
Abstract
Background
Germline cancer genetic testing has become a standard evidence-based practice, with established risk reduction and screening guidelines for genetic carriers. Access to genetic services is limited in many places, which leaves many genetic carriers unidentified and at risk for late diagnosis of cancers and poor outcomes. This poses a problem for childhood cancer survivors, as this is a population with an increased risk for subsequent malignant neoplasms (SMN) due to cancer therapy or inherited cancer predisposition. The ENGaging and Activating cancer survivors in Genetic services (ENGAGE) study evaluates the effectiveness of an in-home, collaborative PCP model of remote telegenetic services to increase uptake of cancer genetic testing in childhood cancer survivors compared to usual care options for genetic testing.
Methods
The ENGAGE study is a 3-arm randomized hybrid type 1 effectiveness and implementation study within the Childhood Cancer Survivor Study population which tests a clinical intervention while gathering information on its delivery during the effectiveness trial and its potential for future implementation among 360 participants. Participants are randomized into three arms. Those randomized to Arm A receive genetic services via videoconferencing, those in Arm B receive these services by phone, and those randomized to Arm C will receive usual care services.
Discussion
With many barriers to accessing genetic services, innovative delivery models are needed to address this gap and increase uptake of genetic services. The ENGAGE study evaluates the effectiveness of an adapted model of remote delivery of genetic services to increase the uptake of recommended genetic testing in childhood cancer survivors. This study assesses the uptake in remote genetic services and identify barriers to uptake to inform future recommendations and a theoretically-informed process evaluation which can inform modifications to enhance dissemination beyond this study population and to realize the benefits of precision medicine.
Trial registration
This protocol was registered at clinicaltrials.gov (NCT04455698) on July 2, 2020.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Childhood cancer survivors and genetic testing
Germline cancer genetic testing has become a standard evidence-based practice, with established risk reduction and screening guidelines for genetic carriers [1,2,3,4]. Yet, many at-risk patients do not have access to genetic services, leaving numerous genetic carriers unidentified and at an increased risk of late diagnosis of cancers and poor outcomes [5,6,7,8,9]. Many areas in the U.S. have limited access to genetic specialists, requiring patients to travel long distances to referral centers to received genetic services. Some patients proceed with testing without a genetic provider (i.e. with their PCP). This has been associated with lower genetic knowledge and satisfaction, and many at-risk patients do not proceed with testing at all [10,11,12,13]. Given increasing precision medicine applications and a limited and geographically restricted workforce of genetic providers, innovative delivery models that are responsive to the needs of geographically and sociodemographically diverse patient populations in their local health care systems are needed [8, 14,15,16,17].
Suboptimal access to genetic services is an acute problem for survivors of childhood cancer, as many in this population are at high risk for subsequent malignant neoplasms (SMN) because of cancer therapy or an inherited cancer predisposition [18, 19]. A recent study revealed that 12% of survivors had a germline mutation in a cancer susceptibility gene (e.g. TP53, BRCA1/2) [20]. Guidelines from National Comprehensive Cancer Network (NCCN) and Children’s Oncology Group (COG) recommend survivors with personal (e.g. sarcoma) and/or family history of cancer be referred for genetic testing to implement appropriate surveillance or preventive measures (e.g. breast cancer surveillance or prophylactic mastectomy in women with TP53 or BRCA1/2) [1, 21]. Yet, less than 15% of survivors have access to genetic services [22]. Further, survivors and their PCPs are largely unaware of survivor’s health risks, and overall adherence to surveillance guidelines is low [23,24,25,26]. These data highlight the need for childhood cancer survivors to be referred for genetic counseling and testing, which could reduce morbidity and mortality in this high-risk population.
Remote telehealth genetic services
Remotely providing genetic services by phone or videoconference as an alternative to in-person delivery could address access barriers. Randomized studies established that patient-reported outcomes (e.g. knowledge, distress) with remote phone services were no worse than in-person services for cancer genetic testing, although uptake of testing in some studies was lower in the remote phone arm than in-person services [27,28,29,30]. Remote videoconference services have been utilized as an alternative to in-person services and have increased during the COVID pandemic [31,32,33,34,35,36]. In cancer genetics, remote videoconference services have demonstrated feasibility and high patient satisfaction, but published studies are limited, heterogeneous in setting and delivery, nonrandomized, small and have limited patient-reported outcomes [37,38,39,40,41,42]. Given lower uptake of genetic testing in two studies utilizing phone services, and preliminary data suggesting potential benefits in knowledge with videoconference in community-based populations, further evaluation of the relative benefits of videoconference over phone are needed. Additionally, moderator analyses can help identify who benefits less or more from access to videoconference over phone services [43].
