
Abstract
Background
Cardiac tumors in cats are relatively rare, with lymphoma accounting for more than half of all cases. However, feline cardiac lymphoma is often diagnosed post-mortem, and it is difficult to diagnose while the cat is still alive. It is the first report of a direct, rather than estimative, diagnosis with cardiac needle biopsy of a living cat with cardiac lymphoma.
Case presentation
A 3-year-old domestic short-haired male cat experienced loss of energy and loss of appetite. Thoracic radiography and transthoracic echocardiography showed cardiomegaly with slight pleural effusion and cardiac tamponade due to pericardial effusion, respectively. In addition, partial hyperechoic and hypertrophy of the papillary muscle and myocardium were observed. Blood test showed an increase in cardiac troponin I levels. Pericardial fluid, removed by pericardiocentesis, was analyzed; however, the cause could not be determined. With the owner’s consent, pericardiectomy performed under thoracotomy revealed a discolored myocardium. Cardiac needle biopsy was performed with a 25G needle, and a large number of large atypical lymphocytes were collected; therefore, a direct diagnosis of cardiac lymphoma was made. Pathological examination of the pericardium diagnosed at a later date revealed T-cell large cell lymphoma. The cat underwent chemotherapy followed by temporary remission but died 60 days after the diagnosis. Postmortem, two-dimensional speckle-tracking echocardiography (data when alive) revealed an abnormal left ventricular myocardial deformation, which corresponded to the site of cardiac needle biopsy.
Conclusions
This rare case demonstrates that cardiac lymphoma should be added to the differential diagnosis in cats with myocardial hypertrophy and that the diagnosis can be made directly by thoracotomy and cardiac needle biopsy. In addition, the measurement of cardiac troponin I levels and local deformation analysis of the myocardium by two-dimensional speckle-tracking echocardiography may be useful in the diagnosis of cardiac tumors.
Similar content being viewed by others


Background
Cardiac tumors in cats are relatively rare, with lymphoma accounting for more than half of all cases. However, feline cardiac lymphoma is often diagnosed post-mortem [1,2,3,4,5,6,7,8,9,10,11,12], and it is difficult to diagnose while the cat is still alive. It is the first report of a direct, rather than estimative, diagnosis with cardiac needle biopsy of a living cat with cardiac lymphoma.
Case presentation
A 3-year-old domestic short-haired male cat experienced loss of energy and loss of appetite. Physical examination at the initial visit showed a body temperature of 38.0 °C, normal auscultation, normal visible mucosa, and slightly elevated blood pressure (systolic blood pressure: 165 mmHg). The cat also had right-sided Horner's syndrome of undetermined etiology, as no gross pathology was found in the right ear canal or neck. Blood chemistry showed elevated levels of plasma total protein and abnormally high levels of cardiac troponin I (cTnI) (1.18 ng/mL; reference range, 0–0.17 ng/mL: i-STAT Heska [13]).
Electrocardiogram findings revealed sinus tachycardia (253 bpm), and thoracic radiography showed no abnormalities. Echocardiography revealed irregular hypertrophy of the anterior papillary muscle and increased echogenicity; however, there were no evidence of congestion such as enlargement of the left atrium (Video 1). A clinical diagnosis of suspected hypertrophic cardiomyopathy (HCM) phenotype (include myocarditis) was made, and the cat was observed on follow-up.
On the 12th day from the initial visit, the cat was brought to the hospital again with the chief complaint of syncope. At the time of admission, the cat presented with open-mouth panting, but no signs of cyanosis were observed. Blood tests showed a higher cTnI level (3.25 ng/mL), and a complete blood count analysis showed eosinophilia. The cat tested positive for both feline immunodeficiency virus and feline leukemia.
