
Abstract
Background
Syndromic surveillance often relies on patients presenting to healthcare. Community cohorts, although more challenging to recruit, could provide additional population-wide insights, particularly with SARS-CoV-2 co-circulating with other respiratory viruses.
Methods
We estimated the positivity and incidence of SARS-CoV-2, influenza A/B, and RSV, and trends in self-reported symptoms including influenza-like illness (ILI), over the 2022/23 winter season in a broadly representative UK community cohort (COVID-19 Infection Survey), using negative-binomial generalised additive models. We estimated associations between test positivity and each of the symptoms and influenza vaccination, using adjusted logistic and multinomial models.
Results
Swabs taken at 32,937/1,352,979 (2.4%) assessments tested positive for SARS-CoV-2, 181/14,939 (1.2%) for RSV and 130/14,939 (0.9%) for influenza A/B, varying by age over time. Positivity and incidence peaks were earliest for RSV, then influenza A/B, then SARS-CoV-2, and were highest for RSV in the youngest and for SARS-CoV-2 in the oldest age groups. Many test positives did not report key symptoms: middle-aged participants were generally more symptomatic than older or younger participants, but still, only ~ 25% reported ILI-WHO and ~ 60% ILI-ECDC. Most symptomatic participants did not test positive for any of the three viruses. Influenza A/B-positivity was lower in participants reporting influenza vaccination in the current and previous seasons (odds ratio = 0.55 (95% CI 0.32, 0.95)) versus neither season.
Conclusions
Symptom profiles varied little by aetiology, making distinguishing SARS-CoV-2, influenza and RSV using symptoms challenging. Most symptoms were not explained by these viruses, indicating the importance of other pathogens in syndromic surveillance. Influenza vaccination was associated with lower rates of community influenza test positivity.
Similar content being viewed by others


Background
Influenza and other respiratory illnesses place large burdens on patients and healthcare [1, 2]. Understanding within-season dynamics is critical to healthcare preparedness and vaccination planning. Routine syndromic and laboratory surveillance is commonly conducted using patients attending community doctors, hospitals, and ambulance services [3], thus being skewed towards symptomatic and more severe cases, and influenced by differential health-care-seeking behaviours [4]. This approach may underestimate the community burden of seasonal influenza, as most cases are mild and/or asymptomatic [5]. Alternative data sources include community surveys, e.g. the UK’s online participatory surveillance system ‘Flusurvey’ [6]. While such cohorts may provide better population-wide estimates, including mild illness, they may still not be representative, tending to underrepresent young children and older adults, both with higher risks of respiratory illness and distinct symptom patterns [7, 8].
Another challenge is the reliance on indicators such as influenza-like illness (ILI) in the absence of virological confirmation [9]. The relationship between ILI and influenza positivity remains complex, influenced by differing case definitions [10, 11], changes in co-circulation of other viruses (notably respiratory syntactical virus (RSV) and SARS-CoV-2) across seasons [12, 13], age-specific dynamics [14], and the non-specific nature of influenza symptoms [15, 16]. Various studies have attempted to assess these relationships, but most have limited their scope to clinical settings, and/or focussed solely on influenza, and/or restricted to patients already reporting ILI or Acute Respiratory Illness (ARI) [7,8,9, 12,13,14, 17, 18]. Similarly, influenza vaccine effectiveness evaluation typically uses disease endpoints, rather than protection from infection [19].
Here we use the Office of National Statistics (ONS) COVID-19 Infection Survey (CIS) to investigate the relationship between respiratory infection test positivity and ILI/other self-reported symptoms. This survey differs from sentinel laboratory surveillance in that routine nose and throat swab testing for SARS-CoV-2 (and on a smaller sub-sample, also for influenza A/B and RSV) was conducted on a community cohort, approached at random from address lists, not limited to those contacting healthcare services or with specific case presentations. We estimated SARS-CoV-2, influenza and RSV positivity and incidence across the 2022/2023 winter season, assessed associations between specific symptoms and test positivity, and evaluated the effects of influenza vaccination on positivity.
Methods
The ONS COVID-19 Infection Survey (CIS)
CIS was a large longitudinal household survey, broadly representative of the wider UK population (Additional file 1: Supplementary Methods [20]), conducting polymerase chain reaction (PCR) tests for SARS-CoV-2 on self-collected nose and throat swabs and collecting questionnaire data including demographics and symptoms approximately monthly (Additional file 1: Supplementary Methods [21]). The study received ethical approval from the South Central Berkshire B Research Ethics Committee (20/SC/0195). From October 2022, a random subset of ~ 750 swabs received per week were additionally tested by multiplex PCR (ThermoFisher TaqPath™ COVID-19, Flu A/B, RSV ComboKit) in a respiratory pilot study [22]. We analysed swabs taken from 10 October 2022 to 26 February 2023 (≥ 350 respiratory pilot samples/week; ≤ 40 pilot samples/week outside this), when all survey assessments were conducted remotely, either online or by telephone, with swab kits posted to participants and returned by post/courier.
Self-reported symptoms
Each month, participants were asked whether they had experienced specific symptoms during the last seven days [23]. This analysis included 12 symptoms solicited from the survey start (cough, sore throat, loss of taste, loss of smell, shortness of breath, fever, muscle ache (myalgia), weakness/tiredness (fatigue), headache, nausea/vomiting, abdominal pain, and diarrhoea) and four added September 2021 (wheezing, sneezing, ‘more trouble sleeping than usual’, and ‘loss of appetite or eating less than usual’), but excluded seven unrelated to respiratory illness added January 2022. Influenza-like illness (ILI) was defined using the World Health Organisation (WHO) (concurrent fever and cough) [24] and the European Centre for Disease Prevention and Control (ECDC) (co-presence of ≥ 1 respiratory symptom (cough, sore throat, shortness of breath) and ≥ 1 systemic symptom (fever, fatigue, headache, myalgia)) [25] definitions.
