gaete X, Cassorla F. Etiology and treatment of Growth Delay in Noonan Syndrome. Front Endocrinol (Lausanne). 2021;12:691240.
Ferreira LV, Souza SA, Arnhold IJ, Mendonca BB, Jorge AA. PTPN11 (protein tyrosine phosphatase, nonreceptor type 11) mutations and response to growth hormone therapy in children with Noonan syndrome. J Clin Endocrinol Metab. 2005;90(9):5156–60.
Choi JH, Lee BH, Jung CW, Kim YM, Jin HY, Kim JM, Kim GH, Hwang JS, Yang SW, Lee J, et al. Response to growth hormone therapy in children with Noonan syndrome: correlation with or without PTPN11 gene mutation. Horm Res Paediatr. 2012;77(6):388–93.
Seok EM, Park HK, Rho JG, Kum CD, Lee HS, Hwang JS. Effectiveness of growth hormone therapy in children with Noonan syndrome. Ann Pediatr Endocrinol Metab. 2020;25(3):182–6.
Yart A, Edouard T. Noonan syndrome: an update on growth and development. Curr Opin Endocrinol Diabetes Obes. 2018;25(1):67–73.
Chen Y, Wen R, Yang S, Schuman J, Zhang EE, Yi T, Feng GS, Wang D. Identification of Shp-2 as a Stat5A phosphatase. J Biol Chem. 2003;278(19):16520–7.
Stofega MR, Argetsinger LS, Wang H, Ullrich A, Carter-Su C. Negative regulation of growth hormone receptor/JAK2 signaling by signal regulatory protein alpha. J Biol Chem. 2000;275(36):28222–9.
Acknowledgements
We are grateful to all patients for their participation in this study.
Funding
This work was supported by the Research Fund for Lin He’s Academician Workstation of New Medicine and Clinical Translation in Jining Medical University (JYHL2018FZD03). The funder had no role in study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Q.Z. carried out the studies and drafted the manuscript. Y.L. and Q.S. provided all patients’ clinical information. C.Z. and S.K. helped with the formal analysis. W.Y. revised the manuscript. B.B. and M.Z. participated in the concept and design of the study, revising it critically for important intellectual content and final approval of the version to be published. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Human Ethics Committee of the Affiliated Hospital of Jining Medical University (2019C003, Jining, China). Written informed consents to participate were obtained from all the participants or the parents of the participants under the age of 16.
Consent for publication
Written consent was provided from all the participants for publication of their clinical data.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhao, Q., Li, Y., Shao, Q. et al. Clinical and genetic evaluation of children with short stature of unknown origin. BMC Med Genomics 16, 194 (2023). https://doi.org/10.1186/s12920-023-01626-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12920-023-01626-4