
Abstract
Background
As dogs age, they face various health challenges, and preventive care may be overlooked, impacting their quality of life. Frailty, a concept established in human medicine, has recently been applied to dogs using validated tools like the frailty index and frailty phenotype. This study aims to characterize frailty in senior pet dogs and investigate associated factors. To achieve this goal, 88 apparently healthy dogs, as reported by their owners, voluntarily participated in thorough consultations. These consultations included supplementary examinations such as urinary analyses, hematological assessments, and blood biochemistry. Additionally, owners completed questionnaires addressing their dog's overall health, cognitive and locomotor status, as well as their own attachment to the dog and personality traits. Subsequently, each dog was classified as robust or frail based on the presence of multiple criteria out of a set of five. All collected data underwent preliminary screening by a multiple factorial analysis, followed by binomial logistic regression to model frailty.
Results
The final population consisted of 74 dogs, with a frailty prevalence of 41.9% (95% CI: 30.5 – 53.9). In the statistical analysis, older age of the dog, lower owner attachment score, lack of regular deworming, and a disparity in extraversion between owner and dog were identified as contributing factors to frailty.
Conclusions
This study emphasizes the importance of regular deworming and strong owner-pet attachment in reducing frailty in dogs. It underscores the significance of proactive pet care and highlights the complex relationship between owner-dog personalities and canine frailty. This research advocates for a holistic approach that considers both human and canine traits to promote better health outcomes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
As companion dogs age, they may develop various health issues that can significantly impact their quality of life and lifespan. These health challenges include, in particular, cardiopulmonary [1], metabolic [2], renal [3], and dental diseases [4], in association with the emergence of issues like sarcopenia and cachexia [5]. Despite the recommendation for annual senior check-ups with additional exams [6], the importance of these preventative measures may not be fully appreciated by dog owners and veterinarians. This oversight can lead to missed opportunities for early intervention and care, potentially altering the health trajectory of these aging dogs and thus reducing their life expectancy and their comfort of life.
These health issues are particularly prevalent in frail individuals, who experience a decline in physiological resilience [7]. The concept of frailty, well-established in human medicine since 2001 [8], denotes a state of decreased autonomy associated with increased comorbidities and a reduced lifespan [9]. This concept has been recently extended to dogs [10, 11]. While a recent review identified 36 frailty detection tools for humans [12], only three have been validated for dogs [10, 11, 13]. These three tools include the frailty index of Banzato et al., which is a quantitative score (from 0 to 1) that increases with frailty severity [13] and two frailty phenotype assessment tools: the Hua phenotype [10] and the Lemaréchal phenotype [11]. These phenotypes categorize dogs as frail, robust, or, in some cases, pre-frail, based on five key criteria: weakness, exhaustion, low physical activity, chronic undernutrition, and poor mobility [10, 11]. Adapted from human studies [8], these phenotypes differ primarily in their methodology. The Hua phenotype relies on owner-reported data for assessing exhaustion and low physical activity, while the Lemaréchal phenotype uses exclusively quantitative measures, which require more time and resources, making it less practical for routine use in canine care. Both tools have demonstrated an association with survival outcomes [10, 11]. While Banzato et al.’s frailty index and Lemaréchal phenotype have been tested in a population of pet dogs [14], the Hua phenotype has only been applied to guide dogs.
In addition to identifying frailty, improving the comfort of older dogs and increasing their life expectancy in good health requires a better understanding of the parameters associated with frailty in the canine species. A study of the canine population would enable us to identify the factors associated with frailty, as has already been done extensively in human studies [15]. In humans, these factors include sociodemographic (age, ethnicity, family dysfunction), physical (obesity, activity level), biological (serum uric acid), lifestyle (diet), and psychosocial aspects (personality, depression) [15,16,17]. Currently, only dog age and female sex have been linked to canine frailty [10].
So this study aimed to achieve two main objectives: firstly, to characterize frailty in a cohort of apparently healthy senior pet dogs, and secondly, to investigate factors associated with the frailty phenotype. Given the parallels between dog aging and human aging [18], the authors hypothesized that similar broad categories of factors could be associated with frailty in dogs. Therefore, a comprehensive approach involving thorough epidemiological and clinical evaluations was adopted. In addition, the results could provide interesting insights on human aging as dogs are recognized as a valuable model due to their similar illnesses, shared lifestyle patterns with their owners (including material and social environments, and activity levels), and their capacity for human-like social relationships [19, 20].
Material and methods
This study has received approval from the Animal Ethical Committee "SCIENCE ET SANTE ANIMALES N°115" in Toulouse, France, under the reference number SSA_2022_014, and the Research Ethical Committee “Comité d’éthique et de la recherche – CER” in Toulouse, France, under the reference number 2023_719.
Animals
The recruitment of dogs for the study was conducted on a voluntary basis using a multi-channels approach. This included leveraging the social media platforms of the Veterinary School of Toulouse, sending email invitations to dog owners who had previously visited the school and consented to receive emails, and promoting the study through an online article in a Toulouse city news outlet. Additionally, a print article was published in a local newspaper, and flyers were distributed to some companies and institutes in Toulouse. The recruitment campaign took place in August 2023 and explicitly sought dogs aged 8 years or over, weighing more than 20 kg and presenting no overt signs of health issues. Owners were required to confirm that their dogs were not receiving any ongoing treatments or suffering from chronic illnesses. To encourage participation, the campaign specified that the consultation would be free of charge and would include complimentary urine analysis and blood tests. Participants were also informed that they would receive a 14kg-bag of premium dog food as a token for appreciation for their participation. Due to limited participation, dogs aged 7 years or older and weighing more than 19 kg were finally also welcomed into the study. Owners were instructed to ensure their dogs fasted for a minimum of 8 h before the consultation.