Statistical methods
Positivity and incidence
In order to quantify the trends in symptoms and test positivity over time, by age group and overall, we estimated the percentage reporting different symptoms including ILI, and positivity for SARS-CoV-2 (full sample) and influenza A/B and RSV (respiratory pilot only), using negative binomial (log link) Generative Additive Models (GAM) (R mgcv package [26]). We used a single explanatory variable for calendar time in days modelled with thin plate splines penalised on the third derivative [27] with k = 45 basis functions determining smoothness (approximately total study days(140)/3). Given expected variation, full sample models were run separately for six age groups (2–6SY (school year, ~ 11 years, Additional file 1: Supplementary Methods), 7SY–11SY, 12SY–34, 35–49, 50–64, and 65 +), collapsing to three wider age-groups (2–11SY, 12SY–49, 50 +) for the smaller respiratory pilot. Our focus was on estimating daily trends and how these varied over time: we therefore made a generalisability assumption that the cohort, recruited predominantly from address lists (see Additional file 1: Supplementary Methods) was broadly representative, rather than attempting to use weights (which would have needed to be calculated daily) or post-stratification [28] which could only be done by region, sex, age and ethnicity given lack of available data on the distribution of other factors in the target population. The latter would have required complex interactions between each factor and time which can have convergence problems [21].
In order to estimate incidence from SARS-CoV-2, influenza A/B, and RSV positivity collected in the respiratory pilot study, we used the Richardson-Lucy-type deconvolution. Deconvolution was performed based on daily estimates of test positivity and the distribution of infection (PCR positivity) duration [29, 30], using 10,000 simulations from the posterior GAM distributions (details in Additional file 1: Supplementary Methods). Incidence is presented from 24 October 2022 to 12 February 2023 (weeks 3–18 of the respiratory pilot) as deconvolution tail estimates are highly uncertain. The infection duration was modelled using a Weibull distribution approximating ILI duration for ‘Flusurvey’ respondents [31] (shape and scale parameters to match reported median (9 days) and IQR (reported = 6–15 days, approximated = 5–15 days). Due to insufficient data on appropriate distributions for influenza and RSV in community settings, other infection duration distributions were considered in sensitivity analyses (Additional file 1: Table S1) [32,33,34,35,36].
Self-reported symptoms, ILI and test positivity
In order to assess the association between self-reported symptoms and test positivity, we estimated a series of GAMs. The probability of testing SARS-CoV-2-positive by age, conditional on reporting specific symptoms, was estimated for the full CIS sample using logistic GAMs. Similar models in the respiratory pilot expanded the outcome to testing positive for influenza A/B, RSV, or SARS-CoV-2, versus no virus identified, using multinomial GAMs (assigning 12 respiratory pilot samples positive for two viruses to the virus with the lowest cycle threshold (Ct) value). Both models included smooths for age and, for SARS-CoV-2 positivity in the larger sample, also calendar time, making predictions at 15 December 2022 to illustrate the contribution of SARS-CoV-2 to reported symptoms when all three pathogens’ positivity was relatively high. We used negative binomial GAMs to estimate the percentage self-reporting ILI and other symptoms by age amongst those testing positive or negative for SARS-CoV-2 in the full sample, and testing positive for influenza A/B and RSV in the respiratory pilot, averaged across the study period. Observations with missing data on self-reported symptoms (< 3%) were excluded from these analyses.
Influenza vaccination
To assess the effect of self-reported influenza vaccination on influenza A/B, RSV, and SARS-CoV-2 positivity, we used logistic GAMs controlling for demographics (age, sex, household size (1, 2, 3 +), ethnicity (white versus non-white due to small numbers), ever worked in patient-facing healthcare, ever reported long-term health conditions, SARS-CoV-2 vaccination and prior SARS-CoV-2 infection (details in Additional file 1: Supplementary Methods)). All models included smooths for calendar time, age, days since the most recent SARS-CoV-2 vaccination, and days since the start of the most recent SARS-CoV-2 infection (the last two truncated at 365 days (reference category), also with binary variables for unvaccinated or non-infected versus ≥ 365 days). Influenza vaccination was self-reported (“Have you received a flu vaccination since the last assessment” Yes/No/Missing). As the vaccination date was not elicited, participants were considered vaccinated if they had reported an influenza vaccination at a strictly prior assessment, or at the current assessment if the prior assessment was > 45 days ago. Very few participants (< 3%) reported influenza vaccination in 22/23 only (Table 1), so these were categorised in models with “Both 22/23 and 21/22”.
Results
Trends in test positivity for SARS-CoV-2, influenza, RSV, and self-reported ILI
Between 10 October 2022 and 26 February 2023, the 20-week period when additional influenza/RSV surveillance was conducted and when BQ.1, CH.1.1 and XBB SARS-CoV-2 sub-lineages were co-circulating in the UK, 32,937 (2.4%) of 1,352,979 swab tests conducted at study assessments were SARS-CoV-2-positive (median (IQR) 4 (3–4) tests/participant, 359,186 unique participants) (Table 1). 14,939 (1.1%) randomly selected swabs from 14,664 unique participants were tested in the respiratory pilot, with similar SARS-CoV-2 positivity (n = 354, 2.4%). RSV and influenza A/B positivity were lower, 1.2% (n = 181) and 0.9% (n = 130), respectively. There were 12 (0.08%) coinfections (4 SARS-CoV-2/influenza, 4 SARS-CoV-2/RSV, 4 influenza/RSV; 653 (4.4%) swabs positive for ≥ 1 of the three viruses). Of 130 influenza A/B positives, subtype could be identified from PCR for 87 (remainder too low viral load/high Ct to amplify); 80 (92.0%) were influenza A, 5 (5.7%) influenza B, and 2 (2.3%) both (from whole genome sequencing 8 H1N1, 40 H3N2, and 1 Victoria) [37]. Percentages reporting ILI over the study period were very similar between the respiratory pilot and full CIS sample, with only minor differences in sample demographics (Table 1).
SARS-CoV-2 positivity and reported ILI-WHO peaked in late December 2022, with similar trends across the pilot and full samples (Fig. 1). Both trends varied by age; SARS-CoV-2 positivity was higher for older versus younger participants, while reported ILI-WHO was higher amongst those in SY11 or younger. In the full sample, SARS-CoV-2 positivity was consistently higher than reported ILI-WHO amongst those ≥ 65 years, and trends in reported ILI-WHO were similar between those testing SARS-CoV-2 negative and positive. RSV and influenza positivity peaked earlier in December 2022, and also varied by age over time, with higher rates in younger children, and earlier peaks in RSV than influenza and SARS-CoV-2, particularly for those ≥ 50 years. Cycle threshold (Ct) values for SARS-CoV-2 followed positivity trends, being lower (i.e. higher viral load) when positivity was higher (Additional file 1: Fig. S1). ILI-ECDC was more common than ILI-WHO, but followed broadly similar trends over time; other symptoms were either approximately constant over time or had similar peaks around December 2022 (Additional file 1: Fig. S2–S4).