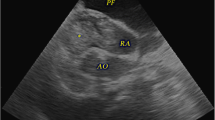
Thoracic radiography revealed cardiomegaly (VHS = 8.5; reference range, 7.5 ± 0.3) with slight pleural effusion. Focused cardiac ultrasound revealed pericardial effusion and increased hypertrophy of the papillary muscles and left ventricular posterior wall. The patient also had right atrial collapse, which was diagnosed as cardiac tamponade (Table 2, Video 2, 3), and 10 mL of pericardial fluid was removed.
The total protein of the pericardial fluid was 5.2 g/dL, the number of nucleated cells was 8300 /mL, and a mixture of neutrophils; macrophages; and large, medium, and small lymphocytes were observed in the sediment smear. These findings are consistent with chronic active inflammation.
After consultation with the owner, pericardiectomy was performed through thoracotomy. The pericardium was slightly thickened and had abundant blood vessels (Fig. 1-a). The left ventricular free wall myocardium had a reddish and rough surface that was found after pericardial removal (Fig. 1-b). The free wall myocardial surface was punctured six to seven times with a 25-G needle without syringe aspiration. There was minimal bleeding from this procedure, and hemostasis was achieved by adding pressure with a cotton swab. No arrhythmia was observed during the procedure. No problems with this procedure occurred after the operation. Cardiac needle biopsy cytology revealed many large, atypical lymphocytes (Fig. 2), which led to a direct diagnosis of cardiac lymphoma on the 12th day from the initial visit.

Before pericardial removal. a After pericardium removal. b The pericardium is slightly thickened and has abundant blood vessels, and the myocardium on the free wall side of the left ventricle after removal of the pericardium is reddish and has a rough surface

Cytology from myocardial needle biopsy. The image shows many lymphoid cells with large dysmorphic nuclei. (Captured by Olympus BX-43 and DP-27, the resolution is 150 dpi, uncompressed)
One day after the diagnosis, the cat received an injection of L-asparaginase (400 IU/kg/subcutaneous injection [SC]), followed by chemotherapy. Subsequently, the following chemotherapy protocol was adhered to: vincristine 0.5 mg/m2/intravenous injection (IV) on the 8th, 22nd, and 36th days after diagnosis; cyclophosphamide 10 mg/kg/IV on the 15th day after diagnosis; methotrexate 0.8 mg/kg/IV on the 29th day after diagnosis; L-Asparaginase 400 IU/kg/SC again on the 43rd day after diagnosis; doxorubicin 1 mg/kg/IV on the 50th day after diagnosis; and cytarabine 100 mg/m2/SC on the 57th and 58th days after diagnosis. We received the results of the pericardial pathological examination six days after the clinical diagnosis. Immunostaining revealed CD3 positive/CD20 negative lymphocytes, and T-cell large cell lymphoma was diagnosed (Fig. 3). On the 15th day after diagnosis, cTnI levels returned to normal (Table 1), and myocardial morphology appeared to have normalized (Table 2, Video 4). On the 43rd day after diagnosis, relapse was observed in places other than the heart. The cat died due to neurological symptoms on the 60th day after diagnosis. The owner did not consent for autopsy. Before death, a mild increase in cTnI levels and papillary muscle hypertrophy were noted, a third papillary muscle was more evident (Video 5), but there were no signs of left atrial enlargement or heart failure (Table 2). Postmortem, two-dimensional speckle-tracking echocardiography (2D-STE) analysis was performed using the echocardiographic data before death (4th day after diagnosis). The cardiac needle biopsy site (myocardium near the anterior papillary muscle of the left ventricle) revealed a marked reduction in myocardial deformity and lack of coordination with other areas of the left ventricular myocardium (Fig. 4, green line).