In a randomized study of remote telegenetic services delivered on-site at community adult oncology practices, 80% of patients who met NCCN criteria had genetic services, as compared to 16% (OR 30.5, p < 0.001) in the usual care arm (in all cases with their local PCP and not a genetic provider) [44]. While remote genetic services can significantly increase uptake of genetic testing in patients in community practices, the on-site model requires multi-level support within practices and still requires proximity to select community sites, which limits scalability for a nationally distributed population (Fig. 1). Thus, a model where any patient or doctor can access services, where services are provided in the home (eliminating any remaining travel burdens) and are not tied to a participating center, could provide even greater scalability, access to genetic services and uptake of genetic testing, which will be critical to realizing the potential of precision medicine.

Comparison of on-site to in-home model of genetic services
The in-home, collaborative PCP model for remote genetic services
To address the gap in access to genetic services, we propose to evaluate the effectiveness of an in-home, collaborative PCP model of remote delivery of genetic services to increase the uptake of recommended genetic assessment and testing in childhood cancer survivors. A PCP Advisory Board, including 8 Family Physicians, General Internists, and an OB/Gyn that practice in diverse community practices (urban, rural, suburban, Northeast, Southeast, Midwest, South and West Coast), informed the development and procedures of the in-home collaborative PCP model and confirm that it is a feasible and acceptable approach (Fig. 1). Advisory board members confirmed the value of access to genetic services, as many PCPs don’t have sufficient expertise to address genetic testing guidelines. They felt many PCPs would be willing to participate if the process was simple and did not require significant provider time. PCPs confirmed that rare and high-risk conditions (e.g. childhood cancer survivors), having patients approach them with requests for services or guideline based recommendations is appropriate (“right place at the right time”). They reported that older PCPs, and those in practices without an electronic medical record or with limited medical and administrative support, might experience barriers to uptake. Recommendations to increase participation included making clear the value of testing, streamlining and simplifying PCP/practice steps, including reminders to minimize burden on the practices, providing access to education materials and answers to frequently asked patient questions and access to the genetic counselor for specific clinical and screening questions even after testing.
Present study
This study, ENGaging and Activating cancer survivors in Genetic services (ENGAGE), describes a 3-arm randomized Hybrid 1 Effectiveness and Implementation study in a population of 360 Childhood Cancer Survivor Study (CCSS) participants to evaluate the effectiveness of an in-home collaborative PCP model of remote telegenetic services to increase uptake of cancer genetic testing in childhood cancer survivors compared to usual care options for genetic testing.
Objectives
The goal of the ENGAGE study is to evaluate the effectiveness of our in-home, collaborative PCP model of remote telegenetic services to increase uptake of cancer genetic testing in childhood cancer survivors compared to usual care options for genetic testing. We hypothesize that this innovative delivery approach has the potential to provide a scalable model that will overcome existing access barriers to services and support optimal patient outcomes in geographically diverse clinical populations, as the indications for genetic testing expand in the era of Precision Medicine.
Specific aim 1
Our primary aim is to evaluate the effectiveness of our in-home collaborative PCP model of remote telegenetic services to increase uptake of genetic services at 6 months as compared to usual care among childhood cancer survivors who meet criteria for cancer genetic testing. The primary outcome is a composite variable indicating whether a person had pre-test counseling or genetic counseling.
Specific aim 2
Our secondary aims are to evaluate the effectiveness of remote videoconferencing to provide greater increase in knowledge and decrease in distress and depression compared with remote phone services (Aim 2a), to examine the moderators of patient outcomes with remote telegenetic services, to understand who benefits less or more from remote services as compared to usual care, and videoconference as compared to phone counseling (Aim 2b), and to estimate intervention costs and incremental cost-effectiveness of the three study arms (Aim 2c).
Specific aim 3
Our third aim is to conduct a multi-stakeholder, mixed-methods Consolidated Framework for Implementation Research (CFIR)-informed implementation evaluation to understand patient, provider and system factors acting as barriers or enablers to uptake of counseling and testing in our in-home, collaborative PCP model to provide recommendations for future wider implementation of this model to populations beyond the CCSS.
Methods
Study design
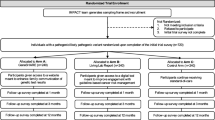
ENGAGE is a 3-arm randomized Hybrid 1 effectiveness and implementation study, which tests a clinical intervention while gathering information on its delivery during the effectiveness trial and its potential for future implementation. We will randomize 360 childhood cancer survivors (1:1:1), who meet guidelines for germline cancer genetic testing (Fig. 2) to remote in-home telegenetic services by videoconference (Aim A), by telephone (Arm B) or to usual care (Aim C). Equally important, we will conduct a multi-stakeholder mixed-methods CFIR-informed concurrent implementation evaluation to understand patient, provider and system factors associated with uptake of telegenetic services and facilitators and barriers to uptake.