Questionnaires
The questionnaires were administered in two sessions: initially, sent by email prior to the consultation, and subsequently during the consultation (in person). This approach ensured that at least 24 h elapsed between the two completions, aiming to prevent owner fatigue and promote focused and concentrated responses [21].
The pre-consultation questionnaire filled by the owners asked details about the dog's diet including the World Small Animal Veterinary Association (WSAVA) diet history form [22], assessment of fecal score based on the Purina Fecal Scoring Chart [23], a scoring system ranging from 1 (hard dry stool) to 7 (liquid stool), veterinary care received, medical history, and an assessment of the senior dog’s health status. The veterinary care section addressed potential medical treatment as well as preventive treatment such as internal and external antiparasitic. A dog was considered as "regularly dewormed" if deworming treatment was administered at least every three months, aligning with the recommendations outlined in groups B and C for treatments by ESCCAP (European Scientific Counsel Companion Animal Parasites) [24]. This questionnaire is provided in Additional File 1.
Then, during the consultation, owners were prompted to provide responses to several established questionnaires. These included the Canine Cognitive Dysfunction Rating scale (CCDR) [25], the Canine Brief Pain Inventory (CBPI) [26, 27], the Big Five inventory (BFI) for themselves [28] and an adaptation of this latter, the succinct Monash Canine Personality Questionnaire (MCPQ-R), for their dogs [29]. The BFI questionnaires chosen allow for comparisons across two dimensions that are comparable between humans and dogs: extraversion and neuroticism [30]. However, the BFI is susceptible to subject bias, which is the systematic tendency of a subject to assign high or low scores [31]. To mitigate this bias, pair comparison is an effective method, as it reduces the impact of noise on raw opinion scores [31]. This can be achieved by calculating the difference between two scores [32]. Therefore, the variable analyzed during statistical analysis was the difference in personality traits between the owner and their dogs, calculated as the owner’s score minus the dog’s score for each trait. Additionally, they were asked to complete the Lexington Attachment to Pet Scale (LAPS) [33] and provide information about their personal circumstances and the living environment of their dog (Additional File 1). Owners were categorized as having "lower attachment" to their dog if their score on the LAPS fell below the median score.
Veterinary consultation
The veterinary consultation, including a thorough examination, required a complete hour and was conducted consistently by the same veterinarian for all dogs, following the same order. The examination was based on a holistic assessment, comprising a 9-point body condition scoring [34], muscle condition evaluation [35], weight measurement using a standardized scale (Precia Molen – Access, France, max 150 kg, accuracy 50 g). Dental health was assessed through tartar [36], gingivitis [37], and periodontal disease [38] scorings, with the average of these three scores used as the “buccal score” in the statistical analysis. Additionally, the examination included a thorough dermatological examination with skin scoring [39], an ophthalmological assessment, a neurological evaluation, and a comprehensive orthopedic examination. At the end of the consultation, each dog participated in a 6-min walk test, conducted at their own pace, accompanied by both the veterinarian and their owner [40]. The physical examination recording form is available in Additional File 2.
Exclusion criteria
Since all participating owners received non-negligible benefits, we anticipated that some might present dogs that were not in apparent good health. Consequently, we excluded dogs exhibiting clear signs of illness that should be noticeable to an average owner, such as labored breathing, obesity, or cachexia. These signs were noted during the distance examination. Additionally, during the consultation, we asked owners about any health issues that had been a concern or were currently concerning. If an owner reported that a condition was ongoing, the dog was excluded from the study.
Sampling and analysis
Urine samples were collected via spontaneous miction at the beginning of the consultation. Urinary dipstick analysis (Combur 10 Test, COBAS, Roche Diagnostics Ltd, Rotkreuz, Switzerland), determination of urine specific gravity (USG) using a refractometer (Indiko Plus, ThermoFisher Scientific, Massachusetts, USA), and sediment examination in case of dipstick abnormalities were conducted promptly upon sample collection.
Blood was collected from the cephalic vein on a 3 mL lithium heparin tube and a 3 mL EDTA tube, at the beginning of the consultation and after urine collection. The blood of the heparinized tube was centrifugated (2,000 RCF for 10 min at room temperature (22 °C)) to isolate the plasma. In total, 18 parameters were evaluated using the same automated chemistry analyzer (Ikems; MS Labos, Osny, France): albumin (ALB), total proteins (TP), alkaline phosphatase (ALP), gamma glutamyl transferase (GGT), alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBIL), phosphates (PHOS), uric acid (UA), urea (BUN), creatinine (CR), amylase (AMY), creatine kinase (CK), Lactate dehydrogenase (LDH), total calcium (CA), glucose (GLU), total cholesterol (TC), and triglycerides (TG).