Pericardial pathology. Immunostaining image showing CD3-positive/CD20-negative lymphocytes, indicating a diagnosis of a T-cell large cell lymphoma. Hematoxylin and eosin staining (× 20) (a) CD3 immunostaining (× 20) (b)

Two-dimensional speckle-tracking echocardiography (on the 4th day after diagnosis). The green lines indicate myocardial deformations of the left ventricular free wall. This site corresponds to the site of myocardial hypertrophy and cardiac needle biopsy. From left to right: results for the endomyocardial layer, whole layer of the myocardium, and the epimyocardial layer. Note the significant decrease in green (segmental strain value is -5%) and pink myocardial site (segmental strain value -3%) in whole layer strain (center)
Discussion and conclusions
Cardiac tumors in cats are relatively rare, with lymphoma accounting for more than half of all cases [1,2,3,4,5,6,7,8,9,10,11,12]. However, feline cardiac lymphoma is often diagnosed post-mortem, and it is difficult to diagnose while the cat is still alive. Delayed diagnosis may lead to delayed treatment, to the cat’s detrimental condition. In previous reports, most cases were clinically diagnosed as "estimated cardiac lymphoma" by analysis of stored pericardial fluid [3, 4, 8] or as lymphoma spillover from other sites and based on the patient’s response to chemotherapy [1, 9]. This is the first report of direct diagnosis with cardiac needle biopsy and early treatment of a living cat with cardiac lymphoma. In addition, as demonstrated in this case, cardiac troponin measurement and 2D-STE analysis may be useful diagnostic tools.
Although there is literature evaluating the safety of cardiac needle biopsy in dogs, there are no reports on this aspect in cats [14].
However, based on the abnormally high level of troponin in this case, which was different from the typical HCM findings, aggressive tests such as cardiac needle biopsy were performed. In this case, open thoracic pericardiectomy was performed for treating cardiac tamponade, during which we performed a cardiac needle biopsy under visualization. Although there are no reports that have evaluated safety in cats, it is likely that puncture with visualization can be performed safely by avoiding major coronary arteries.
In this case, HCM phenotype was suspected and clinically diagnosed because of hypertrophy of the left ventricular papillary muscle at the initial visit. In the ACVIM consensus statement, feline myocardial disease is classified by a clinical morphological approach; accordingly, a diagnosis of the HCM phenotype was made in the present case [15]. However, as opposed to traditional cases of HCM, troponin I values were markedly higher [16]. Furthermore, 2D-STE analysis of the left ventricular myocardium revealed a regional decrease in myocardial function coincident with the hypertrophic and biopsy area; these regional abnormalities are in contrast to typical myocardial function in HCM [17]. In addition to HCM, although they are rare, neoplastic diseases such as lymphoma, myocarditis, and toxoplasma infection have also been reported as myocardial diseases for differentiating hypertrophic myocardium in cats. In such myocardial diseases, cardiac needle biopsy cytology may be useful for diagnosis [18,19,20]. As in this case, cardiac needle biopsy cytology may be a more aggressive diagnostic test in cats with unexplained myocardial hypertrophy and that present with clinical findings different from HCM, especially in cats with abnormally high cTnI levels and abnormal myocardial function based on 2D-STE analysis. Furthermore, the abnormally high cTnI values in this case allowed us to focus on the heart after the cat’s initial visit.
cTnI has already proven useful in numerous studies, as it is an indicator of myocardial damage [16, 21]. In this case, the cTnI values decreased with the start of chemotherapy and normalized two weeks later. They increased again on the 50th day after diagnosis. According to recent studies, there is a correlation between myocardial damage and cTnI values in mice and rats [22]. Therefore, troponin levels may be a diagnostic reflection of myocardial damage due to tumor cell infiltration into the tissue. In this case, 2D-STE analysis showed local abnormalities in myocardial function. Although 2D-STE analysis has been used in past studies for the clinical diagnosis and differentiation of cats with cardiomyopathy [17, 23], it is often due to motor dysfunction of the entire left ventricle rather than a focal myocardial abnormality. Interestingly, in this case, local myocardial dysfunction was observed at the papillary muscle attachment site. However, pathological examination did not reveal tumor cell infiltration distribution or the extent of other myocardial damage such as myocardial necrosis. We believe that, in future cases, 2D-STE will be a useful tool in the diagnosis of cardiac tumors.