Randomized study schema. *6-Month Outcome Survey also given to participants on Arms A and B that have lost contact with Penn Telegenetics before receiving genetic services; participants in Arms A and B who have not had genetic services can still receive services according to their randomized arm
Setting
This study is being conducted within the Childhood Cancer Survivor Study (CCSS), a multi-institutional North American cohort established in 1994 to evaluate the long-term outcomes of childhood cancer survivors [45]. Including patients diagnosed with their primary cancer from 1970 through 1999, the CCSS now follows the outcomes of 24,735 childhood cancer survivors representing both urban and rural North America (See Fig. 3). Based on data from the Surveillance, Epidemiology, and End Results (SEER) Program, the participants in the CCSS cohort are “similar in terms of gender, race, and cancer type by time interval since diagnosis to those reported in SEER, indicating that the CCSS was representative of the larger U.S. population of childhood cancer survivors” [18]. The health care utilization patterns of the CCSS participants have been evaluated periodically, finding that over 80% of participants (regardless of risk of recurrence or late effects) are no longer followed at their treating cancer center [22, 46,47,48], and 88% of CCSS participants report that they have an identified PCP.

U.S. Distribution of CCSS Participants
Remote genetic counseling services in this study are provided through the Penn Telegenetics Program, which was founded in 2012 originating from NCI funded research evaluating remote phone and real-time genetic services in community practices without genetic services [49]. The program has provided remote genetic services by phone or videoconference in cancer and neurogenetics in over 100 national sites through research or clinical contracts [49, 50]. More recently, Penn Telegenetics developed the Patient Access Program (PAP), permitting individual patients and providers across the nation to access Penn Telegenetic services. In the PAP, Penn Telegenetic Counselors collaborate with local health care providers to provide genetic services in the home. This model includes a physician registration process to facilitate this collaborative care model and this model is the basis for the in-home, collaborative PCP model in this study and several other nationally accruing remote services studies (NCT04353973, NCT05427240). At the initiation of ENGAGE, 66 patients (in 17 different states) and 32 physicians had successfully registered with the program and 50 (76%) patients had either completed (n = 44) or scheduled (n = 6) genetic counseling, providing key preliminary data supporting this model. The Penn Telegenetics genetic counselors (GCs) are licensed in all US States as required by state licensure laws [51].
The ENGAGE study is co-implemented with teams at the University of Pennsylvania (Penn Telegenetics), University of Chicago and St. Jude Children’s Research Hospital (Coordinating Center for the Childhood Cancer Survivor Study). Given that primary intervention activities occur with the Penn Telegenetics Program, the University of Pennsylvania is the IRB of record.
Study participants
Eligibility
Eligibility criteria include individuals enrolled in CCSS, who are 18 years or older, able to understand and communicate in English, reside in the United States, have a history of a CNS tumor or sarcoma (excluding Ewing sarcoma), one or more SMN or have a family history of cancer qualifying them for genetic testing according to the NCCN guidelines [1]. Exclusion criteria include uncorrected or uncompensated speech defects that would lead to the participant being unable to communicate effectively with a medical provider, uncontrolled psychiatric/mental condition or severe physical, neurological, or cognitive deficits rendering the individual unable to understand study goals or tasks. Participants who have already received clinically appropriate multi-gene panel genetic testing are excluded. We elected not to exclude individuals without a usual source of care (e.g. primary care provider) or those without health care insurance. For individuals in these categories, we provide educational materials and resources for obtaining care or insurance.
Recruitment
All potential participants are identified through the CCSS Coordinating Center. The CCSS Coordinating Center uses a combination of electronic (email and text message), mailed, and phone-based recruitment methods to contact all potential participants. The introductory letter includes five videos reviewing the value of genetic testing for childhood cancer survivors (brief animated video, physician explaining the benefit of genetic testing, GC explaining the steps of genetic testing, GC explaining costs and addressing genetic discrimination and GC discussing overcoming apprehension regarding genetic testing), including a study invitation letter by email with five reminders and follow up calls.
The ENGAGE study utilizes a participant portal called myLTFU, a HIPAA-compliant interface that allows direct and interactive messaging and web portal-based data collection. This portal allows participants to consent, view educational content, complete surveys, track study progress outcomes, upload and download documents and pictures, and securely interact with the study team. Communication with participants takes place through the DatStat Connect Platform, which allows for pre-programmed messages and workflows to be activated by situational triggers. Recruitment invitations started in August, 2021.