Before hematologic analysis, EDTA tubes were kept at room temperature (22 °C) and placed on an agitator (Specie mix, Drew Scientific Inc) for 20 min. They were then gently inverted to ensure homogenization. Samples with visible or microscopic clots were excluded. Measurements were conducted within 2 h of sampling using the Sysmex XN-V (Sysmex Corporation, Japan) according to the manufacturer's instructions, with settings for "dog" [41]. The following variables were analyzed for this study: red blood cell counts (RBC), hematocrit (HCT), hemoglobin concentration (HGB), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), fluorescence platelet counts (PLT-F), reticulocyte count (RET), white blood cell count (WBC), neutrophils (NEUT), lymphocytes (LYMPH), monocytes (MONO), eosinophils (EO), and basophils (BASO) counts.
Assessment of the frailty phenotype
The frailty phenotype was evaluated using the method developed by Hua et al. [10], considering five criteria: weakness (moderate or severe generalized amyotrophy assessed by the veterinarian [35]), exhaustion (reported physical intolerance by owners), low level of physical activity (owner-reported), chronic undernutrition (assessed by poor coat quality by the veterinarian), and impaired mobility (gait problems assessed by the veterinarian during the consultation or the 6-min walk test). A dog was classified as frail if it met two or more of these criteria.
Statistical analysis
Data were gathered using the software Sphinx iQ3 (Le Sphinx, Chavanod, France) and then extracted and analyzed using R software, version 4.2.2 [42]. The full dataset comprised 102 variables other than frailty phenotype, distributed across several categories. The first category consisted of 29 variables related to the dog (lifestyle, veterinary care, and information about the owner). The second category comprised 11 variables pertaining to the dog's medical history. The third category included 29 variables related to the dog's health. Lastly, the dataset included 33 variables being results from urinary and blood analyses.
A selection process was undertaken first, in order to lower the number of variables potentially relevant to model frailty. Traditional methods like univariable analysis are often employed for this purpose; however, they may oversimplify the intricate relationships between explanatory variables. Therefore, Multiple Factor Analysis (MFA) with the FactoMineR package in R 4.2.2 was opted for [43]. MFA is a robust multivariable analysis technique adept at handling datasets comprising both qualitative and quantitative variables, allowing for comprehensive exploration of interconnections within the data [44].
The 103 variables considered in the MFA were categorized into three groups: quantitative parameters (n = 64), qualitative variables (n = 38), and the frailty phenotype (binary variable: Frail and Robust). A comprehensive list of all variables is provided in Additional File 3. This approach allowed a differentiation between frail and robust individuals. The most discriminant variables were identified by visualization of the squared cosine values (cos2) and selected by the elbow method, which involved stopping the selection when a drastic decrease in cos2 value occurs. The subsequently selected variables have been used for the next step of the analysis.
For the second stage, the selected variables were integrated as explanatory variables in a logistic regression model considering frailty as binary outcome variable. The reference category was dogs considered as robust. Starting with the full model (including all the variables selected through MFA), a stepwise backward and forward selection process based on the Akaike’s Information Criterion (AIC) was applied to select the most parsimonious model. Multicollinearity was checked using variance inflation factor (VIF) values [45]. Type III ANOVA was used to obtain p-values. The final statistical significance was defined as p-value < 0.05.
Results
Population description and selection
Out of the 100 owners who completed the pre-consultation questionnaire, only 74 dog-owner pairs were included in the final analysis (Fig. 1). The primary reasons for exclusion were failure to attend the consultation and dogs displaying obvious signs of illness that should have been apparent to a typical owner. The 74 dogs kept had a median age of 9 years [range: 7 – 14] and a median weight of 29.4 kg [range: 19.3 – 56.3]. Complete description of the study population, including results from clinical examinations, blood and urinary tests, and questionnaires, can be found in Additional file 3.

Inclusion process of the dogs. A total of 100 dog owners completed the recruitment form for the study, of which 88 attended the consultation. Among those who did not attend, 5 owners did not respond upon recontact, 4 owners were unable to make it due to time constraints, and 3 owners reported that their dogs' health had deteriorated since the initial contact. From the 88 dogs presented at the consultation, 14 were excluded from the analysis: one owner declined the blood test, one dog had a purulent wound that affected blood test results, and 12 dogs were deemed not "apparently healthy" based on clinical observations (including 3 with labored breathing, 2 with multiple large masses, 2 obese dogs, 1 exhibiting all visible signs of hypothyroidism, 1 experiencing weekly seizures for 4 months, 1 previously diagnosed with cancer, 1 cachectic dog, and 1 displaying all visible signs of Cushing's syndrome)
Frailty phenotype
Out of 74 dogs assessed, 16 dogs did not meet any frailty criteria, while 27 displayed one criterion, 17 had two criteria, 12 had three criteria, 0 had four criteria and 2 dogs exhibited five criteria (Fig. 2). So, 41.9% (95% CI: 30.5 – 53.9) were classified as frail. Low physical activity (n = 30) was the most prevalent frailty criterion, followed by exhaustion (n = 27), undernutrition (n = 24), weakness (n = 17), and poor mobility (n = 9). Weakness and poor mobility are criteria that are mostly expressed in association with one of the three most prevalent (Fig. 2).