In this case, cardiac lymphoma was directly diagnosed by performing thoracotomy and cardiac needle biopsy cytology. Based on the results of these diagnostics, immediate intervention began with chemotherapy. In cats with suspected cardiac tumors associated with cardiac tamponade, cardiac needle biopsy cytology, in addition to thoracotomy pericardial resection, may be a useful tool for early diagnosis and therapeutic intervention. In addition, measurement of cTnI levels and detection of myocardial damage using 2D-STE may also be useful as a diagnostic aid in these cases.
Availability of data and materials
The data that support our findings are available from the corresponding author on reasonable request.
Abbreviations
- cTnI:
-
Cardiac troponin I
- HCM:
-
Hypertrophic cardiomyopathy
- 2D-STE:
-
Two-dimensional speckle-tracking echocardiography
References
Brummer DG, Moise NS. Infiltrative cardiomyopathy responsive to combination chemotherapy in a cat with lymphoma. J Am Vet Med Assoc. 1989;195(8):1116–9.
Meurs KM, Miller MW, Mackie JR, Mathison P. Syncope associated with cardiac lymphoma in a cat. J Am Anim Hosp Assoc. 1994;30:583–5.
Zoia A, Hughes D, Connolly DJ. Pericardial effusion and cardiac tamponade in a cat with extranodal lymphoma. J Small Anim Pract. 2004;45(9):467–71.
Shinohara N, Macgregor JM, Calo A, Rush JE, Penninck DG, Knoll JS. Presumptive primary cardiac lymphoma in a cat causing pericardial effusion. J Vet Cardiol. 2005;7(1):65–9.
Aupperle H, März I, Ellenberger C, Buschatz S, Reischauer A, Schoon HA. Primary and secondary heart tumours in dogs and cats. J Comp Pathol. 2007;136(1):18–26.
Carter TD, Pariaut R, Snook E, Evans DE. Multicentric lymphoma mimicking decompensated hypertrophic cardiomyopathy in a cat. J Vet Intern Med. 2008;22(6):1345–7.
Kagawa Y, Yamashita T, Maetani S, Aoki Y, Sakaguchi K, Hirayama K, Umemura T, Taniyama H. Cutaneous lymphoplasmacytic lymphoma with systemic metastasis in a cat. J Vet Med Sci. 2011;73(9):1221–4.
Amati M, Venco L, Roccabianca P, Santagostino SF, Bertazzolo W. Pericardial lymphoma in seven cats. J Feline Med Surg. 2014;16(6):507–12.
Shih JL, Brenn S, Schrope DP. Cardiac involvement secondary to mediastinal lymphoma in a cat: regression with chemotherapy. J Vet Cardiol. 2014;16(2):115–20.
Mori M, Izawa T, Sasaki H, Sonoyama J, Nishimura S, Shimamura S, Shimada T, Hasegawa T, Kuwamura M, Yamate J. A Case of Feline T-cell Lymphoma with Tropism for Striated Muscle and Peripheral Nerve. J Comp Pathol. 2019;168:8–12.
Woldemeskel M. Primary Cardiac Lymphoma in a Cat. J Comp Pathol. 2020;174:34–8.
Kharbush RJ, Hohenhaus AE, Donovan TA, Fox PR. B-cell lymphoma invading and compressing the heart base and pericardium in a cat. J Vet Cardiol. 2021;35:84–9.
Côté E. Cardiac biomarkers. In: Côté E, Kristin MDKA, Meurs KM, Sleeper MM, editors. Feline Cardiology. Ames, IA: John Wiley & Sons; 2011. p. 69–75.
Price KC, Weiss JM, Hata D, Smith JR. Experimental needle biopsy of the myocardium of dogs with particular reference to histologic study by electron microscopy. J Exp Med. 1955;101:687–94.