Enrollment goals
As outlined below, our enrollment goal for the primary aim is 120 per arm or 360 participants total. We elected to contact childhood cancer survivors of osteosarcoma, soft-tissue sarcoma, and multiple primary cancers, as no additional information is needed to confirm their eligibility for genetic testing. If necessary, we would next contact individuals with a first-degree relative with ovary, male breast or pancreatic cancer as they meet NCCN criteria with this history alone. Next, we would contact those with a family history of colon, uterine or breast cancer, although family history details would need to be assessed to determine if they meet NCCN criteria for genetic testing. As shown in Table 1, we expect to have sufficient CCSS participants to meet our enrollment goal of 360, although if needed we could extend to all childhood cancer survivors and assess family history for eligibility (N = 19,154). Importantly, to increase the generalizability of our findings, we seek to enroll 30% of participants from under-represented minorities.
Study arms
Once participants have completed informed consent and the baseline (T0) survey, they are randomized into one of the potential arms of the study. Randomization assignments are determined by a permuted block design and stratified by gender (e.g. male, female, other). After randomization, participants are sent a flyer via the myLTFU portal that have instructions for contacting the Penn Telegenetics team to schedule an appointment (for Arms A and B) or usual care options (Arm C) for obtaining genetic services [e.g. ask PCP or providers, use the National Society of Genetic Counselors website (www.nsgc.org)] (Fig. 4). In all arms, participants need to take the first step to initiate services, using information provided in the randomization flyer.

Randomized arm information flyers on how to obtain genetic services
ARM A: Remote telegenetic services by videoconference
Participants who contact Penn Telegenetics in Arm A will complete their pre-test counseling session by videoconference in the home or their selected personal location with a Penn Telegenetic Counselor (GC) utilizing communication protocols from related studies [44, 52]. The Telegenetics team will contact the participant up to 6 times (3 calls and 3 emails) to schedule their pre-test counseling session. If a scheduled participant does not show for their appointment, they are contacted 3 times to reschedule. Participants are provided links to download secure videoconferencing software on their home computer or device. The Penn Telegenetics team utilizes a HIPAA-compliant technology platform (Blue Jeans) for videoconference visits. In our communication protocols, if videoconference technology fails, GCs will convert the session to phone. Based on our experience at study start (> 800 telegenetic sessions across studies and clinical contracts), failures occur only 4% of the time, although this may be higher when adapting our model for in-home videoconferencing.
Consistent with standard clinical practice, GCs will review personal and family history (FH), the risks, benefits and limitations of genetic testing, testing options based on their personal and family history (e.g. TP53 testing or a panel of cancer susceptibility genes) and the costs associated with genetic testing. The Penn GC works with the patient to determine appropriate testing and which lab to utilize for testing, provides instructions for completing the test kit and reviews information on testing costs. GCs order the testing through clinical labs (e.g. Invitae or Ambry Genetics) and the labs send test kits to the participant’s home. Through the ENGAGE portal, participants get 3 email and 3 text reminders to return their test kits.
After results are available, the Penn GC shares results with the patient by videoconference at a scheduled visit, and provides the PCP with the chart note, summarizing the results, implications, cancer risk estimates, and standard risk-reducing or screening strategies and implications for relatives. This chart note is also provided to patients, consistent with routine clinical care. Penn GCs are available to answer PCP questions and facilitate referral to regional centers for genetic carriers as indicated. Patients are recommended to follow-up with their PCP to implement any screening and medical (including risk reduction) recommendations.
ARM B: Remote telegenetic services by phone
Participants who contact Penn Telegenetics in Arm B complete their pre-test counseling session by phone in the home or their selected personal location with a Penn Telegenetic Counselor (GC) utilizing communication protocols from related studies [30, 44, 52]. The remainder of procedures for pre-test counseling, genetic testing and post-test counseling sessions are as described above for Arm A.
ARM C: Usual care
As above, participants in the usual care arm will receive print materials reviewing ways to obtain genetic services. These include speaking with their doctor about testing or accessing the National Society of Genetic Counselors, “find a counselor” function on their website. At 6 months participants will be contacted to evaluate if they had genetic testing (see 6-month status survey in Effectiveness Outcomes below). All Arm C participants who have not had genetic testing at 6 months will be offered remote telegenetic services in a waitlist design (Fig. 2). If they accept remote services, they are re-randomized to Arm A or Arm B. This future potential for Telegenetic services (e.g. waitlist design) is not shared with them at the time of enrollment. Rather, they are told that after they complete the 6-month status survey.