Venn diagram of the criteria of frailty met by the dogs. 16 dogs did not meet any frailty criteria, while 27 displayed one criterion, 17 had two criteria, 12 had three criteria, 0 had four criteria and 2 dogs exhibited the five criteria. Low physical activity (n = 30) was the most prevalent frailty criterion, followed by exhaustion (n = 27), undernutrition (n = 24), weakness (n = 17), and poor mobility (n = 9)
Factors associated with frailty
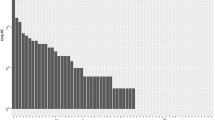
Including all results, MFA allowed a discrimination of the 74 dogs according to the frailty phenotype. Indeed, the first dimension, explaining 8.3% of the total inertia, opposed frail (positive coordinates) to robust dogs (negative coordinates) (Fig. 3). The fifteen most structuring variables for this first dimension (based on cos2 values) are presented in descending order in Fig. 4. Among them regular deworming contributed more than the others, the second position was for age of the dog. The owner's attachment to their dogs and the type of household (house or flat) came in third and fourth respectively. The other contributions, including some biochemical parameters (amylase, CK, LDH), were relatively similar.

Individual factor map of the Multiple Factor Analysis (MFA)

Cos2 values of the 15 first variables structuring Dimension 1, excluding frailty phenotype
All these 15 variables were initially included in the full logistic regression model and 7 variables remained after the stepwise backward and forward selection process. These variables are described for the two groups of interest (frail vs robust) in Additional File 3. As shown in Table 1, absence of regular deworming (OR: 5.85, p = 0.011) and lower attachment score of the owner (OR: 3.91, p = 0.042) were strongly associated with frailty. Older age of the dog (OR: 1.68, p = 0.031) was moderately associated with frailty, while difference in extraversion (owner – dog) (OR: 1.06, p = 0.023) had a minimal effect size. Despite a p-value < 0.05, amylase had no effect on frailty status (OR: 1.00, p = 0.046).
Discussion
With the canine population aging [6, 46], it is increasingly important for veterinarians and pet owners to have a thorough understanding of the factors associated with frailty to ensure healthy aging. In populations of active and nondisabled dogs, the frailty index, which relies on the enumeration of disabilities and diseases, often exhibits low values and limited variability [47]. As a result, its efficacy as a tool for assessing frailty in such cohorts is diminished. Consequently, the frailty phenotype emerges as a superior alternative for studying frailty in these populations [47]. In the current study, we selected the Hua phenotype due to its clinical applicability. To encompass the potential bias of subjectivity described with this latter [10], all the evaluations were performed by the same veterinarian. Our findings establish an association between frailty and age in dogs, thereby validating the effectiveness of the chosen assessment tool within this population [14].
The prevalence of frailty in our population (41.9%) was higher than the prevalence reported in previous studies: 8.6% with Hua phenotype and 17% with Lemaréchal phenotype [10, 11]. Several factors differed between the studied dog populations and may account for this discrepancy. First, our study included a range of breeds and mixed-breed dogs unlike prior studies focusing only on retriever breeds. This selection strategy precludes genetic control [10]; nevertheless, our intention was to capture the diversity inherent in the pet dog population. Moreover, Hua et al. (2016) conducted their study only on guide dogs, still in active service, which are generally subject to rigorous monitoring compared to pet dogs. In addition, they were found to exhibit a superior quality of life characterized by increased levels of physical activity and enhanced social interactions [48], factors playing a pivotal role in mitigating frailty. Then, the age distribution of the study population should also be considered to explain the prevalence of frailty. Hua et al. (2016) described a population with the same median age (9 years) but with values ranging from 5 to 13 years compared with 7 to 14 years in our study. Finally, the voluntary nature of our recruitment strategy may have attracted owners concerned by their dogs and who noticed changes in their senior dog. Thus, our study population may overestimate the prevalence of frailty in elderly dogs. In human, the literature on the topic is more abundant and a large variation in frailty prevalence is described, from 4.0% to 59.1% [16, 49, 50]. Interestingly, in a study where participants were recruited on a voluntary-basis, the prevalence of frailty was closer to our findings: 31.8% [16].
Characterization of frailty phenotype in our population reveals an intriguing disparity among the five criteria of frailty, with prevalence ranked as follows: low physical activity > exhaustion > undernutrition > weakness > poor mobility. The most prevalent criteria could be the earliest or precursors. For instance, low physical activity may lead to poor mobility [51], while undernutrition could result in weakness [52]. However, we cannot ascertain causality or the reasons behind the varying prevalence of these criteria in this study; longitudinal studies are required for such conclusions. Nonetheless, this is an interesting avenue, as identifying early criteria could enable veterinarians to identify dogs at risk of frailty and potentially guide their aging trajectory towards robust aging.
The other main goal of the current study was to identify factors associated with frailty in dogs. Among all the epidemiological and clinical variables evaluated here, a regular deworming and a higher level of attachment were the most associated with a reduced propension of being frail, highlighting the key role that owners play in their dog's health and well-being. The association between current frequent deworming and robustness in dogs raises intriguing questions regarding causality. Given the observational nature of this study, it is possible that owners reduce the frequency of deworming when their dogs begin to show signs of frailty. It is also conceivable that owners who exhibit greater attentiveness to their pets may be more inclined to adhere to regular deworming practices. Alternatively, the observed effect could be attributed to the direct impact of deworming on the health of the dog, potentially mitigating factors contributing to frailty. Common canine parasites in France (Toxocara canis, Echinococcus granulosus, and Dipylidium caninum) are not typically associated with significant health effects in adult dogs [24]. Interestingly, there is even a growing interest in human medicine regarding restorative helminth therapy for its potential anti-inflammaging effects [53]. To explore this further, future studies on aging dogs should incorporate questionnaires about the animal’s deworming history and fecal explorations (parasites, microbiota, inflammatory markers). In the meantime, veterinarians should still strongly recommend regular deworming for older dogs, at least every three months in France, to ensure optimal health and well-being [24].
