
Abstract
Background
Infant neurodevelopment in the first years after birth is determined by multiple factors, including parental care and maternal mental wellbeing. In this study, we aim to assess the impact of persistent maternal depressive symptoms during the first 3 months postpartum on infant neurodevelopment at 6 months.
Methods
Using a longitudinal cohort design, 1253 mother-infant pairs were followed up at 7, 45, and 90 days to assess postpartum depressive symptoms using the Edinburgh Postnatal Depression Scale (EPDS); infants were followed up at 6 months to assess neuro-developmental status using the WHO’s Infant and Young Child Development (IYCD) tool. A generalized linear regression model was used to assess the association between persistent postpartum depressive symptoms and infant neurodevelopmental delay at 6 months. A generalized linear mixed model (GLMM) with a hospital as a random intercept was used to assess the persistent postpartum depressive symptoms with an IYCD score. Linear regression was used to compare the IYCD scores between exposure groups.
Results
In the study population, 7.5% of mothers had persistent depressive symptoms, and 7.5% of infants had neurodevelopmental delay. Infants born to mothers with persistent depressive symptoms had a higher proportion of neurodevelopmental delay than infants born to women without persistent symptoms (48.6% vs 5.1%; p < 0.001). In the adjusted regression model, infants whose mothers had persistent depressive symptoms at 7, 45, and 90 days had a 5.21-fold increased risk of neurodevelopmental delay (aRR, 5.21; 95% CI, 3.17, 8.55). Mean scores in the motor domain (12.7 vs 15.2; p < 0.001) and language domain (6.4 vs 8.5; p < 0.001) were significant when a mother had persistent depression vs. no depression. Mean scores in the general behavioral domain (5.9 vs 10.4, p < 0.001) and the socio-emotional domain (15.4 vs 17.7; p < 0.001) were significantly different when a mother had persistent depression vs no persistent depression.
Conclusions
Our results suggest that 6-month-old infants are at higher risk for neurodevelopment delays if their mother reports persistent symptoms of depression from 7 to 90 days postpartum. The neurodevelopmental delay can be observed in all functional domains. Preventive intervention to reduce maternal postpartum depression may reduce the impact on infant developmental delay.
Similar content being viewed by others


Background
Maternal depression is a global health problem, with an estimated 23.4 million mothers experiencing postpartum depressive symptoms each year and a prevalence rate of 17.2% [1]. Depressive episodes during the postpartum period range from sadness, changes in sleep and eating patterns, despair, crying spells, anxiety, irritability, feelings of isolation, mental liability, thoughts of hurting oneself and/or the infant, and even suicidal thoughts [1]. In South Asia, the rate of maternal depression is 22.2%, with the prevalence rate varying according to the timing and duration of breastfeeding, maternal education, income, life stress, gestational age at birth, and infant illness [1,2,3,4]. Infant and early childhood development is a maturational and interactive process that progressively develops perceptual, motor, cognitive, language, socio-emotional, and self-regulatory skills [5]. Parental psychopathology has been found to be a consistent and robust correlate of child maladjustment, particularly maternal depression [6,7,8,9].
More than 250 million children under the age of 5 were estimated to have developmental delays in LMICs (low- and middle-income countries) worldwide in 2015 [10], highlighting the need to improve access to multisectoral interventions that include health, nutrition, security and safety, responsive care, and early learning for parents [11]. Parents need support to provide nurturing care; they need learning materials and resources to support their children’s neurodevelopment [12]. The fundamental promotive childhood experiences come from the nurturing care and protection received from parents, family, and community, which have lifelong benefits [13].
There are consistent findings linking maternal depression to deficits in both socio-emotional and instrumental functioning. A landmark study conducted by the National Institute of Child Health and Early Development showed that children whose mothers reported depressive symptoms had poorer cognitive functioning and school readiness compared to children who mothers never reported depressive symptoms [14]. Although the literature provides both theoretical and limited empirical support for a reciprocal effects model between maternal depression and child development, a key question remains about the timing of these effects. Children whose mothers reported feeling depressed performed worse on measures of cognitive-linguistic functioning and were rated as less cooperative and more problematic [15, 16].
