
Abstract
Background
Both genetic and pre- and perinatal factors, including birth weight, have been implicated in the onset of attention deficit hyperactivity disorder (ADHD) traits among children. This study aimed to elucidate to what extent the genetic risk of ADHD moderates the association between birth weight and ADHD traits among Japanese children.
Methods
We conducted a longitudinal birth cohort study (Hamamatsu Birth Cohort for Mother and Children Study) to investigate the association of genetic risk for ADHD and low birth weight with ADHD traits among Japanese children. Out of 1258 children, we included 796 who completed follow-ups at 8 to 9 years of age. Birth weight was categorized as <2000 g, 2000–2499 g, and ≥2500 g. Polygenic risk score for ADHD was generated using the summary data of a large-scale genome-wide association study. The Rating Scale IV (ADHD-RS) assessed ADHD traits (inattention and hyperactivity/impulsivity) based on parental reports. Following previous studies, sex, birth order of the child, gestational age at birth, mother’s age at delivery, educational attainment, pre-pregnancy body mass index, pre-pregnancy or during pregnancy smoking status, alcohol consumption during pregnancy, father’s age, education, and annual family income were considered as covariates. Multivariable negative binomial regression was applied to evaluate the association between birth weight and ADHD traits, while adjusting for potential covariates. The interaction term between birth weight categories and binary polygenic risk was added to the model.
Results
Birth weight of 2000–2499 g was not associated with ADHD traits. Birth weight under 2000 g was significantly associated with both inattention and hyperactivity. When accounting for higher and lower genetic risk for ADHD, only those with higher genetic risk and birth weight < 2000 g were associated with inattention (rate ratio [RR] 1.56, 95% CI 1.07–2.27) and hyperactivity (RR 1.87, 95% CI 1.14–3.06).
Conclusions
Birth weight under 2000 g, together with the genetic risk of ADHD, contributes to higher levels of ADHD traits among Japanese children aged 8 to 9 years. The suggested association between low birth weight and ADHD is confined to children with a genetic susceptibility to ADHD, indicating the relevance of genetic-environmental interactions in the etiology.
Similar content being viewed by others


Key points
-
Questions: Does genetic risk moderate the association between birth weight and ADHD traits among Japanese children?
-
Findings: Children with birth weight under 2000 g and higher genetic risk of ADHD showed increased severity of ADHD traits at age 8 to 9 years, compared to those with either normal birth weight or lower genetic risk.
-
Meaning: Japanese children born with birth weight less than 2000 g are more vulnerable to their genetic susceptibility to ADHD. Additional attention is needed to minimize the severity of ADHD traits during childhood.
Background
Attention deficit hyperactivity disorder (ADHD) is one of the most prevalent neurodevelopmental disorders [1, 2], accounting for 1.14 million disability-adjusted life years globally in 2017 [3]. ADHD can be classified as predominantly inattentive, predominantly hyperactive/impulsive, or a combination of both and usually appears during early childhood and continues to manifest throughout the life course [1, 4]. ADHD affects functioning, both in school and daily activities [5], and increases the social and economic burden [6, 7]. In addition, children with ADHD symptoms are often bullied, neglected, and ignored by their peers and others in society due to their inattentive and restless behavioral phenotypes [8]. Although the etiology of ADHD is complex and multifactorial, both pre- and perinatal conditions and genetic risk factors have been implicated in the development of ADHD symptoms among children [9,10,11]. Specifically, low birth weight [12] is the most consistent environmental factor identified in the literature to affect neurodevelopment and the onset of ADHD in childhood [13].
Accumulating evidence suggests that low birth weight is an early biomarker for newborn infants’ vulnerability to experiencing altered neurodevelopment and developmental disorders [14, 15]. A recent meta-analysis reported that children born with very low birth weight have a higher risk of developing ADHD during childhood [14]. Although several previous studies have investigated the association between birth weight and ADHD traits, the results remain inconclusive [16,17,18,19,20,21,22,23,24]. For instance, some studies found a negative relationship between birth weight and ADHD symptoms [17,18,19, 22, 23], while others failed to confirm the association [25, 26]. Moreover, the majority of previous studies have explored the link between ADHD and the extremely low end of the birth weight distribution [14, 27], that is, either very low birth weight (≤1500 g) or extremely low birth weight (≤1000 g), or a low birth weight classified as under 2500 g [18, 21]. A birth weight of 2500 g is the standard cutoff set by the World Health Organization (WHO) to define low birth weight and is generally considered to indicate high-risk newborns. However, the cut-off point for low birth weight remains controversial. Given that Asian children are generally lighter than their Western counterparts [28], the limit of 2500 g is inadequate for defining low birth weight. Recently, a multi-national study suggested a birth weight of around 2000 g as the threshold for defining low birth weight among Asians [29]. Notably, the mean birth weight in Japan has declined significantly in the last three decades (1980–2010) [30]. Thus, the prevalence of low birth weight, particularly birth weights between 1500 to 2499 g, has increased significantly [30]. Therefore, it is of paramount importance to investigate whether intermediate birth weight categories, such as 1500 to 1999g and 2000 to 2499g, are associated with ADHD symptoms among Japanese children.
Besides the birth weight implications for ADHD, it is well known that ADHD is heritable (70–80%) [31, 32]. A previous meta-analysis found significant associations between ADHD and eight candidate variants connected with six genes [33, 34]. In addition, a recent genome-wide association study (GWAS) identified 304 genetic variants in 12 loci that were associated with ADHD [35]. Furthermore, several studies found a significant association between genetic risk, specifically polygenic risk scores (PRS), and ADHD traits [36,37,38].
The influence of some individual candidate genes and several prenatal factors on ADHD traits is known to some extent. While previous studies have highlighted the importance of gene-environmental interactions in the etiology of ADHD [39, 40], the evidence of this relationship remains limited [40,41,42]. Thus, the interactions of genetic liability, measured using PRS, with prenatal factors such as birth weight could elucidate the etiology of ADHD [43]. Understanding the mechanistic pathway between genetic risks and non-genetic risks, such as low birth weight, adjusted for lighter Asian infants, may help identify children at greater risk for ADHD diagnosis later in childhood. This may subsequently reduce the long-term sequelae associated with elevated ADHD traits through timely implementation of behavioral and pharmacological interventions [44]. However, studies on the interactions between birth weight and the genetic risk of ADHD on the symptoms of ADHD in childhood are limited. Therefore, this study aimed to investigate the association of low birth weight and genetic risk for ADHD with the presence of ADHD traits in children. We used a longitudinal birth cohort of the general population in Japan. We hypothesized that a higher polygenic risk of ADHD, together with a lower birth weight, would be associated with higher severity of ADHD traits among Japanese children aged 8 to 9 years.