Genetic testing
Genetic testing in all arms will be clinical cancer genetic testing through standard clinical commercial labs, consistent with real-world practice and as indicated based on their personal and family history. Genetic testing is intentionally not covered by the study to reflect “real-world” practice. For the subset of participants who are not able to get testing covered by insurance, commercial labs offer financial assistance programs and out-of-pocket testing is often no more than $250. Based on prior experience in populations meeting NCCN criteria for testing, we anticipate this will be < 5% of participants [44].
Genetic testing and PCP collaboration (Arms A and B)
If patients elect to proceed with genetic testing, they will be required to provide their PCP’s contact information, who will be the ordering provider as a licensed physician is required to order genetic testing in most states. Consistent with the Penn Telegenetics Patient Access Program procedures, the Penn Telegenetics Team contacts the PCP office, provides information on Penn Telegenetics Program and requests that the provider register with our program. Registration includes providing their credentials and contact information, so that the GC can collaborate with the PCP to facilitate testing. PCP practice staff will be permitted to complete registration on behalf of the PCP. As above, these procedures have been successful to date in a pilot study and were informed by a PCP Advisory Board.
Outcomes
Conceptual model (Fig. 5)

Conceptual model to evaluate outcomes of innovations to delivery of genetic services
Outcomes in the ENGAGE study have been informed by our conceptual model grounded in The Self-Regulation Theory of Health Behavior (SRTHB) to evaluate innovations in the delivery of genetic services [49, 52,53,54]. This model proposes that the reaction to, and use of health (genetic) information is the product of an individual’s understanding, knowledge, and perception of the disease threat and risk reduction behaviors [53, 55,56,57,58,59,60,61]. It emphasizes “common-sense” representations rather than medical or scientific definitions, and incorporates individual cognitive, emotional, familial, and cultural experiences that might contribute to individual variability in understanding. Thus, it has been proposed that the SRTHB is an ideal framework for considering the outcomes of genetic testing [54, 59, 62]. Understanding the moderators of outcomes with delivery innovations are critical to understanding who benefits more, or less from delivery innovations. The literature supports the hypothesis that cognitive, psychological, and behavioral factors will be moderated by biological test results, [63,64,65,66] cancer history, [64, 67,68,69] sociodemographic factors (e.g. education, race/ethnicity) [64, 69,70,71] and cognitive and emotional factors (e.g. health literacy [72,73,74] and self-efficacy [75, 76]).
Our conceptual model is also guided by the Consolidated Framework for Implementation Research (CFIR), which provides and overarching theoretical framework to evaluate barriers, enhancements, and adaptations to increase successful implementation [77]. Even after health-related interventions have proven efficacy and effectiveness, many fail to translate into clinical settings [78, 79]. Thus, there is increasing recognition of the importance of evaluating and addressing barriers to implementation across diverse health care settings. The Consolidated Framework for Implementation Research (CFIR) provides an overarching theoretical framework to evaluate barriers, enhancements and adaptations to increase successful implementation [77]. Based on our stakeholder interviews and implementation science experts, we have included selected constructs from each of the 5 major CFIR domains (intervention characteristics, outer setting, inner setting, characteristics of individuals and process) as they relate to our intervention (Fig. 5) which will be evaluated in our multi-stakeholder mixed-methods process evaluation (Aim 3). As in other studies, [80,81,82] evaluation of CFIR components is expected to identify patient, provider and system barriers and enablers of our remote delivery interventions and increase future dissemination to increase access and adoption of genetic services.
Effectiveness outcomes (Aim 1)
The primary outcome of Aim 1 is a composite variable of whether the participant had genetic testing or counseling by six months, and uptake of genetic counseling and identification of genetic carriers are considered secondary outcomes. Uptake of counseling, testing and identification of carriers at 6 months (Aim 1) will be obtained through study records for Arms A and B (intervention arms) and through the 6-month status survey in Arm C (usual care) and participants in Arms A and B who did not complete remote services. This time frame was selected as it allows for a range of delays in completion of counseling and testing and was found to be a reasonable time frame in our prior study [44]. The 6-month status survey includes two closed ended questions for the primary outcome (“Have you completed genetic counseling/testing in the past six months?)”. Secondary closed and open-ended items evaluate how they obtained usual care genetic services (provider, setting, method, and costs), their experience (e.g. what was easy/hard? do you have questions about your results?). For those who did not complete genetic services, secondary items explore barriers to services and what might change their interest in genetic services. The 6-month status survey is designed to be interviewer administered, but if necessary can be completed self-administered. Participants who complete the 6-month outcome survey receive a $75 gift card code.