Percentage (95% CI) reporting ILI-WHO (full CIS and respiratory pilot) and test positivity for SARS-CoV-2 (full CIS and respiratory pilot), influenza A/B (respiratory pilot) and RSV (respiratory pilot). Note: SY, school year. See Additional file 1 for raw daily percentages for the full CIS sample (Additional file 1: Fig. S15) and cumulative numbers positive for SARS-CoV-2, influenza A/B and RSV, and reporting ILI-WHO in the respiratory pilot (Additional file 1: Fig. S16)
Incidence of SARS-CoV-2, influenza and RSV
Estimated incidence of SARS-CoV-2, influenza and RSV therefore also varied by age over time (Fig. 2). In those 2-11SY, peak estimated incidence was higher and occurred earlier for RSV and influenza than SARS-CoV-2 (Table 2), although overlapping credible intervals around estimated incidence over time indicated considerable uncertainty. For older age groups, peak estimated SARS-CoV-2 incidence was higher than RSV and influenza, but with similar shifts in timing (SARS-CoV-2 peaks occurring later than RSV and influenza). However, compared with younger children, peak RSV incidence was lower and slightly later in older age groups (by approximately 1 week), and peak daily influenza incidence also shifted later with increasing age, with 17 days difference between peak influenza incidence between the youngest (2–11SY) and oldest (50 +) age groups (Table 2). The choice of infection duration distribution did not alter the timing of the estimated peaks but influenced absolute incidence estimates (Additional file 1: Fig. S5). Distributions with lower mean duration resulted in higher incidence, by approximately the inverse ratio of means (as expected from first-order approximations), so were ~ 1.4 times higher using a distribution with mean 7.5 versus 10.4 days (Additional file 1: Table S1), although credible intervals overlapped for RSV and influenza.

Estimated incidence (95%CI) of SARS-CoV-2 (full CIS), RSV (respiratory pilot), and influenza A/B (respiratory pilot). Note: Time frame covering October 24, 2022–February 13, 2023. SY, school year. Estimates based on a Weibull-ILI survival curve for infection duration. See Additional file 1 for further details on survival distributions (Additional file 1: Table S1, Figure S5)
Association between test positivity and self-reported symptoms
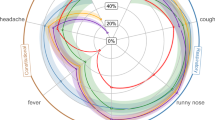
Considering age as a continuous variable (Fig. 3), over 50% of SARS-CoV-2-positives aged 30–70 years reported symptoms consistent with ILI-ECDC, compared to at most ~ 25% in those 30–65 years for ILI-WHO. ILI-ECDC symptoms were also more commonly reported than ILI-WHO amongst those testing positive for RSV or influenza, with ILI-WHO being particularly uncommon amongst RSV-positives, due to low rates of self-reported fever amongst RSV-positives across all ages. Cough and sore throat were amongst the most common symptoms for SARS-CoV-2-positives, with a prevalence of cough > 50% in those over ~ 20 years. However, in the youngest children, cough was almost as common in SARS-CoV-2-negatives as positives, consistent with multiple other causes. Sneezing, fatigue, and headache were other common symptoms amongst SARS-CoV-2-positives (Additional file 1: Fig. S6), with higher rates amongst middle-aged versus younger and older participants. As for SARS-CoV-2-positives, cough, sore throat, sneezing, fatigue and headache were amongst the most commonly reported symptoms for RSV- and influenza-positives, with broadly similar trends across age (Fig. 3, Additional file 1: Fig. S7), including most symptoms being more commonly reported amongst middle-aged participants. Most symptoms were more commonly reported in influenza- than RSV-positives, wheezing being the main exception, being more commonly reported in older participants testing positive for RSV than influenza or SARS-CoV-2. However, absolute percentages reporting wheezing were lower than for other symptoms, and confidence intervals were wide.

Prevalence of reported symptoms by SARS-CoV-2 test result (full CIS sample), and amongst those testing positive for RSV and influenza A/B (respiratory pilot). Note: See Additional file 1: Fig. S6–S7 for the remaining symptoms. Predictions are averaged across time (no smooth for calendar time included in models). The respiratory pilot analysis excluded loss of smell due to the small absolute number of participants reporting this symptom. Predictions were restricted to ages 10–75 years for the respiratory pilot due to the small absolute number outside this range (approximate 5th–95th percentiles), and 5–85 years for the full CIS (approximate 1st–99th percentiles)
Association between self-reported symptoms and test positivity
Nevertheless, whether symptoms were defined by either ILI definition or individually, most (> 65%) symptomatic (community-based) participants were not positive for SARS-CoV-2, influenza A/B, or RSV (Fig. 4, Additional file 1: Fig. S8–S9). The predicted probability of testing SARS-CoV-2-positive given specific symptoms generally increased with age and was higher for ILI-WHO than ILI-ECDC. This appeared to be driven by higher probabilities of SARS-CoV-2 amongst participants reporting fever, the individual symptom with the largest percentage of confirmed viral cases in the full and respiratory pilot samples (Fig. 4). The respiratory pilot estimates suggested that, beyond SARS-CoV-2, RSV and influenza could only explain minor additional fractions of reported symptoms (Fig. 4, Additional file 1: Fig. S9). Further, the probability of confirmed influenza infection tended to decrease with age amongst symptomatic participants, compared to the increasing trend for SARS-CoV-2, although uncertainty was relatively large (Additional file 1: Fig. S10).