Methods
Study cohort
This study used data from the Hamamatsu Birth Cohort for Mother and Child (HBC) Study, which is an ongoing prospective birth cohort study designed to investigate the neurodevelopmental trajectories of children in the general population. The children in the cohort were born in Hamamatsu City, Japan, between November 2007 and March 2011. The details of the HBC study are presented elsewhere [45]. In the HBC study, out of 1258 children, 826 were successfully followed up until 8 to 9 years. We excluded twins (n=28) and children with Down syndrome (n=2) from this study. Ultimately, 796 children and their mothers were included in this study.
Exposures
Birth weight categories
Birth weight below 1500 g and 2500 g are recognized as very low birth weight and low birth weight, respectively. However, in this study, we had only three children (out of 796) whose birth weight was below 1500 g. Moreover, a recent multi-national study has highlighted the need for redefining low birth weight with a threshold of birth weight of around 2000 g among Asian children [29]. Thus, we classified birth weight into three categories: normal birth weight (≥2500 g), intermediate birth weight (2000–2499 g), and birth weight <2000 g.
Polygenic risk score for ADHD
The genetic risk for ADHD in the HBC study was assessed using PRS. PRS represents the approximate genetic liability for a disease or disorder using the number of risk alleles from a set of single-nucleotide polymorphisms (SNPs) [46]. The detailed estimation procedure of the PRS and quality controls of SNPs in the HBC study were described in our previous study [47]. Trained clinicians collected buccal swabs (DNA samples) from children during the follow-up surveys conducted either at age 32 months, 40 months, 4.5 years, or 6 years. In this study, out of 796 children, a total of 137 children were excluded from the PRS analysis because genomic DNA was unavailable due to a low call rate (<97%) or a refusal or reluctance of buccal swab collection. A Japonica array was used for SNP genotyping [48] and BEAGLE 5.0 of phase 3 of the 1000 genome project was used as the reference panel for Japanese populations in the genotyping imputation [49]. Next, the PRS was generated in PRSice-2 software using a previous GWAS study for ADHD, conducted by the Lundbeck Foundation Initiative for Integrative Psychiatric Research, as the discovery cohort [50]. Although the ADHD-PRS was estimated at several p-value thresholds, we considered the best fit PRS for this study. The ADHD-PRS for the included 659 samples had a bell-shaped distribution with a mean of 0.00124 and median of 0.00123 (Supplementary Figure 1). The score in the middle of the distribution (a PRS value of 0) corresponds to the average risk for developing ADHD. The score on the right tail of the distribution indicates a relatively higher genetic risk of ADHD than the average, and the left tail represents a lower risk. When investigated the distribution of genetic risk across children with different birth weight categories, we observed that children were almost equally distributed to higher or lower genetic risk group in each birth weight category (see Additional file 1: Figure S1).
Outcome: ADHD traits
The main outcomes were the behavioral traits of ADHD, which comprise inattention and hyperactivity domains. To quantify these domains, we used the ADHD Rating Scale IV (ADHD-RS) based on parental reports to assess the severity of ADHD traits at ages 8 to 9 years. The ADHD-RS comprises 18 items covering the spectrum of the inattention (9 items) and hyperactivity/impulsivity domains (9 items) [51]. Responses are rated on a 4-point Likert scale ranging from 0 (“never” or “rarely”) to 3 (“very often”) [51].
Covariates
Following previous studies [52, 53], the sex, birth order of the child, gestational age at birth, mother’s age at delivery, educational attainment, pre-pregnancy body mass index (BMI), pre-pregnancy or during pregnancy smoking status, alcohol consumption during pregnancy, father’s age at birth, education, and annual family income (at birth) were considered as confounders and were included in the model.
Statistical analysis
Frequency distribution and univariate statistics were used to describe the characteristics of children and their mothers. The data were not normally distributed as indicated by a Shapiro-Wilk test (p<0.001 for all three outcomes related to ADHD-RS total, inattention, and hyperactivity scores). Therefore, negative binomial regression models were employed to investigate the association between the exposure and outcome variables. The choice of negative binomial models was determined by considering overdispersion that was present for both the Poisson and zero-inflated Poisson models. The negative binomial regression model provided rate ratios (RR) along with 95% confidence intervals (CIs), which indicates the number of times that the ADHD score is higher (when RR>1) or lower (RR<1) than the reference group. In the case of continuous exposure, an RR value higher than 1 indicates a higher severity associated with a one-unit increase in the exposure, and vice versa. Model 1 was adjusted for variations in survey time only. Model 2 was additionally adjusted for gender, birth order of the child, maternal age at delivery, education, pre-pregnancy BMI, smoking status, and alcohol intake to control for maternal and infant-related factors. Model 3 was further adjusted to include the father’s age at birth, education, and annual family income to control for paternal factors. We found significant interaction effects between birth weight categories and ADHD-PRS. To facilitate interpretation, we classified the PRS into a binary variable using the median value as the threshold. Therefore, any PRS above the median was defined as “having higher genetic risk than average” and PRS values below the median were considered as “having lower genetic risk than average”. We also considered the interaction of birth weight categories and binary polygenic risk variable in the model to estimate the RR for each combination of birth weight category and binary polygenic risk variable. Clustering was allowed for with the Huber-White sandwich estimator in all the included models, as some children included in this study were born to the same mother. Furthermore, background characteristics of children included in the analysis and those excluded from the analysis were compared. The Little’s test for Missing Completely at random (MCAR) was used to test whether missingness of ADHD trait scores and ADHD-PRS were completely at random [54], while an extension of the Little’s MCAR test, with several combinations of auxiliary variables as covariates into the test, was employed to test the covariate-dependent missingness [55]. Then we performed multiple imputation of ADHD-PRS for children with missing information, assuming missing completely at random, to evaluate the potential impact of missing observations (17.2%) on the association between birth weight and ADHD traits. In addition, we performed sensitivity analyses by considering missing ADHD-PRS to the end of the spectrum, i.e., recoding all missing ADHD-PRS as high risk or low risk. Statistical analyses were performed using Stata MP version 16.1.