Effectiveness outcomes (Aim 2)
Outcomes to evaluate the effectiveness of remote videoconference as compared to phone services are shown in Table 2. Upon completion of the T0 survey, T1 survey, and T2 survey, participants receive a $25 gift card code. Participants who complete the T3 survey and T4 survey receive a $30 gift card code.
-
1)
Understanding of genetic information will be assessed at baseline (T0, all Arms), post genetic pre-test counseling session (T1), post genetic test (T2), 6 months post genetic testing (T3), and 12 months post genetic testing (T4) for those in Telegenetic Arms A and B. Knowledge of genetic disease will be evaluated using The KnowGene Scale, a 16-item scale administered to patients after genetic testing and/or genetic counseling to measure their understanding of the health implications of genetic testing results. It includes health implications to oneself as well as relatives. This measure covers penetrance, actionability, limitations of current technology, and monogenic inheritance patterns [83].
Perception of genetic disease will include three items (T0-T4), utilized in related research and evaluating perceived risk of developing a second cancer on a verbal scale and perceived numerical risk, as well as a single item evaluating perceived timeline [56, 59].
-
2)
Reactions to genetic information will be assessed at baseline (T0, all Arms), post genetic pre-test counseling session (T1), post genetic test (T2), 6 months post genetic testing (T3), and 12 months post genetic testing (T4) for those in Telegenetic Arms A and B).
-
a)
General anxiety and Depression will be assessed by the 4-item each short Patient Reported Outcomes Measurement Information System (PROMIS), a system of highly reliable, precise measures of patient-reported health status for physical, mental, and social well-being [84,85,86,87].
-
b)
Disease-specific distress will be measured using the 8 –item Impact of Events Scale (IES) [88, 89], also with strong internal consistency (alpha = 0.82–0.90) in genetic delivery studies [90,91,92].
-
c)
Satisfaction with genetic services will be assessed with 9-items evaluating satisfaction with genetic services (T1 and T2). These items have been utilized in our related studies evaluating alternative and traditional genetic delivery models (alpha = 0.73–0.85) [90,91,92,93,94,95,96].
-
d)
Satisfaction with telemedicine will be assessed with 8-items adapted for genetic counseling sessions and utilized in our preliminary studies [44, 97].
-
e)
Multidimensional responses to genetic testing, including positive responses and uncertainty will be assessed using the Multi-dimensional Impact of Cancer Risk Assessment Questionnaire (MICRA) at T2-T4. The MICRA is a 21-items scale that has been utilized in many genetic studies to evaluate distress, uncertainty and positive responses to receipt of genetic test results [98]. The final item was excluded as it is not included in the three subscales and assessed regret which will be assessed in a separate scale.
-
f)
Decisional regret (T2-T4) will be assessed with the 5-item validated Decision Regret Scale used frequently in related genetic studies [99, 100].
-
a)
-
3)
Use of genetic information will include endorsement of behavior items utilized in the CCSS and related studies (T0, T3, T4). Behaviors will include cancer specific (screening, prophylactic surgery, chemoprevention) and general risk modifying behaviors (e.g. diet, exercise, tobacco and alcohol use). Communication with providers and relatives following disclosure will be measured as well.
-
4)
Cost of remote services and usual care: Estimation of intervention costs will adopt a societal perspective, including relevant direct medical and nonmedical costs borne by providers, payers and patients. Information to estimate intervention costs will be collected from study billing and payment records (e.g. print materials, postage) and telegenetic staff logs (personnel time). Intervention cost estimates will not include the cost of resources used solely for research purposes. Information about patient time and travel and other out-of-pocket costs (e.g. co- payments), will be obtained through the participant surveys. Service use will be assessed at T1, T2, T3 and T4 timepoints.
-
5)
Moderators of patient outcomes with remote telegenetic services (Aim 2b) will be collected at T0 only and include:
-
a)
Sociodemographic data will include race/ethnicity, education, marital status, gender, age, employment status, household income, health insurance (yes/no) and a usual source of medical care (yes/no) which will be collected in the Baseline Survey (T0).
-
b)
History of cancer will be collected in the Baseline Survey (T0).
-
c)
Genetic test result (positive, negative, true negative and test/genes included) will be obtained from Telegenetic Service records and the 6-Month Outcome Survey.
-
d)
Health literacy will be assessed at baseline (T0) with 3 health literacy Brief Literacy Screen (BHLS) screening items which have been validated to detect inadequate health literacy in clinical medical populations [101].
-
e)
Computer literacy will be assessed at baseline (T0) with selected items from the NCI Health Information National Trends Survey (HINTS), including internet and social media use (8 items), electronic medical record use and perceptions of privacy (14 items) [102].