Since the domestication, humans and dogs live and evolve side by side. The human-canine bond is more and more explored but mainly through the benefits of owning a dog for humans. For example, for elderly individuals, having a pet bring companionship, enhance physical, mental health and social facilitation [54,55,56]. From the dog's perspective, this study is the first to emphasize the critical role that owners play in maintaining the robustness of senior dogs. This finding resonates with prior research indicating that owners who share a strong emotional bond with their dogs tend to engage in more physical activities together [57], are more inclined to provide veterinary care (including preventative measures) [58,59,60], and maintain hygiene care standards [60]. Consequently, these dogs generally exhibit better health [61] and enjoy an enhanced quality of life [62]. Considering these myriad benefits, it stands to reason that the outcome would manifest as more robust senior dogs. However, it is equally plausible that a frail dog, due to its reduced interactivity, might lead to decreased attachment from the owner.
Some studies have found links between personality and frailty in humans [17], with two indicating that higher extraversion is associated with lower frailty [63, 64], likely due to its association with increased physical activity [65]. However, there is limited research on the impact of non-human animal personality on their health [66]. In the actual study, a greater gap in extraversion scores between owners and dogs was slightly linked to increased frailty in this canine cohort. Both human extraversion (outgoing, friendly, energetic, talkative) and canine extraversion (energetic, hyperactive, active, restless, lively, excitable) are linked to energy levels. When an owner is more extraverted than their dog, they may perceive their dog as less active because of the mismatch in energy levels. Since activity level is a criterion in the frailty phenotype studied here, this perception could bias the assessment of the dog's actual activity potentially leading to a higher likelihood of classifying the dog as “frail.” Nevertheless, it's possible that the owner's higher extraversion could influence the dog’s health, as previous studies have shown that extraverted owners with active social lives may exhibit lower attachment and caregiving behaviors toward their dogs [62, 67]. Conversely, it is also plausible that frailty in dogs could contribute to a decrease in their extraversion scores. In any case, the study of psychology of both dog and owner holds significant importance in assessing frailty in dogs. In human research, tools integrating psychological factors have proven effective in assessing frailty [68]. Mirroring these approaches, developing a tool that incorporates psychological factors could immensely benefit the evaluation of frailty in dogs.
In this study, various blood parameters were explored within the context of frailty. Our analysis centered on a routine comprehensive blood panel commonly conducted by veterinarians in clinical settings. Indeed, identifying frailty biomarkers within these parameters held substantial implications for clinical practice, facilitating early detection and monitoring of frailty in pet dogs. Among them, our study revealed only a weakly significant association between plasma amylase concentration and frailty (p = 0.046), albeit with no meaningful clinical interest (OR: 1.00, 95%CI: [1.00, 1.01]). In human research, salivary alpha-amylase has emerged as a key biomarker for frailty, above various biosocial factors, general health indicators, cytokine profiles, sex hormones, salivary antimicrobial proteins, and blood cell counts [69]. Our study quantified plasma amylase concentration, reflecting contributions from both salivary glands and the pancreas [70]. This broader source spectrum may explain the lack of clinical relevance observed between our frail and robust subjects (median 819 U/L [range: 257 – 1617] vs. 783 U/L [range: 285 – 1585] respectively). Future investigations should prioritize the assessment of salivary alpha-amylase, given its potential as a more discriminatory biomarker for frailty.
From a more global point of view, the links between frailty and biological or biochemical parameters may have been hidden by the importance of factors linked to owners. Indeed, dogs were recruited on a voluntary basis, which inevitably introduced selection biases, and prevents us from generalizing the findings to the entire population of dogs. Moreover, the relatively small sample size may have led us to overlook certain results due to low statistical power. This study specifically targeted dogs weighing more than 19 kg, with weights ranging from 19 to 56 kg. While this focus helped reduce variability, as dogs age differently depending on their size [71], it also restricted the study's scope. As a result, the findings cannot be extrapolated to smaller dogs. However, despite these limitations, this study stands as the pioneering effort to examine factors linked with frailty within a population of pet dogs using a comprehensive epidemiological and clinical methodology. The two-step statistical analyses employed allowed for the exploration of numerous factors and permitted the identification of significant associations.
Conclusion
Regular deworming practices and heightened levels of attachment emerged as significant factors associated with robustness, emphasizing the pivotal role of pet owner’s concern of its care. Furthermore, the study sheds light on the nuanced interplay between owner-dog personality differences and canine frailty, advocating for a comprehensive approach that considers both human and canine characteristics in promoting optimal health outcomes. Serving as a pioneering effort in comprehensively examining factors linked with frailty in pet dogs, this research highlights the essential role of proactive involvement from pet owners in enhancing the quality of life and well-being of their senior dogs.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BFI:
-
Big Five Inventory
- ESCCAP:
-
European Scientific Counsel Companion Animal Parasites
- MCS:
-
Muscle Condition Score
- OR:
-
Odds ratio
- WSAVA:
-
World Small Animal Veterinary Association
References
Miller MS, Tilley LP, Smith FWK. Cardiopulmonary Disease in the Geriatric Dog and Cat. Vet Clin North Am Small Anim Pract. 1989J 1;19(1):87–102.
Hayek MG, Davenport GM. Nutrition and Aging in Companion Animals. J Anti-Aging Med. 1998Jan;1(2):117–23.