Results
Characteristics of participants
Table 1 shows the demographic characteristics of the study participants. A total of 796 children (49.2% females; 50.8% males) aged 8 to 9 years were included in this study. Among them, 6.4% were born preterm (before the gestational age of 37 weeks). The mean (±SD) birth weight and gestational age at birth were 2949.3 g (440.1) and 38.9 weeks (1.52), respectively. Additionally, 87.3% of children had a normal birth weight, 10.3% had a birth weight between 2000 to 2499 g, and 2.4% had a birth weight under 2000 g. The median scores for ADHD combined traits, as well as inattention and hyperactivity traits, were significantly higher among children who had a birth weight < 2000 g (see Additional file 2: Table S1). These scores were lowest among children with birth weights between 2000 and 2499 g (see Additional files 3 and 4: Figures S2-S3).
Independent effects of birth weight and ADHD
In the negative binomial models, birth weight, when considered as continuous, was not significantly associated with ADHD scores (see Additional files 5: Table S2). However, when birth weight was considered as categorical, we found that birth weight < 2000 g was significantly associated with higher ADHD trait scores (RR 1.60, 95% CI 1.16–2.22) (Table 2). Similar findings were observed for both inattention and hyperactivity domains. Birth weight < 2000 g was significantly associated with higher scores of both inattention (RR 1.50, 95% CI 1.10–2.06) and hyperactivity traits (RR 1.82, 95% CI 1.17–2.83) compared to normal birth weight (≥2500 g) (model 1). After adjusting for potential covariates in model 3, the results remained statistically significant for both inattention (RR 1.49, 95% CI 1.15–1.94) and hyperactivity traits (RR 1.78, 95% CI 1.19–2.67).
Interaction of genetic risk of ADHD and birth weight on ADHD traits
We found a significant interaction effect of birth weight categories and ADHD-PRS on ADHD scores (Wald chi-squared test, p<0.05 for ADHD total score) (see Additional files 6: Table S3). This provided evidence of the moderating effects of genetic risk on the association between birth weight and ADHD traits. Thus, we included the interaction of birth weight categories and binary polygenic risk variables in the model.
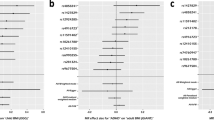
Higher genetic risk of ADHD and birth weight < 2000 g were associated with higher severity of ADHD traits (RR 1.82, 95% CI 1.10–3.01) compared to those born with normal birth weight or had lower genetic risk (Table 3). Similar findings were observed for both inattention and hyperactivity traits (Table 4 and Fig. 1).

Multivariable-adjusted rate ratios (RR) and 95% confidence intervals (CI) for the association of birth weight categories and genetic risk with inattention and hyperactivity scores among Japanese children at age 8–9 years. Note: Normal birth weight was defined as birth weight ≥ 2500 g and considered as the reference category. Models were adjusted for gender of child, parity, maternal age, education, pre-pregnancy body mass index, pre-pregnancy smoking status, alcohol intake, variations in survey time, father’s age at birth and household annual income
In model 1, birth weight under 2000 g and higher genetic risk of ADHD were significantly associated with higher scores of inattention (RR 1.70, 95% CI 1.02–2.83) and hyperactivity (RR 2.10, 95% CI 1.10–3.98). These results remain statistically significant after additionally adjusting for potential confounders in model 3. The corresponding RRs were 1.56 (95% CI 1.07–2.27) for inattention traits and 1.87 (95% CI 1.14–3.06) for hyperactivity traits (Table 4).
Attrition
We compared background characteristics of children included in the analysis and those excluded due to missing information on ADHD trait scores and ADHD-PRS. The proportion of missing ADHD trait scores or ADHD-PRS was slightly higher among children of younger mother, less educated, and smoker mother (see Additional files 7: Table S4). However, the Little’s test confirmed that missingness of ADHD trait scores and ADHD-PRS were completely at random as well as missingness was not covariate-dependent (see Additional files 8: Table S5). We performed multiple imputation of ADHD-PRS for children with missing information on ADHD-PRS and the results remained virtually the same (N=796) (see Additional files 9 and 10: Tables S6-S7). The effect sizes remain almost same and significant in the sensitivity analyses where we considered all missing PRS as high risk or low risk (see Additional files 11 and 12: Tables S8-S9).
Discussion
Using a prospective birth cohort study, we found that birth weight under 2000 g was significantly associated with an increased likelihood of having higher ADHD trait scores among Japanese children aged 8 to 9 years. Furthermore, such increased risks were confined but significant for children with relatively higher polygenic risk of ADHD and birth weight under 2000 g. This confirms our hypothesis that reduced birth weight (<2000 g), together with higher genetic susceptibility for ADHD, are associated with an elevated risk of developing ADHD traits during childhood. To our knowledge, this is the first epidemiological study to evaluate the joint contribution of birth weight and polygenic risk of ADHD on the domains of inattention and hyperactivity/impulsivity.
Consistent with previous studies [14, 56,57,58], we found that children with birth weight < 2000 g had approximately 50% higher ADHD trait scores than those born with normal birth weight. This finding is also consistent with previous studies conducted among participants who were clinically diagnosed with ADHD [21, 52, 59]. The effect size for the association remained materially unchanged even after adjusting for parental factors and other potential confounders, suggesting an independent association between birth weight and ADHD traits. Notably, most previous studies considered 1000 g, 1500 g, or 2500 g as the threshold for extremely low, very low, or low birth weight categories, respectively. However, our study focused on intermediate low birth weight categories (i.e., <2000 g; 2000 to 2499 g) and observed a higher risk of ADHD traits for birth weight under 2000 g. This highlights the need for adopting lower cut-off points to define low birth weight regarding ADHD risk. This finding is congruent with previous studies that hypothesized that low birth weight, as an early life adversity (e.g., impaired nourishment in utero), is associated with neurodevelopmental difficulties [60]. Although birth weight < 1500 g is classified as very low in clinical practice, there were only three children in this category in our study. Therefore, we could not evaluate the association between very low birth weight and ADHD traits. Nevertheless, our findings on the higher severity of ADHD traits and birth weight under 2000 g have clinical importance. This is because the percentages of children born with birth weight between 1500 and 1999 g or 2000 and 2499 g are much larger than children born with extremely low or very low birth weight, particularly in Japan [30]. Thus, our study expands on previous research by evaluating the risk estimates for different categories of birth weight, and by adjusting for a wide range of potential covariates. In addition, this study provides evidence of the independent association between low birth weight and ADHD traits among children. It further emphasizes that the neurodevelopmental progress of children with low birth weight under 2000 g should be monitored closely, as these children are at heightened risk of developing ADHD traits in early childhood. Regarding the two domains of ADHD, we found that children whose birth weight was less than 2000 g had 1.49 times higher scores of inattention traits and 1.78 times higher hyperactivity scores. This is consistent with a previous study conducted among British and Brazilian children that observed higher risks of attention difficulties for birth weights under 2500 g [61]. Furthermore, although we found no significant difference between the RRs of inattention and hyperactivity scores for children with birth weights under 2000 g, we found that the risk of hyperactivity was slightly higher than that of inattention (RR 1.78 vs. 1.49). To date, no study has considered the direct comparison of the effect size for hyperactivity traits. Therefore, further studies are necessary to confirm this finding.