-
f)
Self-Efficacy will be measured at baseline (T0) with the 4-item PROMIS Self-efficacy short form for managing chronic conditions, which has been validated in adults with medical conditions (including cancer) and has good internal consistency (alpha = 0.85–0.92) [103].
-
g)
Financial wellness will be measure at baseline (T0) with 2 items from the Personal Financial Wellness Scale [104].
-
h)
Psychological impacts due to COVID-19 will be assessed using 15–16 items previously utilized in the CCSS to assess the impact of the COVID-19 pandemic on CCSs. The final item asking about number of individuals in the household is excluded at T2. While this protocol is independent of COVID-19, there is potential for COVID-19 events and impact on psychosocial outcomes to impact other primary and secondary outcomes. The measure is included to allow for analyses to evaluate the impact of these on study outcomes [105].
-
a)
Implementation outcomes
Implementation outcomes are determined by identifying key CFIR-informed constructs across the five domains to evaluate factors related to uptake of remote telegenetic services, implementation facilitators, and barriers and adaptations (Fig. 5, Table 3). Key informant interviews will be conducted with patients, PCPs and practice staff as part of our Aim 3 implementation evaluation. Key informants will include:
-
1)
Patients: A purposive sample of 20–40 patients in intervention arms A and B (e.g. up to 20 from each arm). Throughout recruitment, diversity variables will be tracked in order to inform ongoing sampling and maximize representativeness in terms of gender, race/ethnicity, education and uptake (enrolled but did not complete counseling, completed counseling and completed testing);
-
2)
PCPs: 15–30 PCPs identified by participants to collaborate for delivery of remote telegenetic services in Arms A or B. As above, we will seek to maximize representativeness in terms of gender, race/ethnicity, years in practice, type of practice and uptake (registered with patient and completed services, registered but did not complete services, declined registration);
-
3)
Medical office staff: 15–30 office staff affiliated with PCPs will be contacted. Staff can participate even if the PCP declines participation in the process evaluation.
We seek to continue recruitment to the above enrollment goals or until data saturation occurs across the theoretical domain (e.g. no new themes introduced within the constructs included in key informant interviews) [106]. Interviews will be conducted by phone by research staff, audio recorded and transcribed.
Data analysis plan
Primary effectiveness analysis: remote telegenetic services compared to usual care (Aim 1)
We hypothesize that participants who are randomized to remote telegenetic services will have significantly higher uptake of genetic testing or genetic counseling at 6 months. We will use Fisher’s Exact tests to compare uptake of genetic testing and pre-test counseling between the arms, and these will be two separate binary 0/1 variables. The primary comparison groups will be the usual care and wait list group versus the combined remote telegenetics groups (videoconference plus phone) prior to randomization of the waitlist group. For the primary analyses, we will use an intention to treat approach where comparisons are made between randomization arms. In secondary analyses, we will compare the randomization arms to investigate if potential confounders (e.g. age) are balanced among the randomization arms, and this will be done via pairwise Wilcoxen-rank sum tests and Chi-squared tests as appropriate. If any potential confounders are not found to be balanced among the randomization arms (i.e. p < 0.10 for any potential confounders in pairwise comparisons), we will use multiple logistic regressions of uptake to investigate the randomization arm effect. In these models, we will include randomization arms as binary (0/1) indicator covariates (leaving one out as the reference), and we will also include the potential confounders as covariates in the regressions.
We do not expect substantial missing data, although there may be loss to follow-up over time. For the primary outcomes, we will assume that those lost to follow-up did not have pre-test counseling or testing (i.e. failures under the intention-to-treat paradigm). Data from our community practice stakeholder interviews suggests this is reasonable since many patients do not get genetic services even when referred. In secondary analyses, we will account for missing data using the multiple imputation technique of Raghunathan with 25 imputed datasets [107]. We will contrast the results obtained through imputation and those obtained from complete case analyses to study if missing data bias could be substantially affecting our inferences.
Sample size justification for aim 1
We chose our sample size to have sufficient power for both Aims 1 and 2. For Aim 1, the sample size was selected to detect average differences in the primary endpoint (a composite variable indicating either genetic testing or genetic counseling) between the primary randomization arms of interest. The primary comparison groups will be the usual care/waitlist group versus the combined remote telegenetics groups (phone or video conference as one group); the primary analysis will consider the groups prior to the waitlist rerandomization. Preliminary data demonstrated that uptake of genetic testing from an ongoing registered randomized trial of remote telegenetic services vs. usual care for cancer genetic testing in community practices was at least 53% (29/55 with uptake) in the intervention arm, but only 17% (4/24 with uptake) in the control arm. With 120 patients in the usual care/waitlist group and 240 patients in the combined telegenetics groups with complete data (after accounting for loss to follow up), we will have > 99% power to detect a similar difference in uptake of genetic testing. This assumes a 1% Type I error rate (2-sided) and the use of Fisher's Exact Test. We set the Type I error rate to a conservative 1% to partially account for multiple hypothesis testing when including secondary outcomes and potential moderators in Aim 3. Given the magnitude of the pilot data differences, we anticipate excellent power for the moderator/subgroup analyses. The comparison of the usual care/waitlist group to the combined telegenetics group will be the comparison used to determine if the study accomplishes its primary objective. The uptake of pre-test counseling (Aim 1 secondary objective) and comparison between the phone and videoconference groups (see Aim 2a) are secondary objectives.