Bartges JW. Chronic kidney disease in dogs and cats. Vet Clin North Am Small Anim Pract. 2012;42(4):669–92 vi.
Kyllar M, Witter K. Prevalence of dental disorders in pet dogs. Veterinární Medicína. 2005Nov 30;50(11):496–505.
Freeman LM. Cachexia and sarcopenia: emerging syndromes of importance in dogs and cats. J Vet Intern Med. 2012Feb;26(1):3–17.
Dhaliwal R, Boynton E, Carrera-Justiz S, Cruise N, Gardner M, Huntingford J, et al. 2023 AAHA Senior Care Guidelines for Dogs and Cats. J Am Anim Hosp Assoc. 2023Jan 1;59(1):1–21.
Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. The Lancet. 2013Mar 2;381(9868):752–62.
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001Mar;56(3):M146–156.
Gonçalves RS, Maciel ÁC, Rolland Y, Vellas B, de Souto Barreto P. Frailty biomarkers under the perspective of geroscience: A narrative review. Ageing Res Rev. 2022;81:101737.
Hua J, Hoummady S, Muller C, Pouchelon JL, Blondot M, Gilbert C, et al. Assessment of frailty in aged dogs. Am J Vet Res. 2016Dec;77(12):1357–65.
Lemaréchal R, Hoummady S, Barthélémy I, Muller C, Hua J, Gilbert C, et al. Canine model of human frailty: adaptation of a frailty phenotype in older dogs. J Gerontol A Biol Sci Med Sci. 2023 Jan 6;glad006.
Bamps J, Capouillez B, Rinaldi R, Patris S. Frailty detection by healthcare professionals: a systematic review of the available English and French tools and their validation. Eur Geriatr Med. 2023Aug;14(4):773–87.
Banzato T, Franzo G, Di Maggio R, Nicoletto E, Burti S, Cesari M, et al. A Frailty Index based on clinical data to quantify mortality risk in dogs. Sci Rep. 2019Nov 14;9(1):16749.
Chen FL, Ullal TV, Graves JL, Ratcliff ER, Naka A, McKenzie B, et al. Evaluating instruments for assessing healthspan: a multi-center cross-sectional study on health-related quality of life (HRQL) and frailty in the companion dog. GeroScience. 2023;45(4):2089–108.
Feng Z, Lugtenberg M, Franse C, Fang X, Hu S, Jin C, et al. Risk factors and protective factors associated with incident or increase of frailty among community-dwelling older adults: A systematic review of longitudinal studies. PLoS ONE. 2017Jun 15;12(6): e0178383.
Barbosa da Silva A, Queiroz de Souza I, da Silva IK, Borges Lopes Tavares da Silva M, Oliveira Dos Santos AC. Factors Associated with Frailty Syndrome in Older Adults. J Nutr Health Aging. 2020;24(2):218–22.
Hajek A, Kretzler B, König HH. Relationship between personality factors and frailty. A systematic review Arch Gerontol Geriatr. 2021;97: 104508.
Ruple A, MacLean E, Snyder-Mackler N, Creevy KE, Promislow D. Dog Models of Aging. Annu Rev Anim Biosci. 2022Feb;15(10):419–39.
Cotman CW, Head E. The canine (dog) model of human aging and disease: dietary, environmental and immunotherapy approaches. J Alzheimers Dis JAD. 2008Dec;15(4):685–707.
Hoffman JM, Creevy KE, Franks A, O’Neill DG, Promislow DEL. The companion dog as a model for human aging and mortality. Aging Cell. 2018Jun;17(3): e12737.
Adams A, Cox AL. Questionnaires, in-depth interviews and focus groups. In: Cairns P, Cox AL, editors. Research Methods for Human-Computer Interaction. 1st ed. Cambridge University Press; 2008. p. 17–34.
WSAVA. WSAVA Diet History Form. 2020. Available from: https://wsava.org/wp-content/uploads/2020/01/Diet-History-Form.pdf. Cited 2024 Apr 19.
Purina institute. Purina Fecal Scoring Chart. 2019. Available from: https://www.purinainstitute.com/centresquare/nutritional-and-clinical-assessment/purina-fecal-scoring-chart. Cited 2024 Apr 18.
ESCCAP. ESCCAP Guideline 01 Third Edition. 2021. Worm control in dogs and cats. Available from: https://www.esccap.org/uploads/docs/oc1bt50t_0778_ESCCAP_GL1_v15_1p.pdf. Cited 2024 Apr 13.
Salvin HE, McGreevy PD, Sachdev PS, Valenzuela MJ. The canine cognitive dysfunction rating scale (CCDR): a data-driven and ecologically relevant assessment tool 1997. Vet J Lond Engl. 2011;188(3):331–6.
Ragetly GR, Massey L, Brown DC. Initial psychometric testing and validation of the French version of the Canine Brief Pain Inventory. Vet Anaesth Analg. 2019Sep 1;46(5):667–72.
Wells JR, Young AL, Crane A, Moyaert H, Michels G, Wright A. Linguistic Validation of the Canine Brief Pain Inventory (CBPI) for Global Use. Front Vet Sci. 2021;8: 769112.
Plaisant O, Courtois R, Réveillère C, Mendelsohn GA, John OP. Validation par analyse factorielle du Big Five Inventory français (BFI-Fr). Analyse convergente avec le NEO-PI-R. Ann Méd-Psychol Rev Psychiatr. 2010;168(2):97–106.