By including an interaction term of polygenic risk and birth weight categories to the multivariable models, the risk-conferring effect of low birth weight under 2000 g was found in children with higher genetic risk of ADHD, but not in children of lower genetic risk. This effect highlights that genetic risk could moderate the association between birth weight and ADHD traits. These results were anticipated, as a previous GWAS conducted among English children aged 7 years found a positive association between PRS and inattentive traits, hyperactive/impulsive traits, and overall ADHD traits [36]. In addition, another study conducted among Dutch children found a significant association between ADHD-PRS and clinical ADHD [37]. Unfortunately, we could not compare these effect sizes with previous research, as none of the prior studies evaluated the joint effect of low birth weight and genetic vulnerability on ADHD traits.
Notably, the risk was confined to those born under 2000 g in our Japanese sample, while previous studies from the USA indicated that the risk was observed among children born under 2500 g [62]. This contrast may indicate the relevance of racial differences in maternal and child body weight to the study variables. However, since we adjusted for maternal BMI, and the limited sample size did not allow us to calibrate the effect of small differences in birth weight, future studies with larger sample sizes are warranted to address this as a global public health issue.
Biological mechanisms
The precise biological mechanisms underlying the association between birth weight and ADHD traits remain uncertain; however, several hypotheses have been proposed by previous studies. It may be attributed to the inadequate supply of oxygen and necessary nutrient transport from the mother’s blood to the fetus, known as prenatal ischemia-hypoxia (PIH), which restricts fetal growth and alters placental development, causing low birth weight [63]. PIH causes several functional problems and neuropsychiatric disorders, including the symptoms of ADHD, through altered brain development of the fetus and increased susceptibility to neurodevelopmental problems [63, 64]. In addition, the immune system increases the release of circulating pro-inflammatory cytokines in response to PIH, resulting in systemic inflammation, which further leads to impaired neurodevelopment [65]. Another possibility is the role of hypothalamic-pituitary-adrenal (HPA) axis dysregulation, which is the main component of the stress response and regulation system. This is common among infants born prematurely or born with low birth weight due to the insufficient supply of nutrients to the fetus [66]. It has been suggested that the disturbances of the HPA axis and resulting fetal exposure to excess glucocorticoid levels may influence developmental pathways, leading to impaired brain development, behavioral impairments, and psychiatric disorders, including ADHD [67, 68]. Further experimental studies are needed to confirm the causal relationships between low birth weight and ADHD traits.
The underlying factors of the interaction of genetic risk for ADHD and low birth weight on ADHD traits remains unclear. Therefore, few hypotheses have been suggested to explain this interaction. The complex blend of numerous common genetic variants, such as dopaminergic, noradrenergic, and serotoninergic genes, and rare genetic variants are likely to be implicated in the pathophysiology of ADHD [33, 69, 70]. Higher genetic susceptibility to ADHD may moderate the association between reduced birth weight and ADHD through impaired inflammatory response [65] and/or dysfunctions of the HPA axis. Specifically, variations in cytokine genes (IL16 and S100B) may moderate the association between birth weight and the severity of ADHD symptoms [71]. In addition, polymorphism in the glucocorticoid receptor gene (NR3C1) moderates the relationship between stress responses and the severity of ADHD symptoms [66, 72]. This may partially explain the elevated risk of ADHD among children with higher genetic risk for ADHD and reduced birth weight. Previous studies also revealed that the complex interaction of reduced birth weight with both common and rare genetic variants associated with ADHD further leads to several neurobiological changes such as dysfunctions in the brain’s default network, cognitive control systems, and the amygdala-frontal or reward circuit [69]. Such neurobiological changes can be further implicated in several neuropsychological impairments, including among individuals with ADHD symptoms [69].
Limitations and strengths
Our study had several limitations. First, our study had a relatively small sample size, particularly due to the exclusion of participants without genomic DNA collection. The generalizability of the finding is limited to this population until it can be replicated. However, the participants included in the HBC study comprised a representative sample of the Japanese population. Second, our study lacked diagnostic assessment of ADHD. The ADHD traits were measured based on parental reports on their children using ADHD-RS, which may be subject to social desirability bias. However, the ADHD-RS is a widely used, valid, and reliable scale to assess the severity of ADHD symptoms [73]. Third, participants with ADHD-PRS values higher than the median were considered to have a higher genetic risk for ADHD, since PRS has been standardized in our studied sample. Thus, caution should be taken when generalizing these results, as higher genetic risk in this study indicates a higher risk than the average population. Finally, this study was conducted among Japanese children; thus, the findings may not be generalized to other races or ethnic groups as the genetic background is quite variable.
Despite these limitations, our study has several strengths. The major strengths of this study include the prospective design (birth cohort), lower attrition rate, and representativeness of the sample, making the results of this study applicable to the general Japanese populations. Moreover, this is the first study to investigate the association between birth weight and ADHD traits in childhood while accounting for the genetic risks of developing ADHD. As neurodevelopmental disorders are genetically complex to understand, the inclusion of a single gene marker in the model may not be useful. Since the PRS elucidates the genetic risk through the prediction of complex genetic phenotypes, we accounted for both common and rare genetic risk variants of each participant through the inclusion of PRS in this study [74].
Clinical implications
Taken together, our findings highlight the importance of vigilant monitoring of children born with birth weight < 2000 g, especially for those with genetic susceptibility to ADHD. Our findings have several clinical implications. First, it would help clinicians, based on birth weight information, to decide whether a child is at a greater biological risk of developing ADHD symptoms later on. Subsequently, the genetic risk for ADHD should be assessed for children with reduced birth weight to identify whether their biological risk may be exacerbated by their higher genetic loading for clinical ADHD. Such information would also support clinicians in the early detection of other co-occurring neuropsychiatric diseases, including autism spectrum disorder [37], anxiety [75], and depression [75, 76].