For participants reporting selected symptoms, predicted probabilities of a positive test result for SARS-CoV-2 on 15 December 2022 (full CIS sample), and for SARS-CoV-2, influenza A/B or RSV (respiratory pilot sample), by age. Note: See Additional file 1: Fig. S8–S9, for the remaining symptoms. Predictions for the full CIS sample were made on 15 December 2022 from models which adjusted for time, results for additional dates are shown in Additional file 1: Fig. S17. Predictions for the respiratory pilot are from a model not adjusted for time (given the limited sample size) and therefore represent an overall average over time. Predictions were made for ages 5–85 (approx. 1st–99th percentiles)
Influenza vaccination
In the respiratory pilot (winter 22/23), influenza A/B positivity was significantly lower for those reporting influenza vaccination both in the current 22/23 and prior 21/22 season versus not reporting influenza vaccination in either season (adjusted OR = 0.55 (95% CI 0.32, 0.95)); there was no evidence of association with influenza vaccination only in the past 21/22 season (aOR = 0.81 (0.52, 1.26), heterogeneity p = 0.125) (Table 3, Additional file 1: Fig. S11). Influenza A/B positivity was higher in those working in patient-facing healthcare (aOR = 2.51 (1.31, 4.79)). There was very weak evidence of interaction between vaccination status and age for influenza vaccination in the current and previous seasons (categorising as ≥ versus < 18 years heterogeneity p = 0.541 and 0.113, respectively, Additional file 1: Table S2). Including a continuous interaction with age (Additional file 1: Fig. S12), the decreased risk associated with current and previous vaccination was greatest amongst young children and older adults. There was no evidence of association between influenza vaccination and RSV positivity or between prior SARS-CoV-2 infection or vaccination and influenza A/B or RSV positivity (Table 3, Additional file 1: Fig. S11, S13). Interestingly, in the much larger full sample, influenza vaccination in the current and prior season was associated with a slightly elevated risk of SARS-CoV-2-positivity (aOR = 1.10 (1.05, 1.14)), and similarly only in the prior season (aOR = 1.09 (1.05, 1.13)), heterogeneity p = 0.688), consistent with competing risks between SARS-CoV-2 and influenza or influenza vaccination targeting those most vulnerable to respiratory infection (Table 3). We found evidence of waning protection against SARS-CoV-2 positivity over time from previous SARS-CoV-2 vaccination, and from previous SARS-CoV-2 infection after the initial period of PCR positivity (Additional file 1: Fig. S14). Those never previously infected with SARS-CoV-2 had a slightly increased risk of SARS-CoV-2 positivity compared to those last infected > 365 days ago (reference category) (aOR = 1.10 (1.06, 1.14)), with risk of reinfection increasing over time from previous test positivity in those last infected < 365 days ago (Additional file 1: Fig. S14). However, those not reporting prior SARS-CoV-2 vaccination had a slightly lower risk compared to those last vaccinated > 365 days ago (reference category) (aOR = 0.81 (0.75, 0.88)).
Discussion
Positivity and incidence
Estimates from the full ONS CIS and its respiratory pilot suggest that positivity and incidence of SARS-CoV-2, influenza, and RSV varied by age and time across the 22/23 winter season. Peak incidence rates appeared somewhat delayed with increasing age for each virus, but particularly for influenza, with peaks observed approximately 2 weeks later for those 50 years + versus children 11SY or below. RSV peaked before influenza, and then SARS-CoV-2 in each age group, although peaks were relatively close. Increasing influenza cases amongst children could hence provide an early warning for older age groups, consistent with the former being the key driver of influenza transmission [38], and supporting early timing of child vaccination programmes to reduce overall transmission. We also observed higher RSV positivity and incidence for those 2–11SY versus older age groups, and lower influenza positivity/incidence for those ≥ 50 years.
Symptoms and test positivity
A large fraction of symptoms reported by participants could not be attributed to test positivity for SARS-CoV-2, influenza A/B or RSV. This highlights the role of other infections not included in this study in symptom trends, including rhinovirus, adenovirus, human metapneumovirus, and parainfluenza as identified in syndromic surveillance [39], plus bacterial causes [40]. Given the high prevalence of background symptoms observed in SARS-CoV-2-negatives, the symptoms reported by test positives for SARS-CoV-2, influenza A/B or RSV may not necessarily be caused by these infections specifically. That is, test positives for any of these three infections could even be reporting symptoms that are caused by co-infections with e.g. rhinovirus, rather than by SARS-CoV-2, influenza A/B, or RSV specifically.
RSV-positives generally tended to report fewer symptoms than SARS-CoV-2 or influenza-positives, but symptomatology generally appeared more strongly influenced by age than aetiology. Cough, sore throat, sneezing, fatigue and headache were all amongst the most commonly reported symptoms for each of the three infections, suggesting that discriminating between SARS-CoV-2, influenza and RSV based on symptoms alone may prove challenging, with implications for antiviral treatment and testing. Overall, our findings highlight that in the community, the contributions of these three pathogens to overall symptomatology appear modest. While ILI-ECDC was more commonly reported than ILI-WHO across all ages for the three infections, only ~ 15% of reported ILI-ECDC could be explained by test positivity for SARS-CoV-2, influenza A/B, or RSV. Prior studies have found higher rates of respiratory test positivity amongst those reporting ILI (and conversely, higher rates of ILI amongst influenza-positives), yet these estimates have generally been based on patients presenting to healthcare with symptoms of respiratory infection [8, 9, 12,13,14, 17, 18, 41]. Such samples will be skewed towards more severe cases, as individuals with milder disease are less likely to seek healthcare. For instance, Casalegno et al. found that 90% of influenza-positives in their study reported cough [8], a considerably higher fraction than our equivalent estimate of ~ 50%, yet this study was restricted to patients presenting to physicians with ARI. On the other hand, a study by Jiang et al. with a comparable design to ours (self-reported symptoms in a community sample regularly tested for influenza A), found that influenza cases accounted for 18% of ILI-ECDC [11], an estimated more in line with our findings.
Careful consideration of background rates and age-specific dynamics are thus necessary when using self-reported symptoms from community cohorts as a surveillance method for respiratory illness, highlighting the potential benefits of more flexible ILI definitions [7, 15]. This finding also underscores the consideration needed when applying ILI definitions in a ‘true community’ context, where the likelihood of milder (and asymptomatic) infection is much higher than in the healthcare settings where surveillance studies are normally performed. Our findings of higher rates of self-reported symptoms in middle-aged participants, broadly consistent across symptoms and the three infections studied, also raise important questions regarding the role of age in infection susceptibility, illness natural history, reporting behaviour, and vulnerability to other symptom-inducing conditions.
Although we confirmed previous findings of high rates of cough in test-negatives [14], we also found evidence of particularly high rates in older RSV-positives. This was the only symptom that approached rates of 50% amongst RSV-positives and confirms prior findings of cough’s relevance to RSV discrimination [12, 42, 43]. In contrast, fever was rarely reported amongst RSV-positives across all ages. Fever has previously been identified as an important predictor of influenza [14, 16, 41], and we also found it was more commonly reported with influenza than SARS-CoV-2 or RSV for those < 20 years. Consequently, fever may have a higher value for predicting influenza in children, yet it was also relatively common amongst SARS-CoV-2-positives. ILI-WHO and ILI-ECDC were similarly reported in SARS-CoV-2-positives and influenza-positives, indicating that the emergence of SARS-CoV-2 may complicate surveillance specifically targeting influenza. As previously suggested, ILI-WHO appears poorly suited to monitor RSV in the community [44,45,46], due to its inclusion of fever.