Ley JM, McGreevy P, Bennett PC. Inter-rater and test–retest reliability of the Monash Canine Personality Questionnaire-Revised (MCPQ-R). Appl Anim Behav Sci. 2009Jun 1;119(1):85–90.
Ley JM, Bennett PC, Coleman GJ. Personality dimensions that emerge in companion canines. Appl Anim Behav Sci. 2008;110:305–17.
Tiotsop LF, Servetti A, Barkowsky M, Masala E. Modeling Subject Scoring Behaviors in Subjective Experiments Based on a Discrete Quality Scale. IEEE Trans Multimed. 2024;26:8742–57.
Mantiuk RK, Tomaszewska A, Mantiuk R. Comparison of Four Subjective Methods for Image Quality Assessment. Comput Graph Forum. 2012Dec;31(8):2478–91.
Johnson TP, Garrity TF, Stallones L. Psychometric Evaluation of the Lexington Attachment to Pets Scale (Laps). Anthrozoös. 1992Sep;5(3):160–75.
Laflamme D. Development and validation of a body condition score system for dogs. Canine Pract. 1997;22:10–5.
WSAVA, Freeman L, Becvarova I, Cave N, MacKay C, Nguyen P, et al. WSAVA Nutritional Assessment Guidelines. J Small Anim Pract. 2011 52(7):385–96.
Hennet P, Servet E, Salesse H, Soulard Y. Evaluation of the Logan & Boyce plaque index for the study of dental plaque accumulation in dogs. Res Vet Sci. 2006May;1(80):175–80.
Wolf HF, Hassell TM, Rateitschak-Plüss EM, Rateitschak KH. Gingivitis. In: Color Atlas of Dental Medicine: Periodontology. Stuttgart: Georg Thieme Verlag; 2005. p. 79–81.
AVDC. Stages of Pet Periodontal Disease. 2014. Available from: https://afd.avdc.org/five-stages-of-pet-periodontal-disease/, https://afd.avdc.org/five-stages-of-pet-periodontal-disease/. Cited 2024 May 13.
Devriendt N, Rodrigues TCN, Vandenabeele S, Favril S, Biscop A, Marynissen S, et al. Validation of a skin and coat scoring protocol in dogs. Vlaams Diergeneeskd Tijdschr. 2021Oct 29;90(5):227–30.
Swimmer RA, Rozanski EA. Evaluation of the 6-minute walk test in pet dogs. J Vet Intern Med. 2011Apr;25(2):405–6.
Grebert M, Granat F, Braun J, Leroy Q, Bourgès-Abella N, Trumel C. Validation of the Sysmex XN-V hematology analyzer for canine specimens. Vet Clin Pathol. 2021Jun;50(2):184–97.
R Core Team. R Foundation for Statistical Computing, Vienna, Austria. 2021. R: A language and environment for statistical computing. Available from: https://www.r-project.org/.
Lê S, Josse J, Husson F. FactoMineR: An R Package for Multivariate Analysis. J Stat Softw. 2008Mar;18(25):1–18.
Escofier B, Pagès J. Multiple factor analysis (AFMULT package). Comput Stat Data Anal. 1994Aug 1;18(1):121–40.
Kim JH. Multicollinearity and misleading statistical results. Korean J Anesthesiol. 2019Dec;72(6):558.
FACCO. Rapport annuel 2023. Enquête Kantar/FACCO. Available from: https://www.facco.fr/connaissez-vous-lage-des-chats-et-des-chiens-en-france/. Cited 2024 Jun 17.
Cesari M, Gambassi G, van Kan GA, Vellas B. The frailty phenotype and the frailty index: different instruments for different purposes. Age Ageing. 2014Jan;43(1):10–2.
Yamamoto M, Yamamoto MM, Hart LA. Physical Activity and Welfare of Guide Dogs and Walking Activity of Their Partners. Anthrozoös. 2015Jun 1;28(2):277–89.
Buckinx F, Rolland Y, Reginster JY, Ricour C, Petermans J, Bruyère O. Burden of frailty in the elderly population: perspectives for a public health challenge. Arch Public Health. 2015Apr 10;73(1):19.
Cesari M, Onder G, Russo A, Zamboni V, Barillaro C, Ferrucci L, et al. Comorbidity and physical function: results from the aging and longevity study in the Sirente geographic area (ilSIRENTE study). Gerontology. 2006;52(1):24–32.
Visser M, Pluijm SMF, Stel VS, Bosscher RJ, Deeg DJH. Physical Activity as a Determinant of Change in Mobility Performance: The Longitudinal Aging Study Amsterdam. J Am Geriatr Soc. 2002;50(11):1774–81.
Woo J. Nutrition and Frailty. J Nutr Health Aging. 2018Nov 1;22(9):1025–7.
Zhang B, Gems D. Gross ways to live long: Parasitic worms as an anti-inflammaging therapy? Soldati-Favre D, editor. Life. 2021;10:e65180.
Enders-Slegers MJ, Hediger K. Pet Ownership and Human-Animal Interaction in an Aging Population: Rewards and Challenges. Anthrozoös. 2019Mar 4;32(2):255–65.
Park RM, Gruen ME, Royal K. Association between Dog Owner Demographics and Decision to Seek Veterinary Care. Vet Sci. 2021Jan;8(1):7.