Conclusions
In conclusion, birth weight < 2000 g is significantly associated with an increase in the severity of inattention, hyperactivity, and combined ADHD traits among Japanese children aged 8 to 9 years. The presence of higher genetic risk for ADHD among children with reduced birth weight further elevates such risk. The introduction of effective interventions aimed at reducing the incidence of low birth weight, especially among children whose parents have known ADHD symptoms and diagnoses, may play a crucial role in reducing the risk of developing ADHD.
Availability of data and materials
Data are not publicly available but can be used for onsite analysis on a reasonable request to the corresponding author (Prof. Kenji J. Tsuchiya).
Abbreviations
- ADHD:
-
Attention deficit hyperactivity disorder
- CI:
-
Confidence interval
- GWAS:
-
Genome-wide association study
- HBC:
-
Hamamatsu Birth Cohort for Mother and Child
- HPA:
-
Hypothalamic-pituitary-adrenal
- PIH:
-
Prenatal ischemia-hypoxia
- PRS:
-
Polygenic risk scores
- RR:
-
Rate ratio
- SNPs:
-
Single-nucleotide polymorphisms
- WHO:
-
World Health Organization
References
American Psychiatric Association. DSM-5: Diagnostic and statistical manual of mental disorders. Arlington: American Psychiatric Publishing; 2013.
Polanczyk G, De Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–8. https://doi.org/10.1176/ajp.2007.164.6.942.
Institute for Health Metrics and Evaluation (IHME). GBD Compare. Seattle: IHME, University of Washington; 2021. http://vizhub.healthdata.org/gbd-compare. Accessed January 12, 2021
Barbaresi WJ, Colligan RC, Weaver AL, Voigt RG, Killian JM, Katusic SK. Mortality, ADHD, and psychosocial adversity in adults with childhood ADHD: a prospective study. Pediatrics. 2013;131(4):637–44. https://doi.org/10.1542/peds.2012-2354.
Harpin VA. The effect of ADHD on the life of an individual, their family, and community from preschool to adult life. Arch Dis Child. 2005;90(suppl 1):i2–7. https://doi.org/10.1136/adc.2004.059006.
Gupte-Singh K, Singh RR, Lawson KA. Economic burden of attention-deficit/hyperactivity disorder among pediatric patients in the United States. Value Health. 2017;20(4):602–9. https://doi.org/10.1016/j.jval.2017.01.007.
Quintero J, Ramos-Quiroga JA, San Sebastián J, Montañés F, Fernández-Jaén A, Martínez-Raga J, et al. Health care and societal costs of the management of children and adolescents with attention-deficit/hyperactivity disorder in Spain: a descriptive analysis. BMC Psychiatry. 2018;18(1):40. https://doi.org/10.1186/s12888-017-1581-y.
Hadianfard H. Child abuse in group of children with attention deficit-hyperactivity disorder in comparison with normal children. Int J Community Based Nurs Midwifery. 2014;2(2):77–84.
Larsson J-O, Larsson H, Lichtenstein P. Genetic and environmental contributions to stability and change of ADHD symptoms between 8 and 13 years of age: a longitudinal twin study. J Am Acad Child Adolesc Psychiatry. 2004;43(10):1267–75. https://doi.org/10.1097/01.chi.0000135622.05219.bf.
Froehlich TE, Anixt JS, Loe IM, Chirdkiatgumchai V, Kuan L, Gilman RC. Update on environmental risk factors for attention-deficit/hyperactivity disorder. Curr Psychiatry Rep. 2011;13(5):333–44. https://doi.org/10.1007/s11920-011-0221-3.
Burt SA. Rethinking environmental contributions to child and adolescent psychopathology: a meta-analysis of shared environmental influences. Psychol Bull. 2009;135(4):608–37. https://doi.org/10.1037/a0015702.
Hatch B, Healey DM, Halperin JM. Associations between birth weight and attention-deficit/hyperactivity disorder symptom severity: indirect effects via primary neuropsychological functions. J Child Psychol Psychiatry. 2014;55(4):384–92. https://doi.org/10.1111/jcpp.12168.
Kim JH, Kim JY, Lee J, Jeong GH, Lee E, Lee S, et al. Environmental risk factors, protective factors, and peripheral biomarkers for ADHD: an umbrella review. Lancet Psychiatry. 2020;7(11):955–70. https://doi.org/10.1016/S2215-0366(20)30312-6.
Franz AP, Bolat GU, Bolat H, Matijasevich A, Santos IS, Silveira RC, et al. Attention-deficit/hyperactivity disorder and very preterm/very low birth weight: a meta-analysis. Pediatrics. 2018;141(1):e20171645. https://doi.org/10.1542/peds.2017-1645.
Upadhyay RP, Naik G, Choudhary TS, Chowdhury R, Taneja S, Bhandari N, et al. Cognitive and motor outcomes in children born low birth weight: a systematic review and meta-analysis of studies from South Asia. BMC Pediatr. 2019;19(1):35. https://doi.org/10.1186/s12887-019-1408-8.
Kelly YJ, Nazroo JY, McMunn A, Boreham R, Marmot M. Birthweight and behavioural problems in children: a modifiable effect? Int J Epidemiol. 2001;30(1):88–94. https://doi.org/10.1093/ije/30.1.88.
Møllegaard S. The effect of birth weight on behavioral problems in early adolescence: new evidence from monozygotic twins. Econ Hum Biol. 2020;36:100828. https://doi.org/10.1016/j.ehb.2019.100828.
Gupta ND, Deding M, Lausten M. The effect of low birth weight on height, weight and behavioral outcomes in the medium-run. Econ Hum Biol. 2013;11(1):42–55. https://doi.org/10.1016/j.ehb.2011.06.002.
Pettersson E, Larsson H, D’Onofrio B, Almqvist C, Lichtenstein P. Association of fetal growth with general and specific mental health conditions. JAMA Psychiatry. 2019;76(5):536–43. https://doi.org/10.1001/jamapsychiatry.2018.4342.
McCormick MC, Gortmaker SL, Sobol AM. Very low birth weight children: behavior problems and school difficulty in a national sample. J Pediatr. 1990;117(5):687–93. https://doi.org/10.1016/S0022-3476(05)83322-0.