Luis Fuentes V, Abbott J, Chetboul V, Côté E, Fox PR, Häggström J, Kittleson MD, Schober K, Stern JA. ACVIM consensus statement guidelines for the classification, diagnosis, and management of cardiomyopathies in cats. J Vet Intern Med. 2020;34:1062–77.
Hori Y, Iguchi M, Heishima Y, Yamashita Y, Nakamura K, Hirakawa A, Kitade A, Ibaragi T, Katagi M, Sawada T, Yuki M, Kanno N, Inaba H, Isayama N, Onodera H, Iwasa N, Kino M, Narukawa M, Uchida S. Diagnostic utility of cardiac troponin I in cats with hypertrophic cardiomyopathy. J Vet Intern Med. 2018;32:922–9.
Suzuki R, Mochizuki Y, Yoshimatsu H, Niina A, Teshima T, Matsumoto H, Koyama H. Layer-specific myocardial function in asymptomatic cats with obstructive hypertrophic cardiomyopathy assessed using 2-dimensional speckle-tracking echocardiography. J Vet Intern Med. 2019;33:37–45.
Treggiari E, Pedro B, Dukes-McEwan J, Gelzer AR, Blackwood L. A descriptive review of cardiac tumours in dogs and cats. Vet Comp Oncol. 2017;15:273–88.
Glaus T, Wess G. Left ventricular hypertrophy in the cat-“when hypertrophic cardiomyopathy is not hypertrophic cardiomyopathy.” Schweiz Arch Tierheilkd. 2010;152:325–30 (article in German).
Simpson KE, Devine BC, Gunn-Moore D. Suspected toxoplasma–associated myocarditis in a cat. J Feline Med Surg. 2005;7:203–8.
Herndon WE, Kittleson MD, Sanderson K, Drobatz KJ, Clifford CA, Gelzer A, Summerfield NJ, Linde A, Sleeper MM. Cardiac troponin I in feline hypertrophic cardiomyopathy. J Vet Intern Med. 2002;16:558–64.
Frobert A, Valentin J, Magnin JL, Riedo E, Cook S, Giraud MN. Prognostic value of troponin I for infarct size to improve preclinical myocardial infarction small animal models. Front Physiol. 2015;6:353.
Suzuki R, Yuchi Y, Kanno H, Teshima T, Matsumoto H, Koyama H. Left and right myocardial functionality assessed by two-dimensional speckle-tracking echocardiography in cats with restrictive cardiomyopathy. Animals (Basel). 2021;11:1578.
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
ST; data collection, data analysis and writing the paper. RS; study design, 2D-STE analysis. MH; cytological diagnosis. YK; Histopathological diagnosis. HK; study concept. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Video 1. At initial presentation. (Right parasternal short axis view of the papillary muscle level). The video shows the irregular hypertrophy of the anterior papillary muscle and increased echogenicity.
Additional file 2: Video 2. On day of the diagnosis. (Right parasternal short axis view of the papillary muscle level). The video shows pericardial effusion and further hypertrophy of the papillary muscles and left ventricular posterior wall.
Additional file 3: Video 3. On day of the diagnosis. (Right parasternal long axis view). The video shows cardiac tamponade (right atrial collapse).
Additional file 4: Video 4. On the 15th day after diagnosis. (Right parasternal short axis view of the papillary muscle level). The video shows that myocardial morphology appeared to have normalized.
Additional file 5: Video 5. On the 57th day after diagnosis. (Right parasternal short axis view of the papillary muscle level). The video shows that papillary muscle hypertrophy has returned.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tanaka, S., Suzuki, R., Hirata, M. et al. Unusual diagnosis of feline cardiac lymphoma using cardiac needle biopsy. BMC Vet Res 18, 251 (2022). https://doi.org/10.1186/s12917-022-03357-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12917-022-03357-7