In Nepal, studies have shown that the population prevalence of maternal postpartum depressive symptoms ranges from 28 to 33% [17, 18], indicating that one-third of the women have depressive symptoms, which is higher than estimates (20% prevalence) made for mothers in LMIC [19]. Given the high burden of postpartum depressive symptoms in Nepal and the link between infant neurodevelopment and maternal mental health, this study aims to assess the impact of persistent maternal depressive symptoms during the first 3 months of the postpartum period on infant neurodevelopment at 6 months.
Methods
Design
This is a longitudinal cohort study design nested within an ongoing quality improvement study in 9 surveillance site hospitals in Nepal. From the women-infant pairs enrolled in the ongoing quality improvement study, a sample of women-infant pairs was selected and followed up until 6 months postpartum. The sample of women who delivered between April and July 2023 were assessed for depressive symptoms between April 28 and September 29, 2020, and developmental assessment follow-up at 6 months was conducted between October 10, 2020 and January 29, 2021 [20, 21].
Study setting
The nine public referral hospitals included in the study represented the seven administrative provinces and the population of the country. Seti Provincial Hospital and Dadeldhura Hospital represented the marginalized population in the far western province; Surkhet Provincial Hospital catered service to the mid-western hilly population; Bheri, Lumbini, Janakpur, and Koshi Hospitals represented the population in the Southern plain province of the country; and Kaski Hospital represented the central hilly population of the country.
Inclusion criteria
Mothers who had singleton live born infants were eligible for inclusion in the study and were approached for consent [22]. Mothers who experienced birth trauma and understood the Nepali language were also eligible to participate. Mothers who consented to the study were followed up at 7, 45, and 90 days for depressive symptoms using the Edinburgh Postpartum Depression Scale (EPDS), and infant neuro-developmental assessment was conducted at 6 months (180 days) using the World Health Organization’s Infant and Young Child Development (IYCD) tool.
Sample
We randomly selected 10% of the mothers enrolled in the quality improvement study in the nine hospitals for this longitudinal cohort study using random sequence generation in an Excel spreadsheet with all participants. Of the 2022 mothers enrolled, longitudinal follow-up was conducted at 7, 45, 90, and 180 days (Fig. 1).

Study flow diagram
Measure
Exposure
Symptoms of postpartum depression were measured using the EPDS. EPDS is a validated self-reported 10-question self-report questionnaire with a scale of 0 to 3 to measure depressive symptoms in postpartum mothers [23, 24], and for this study, a score of ≥ 12 was used to categorize mothers with depressive symptoms. Persistent depressive symptoms were defined as scores ≥ 12 at all three time points (7, 45, and 90 days).
Outcome
Infant neurodevelopment was measured using the WHO’s IYCD, an open-access, validated, mother-reported tool for child development in the domains of motor, language-cognitive, social-emotional, and general behavior [25, 26]. The IYCD was a 100-item parent report tool (40 fine motor and gross motor, 30 language, 20 socio-emotional, and 10 unscored behavioral items). Delayed infant neurodevelopment at 6 months was based on a centile score of 10 or less, based on previous literature [25, 26].
Covariates
Ethnicity
In Nepal, the social class system determines the social access to resources. For the purpose of this study, ethnicity was divided into two social groups, first a disadvantaged social group which included janjati, muslim, madeshi, and dalit ethnic groups and an advantaged social group such as chettri-brahmin. Maternal education was categorized as uneducated (illiterate and unable to read and write) and educated (primary education and above).
Preterm birth
Based on the date of last menstrual cycle date, preterm birth was defined as birth occurring before 37 weeks of gestation; low birth weight was defined as birth weight < 2500 g, and infant sex was categorized as boy or girl.
Data collection
The hospital research surveillance team approached eligible women, informed them of the study, and enrolled those who provided written consent. The trained research surveillance team conducted telephone follow-ups at 7, 45, 90, and 180 days after delivery. During the telephone follow-up with the mother, sociodemographic, obstetric, postpartum depression (EPDS 10), and infant neurodevelopment (IYCD) data were collected using a semi-structured questionnaire from a tablet-based application.