Limitations
Lower specificity and sensitivity of ILI definitions in our community sample compared to those presenting to clinical settings is perhaps unsurprising; however, one limitation is that the approximate monthly testing intervals in the full sample (from which the respiratory pilot was randomly selected) may also have affected the likelihood of symptom reporting, since questionnaires elicited symptoms in the last 7 days. For example, the design will have resulted in cases being identified at differing timepoints in their infection, so that those in a later stage of illness (or experiencing prolonged viral shedding) may appear asymptomatic at assessment although having experienced symptoms earlier in their infection, or may not test positive any longer despite still having symptoms. When positivity rates were low, Ct values supported a larger fraction of cases being identified late in infection (Additional file 1: Fig. S1). Another limitation is that we lacked information on the onset of individual symptoms, as all symptoms experienced within the past week were jointly reported. Further, the likelihood of reporting symptoms consistent with ILI is affected by other demographic factors including gender [47]; we chose to focus on age as the main determinant of symptomatology, determinant of vaccination strategies and hence target of surveillance.
The main limitation is the smaller sample size in the respiratory pilot (which still tested ~ 15,000 swabs), leading to greater uncertainty given the low event rates of RSV and influenza A/B. Although much smaller than the sample tested for SARS-CoV-2, this was still one of the larger community studies to date. Although broadly representative, non-white ethnicities and younger ages remained slightly under-represented, and SARS-CoV-2 vaccination was slightly over-represented (although this has been shown to have short-lived effects on infection). Future studies could try to use modelling techniques such as post-stratification [28] or survey weights to assess the potential impact of disproportional representation of i.e. older ages on positivity and incidence estimates, although these have challenges (see the “Methods” section). Similarly, the limited data on infection duration distributions for RSV and influenza meant incidence estimates were approximate, although the choice of distribution affected absolute levels rather than relative rates or timing of peaks. Furthermore, the 22/23 winter season may not yet equate to steady-state post-pandemic mixing patterns in older adults [48]. Influenza A and B were not differentiated in the multiplex assay, although the vast majority were A on further PCR (only successful in 67%), and we did not consider the impact of SARS-CoV-2 variant on symptomatology. During the study period, BQ.1, CH1.1 and XBB sub-lineages were co-circulating, and the high Ct values (low viral load) of many SARS-CoV-2-positives precluded universal sequencing to identify variants. Nevertheless, prior studies suggest that any symptom differences between influenza A and B are due to age and other risk factors [8, 9].
Influenza vaccination
We found that influenza vaccination in both the current (22/23) and prior (21/22) seasons was associated with ~ 45% protection against influenza test positivity in this general community sample, with no evidence of the effect of vaccination in the prior season (21/22) only (point estimate ~ 20% reduction). Numbers were too few to robustly assess the impact of vaccination in 22/23 only, although a recent test-negative case–control study suggested this group could have slightly greater benefit [49]. Similarity in influenza strains included in the vaccine across the two seasons means that prior vaccination might have conferred some protection in the 22/23 season [50]. The main influenza strains circulating in the 21/22 and 22/23 seasons were similar, with influenza A (H3N2) being the predominant subtype. In both seasons, the H3N2 strain recommended in the northern hemisphere influenza vaccines (A/Cambodia in 21/22 and A/Darwin in 22/23) also belonged to the same genetic subclade (3C.2a1b) [38, 51]. Alternatively, behavioural patterns or other factors differentiating those choosing vaccination could affect positivity. While live attenuated influenza vaccine (LAIV) could lead to vaccination-induced test positivity in children < 18 years, our estimates of protection were similar restricting to ≥ 18 years, suggesting that effects of vaccination can still be identified in relatively small community cohorts.
Conclusions
In conclusion, our findings highlight the complex relationship between trends in test positivity for RSV, influenza A/B, and SARS-CoV-2, which peaked successively over the 22/23 winter season but to different degrees in different age groups, and self-reported symptoms. Symptom profiles varied more by age than aetiology, making distinguishing between SARS-CoV-2, influenza and RSV on symptoms alone challenging, and most reported symptoms could not be explained by these viruses. Our findings emphasise the value of community-level data in understanding symptomatology in cases beyond those presenting to healthcare services and have implications for COVID-19 contingency planning, particularly in regards to the percentages not reporting respiratory symptoms.
Availability of data and materials
De-identified study data are available for access by accredited researchers in the ONS Secure Research Service (SRS) for accredited research purposes under part 5, chapter 5 of the Digital Economy Act 2017. For further information about accreditation, contact research.support@ons.gov.uk or visit the SRS website.
Abbreviations
- ARI:
-
Acute respiratory illness
- CIS:
-
COVID-19 infection survey
- Ct:
-
Cycle threshold
- ECDC:
-
European Centre for Disease Prevention and Control
- GAM:
-
Generative additive models
- ILI:
-
Influenza-like illness
- ONS:
-
Office of National Statistics
- PCR:
-
Polymerase chain reaction
- RSV:
-
Respiratory syncytial virus
- SY:
-
School year
- WHO:
-
World Health Organisation
References
Moss JWE, Davidson C, Mattock R, Gibbons I, Mealing S, Carroll S. Quantifying the direct secondary health care cost of seasonal influenza in England. BMC Public Health. 2020;20(1):1464.
Shi T, Denouel A, Tietjen AK, Campbell I, Moran E, Li X, et al. Global disease burden estimates of respiratory syncytial virus-associated acute respiratory infection in older adults in 2015: a systematic review and meta-analysis. J Infect Dis. 2020;222(Supplement 7):S577–83.
Hammond A, Kim JJ, Sadler H, Vandemaele K. Influenza surveillance systems using traditional and alternative sources of data: a scoping review. Influenza Other Respir Viruses. 2022;16(6):965–74.
Brooks-Pollock E, Tilston N, Edmunds WJ, Eames KT. Using an online survey of healthcare-seeking behaviour to estimate the magnitude and severity of the 2009 H1N1v influenza epidemic in England. BMC Infect Dis. 2011;11:68.
Fragaszy EB, Warren-Gash C, Wang L, Copas A, Dukes O, Edmunds WJ, et al. Cohort profile: the flu watch study. Int J Epidemiol. 2017;46(2):e18.
Adler AJ, Eames KT, Funk S, Edmunds WJ. Incidence and risk factors for influenza-like-illness in the UK: online surveillance using Flusurvey. BMC Infect Dis. 2014;14(1):1–8.