Taeckens A, Corcoran M, Wang K, Morris KN. Examining human-animal interactions and their effect on multidimensional frailty in later life: a scoping review. Front Public Health. 2023Jun;21(11):1214127.
Väätäjä H, Majaranta P, Cardó AV, Isokoski P, Somppi S, Vehkaoja A, et al. The Interplay Between Affect, Dog’s Physical Activity and Dog-Owner Relationship. Front Vet Sci. 2021Dec;9(8): 673407.
Belshaw Z, Dean R, Asher L. “You can be blind because of loving them so much”: the impact on owners in the United Kingdom of living with a dog with osteoarthritis. BMC Vet Res. 2020Jun 11;16(1):190.
Lue TW, Pantenburg DP, Crawford PM. Impact of the owner-pet and client-veterinarian bond on the care that pets receive. J Am Vet Med Assoc. 2008Feb 15;232(4):531–40.
Rohlf VI, Bennett PC, Toukhsati S, Coleman G. Beliefs Underlying Dog Owners’ Health Care Behaviors: Results from a Large, Self-Selected. Internet Sample Anthrozoös. 2012Jun 1;25(2):171–85.
McCoy B, Brassington L, Jin K, Dolby G, Shrager S, Collins D, et al. Social determinants of health and disease in companion dogs: A cohort study from the Dog Aging Project. Evol Med Public Health. 2023May;13:11.
Marinelli L, Adamelli S, Normando S, Bono G. Quality of life of the pet dog: Influence of owner and dog’s characteristics. Appl Anim Behav Sci. 2007Dec;108(1–2):143–56.
Gale CR, Mõttus R, Deary IJ, Cooper C, Sayer AA. Personality and Risk of Frailty: the English Longitudinal Study of Ageing. Ann Behav Med Publ Soc Behav Med. 2017Feb;51(1):128–36.
Stephan Y, Sutin AR, Canada B, Terracciano A. Personality and Frailty: Evidence From Four Samples. J Res Personal. 2017Feb;66:46–53.
Sutin AR, Stephan Y, Luchetti M, Artese A, Oshio A, Terracciano A. The five-factor model of personality and physical inactivity: A meta-analysis of 16 samples. J Res Personal. 2016Aug;1(63):22–8.
Reaney SJ, Zulch H, Mills D, Gardner S, Collins L. Emotional affect and the occurrence of owner reported health problems in the domestic dog. Appl Anim Behav Sci. 2017Nov;1(196):76–83.
Bender Y, Bräuer J, Schweinberger SR. What makes a good dog-owner team? – A systematic review about compatibility in personality and attachment. Appl Anim Behav Sci. 2023Mar;1(260): 105857.
Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and reliability of the Edmonton Frail Scale. Age Ageing. 2006Sep;35(5):526–9.
Furtado GE, Uba Chupel M, Minuzzi L, Patrício M, Loureiro M, Bandelow S, et al. Exploring the potential of salivary and blood immune biomarkers to elucidate physical frailty in institutionalized older women. Exp Gerontol. 2020Jan;1(129): 110759.
Pieper-Bigelow C, Strocchi A, Levitt MD. Where does serum amylase come from and where does it go? Gastroenterol Clin North Am. 1990Dec;19(4):793–810.
Galis F, Van der Sluijs I, Van Dooren TJM, Metz JAJ, Nussbaumer M. Do large dogs die young? J Exp Zoolog B Mol Dev Evol. 2007Mar 15;308(2):119–26.
Acknowledgements
The authors would like to thank all of the owners who kindly bring their dogs allowing the completion of this study. The authors also gratefully thank the Comparative Medical Biology and Histology team of CREFRE, Université de Toulouse, Inserm, UPS, ENVT, Toulouse, France and acknowledge the financial support of Melet Schloesing Laboratories Inc (Osny, France).
Funding
This study was partially funded by Lallemand SAS (Blagnac, France) and supported by Melet Schloesing Laboratories Inc (Osny, France), which provided all the resources needed for biochemistry measurements.
Author information
Authors and Affiliations
Contributions
TB designed the project, enrolled dogs and was responsible for follow-up visits and surveys, and for sampling, performed laboratory and statistical analysis, interpreted the data, and drafted the manuscript, AMu participated in study design, contributed to interpretation of data and manuscript preparation, SD verified statistical analysis, contributed to manuscript preparation, NP co-supervised the study, participated in study design, and AMe senior author, supervised the study, participated in study design, contributed to interpretation of data and manuscript preparation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study has received approval from the Animal Ethical Committee "SCIENCE ET SANTE ANIMALES CEEA N°115" (ANIMAL SCIENCE AND HEALTH CEEA N°115) in Toulouse, National Veterinary School of Toulouse, France, under the reference number SSA_2022_014. During the study, AMe and NP were members of this committee but the conflict of interest was properly declared. This study also received approval from the Human Research Ethical Committee “Comité d’éthique et de la recherche – CER” (Ethics and Research Committee – CER) in Toulouse, Toulouse Midi Pyrénées Federal University, France, under the reference number 2023_719. The authors of the study do not have any link with this committee. Informed consent was obtained from all the dog owners.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Blanchard, T., Mugnier, A., Déjean, S. et al. Exploring frailty in apparently healthy senior dogs: a cross-sectional study. BMC Vet Res 20, 436 (2024). https://doi.org/10.1186/s12917-024-04296-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12917-024-04296-1