Data management and analysis
Descriptive statistics on the prevalence of maternal depressive symptoms at 7, 45, and 90 days and persistent depressive symptoms were calculated in Additional file 1: Table S1. The IYCD as a score for a global developmental domain and subdomains was analyzed using percentile cut-offs calculated in Additional file 1: Table S2. Differences in the population characteristics (maternal ethnicity, maternal education), birth characteristics (preterm birth, LBW, and infant sex), maternal depression (exposure), and infants with developmental delay (outcome) were analyzed using Pearson’s chi-square, and Fisher’s exact test was done in Tables 2 and 3. We used three different statistical models to assess the causal relationship between maternal depression and infant neurodevelopment. In the first statistical model, a generalized linear regression model was used to assess the association between maternal depression at 7, 45, and 90 days and persistent postpartum depressive symptoms with an infant’s neurodevelopmental delay at 6 months, as shown in Additional file 1: Table S3. In the second statistical model, the generalized linear mixed model (GLMM) with the hospital as a random intercept was used. In this model, because there were not enough children with developmental problems in all the hospitals, we decided not to use a binary outcome and instead modeled the outcome as a continuous variable (IYCD6 continuous) using a mixed effects linear regression model with the hospital as a random intercept in Table 4. In the third statistical model, the mean score with standard deviation of IYCD and functional domain of infants whose mothers had persistent depression compared to infants whose mothers did not have persistent depression using linear regression model in Fig. 2 and Additional file 1: Table S2. The sociodemographic factors (ethnicity and maternal education) and biological factors (infant sex and prematurity) that differed in the exposure population were adjusted in all three statistical models. Statistical analysis was performed using IBM SPSS Statistics SPSS 28.0.2 version for generating supplementary tables and R program-4.3.3 version for generating main text tables and the “glmm” package for GLMM regression [27, 28]. Missing data for any exposure or outcome of interest were excluded at the pairwise level.

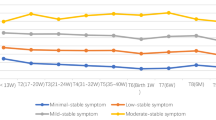
Scores in different functional domains among infants at 6 months born to mothers with/without depressive symptoms
Results
During the recruitment period, a total of 24,912 mothers delivered at the nine study hospitals. Of those who gave birth, 21,805 were eligible for enrollment, and 10% of them were randomly selected for this study. Of the 2022 mothers enrolled in this study, 1253 were successfully contacted during the 7 days follow-up to assess depressive symptoms, 961 were successfully followed up at 45 days (292 lost to follow-up), and 1201 were successfully followed up at 90 days (52 lost to follow-up). Of the mothers who were followed, 946 were successfully contacted at all three time points (307 were lost to follow-up at all three time points). At 6 months, 1253 mothers had a successful postnatal interview to assess the infant neurodevelopmental status using the IYCD reporting tool (Fig. 1).
Maternal depression and population characteristics
Among the follow-up study cohort, the prevalence of mothers with depressive symptoms at 7, 45, and 90 days was 10.1% (n = 127), 11.6% (n = 111), and 9.6% (n = 115) respectively. The prevalence of mothers with persistent depressive symptoms was 7.5% (n = 71) (Additional file 1: Table S1). There was a statistical difference in the persistent depressive symptoms among mothers by social group (p < 0.001), maternal education (p < 0.001), and infant’s prematurity (p < 0.001) (Table 1).
Infant neurodevelopmental delay and population characteristics
Among the infants, the IYCD development score at the 10th, 50th, and 95th percentiles were 44, 53, and 59 respectively (Additional file 1: Table S2). In the population, 7.5% of the infants had a total IYCD score ≤ 44 and were classified as having neurodevelopmental delay. There was a statistical difference in infant neurodevelopment delayed among mothers stratified by social group (p < 0.001), maternal education (p < 0.001), infant sex (p < 0.05), and prematurity (p < 0.001). Infants born to mothers with persistent depressive symptoms had a higher proportion of neurodevelopmental delay than infants born to women without persistent depressive symptoms (47.9% vs 4.6%, p < 0.001) (Table 2).
Statistical model using generalized linear regression
After adjustment for sociodemographic (social group and maternal education) and birth characteristics (infant’s sex and prematurity), infants whose mothers had depressive symptoms at 7 days had a 4.19-fold increased risk of neurodevelopmental delay compared with infants whose mothers did not have depressive symptoms (aRR, 4.19; 95% CI; 2.79, 6.30; p < 0.001). In the adjusted model, infants whose mothers had depressive symptoms at 90 days had a 3.32-fold increased risk of neurodevelopmental delay (aRR, 3.32; 95% CI; 2.15, 5.13; p < 0.001). In the adjusted model, infants whose mothers had persistent depressive symptoms had a 5.21-fold increased risk of neurodevelopmental delay compared with infants whose mothers did not have persistent depressive symptoms (aRR, 5.21; 95% CI, 3.17, 8.55; p < 0.001) (Additional file 1: Table S3).