Yang TU, Cheong HJ, Song JY, Lee JS, Wie S-H, Kim YK, et al. Age- and influenza activity-stratified case definitions of influenza-like illness: experience from hospital-based influenza surveillance in South Korea. PLoS One. 2014;9(1):e84873.
Casalegno JS, Eibach D, Valette M, Enouf V, Daviaud I, Behillil S, et al. Performance of influenza case definitions for influenza community surveillance: based on the French influenza surveillance network GROG, 2009–2014. Euro Surveill. 2017;22(14):30504.
Domínguez À, Soldevila N, Torner N, Martínez A, Godoy P, Rius C, et al. Usefulness of clinical definitions of influenza for public health surveillance purposes. Viruses. 2020;12(1):95.
Aguilera JF, Paget WJ, Mosnier A, Heijnen ML, Uphoff H, van der Velden J, et al. Heterogeneous case definitions used for the surveillance of influenza in Europe. Eur J Epidemiol. 2003;18(8):751–4.
Jiang L, Lee VJ, Lim WY, Chen MI, Chen Y, Tan L, et al. Performance of case definitions for influenza surveillance. Eurosurveillance. 2015;20(22):21145.
Davis W, Duque J, Huang QS, Olson N, Grant CC, Newbern EC, et al. Sensitivity and specificity of surveillance case definitions in detection of influenza and respiratory syncytial virus among hospitalized patients, New Zealand, 2012–2016. J Infect. 2022;84(2):216–26.
Souty C, Masse S, Valette M, Behillil S, Bonmarin I, Pino C, et al. Baseline characteristics and clinical symptoms related to respiratory viruses identified among patients presenting with influenza-like illness in primary care. Clin Microbiol Infect. 2019;25(9):1147–53.
Heinonen S, Peltola V, Silvennoinen H, Vahlberg T, Heikkinen T. Signs and symptoms predicting influenza in children: a matched case–control analysis of prospectively collected clinical data. Eur J Clin Microbiol Infect Dis. 2012;31(7):1569–74.
Kalimeri K, Delfino M, Cattuto C, Perrotta D, Colizza V, Guerrisi C, et al. Unsupervised extraction of epidemic syndromes from participatory influenza surveillance self-reported symptoms. PLoS Comput Biol. 2019;15(4):e1006173.
Ma X, Conrad T, Alchikh M, Reiche J, Schweiger B, Rath B. Can we distinguish respiratory viral infections based on clinical features? A prospective pediatric cohort compared to systematic literature review. Rev Med Virol. 2018;28(5):e1997.
Barry MA, Arinal F, Talla C, Hedible BG, Sarr FD, Ba IO, et al. Performance of case definitions and clinical predictors for influenza surveillance among patients followed in a rural cohort in Senegal. BMC Infect Dis. 2021;21(1):31.
Soldevila N, Toledo D, Martínez A, Godoy P, Torner N, Rius C, et al. Does knowing the influenza epidemic threshold has been reached influence the performance of influenza case definitions? PLoS One. 2022;17(7):e0270740.
Belongia EA, Simpson MD, King JP, Sundaram ME, Kelley NS, Osterholm MT, McLean HQ. Variable influenza vaccine effectiveness by subtype: a systematic review and meta-analysis of test-negative design studies. Lancet Infect Dis. 2016;16(8):942–51.
Vihta KD, Pouwels KB, Peto TEA, Pritchard E, Eyre DW, House T, et al. Symptoms and Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) positivity in the general population in the United Kingdom. Clin Infect Dis. 2022;75(1):e329–37.
Pouwels KB, House T, Pritchard E, Robotham JV, Birrell PJ, Gelman A, et al. Community prevalence of SARS-CoV-2 in England from April to November, 2020: results from the ONS coronavirus infection survey. Lancet Public Health. 2021;6(1):e30–8.
Office for National Statistics. Influenza and other respiratory viruses pilot study: Coronavirus (COVID-19) Infection Survey, UK. 2023. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandlifeexpectancies/articles/influenzaandotherrespiratoryvirusespilotstudycoronaviruscovid19infectionsurveyuk/october2022tofebruary2023.
Nuffield Department of Medicine. University of Oxford. Questionnaires. 2023. Available from: https://www.ndm.ox.ac.uk/covid-19/covid-19-infection-survey/case-record-forms.
Fitzner J, Qasmieh S, Mounts AW, Alexander B, Besselaar T, Briand S, et al. Revision of clinical case definitions: influenza-like illness and severe acute respiratory infection. Bull World Health Organ. 2018;96(2):122–8.
Commission E. Commission Implementing Decision (EU) 2018/945 of 22 June 2018 on the communicable diseases and related special health issues to be covered by epidemiological surveillance as well as relevant case definitions. OJEU. 2018;61:170.
Wood S. Package ‘mgcv’. 2023. Available from: https://cran.r-project.org/web/packages/mgcv/mgcv.pdf.
Wood SN. Thin plate regression splines. J R Stat Soc Ser B Stat Methodol. 2003;65(1):95–114.
Gelman A, Little T. Poststratification into many categories using hierarchical logistic regression. Surv Methodol. 1997;23(2):127–35.
Goldstein E, Dushoff J, Ma J, Plotkin JB, Earn DJ, Lipsitch M. Reconstructing influenza incidence by deconvolution of daily mortality time series. Proc Natl Acad Sci U S A. 2009;106(51):21825–9.
Goldstein E, Cowling BJ, Aiello AE, Takahashi S, King G, Lu Y, Lipsitch M. Estimating incidence curves of several infections using symptom surveillance data. PLoS One. 2011;6(8):e23380.
Camacho A, Eames K, Adler A, Funk S, Edmunds J. Estimation of the quality of life effect of seasonal influenza infection in the UK with the internet-based Flusurvey cohort: an observational cohort study. Lancet. 2013;382:S8.
Seran H, Jie Z, Jakob J, Anika S, Jack LB, Kieran JM, et al. Onset and window of SARS-CoV-2 infectiousness and temporal correlation with symptom onset: a prospective, longitudinal, community cohort study. Lancet Respir Med. 2022;10(11):1061–73.
Blake J. Personal communication. 2023.
Vos LM, Bruyndonckx R, Zuithoff NPA, Little P, Oosterheert JJ, Broekhuizen BDL, et al. Lower respiratory tract infection in the community: associations between viral aetiology and illness course. Clin Microbiol Infect. 2021;27(1):96–104.