Mick E, Biederman J, Prince J, Fischer MJ, Faraone SV. Impact of low birth weight on attention-deficit hyperactivity disorder. J Dev Behav Pediatr. 2002;23(1):16–22. https://doi.org/10.1097/00004703-200202000-00004.
Halmøy A, Klungsøyr K, Skjærven R, Haavik J. Pre-and perinatal risk factors in adults with attention-deficit/hyperactivity disorder. Biol Psychiatry. 2012;71(5):474–81. https://doi.org/10.1016/j.biopsych.2011.11.013.
Pettersson E, Sjölander A, Almqvist C, Anckarsäter H, D'Onofrio BM, Lichtenstein P, et al. Birth weight as an independent predictor of ADHD symptoms: a within-twin pair analysis. J Child Psychol Psychiatry. 2015;56(4):453–9. https://doi.org/10.1111/jcpp.12299.
van Mil NH, Steegers-Theunissen RP, Motazedi E, Jansen PW, Jaddoe VW, Steegers EA, et al. Low and high birth weight and the risk of child attention problems. J Pediatr. 2015;166(4):862–9. e3.
Lahti J, Räikkönen K, Kajantie E, Heinonen K, Pesonen AK, Järvenpää AL, et al. Small body size at birth and behavioural symptoms of ADHD in children aged five to six years. J Child Psychol Psychiatry. 2006;47(11):1167–74. https://doi.org/10.1111/j.1469-7610.2006.01661.x.
Huhdanpää H, Morales-Muñoz I, Aronen ET, Pölkki P, Saarenpää-Heikkilä O, Kylliäinen A, et al. Prenatal and postnatal predictive factors for children’s inattentive and hyperactive symptoms at 5 years of age: the role of early family-related factors. Child Psychiatry Hum Dev. 2020:1–17.
Aarnoudse-Moens CSH, Weisglas-Kuperus N, van Goudoever JB, Oosterlaan J. Meta-analysis of neurobehavioral outcomes in very preterm and/or very low birth weight children. Pediatrics. 2009;124(2):717–28. https://doi.org/10.1542/peds.2008-2816.
Wang X, Guyer B, Paige DM. Differences in gestational age-specific birthweight among Chinese, Japanese and white Americans. Int J Epidemiol. 1994;23(1):119–28. https://doi.org/10.1093/ije/23.1.119.
Laopaiboon M, Lumbiganon P, Rattanakanokchai S, Chaiwong W, Souza JP, Vogel JP, et al. An outcome-based definition of low birthweight for births in low-and middle-income countries: a secondary analysis of the WHO global survey on maternal and perinatal health. BMC Pediatr. 2019;19(1):166. https://doi.org/10.1186/s12887-019-1546-z.
Takemoto Y, Ota E, Yoneoka D, Mori R, Takeda S. Japanese secular trends in birthweight and the prevalence of low birthweight infants during the last three decades: a population-based study. Sci Rep. 2016;6(1):1–6.
Nikolas MA, Burt SA. Genetic and environmental influences on ADHD symptom dimensions of inattention and hyperactivity: a meta-analysis. J Abnorm Psychol. 2010;119(1):1–17. https://doi.org/10.1037/a0018010.
Brikell I, Kuja-Halkola R, Larsson H. Heritability of attention-deficit hyperactivity disorder in adults. Am J Med Genet B Neuropsychiatr Genet. 2015;168(6):406–13. https://doi.org/10.1002/ajmg.b.32335.
Gizer IR, Ficks C, Waldman ID. Candidate gene studies of ADHD: a meta-analytic review. Hum Genet. 2009;126(1):51–90. https://doi.org/10.1007/s00439-009-0694-x.
Faraone SV, Larsson H. Genetics of attention deficit hyperactivity disorder. Mol Psychiatry. 2019;24(4):562–75. https://doi.org/10.1038/s41380-018-0070-0.
Demontis D, Walters RK, Martin J, Mattheisen M, Als TD, Agerbo E, et al. Discovery of the first genome-wide significant risk loci for attention deficit/hyperactivity disorder. Nat Genet. 2019;51(1):63–75. https://doi.org/10.1038/s41588-018-0269-7.
Martin J, Hamshere ML, Stergiakouli E, O’Donovan MC, Thapar A. Genetic risk for attention-deficit/hyperactivity disorder contributes to neurodevelopmental traits in the general population. Biol Psychiatry. 2014;76(8):664–71. https://doi.org/10.1016/j.biopsych.2014.02.013.
Jansen AG, Dieleman GC, Jansen PR, Verhulst FC, Posthuma D, Polderman TJ. Psychiatric polygenic risk scores as predictor for attention deficit/hyperactivity disorder and autism spectrum disorder in a clinical child and adolescent sample. Behav Genet. 2019:1–10.
Groen-Blokhuis MM, Middeldorp CM, Kan K-J, Abdellaoui A, Van Beijsterveldt CE, Ehli EA, et al. Attention-deficit/hyperactivity disorder polygenic risk scores predict attention problems in a population-based sample of children. J Am Acad Child Adolesc Psychiatry. 2014;53(10):1123–9. e6.
Nigg J, Nikolas M, Burt SA. Measured gene-by-environment interaction in relation to attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2010;49(9):863–73. https://doi.org/10.1016/j.jaac.2010.01.025.
Gould KL, Coventry WL, Olson RK, Byrne B. Gene-environment interactions in ADHD: the roles of SES and chaos. J Abnorm Child Psychol. 2018;46(2):251–63. https://doi.org/10.1007/s10802-017-0268-7.
Todd RD, Neuman RJ. Gene–environment interactions in the development of combined type ADHD: evidence for a synapse-based model. Am J Med Genet B Neuropsychiatr Genet. 2007;144(8):971–5.
Nikolas M, Friderici K, Waldman I, Jernigan K, Nigg JT. Gene× environment interactions for ADHD: synergistic effect of 5HTTLPR genotype and youth appraisals of inter-parental conflict. Behav Brain Funct. 2010;6(1):23. https://doi.org/10.1186/1744-9081-6-23.
Langley K, Turic D, Rice F, Holmans P, Van Den Bree M, Craddock N, et al. Testing for gene× environment interaction effects in attention deficit hyperactivity disorder and associated antisocial behavior. Am J Med Genet B Neuropsychiatr Genet. 2008;147(1):49–53.