Statistical model using GLMM with the hospital as random intercept
In this model, with adjustment for sociodemographic and birth characteristics, with each increase in EPDS score at day 7, the IYCD score decreased by 0.13 (p = 0.005). With each increase in depressive score at all three time points (7, 45, and 90 days), the IYCD score decreased by − 0.19 (β coefficient = − 0.19; p = 0.019) (Table 3).
Statistical model using linear regression for individual neurodevelopmental domains
There was a difference in the mean IYCD score between infants born to mothers with persistent depressive symptoms and those born to non-depressive mothers (40.7 vs 51.9; p < 0.001). The mean score and adjusted regression score in the motor domain were significant when a mother had persistent depression compared to no depression (12.7 vs 15.2; β coefficient = − 1.92; p < 0.001). The mean score and adjusted regression scores in the language domain were also significant between the two groups (6.4 vs 8.5; β coefficient = − 1.80; p < 0.001). The mean score and adjusted regression score in the socio-emotional domain were also significant between the groups (15.4 vs 17.7; β coefficient = − 3.96; p < 0.001). Mean score and adjusted regression score in the general behavior domain were significant when a mother had persistent depression vs no depression (5.9 vs 10.4; β coefficient = − 3.96; p < 0.001) (Table 4 and Fig. 2).
Discussion
In this study, the prevalence of postpartum depressive symptoms persisted at 7, 45, and 90 days with similar prevalence rates, indicating that maternal stress remains high during the postpartum period. In the study cohort, one in nine infants had neurodevelopmental delay at 6 months, and the risk increased fivefold for infants born to mothers with persistent depressive symptoms up to 90 days. Due to the persistence of maternal depressive symptoms, the infants were delayed in all four functional domains, but more so in the general behavioral and social-emotional domains. Delayed infant neurodevelopment was higher among women who were from socially disadvantaged populations, had no maternal education, and were born preterm.
As the study result shows, the early infancy is a time of major transition in terms of physical and social maturation, which is influenced by the presence of maternal depression [29]. Persistent maternal depression may affect breastfeeding behavior and hinder infant stimulation and mother–child attachment, in line with our study, where the infant’s social-emotional domain and general behavior among those born to mothers with persistent depression were affected; a study in the United States reported that exposure to maternal depression was associated with difficulties in the development of infant’s social competence and emotional maturity [30]. Children exposed to maternal depression before the age of 5 had a higher risk of developmental vulnerability at school entry than children not exposed to maternal depression before the age of 5. A study in a Finnish cohort of 270 mother–child pairs showed that maternal postnatal depressive symptoms predicted low social competence in children. The children of mothers with depressive symptoms had lower problem-solving and externalizing scores than those of mothers without depression [31].
Similar to our findings of poor child development and behavioral problems in children born of mothers with postpartum depression, cohort studies in LMICs have reported similar results. A study in South Africa showed that children whose mothers had postpartum depression were more likely to have mental health problems later in life [32]. The study also showed that children from poor social groups had more social-emotional difficulties than those from relatively better social groups, which was also reported in our study. A study in Ethiopia showed that caretakers’ mental health had negative effects on personal-social, fine and gross motor, and language development [33]. The study also showed the difference in neurodevelopmental outcomes according to the sex of the infant as shown in our study. A country neighboring Nepal with similar study settings, India, has shown delayed neurodevelopment in infants whose mothers had postpartum depression [34]. This study in India also showed, as highlighted in our study, that prematurity and birth weight affect infant neurodevelopment, highlighting fetal growth as an important covariate for later development.
In settings such as Nepal, the early screening for postpartum depression has not been recommended in postpartum clinical care, resulting in early detection and management of postpartum depressive symptoms not being routine care [35]. Similarly, the system for detection and management of children with developmental delay is still under development in countries like Nepal, which mainly requires close interaction between the health and education sectors [36]. The World Health Organization recognizes maternal depression as a key health issue and recommends countries for early screening, referral, and management as part of routine postpartum care [37]. There is also a need to assess how improving the management of maternal depression reduces the risk of delayed early childhood development.