Munywoki PK, Koech DC, Agoti CN, Kibirige N, Kipkoech J, Cane PA, et al. Influence of age, severity of infection, and co-infection on the duration of respiratory syncytial virus (RSV) shedding. Epidemiol Infect. 2015;143(4):804–12.
Fielding JE, Kelly HA, Mercer GN, Glass K. Systematic review of influenza A(H1N1)pdm09 virus shedding: duration is affected by severity, but not age. Influenza Other Respir Viruses. 2014;8(2):142–50.
Cane J, Street T, Sanderson N, Swann J, Vaughan A, Morgan M, et al. Nanopore whole genome sequencing of community and hospital influenza in the United Kingdom, 2022-2023. Poster session session presented at: ECCMID 2023. 33rd European Congress of Clinical Microbiology and Infectious Diseases (ECCMID); 2023 Apr 15-18; Copenhagen, Denmark.
UK Health Security Agency. Surviellance of influenza and other seasonal respiratory viruses in the UK, winter 2022 to 2023. 2023. https://www.gov.uk/government/statistics/annual-flu-reports/surveillance-of-influenza-and-other-seasonal-respiratory-viruses-in-the-uk-winter-2022-to-2023.
UK Health Security Agency. Weekly national Influenza and COVID-19 surveillance report: Week 5 report (up to week 4 data). 2023. https://www.gov.uk/government/statistics/national-flu-and-covid-19-surveillance-reports-2022-to-2023-season.
Guy R, Henderson KL, Coelho J, Hughes H, Mason EL, Gerver SM, et al. Increase in invasive group A streptococcal infection notifications, England, 2022. Euro Surveill. 2023;28(1):2200942.
Yang J, Huang P, Shie S, Yang S, Tsao K, Wu T, et al. Predictive symptoms and signs of laboratory-confirmed influenza: a prospective surveillance study of two metropolitan areas in Taiwan. Medicine (Baltimore). 2015;94(44):e1952.
Sáez-López E, Pechirra P, Costa I, Cristóvão P, Conde P, Machado A, et al. Performance of surveillance case definitions for respiratory syncytial virus infections through the sentinel influenza surveillance system, Portugal, 2010 to 2018. Euro Surveill. 2019;24(45):1900140.
Colosia A, Costello J, McQuarrie K, Kato K, Bertzos K. Systematic literature review of the signs and symptoms of respiratory syncytial virus. Influenza Other Respir Viruses. 2023;17(2):e13100.
Korsten K, Adriaenssens N, Coenen S, Butler CC, Verheij TJM, Bont LJ, Wildenbeest JG. World Health Organization influenza-like illness underestimates the burden of respiratory syncytial virus infection in community-dwelling older adults. J Infect Dis. 2022;226(Suppl 1):S71–8.
Rha B, Dahl RM, Moyes J, Binder AM, Tempia S, Walaza S, et al. Performance of surveillance case definitions in detecting respiratory syncytial virus infection among young children hospitalized with severe respiratory illness-South Africa, 2009–2014. J Pediatric Infect Dis Soc. 2019;8(4):325–33.
Subissi L, Bossuyt N, Reynders M, Gérard M, Dauby N, Bourgeois M, et al. Capturing respiratory syncytial virus season in Belgium using the influenza severe acute respiratory infection surveillance network, season 2018/19. Euro Surveill. 2020;25(39):1900627.
Office for National Statistics. Prevalence of symptoms and impact of respiratory infections, UK. 2023. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofsymptomsandimpactofrespiratoryinfectionsuk/10july2023.
Gimma A, Munday JD, Wong KLM, Coletti P, Zandvoort KV, Prem K, et al. Changes in social contacts in England during the COVID-19 pandemic between March 2020 and March 2021 as measured by the CoMix survey: A repeated cross-sectional study. PLOS Med. 2022;19(3):e1003907.
Bi Q, Dickerman BA, McLean HQ, Martin ET, Gaglani M, Wernli KJ, et al. Evaluating reduced effectiveness after repeat influenza vaccination while accounting for confounding by recent infection and within-season waning. medRxiv. 2023:2023.03.12.23287173.
The Francis Crick Institute. Vaccine composition 2022. Available from: https://www.crick.ac.uk/research/platforms-and-facilities/worldwide-influenza-centre/vaccine-composition.
UK Health Security Agency. Surveillance of influenza and other seasonal respiratory viruses in winter 2021 to 2022. 2023. https://www.gov.uk/government/statistics/annual-flu-reports/surveillance-of-influenza-and-other-seasonal-respiratory-viruses-in-winter-2021-to-2022.
Office for National Statistics. Coronavirus (COVID-19) infection survey: technical data. 2022. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/covid19infectionsurveytechnicaldata.
Office for National Statistics. Coronavirus (COVID-19) infection survey quality report. 2022. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/methodologies/coronaviruscovid19infectionsurveyqualityreportaugust20222022.
Office for National Statistics. Coronavirus (COVID-19) infection survey quality report. 2022. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/methodologies/coronaviruscovid19infectionsurveyqualityreportdecember20222022.
Office for National Statistics. Prevalence of ongoing symptoms following coronavirus (COVID-19) infection in the UK. 2022. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/1september2022#impact-of-moving-to-remote-data-collection2022.
Hay JA, Kissler SM, Fauver JR, Mack C, Tai CG, Samant RM, et al. Quantifying the impact of immune history and variant on SARS-CoV-2 viral kinetics and infection rebound: a retrospective cohort study. eLife. 2022;11:e81849. citation = eLife 2022;11 e.
Office for National Statistics. Coronavirus (COVID-19) infection survey: quality and methodology information (QMI). 2023. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/methodologies/coronaviruscovid19infectionsurveyqmi.
Acknowledgements
We wish to thank all the individuals who participated in the COVID-19 Infection Survey.