Sonuga-Barke EJ, Koerting J, Smith E, McCann DC, Thompson M. Early detection and intervention for attention-deficit/hyperactivity disorder. Expert Rev Neurother. 2011;11(4):557–63. https://doi.org/10.1586/ern.11.39.
Takagai S, Tsuchiya KJ, Itoh H, Kanayama N, Mori N, Takei N. Cohort profile: Hamamatsu birth cohort for mothers and children (HBC Study). Int J Epidemiol. 2016;45(2):333–42. https://doi.org/10.1093/ije/dyv290.
Lewis CM, Vassos E. Prospects for using risk scores in polygenic medicine. Genome Med. 2017;9(1):96. https://doi.org/10.1186/s13073-017-0489-y.
Takahashi N, Harada T, Nishimura T, Okumura A, Choi D, Iwabuchi T, et al. Association of genetic risks with autism spectrum disorder and early neurodevelopmental delays among children without intellectual disability. JAMA Netw Open. 2020;3(2):e1921644-e.
Kawai Y, Mimori T, Kojima K, Nariai N, Danjoh I, Saito R, et al. Japonica array: improved genotype imputation by designing a population-specific SNP array with 1070 Japanese individuals. J Hum Genet. 2015;60(10):581–7. https://doi.org/10.1038/jhg.2015.68.
Browning BL, Zhou Y, Browning SR. A one-penny imputed genome from next-generation reference panels. Am J Hum Genet. 2018;103(3):338–48. https://doi.org/10.1016/j.ajhg.2018.07.015.
de Toro-Martín J, Guénard F, Tchernof A, Pérusse L, Marceau S, Vohl M-C. Polygenic risk score for predicting weight loss after bariatric surgery. JCI Insight. 2018;3(17).
DuPaul GJ, Power TJ, McGoey KE, Ikeda MJ, Anastopoulos AD. Reliability and validity of parent and teacher ratings of attention-deficit/hyperactivity disorder symptoms. J Psychoeduc Assess. 1998;16(1):55–68. https://doi.org/10.1177/073428299801600104.
Nigg JT, Breslau N. Prenatal smoking exposure, low birth weight, and disruptive behavior disorders. J Am Acad Child Adolesc Psychiatry. 2007;46(3):362–9. https://doi.org/10.1097/01.chi.0000246054.76167.44.
Ask H, Gustavson K, Ystrom E, Havdahl KA, Tesli M, Askeland RB, et al. Association of gestational age at birth with symptoms of attention-deficit/hyperactivity disorder in children. JAMA Pediatr. 2018;172(8):749–56. https://doi.org/10.1001/jamapediatrics.2018.1315.
Little RJ. A test of missing completely at random for multivariate data with missing values. J Am Stat Assoc. 1988;83(404):1198–202. https://doi.org/10.1080/01621459.1988.10478722.
Li C. Little's test of missing completely at random. Stata J. 2013;13(4):795–809. https://doi.org/10.1177/1536867X1301300407.
Pharoah P, Stevenson C, Cooke R, Stevenson R. Prevalence of behaviour disorders in low birthweight infants. Arch Dis Child. 1994;70(4):271–4. https://doi.org/10.1136/adc.70.4.271.
Shariat M, Gharaee J, Dalili H, Mohammadzadeh Y, Ansari S, Farahani Z. Association between small for gestational age and low birth weight with attention deficit and impaired executive functions in 3–6 years old children. J Matern Fetal Neonatal Med. 2019;32(9):1474–7. https://doi.org/10.1080/14767058.2017.1408071.
Galéra C, Côté SM, Bouvard MP, Pingault J-B, Melchior M, Michel G, et al. Early risk factors for hyperactivity-impulsivity and inattention trajectories from age 17 months to 8 years. Arch Gen Psychiatry. 2011;68(12):1267–75. https://doi.org/10.1001/archgenpsychiatry.2011.138.
Stein RE, Siegel MJ, Bauman LJ. Are children of moderately low birth weight at increased risk for poor health? a new look at an old question. Pediatrics. 2006;118(1):217–23. https://doi.org/10.1542/peds.2005-2836.
Groen-Blokhuis MM, Middeldorp CM, van Beijsterveldt CE, Boomsma DI. Evidence for a causal association of low birth weight and attention problems. J Am Acad Child Adolesc Psychiatry. 2011;50(12):1247–54. e2.
Murray E, Pearson R, Fernandes M, Santos IS, Barros FC, Victora CG, et al. Are fetal growth impairment and preterm birth causally related to child attention problems and ADHD? evidence from a comparison between high-income and middle-income cohorts. J Epidemiol Community Health. 2016;70(7):704–9. https://doi.org/10.1136/jech-2015-206222.
Bohnert KM, Breslau N. Stability of psychiatric outcomes of low birth weight: a longitudinal investigation. Arch Gen Psychiatry. 2008;65(9):1080–6. https://doi.org/10.1001/archpsyc.65.9.1080.
Smith TF, Schmidt-Kastner R, McGeary JE, Kaczorowski JA, Knopik VS. Pre-and perinatal ischemia-hypoxia, the ischemia-hypoxia response pathway, and ADHD risk. Behav Genet. 2016;46(3):467–77. https://doi.org/10.1007/s10519-016-9784-4.
Getahun D, Rhoads GG, Demissie K, Lu S-E, Quinn VP, Fassett MJ, et al. In utero exposure to ischemic-hypoxic conditions and attention-deficit/hyperactivity disorder. Pediatrics. 2013;131(1):e53–61. https://doi.org/10.1542/peds.2012-1298.
Anand D, Colpo GD, Zeni G, Zeni CP, Teixeira AL. Attention-deficit/hyperactivity disorder and inflammation: what does current knowledge tell us? a systematic review. Front Psychiatry. 2017;8:228. https://doi.org/10.3389/fpsyt.2017.00228.
Fortier M-È, Sengupta SM, Grizenko N, Choudhry Z, Thakur G, Joober R. Genetic evidence for the association of the hypothalamic–pituitary–adrenal (HPA) axis with ADHD and methylphenidate treatment response. NeuroMolecular Med. 2013;15(1):122–32. https://doi.org/10.1007/s12017-012-8202-1.
Graignic-Philippe R, Dayan J, Chokron S, Jacquet A, Tordjman S. Effects of prenatal stress on fetal and child development: a critical literature review. Neurosci Biobehav Rev. 2014;43:137–62. https://doi.org/10.1016/j.neubiorev.2014.03.022.