Methodological considerations
The maintenance of a cohort of mother-infant pairs who were observed at birth during the COVID-19 pandemic is one of the major strengths of the study. The enrolled mother-infants came from diverse populations representing different hospitals and community settings, which helped to generalize the result. To our knowledge, this is one of the largest cohort studies assessing persistent maternal depression in Southeast Asia, which contributes to the generalizability of the findings. The study did not collect data on breastfeeding status at the time of IYCD assessment at 6 months, which was a major limitation, as breastfeeding, especially exclusive breastfeeding, is a meditator to maternal postpartum depression and infant neurodevelopmental status. A major limitation is that we did not assess maternal antepartum depression, which is a strong correlate of postpartum depression and has also been associated with neurodevelopmental delays [38]. Third, the IYCD is a mother-reported measure of infant neurodevelopment function and has a lower sensitivity than developmental assessment conducted using structured tools such as the Malawi Development Assessment Tool (MDAT) [39]. Finally, attrition from 2022 participants enrolled to 1253 followed up at 6 months may have introduced to sampling bias. However, when we compared the population characteristics between those lost to follow-up and those who were followed up, there was no difference in maternal ethnicity, maternal age, birth complications, and prematurity, but there was difference in infant sex (Additional file 1: Table S4).
Conclusions
The burden of persistent maternal depression and its interlinkage with delayed infant neurodevelopment will have an unprecedented societal public health impact. The vicious cycle between poor maternal mental health and poor child developmental outcomes will be detrimental to the family and society. There is a need to further develop interventions to improve both maternal mental health and infant development through a common clinical setting so that mothers attending postpartum follow-up are screened for depressive symptoms, while infants are screened for functional neurodevelopment.
Availability of data and materials
The dataset generated and analyzed is available and provided on request.
Abbreviations
- aRR:
-
Adjusted risk ratio
- CI:
-
Confidence interval
- EPDS:
-
Edinburgh Postnatal Depression Scale
- GLM:
-
Generalized linear modeling
- IYCD:
-
Infant and Young Child Develop Tool
- LMIC:
-
Low- and middle-income countries
- MDAT:
-
Malawi Development Assessment Tool
- SDG:
-
Sustainable development goal
References
Wang ZY, Liu JY, Shuai H, Cai ZX, Fu X, Liu Y, Xiao X, Zhang WH, Krabbendam E, Liu S, et al. Mapping global prevalence of depression among postpartum women. Transl Psychiatry. 2021;11(1):543.
Al-Abri K, Edge D, Armitage CJ. Prevalence and correlates of perinatal depression. Soc Psychiatry Psychiatr Epidemiol. 2023;58(11):1581-90.
Bhusal BR, Bhandari N. Identifying the factors associated with depressive symptoms among postpartum mothers in Kathmandu, Nepal. Int J Nurs Sci. 2018;5(3):268–74.
Khadka R, Hong SA, Chang YS. Prevalence and determinants of poor sleep quality and depression among postpartum women: a community-based study in Ramechhap district, Nepal. Int Health. 2020;12(2):125–31.
Sameroff A. The transactional model of development: how children and contexts shape each other. American Psychological Association; 2009.
Brentani A, Fink G. Maternal depression and child development: evidence from Sao Paulo’s Western Region Cohort Study. Rev Assoc Med Bras (1992). 2016;62(6):524–9.
Comaskey B, Roos NP, Brownell M, Enns MW, Chateau D, Ruth CA, Ekuma O. Maternal depression and anxiety disorders (MDAD) and child development: a Manitoba population-based study. PLoS One. 2017;12(5):e0177065.
Koutra K, Roumeliotaki T, Kyriklaki A, Kampouri M, Sarri K, Vassilaki M, Bitsios P, Kogevinas M, Chatzi L. Maternal depression and personality traits in association with child neuropsychological and behavioral development in preschool years: mother-child cohort (Rhea Study) in Crete, Greece. J Affect Disord. 2017;217:89–98.
Rogers A, Obst S, Teague SJ, Rossen L, Spry EA, Macdonald JA, Sunderland M, Olsson CA, Youssef G, Hutchinson D. Association between maternal perinatal depression and anxiety and child and adolescent development: a meta-analysis. JAMA Pediatr. 2020;174(11):1082–92.