We are grateful for the support of all the COVID-19 Infection Survey team:
Office for National Statistics: Sir Ian Diamond, Emma Rourke, Ruth Studley, Nick Taylor, Tina Thomas, Fiona Dawe;
Office for National Statistics COVID Infection Survey Analysis and Operations teams in particular Dawid Pienaar, Joy Preece, Sarah Crofts, Lina Lloyd, Michelle Bowen, Daniel Ayoubkhani, Russell Black, Antonio Felton, Megan Crees, Joel Jones, Esther Sutherland;
University of Oxford, Nuffield Department of Medicine: Ann Sarah Walker, Derrick Crook, Philippa C Matthews, Tim Peto, Emma Pritchard, Nicole Stoesser, Karina-Doris Vihta, Jia Wei, Alison Howarth, Kevin K Chau, Lucas Martins Ferreira, Brian D Marsden, Wanwisa Dejnirattisai, Juthathip Mongkolsapaya, Sarah Hoosdally, Richard Cornall, David I Stuart, Gavin Screaton;
University of Oxford, Nuffield Department of Population Health: Koen Pouwels;
University of Oxford, Big Data Institute: David W Eyre, Katrina Lythgoe, David Bonsall, Tanya Golubchik, Helen Fryer;
University of Oxford, Radcliffe Department of Medicine: John Bell;
Oxford University Hospitals NHS Foundation Trust: Stuart Cox, Kevin Paddon, Tim James; University of Manchester: Thomas House;
UK Health Security Agency: Julie Robotham, Paul Birrell;
Office for Health Improvement and Disparities: John Newton,
IQVIA: Helena Jordan, Tim Sheppard, Graham Athey, Dan Moody, Leigh Curry, Pamela Brereton;
National Biocentre: Ian Jarvis, Anna Godsmark, George Morris, Bobby Mallick, Phil Eeles;
Glasgow Lighthouse Laboratory: Jodie Hay, Harper VanSteenhouse;
Berkshire and Surrey Pathology Services: Muhammad Ehsaan; Eric Haduli, Hugh Boothe, Reggie Samuel;
Welsh Government: Sean White, Tim Evans, Lisa Bloemberg;
Scottish Government: Katie Allison, Anouska Pandya, Sophie Davis;
Public Health Scotland: David I Conway, Margaret MacLeod, Chris Cunningham.
Funding
This study was funded by the Department of Health and Social Care and the UK Health Security Agency with in-kind support from the Welsh Government, the Department of Health on behalf of the Northern Ireland Government and the Scottish Government. ED, EP, K-DV, KBP, ASW, TEAP, NS, and DE are supported by the National Institute for Health Research Health Protection Research Unit (NIHR HPRU) in Healthcare Associated Infections and Antimicrobial Resistance at the University of Oxford in partnership with Public Health England (PHE) (NIHR200915). ASW and TEAP are also supported by the NIHR Oxford Biomedical Research Centre. KBP is also supported by the Huo Family Foundation. ASW is an NIHR Senior Investigator. PCM is funded by Wellcome (intermediate fellowship, grant ref 110110/Z/15/Z) and holds an NIHR Oxford BRC Senior Fellowship award. DWE is supported by a Robertson Fellowship and an NIHR Oxford BRC Senior Fellowship. NS is an Oxford Martin Fellow and an NIHR Oxford BRC Senior Fellow. JB is funded by the Bayes4Health grant. The views expressed are those of the authors and not necessarily those of the National Health Service, NIHR, Department of Health, or UKHSA. This work contains statistical data from ONS which is Crown Copyright. The use of the ONS statistical data in this work does not imply the endorsement of the ONS in relation to the interpretation or analysis of the statistical data. This work uses research datasets which may not exactly reproduce National Statistics aggregates. The funder/sponsor did not have any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. All authors had full access to all data analysis outputs (reports and tables) and took responsibility for their integrity and accuracy. For the purpose of Open Access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
Author information
Authors and Affiliations
Contributions
The COVID-19 Infection Survey was designed and planned by ASW, ID and KBP and was conducted by ASW, RS, NT, TEAP, PCM, NS, DWE, and the COVID-19 Infection Survey Team. Assays were conducted by ME, EH and HB at Berkshire and Surrey Pathology Services (BSPS). This specific analysis was originally designed by ASW and ED, but with ongoing input on methods and results from EP, KBP, JB, CG, KDV, TEAP, NS, PM, NT, ID, RS, ER, PB, DDA, TF, CW, DWE, and TH. ED conducted the statistical analysis of the survey data, with assistance from EP, KBP, JB and CG regarding code and analysis. ED and ASW drafted the manuscript and all authors contributed to interpretation of the data and results and revised the manuscript. All authors approved the final version of the manuscript.
Authors’ Twitter handles
Twitter handles: Modernising Medical Microbiology, NDM University of Oxford (@ModMedMicro)
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study received ethical approval from the South Central Berkshire B Research Ethics Committee (20/SC/0195). Following verbal agreement to participate, a study worker visited each selected household to take written informed consent for individuals aged 2 years and over. For those aged 2–15 years, consent was provided by their parents or carers; those aged 10–15 years also provided written assent.
Consent for publication
Not applicable.
Competing interests
DWE declares lecture fees from Gilead, outside the submitted work. PCM has received GSK funding support.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Methods. Table S1.
Infection duration distributions. Table S2. Differential influenza vaccination effects for Adults/Children. Figure S1. Distribution of Ct values. Figure S2. Fractions reporting ILI-ECDC and respiratory symptoms. Figure S3. Fractions reporting systemic symptoms. Figure S4. Fractions reporting loss of taste/smell and GI symptoms. Figure S5. Incidence by infection duration distribution. Figure S6. Prevalence of symptoms by SARS-CoV-2 test result. Figure S7. Prevalence of symptoms for RSV and influenza A/B positives. Figure S8. Probabilities of SARS-CoV-2 positivity by symptom. Figure S9. Probabilities of SARS-CoV-2, RSV or influenza A/B positivity by symptom. Figure S10. Probabilities of SARS-CoV-2, RSV or influenza A/B positivity with 95% Cis. Figure S11. Associations between selected variables and influenza A/B positivity. Figure S12. Association between age and influenza A/B positivity by vaccination category. Figure S13. Associations between selected variables and RSV positivity. Figure S14. Associations between selected variables and SARS-CoV-2 positivity. Figure S15. Raw percentages reporting ILI-WHO and SARS-CoV-2 test positivity. Figure S16. Cumulative numbers of ILI-WHO, SARS-CoV-2, RSV and Influenza A/B. Figure S17. Probabilities of SARS-CoV-2 positivity by symptom at different dates [52,53,54,55,56,57].
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Dietz, E., Pritchard, E., Pouwels, K. et al. SARS-CoV-2, influenza A/B and respiratory syncytial virus positivity and association with influenza-like illness and self-reported symptoms, over the 2022/23 winter season in the UK: a longitudinal surveillance cohort. BMC Med 22, 143 (2024). https://doi.org/10.1186/s12916-024-03351-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-024-03351-w