Schote AB, Bonenberger M, Pálmason H, Seitz C, Meyer J, Freitag CM. Glucocorticoid receptor variants in childhood attention-deficit/hyperactivity disorder and comorbid psychiatric disorders. Psychiatry Res. 2016;246:275–83. https://doi.org/10.1016/j.psychres.2016.10.001.
Dias TGC, Kieling C, Graeff-Martins AS, Moriyama TS, Rohde LA, Polanczyk GV. Developments and challenges in the diagnosis and treatment of ADHD. Braz J Psychiatry. 2013;35(suppl 1):S40–50. https://doi.org/10.1590/1516-4446-2013-S103.
Thapar A, Cooper M, Eyre O, Langley K. Practitioner review: what have we learnt about the causes of ADHD? J Child Psychol Psychiatry. 2013;54(1):3–16. https://doi.org/10.1111/j.1469-7610.2012.02611.x.
Smith TF, Anastopoulos AD, Garrett ME, Arias-Vasquez A, Franke B, Oades RD, et al. Angiogenic, neurotrophic, and inflammatory system SNPs moderate the association between birth weight and ADHD symptom severity. Am J Med Genet B Neuropsychiatr Genet 2014;165(8):691-704, DOI: https://doi.org/10.1002/ajmg.b.32275.
van der Meer D, Hoekstra P, Bralten J, Van Donkelaar M, Heslenfeld D, Oosterlaan J, et al. Interplay between stress response genes associated with attention-deficit hyperactivity disorder and brain volume. Genes Brain Behav. 2016;15(7):627–36. https://doi.org/10.1111/gbb.12307.
Ohnishi M, Okada R, Tani I, Nakajima S, Tsujii M. Japanese version of school form of the ADHD-RS: an evaluation of its reliability and validity. Res Dev Disabil. 2010;31(6):1305–12. https://doi.org/10.1016/j.ridd.2010.07.011.
Duncan L, Shen H, Gelaye B, Meijsen J, Ressler K, Feldman M, et al. Analysis of polygenic risk score usage and performance in diverse human populations. Nat Commun. 2019;10(1):1–9.
Du Rietz E, Coleman J, Glanville K, Choi SW, O’Reilly PF, Kuntsi J. Association of polygenic risk for attention-deficit/hyperactivity disorder with co-occurring traits and disorders. Biol Psychiatry Cogn Neurosci Neuroimaging. 2018;3(7):635–43. https://doi.org/10.1016/j.bpsc.2017.11.013.
Brikell I, Larsson H, Lu Y, Pettersson E, Chen Q, Kuja-Halkola R, et al. The contribution of common genetic risk variants for ADHD to a general factor of childhood psychopathology. Mol Psychiatry. 2018:1–13.
Acknowledgements
We are grateful to the study participants for their cooperation and participation in the HBC Study. We would like to thank Ms. Chikako Nakayasu, Ms. Yuko Amma, and Ms. Haruka Suzuki for the data collection and Ms. Noriko Kodera and Ms. Emi Higashimoto for the administration. We would also like to thank Editage (www.editage.com) for the English language editing.
Funding
This research was funded by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology in Japan (Grant Number 19H03582 awarded to KJT and Grant Number 21K17268 to MSR); Japan Agency for Medical Research and Development (AMED BIRTHDAY Grant Number JP20gk0110039 to KJT); HUSM Grant-in-Aid (Grant Number 101337 to MSR); and Collaborative Research Network for Asian Children with Developmental Disorders (MSR). The funders had no role in the study design; data collection, analysis, and interpretation of data; and writing of the manuscript.
Author information
Authors and Affiliations
Contributions
MSR, NaT, and KJT have conceptualized the study. KJT supervised the study. TI, TN, TH, AO, and KJT collected the data for the study. NaT analyzed and imputed the genetic risk score. MSR performed the statistical analysis. MSR drafted the manuscript in consultation with KJT and intellectual inputs from NaT, TI, TN, TH, AO, YN, NT, and KJT. All authors contributed to the critical revision of the manuscript. MSR and KJT had primary responsibility for final content. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study procedures were approved by the Hamamatsu University School of Medicine and the University Hospital Ethics Committee (approval number: 17-037, 19-145 and 20-233). Written informed consent was obtained from each caregiver for his/her infant’s participation. The study was performed following the Helsinki declaration.
Consent for publication
Not applicable
Competing interests
The authors have declared that no competing interests exist.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional File 1.
Figure S1 - Distribution of polygenic risk score for ADHD in HBC study.
Additional File 2.
Table S1 - Background characteristics of study participants according to birth weight categories.
Additional File 3.
Figure S2 - Distribution of ADHD total scores between birth weight categories.
Additional File 4.
Figure S3 - Distribution of scores on inattention traits and hyperactivity traits between birth weight categories.
Additional File 5.
Table S2 - Association of birth weight (continuous) and polygenic risk with ADHD scores among Japanese children at age 8-9 years.
Additional File 6.
Table S3 - Independent and interaction effects of birth weight categories and polygenic risk score for ADHD with ADHD total score among Japanese children at age 8-9 years.
Additional File 7.
Table S4 - Comparison of background characteristics of children included in the analysis and those excluded from the analysis due missing information on ADHD-RS or PRS.
Additional File 8.
Table S5 - Little’s test for Missing Completely at random and test for covariate-dependent missingness.
Additional File 9.
Table S6 - Association of birth weight categories and genetic risk with ADHD total score among Japanese children at age 8-9 years after multiple imputation of missing polygenic risk score for 137 children.
Additional File 10.
Table S7 - Association of birth weight categories and genetic risk with inattention and hyperactivity scores among Japanese children at age 8-9 years after multiple imputation of missing polygenic risk score for 137 children.
Additional File 11.
Table S8 - Sensitivity analysis for the association of birth weight categories and genetic risk with ADHD total score among Japanese children at age 8-9 years after recoding missing PRS to the end of the spectrum.
Additional File 12.
Table S9 - Sensitivity analysis for the association of birth weight categories and genetic risk with inattention and hyperactivity scores among Japanese children at age 8-9 years after recoding missing PRS to the end of the spectrum.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rahman, M.S., Takahashi, N., Iwabuchi, T. et al. Elevated risk of attention deficit hyperactivity disorder (ADHD) in Japanese children with higher genetic susceptibility to ADHD with a birth weight under 2000 g. BMC Med 19, 229 (2021). https://doi.org/10.1186/s12916-021-02093-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-021-02093-3