Black MM, Walker SP, Fernald LCH, Andersen CT, DiGirolamo AM, Lu CL, McCoy DC, Fink G, Shawar YR, Shiffman J, et al. Early childhood development coming of age: science through the life course. Lancet. 2017;389(10064):77–90.
Richter LM, Daelmans B, Lombardi J, Heymann J, Boo FL, Behrman JR, Lu CL, Lucas JE, Perez-Escamilla R, Dua T, et al. Investing in the foundation of sustainable development: pathways to scale up for early childhood development. Lancet. 2017;389(10064):103–18.
Shonkoff JP, Radner JM, Foote N. Expanding the evidence base to drive more productive early childhood investment. Lancet. 2017;389(10064):14–6.
Britto PR, Lye SJ, Proulx K, Yousafzai AK, Matthews SG, Vaivada T, Perez-Escamilla R, Rao N, Ip P, Fernald LCH, et al. Nurturing care: promoting early childhood development. Lancet. 2017;389(10064):91–102.
National Inst of Child Health & Human Development, Early Child Care Research Network. (1999). Chronicity of maternal depressive symptoms, maternal sensitivity, and child functioning at 36 months. Dev Psychol. 1999;35(5):1297–1310.
Slomian J, Honvo G, Emonts P, Reginsteri JY, Bruyere O. Consequences of maternal postpartum depression: a systematic review of maternal and infant outcomes. Womens Health. 2019;15:1745506519844044.
Beck CT. The effects of postpartum depression on child development: a meta-analysis. Arch Psychiat Nurs. 1998;12(1):12–20.
Singh DR, Sunuwar DR, Adhikari S, Singh S, Karki K. Determining factors for the prevalence of depressive symptoms among postpartum mothers in lowland region in southern Nepal. PloS One. 2021;16(1):e0245199.
Giri RK, Khatri RB, Mishra SR, Khanal V, Sharma VD, Gartoula RP. Prevalence and factors associated with depressive symptoms among post-partum mothers in Nepal. BMC Res Notes. 2015;8:111.
Fisher J, Cabral de Mello M, Patel V, Rahman A, Tran T, Holton S, Holmes W. Prevalence and determinants of common perinatal mental disorders in women in low- and lower-middle-income countries: a systematic review. Bull World Health Organ. 2012;90(2):139G-149G.
Gurung R, Gurung A, Basnet O, Eilevstjonn J, Myklebust H, Girnary S, Shrestha SK, Singh D, Bastola L, Paudel P, et al. REFINE (Rapid Feedback for quality Improvement in Neonatal rEsuscitation): an observational study of neonatal resuscitation training and practice in a tertiary hospital in Nepal. BMC Pregnancy Childbirth. 2020;20(1):756.
Gurung R, Jha AK, Pyakurel S, Gurung A, Litorp H, Wrammert J, Jha BK, Paudel P, Rahman SM, Malla H, et al. Scaling Up Safer Birth Bundle Through Quality Improvement in Nepal (SUSTAIN)-a stepped wedge cluster randomized controlled trial in public hospitals. Implement Sci. 2019;14(1):65.
Kc A, Acharya A, Bhattarai P, Basnet O, Shrestha A, Rijal G, Skalkidou A. Association of disrespectful care after childbirth and COVID-19 exposure with postpartum depression symptoms- a longitudinal cohort study in Nepal. BMC Pregnancy Childbirth. 2023;23(1):145.
Bhusal BR, Bhandari N, Chapagai M, Gavidia T. Validating the Edinburgh Postnatal Depression Scale as a screening tool for postpartum depression in Kathmandu, Nepal. Int J Ment Health Sy. 2016;10:71.
Ho-Yen SD, Bondevik GT, Eberhard-Gran M, Bjorvatn B. The prevalence of depressive symptoms in the postnatal period in Lalitpur district, Nepal. Acta Obstet Gyn Scan. 2006;85(10):1186–92.
Lancaster GA, McCray G, Kariger P, Dua T, Titman A, Chandna J, McCoy D, Abubakar A, Hamadani JD, Fink G, et al. Creation of the WHO Indicators of Infant and Young Child Development (IYCD): metadata synthesis across 10 countries. BMJ Glob Health. 2018;3(5):e000747.
Gladstone M, Lancaster G, McCray G, Cavallera V, Alves CRL, Maliwichi L, Rasheed MA, Dua T, Janus M, Kariger P. Validation of the infant and young child development (IYCD) indicators in three countries: Brazil, Malawi and Pakistan. Int J Environ Res Public Health. 2021;18(11):6117.
IBM Corp. Released. IBM SPSS Statistics for Windows, Version 29.0.2.0 Armonk: IBM Corp; 2023.
R Core Team. _R: A Language and Environment for Statistical Computing_. Vienna: R Foundation for Statistical Computing; 2023.
Culp AM. The transactional model of development: how children and contexts shape each other. Infant Ment Health J. 2010;31(1):115–7.
Wall-Wieler E, Roos LL, Gotlib IH. Maternal depression in early childhood and developmental vulnerability at school entry. Pediatrics. 2020;146(3):e20200794.
Luoma I, Tamminen T, Kaukonen P, Laippala P, Puura K, Salmelin R, Almqvist F. Longitudinal study of maternal depressive symptoms and child well-being. J Am Acad Child Adolesc Psychiatry. 2001;40(12):1367–74.
Verkuijl NE, Richter L, Norris SA, Stein A, Avan B, Ramchandani PG. Postnatal depressive symptoms and child psychological development at 10 years: a prospective study of longitudinal data from the South African Birth to Twenty cohort. Lancet Psychiatry. 2014;1(6):454–60.
Hadley C, Tegegn A, Tessema F, Asefa M, Galea S. Parental symptoms of common mental disorders and children’s social, motor, and language development in sub-Saharan Africa. Ann Hum Biol. 2008;35(3):259–75.
Patel V, DeSouza N, Rodrigues M. Postnatal depression and infant growth and development in low income countries: a cohort study from Goa, India. Arch Dis Child. 2003;88(1):34–7.
Cavallera V, Tomlinson M, Radner J, Coetzee B, Daelmans B, Hughes R, Perez-Escamilla R, Silver KL, Dua T. Scaling early child development: what are the barriers and enablers? Arch Dis Child. 2019;104:S43–50.
Milner KM, Salazar RB, Bhopal S, Brentani A, Britto PR, Dua T, Gladstone M, Goh E, Hamadani J, Hughes R, et al. Contextual design choices and partnerships for scaling early child development programmes. Arch Dis Child. 2019;104:S3–12.
The Lancet. Adolescence: a second chance to tackle inequities, The Lancet. 2013;382(9904):1535
Fransson E, Sorensen F, Kallak TK, Ramklint M, Eckerdal P, Heimgartner M, Krageloh-Mann I, Skalkidou A. Maternal perinatal depressive symptoms trajectories and impact on toddler behavior ? the importance of symptom duration and maternal bonding. J Affect Disorders. 2020;273:542–51.
Gladstone M, Lancaster GA, Umar E, Nyirenda M, Kayira E, van den Broek NR, Smyth RL. The Malawi Developmental Assessment Tool (MDAT): the creation, validation, and reliability of a tool to assess child development in rural African settings. PloS Medicine. 2010;7(5):e1000273.
Acknowledgements
We would like to thank Omkar Banset, Honey Malla, Avinash K Sunny, Prajwal Paudel, and Pratiksha Paudel and surveillance officers, the hospital manager, the nurse in charge, all the nurses, and support staff working in the labor and delivery unit during this unprecedented time. We would like to thank Richard White for his statistical advice and revision of the statistics.
Funding
Open access funding provided by University of Gothenburg. For this study, no funding was available.
Author information
Authors and Affiliations
Contributions
AKC and AS conceptualized the study. AA conducted the first draft of the analysis, and AKC conducted the second draft of the analysis. AKC conducted the first draft of the manuscript. AS, RG, JC, and CA authors provided input in the first draft. AS and AKC conducted the third and final draft of the analysis. All authors read and approved the final manuscript.
Authors’ X handles
@Ashish_K_C, @jayachandna, @RejinaGurung3, @ASkalkidou.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethical committee of the Nepal Health Research Council (439/2020). Written consents were obtained from all women before participation in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
KC, A., Chandna, J., Acharya, A. et al. A longitudinal multi-centric cohort study assessing infant neurodevelopment delay among women with persistent postpartum depression in Nepal. BMC Med 22, 284 (2024). https://doi.org/10.1186/s12916-024-03501-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-024-03501-0