Secondary effectiveness analysis: remote videoconference compared to phone services (Aim 2a)
We hypothesize that remote telegenetic services by videoconferencing will be associated with greater decreases in cancer related distress and depression and increases in knowledge when compared to phone services. We will compare the usual care at baseline group to the combined arms receiving remote services at baseline. For comparisons between the remote videoconferencing versus phone groups, we will assign participants to the remote group assigned at baseline, or after rerandomization for the waitlist group. Our primary change scores for the first three variables will be change between baseline and immediately post genetic testing. For the waitlist group, there will be a second baseline measurement after the usual care period has ended. For the 3 primary analyses in Aim 2, we will use T-tests. We will assess balance of potential confounders (e.g. age, race, study site, waitlist assignment) between arms using T-tests or Fisher’s exact tests as appropriate. Waitlist group will be considered a confounder in these secondary regression analyses. We will use multiple linear regression models to control for potential confounders inadequately balanced. We will include in the models the confounding variables and indicator (binary 0/1 variables) to indicate randomization arms (leaving one group out as the reference). For longitudinal analyses, we will examine time trajectories using regressions estimated by Generalized Estimating Equations (GEE) to account for within subject temporal correlation. Panel time will be included via indicator variables. We will also include interaction terms between randomization arm and time indicators to investigate temporal effects [108]. We will repeat analyses, but assign participants to per-protocol (i.e. restricting sample to those who properly used the assigned method of disclosure) or as-treated groups (e.g. assigning all participants to a group based on the method of disclosure used, regardless of assignment). For Aim 2 secondary outcomes, we will use multiple linear regressions for continuous outcomes and multiple logistic regressions for binary outcomes using GEE-estimation as described.
Sample size justification for aim 2a
We further chose our sample size such that we would have sufficient power for Aim 2 comparisons of the videoconference versus phone arms. After re-randomization of the waitlist group, we anticipate potentially having 180 people/arm randomized to the videoconference or phone arms. Based on prior experience, we anticipate that loss to follow-up will be less than 28% in each arm, leaving us with 130 evaluable participants with follow-up data in each group (180–180*28% = approximately 130). Some of the loss to follow-up will occur prior to the waitlist group being rerandomized. We used our pilot data to determine power for this aim (see Table 2 for estimates). We assumed 85% power and a 1.67% Type I error rate. We used a 1.67% Type 1 error rate (2-sided) by applying a Bonferroni correction for the three outcomes of interest to the typical 5% Type I error rate (5%/3 = 1.67%). We see in Table 4 that we have excellent power for all three arms with at least 95/arm, which is well below our expected 130/arm anticipated sample size. Table 4 also demonstrates that we have sufficient power for subgroup analyses, with a sample size of just 22/arm needed for knowledge comparisons between arms.
Moderator analysis (Aim 2b)
To evaluate moderators of patient cognitive, affective and behavioral outcomes (Aim 2b), we will use logistic regressions in which we include variables of interest as covariates. For moderation (i.e. effect modifier analyses), we will include indicator variables for randomization arms in the GEE-estimated multiple linear (for continuous outcomes) or logistic regressions (for uptake). We will also include panel time indicators, the potential moderator variables, and all two-way and three-way interactions among the arm/time/moderator variables. Interactions are created by multiplying two variables together [108]. We will examine non-time moderators separately, and will examine multiple regression models with potential confounding variables.
We will repeat the analyses but assign participants to per-protocol (i.e. restricting sample to those who properly used the method of disclosure as assigned) or as-treated groups (e.g. assigning all participants to a group based on the method of disclosure used, regardless of group assignment).
Intervention costs and incremental cost-effectiveness analysis (Aim 2c)
The economic impact of remote telegenetic services (Aim 2c) will be assessed by performing: 1) cost analysis and 2) cost-effectiveness analysis. The goal of the cost analysis is to estimate the cost of delivering remote telegenetic services, by phone and videoconference, compared to usual care. As above, the cost analysis will take a societal perspective, including the costs of all resources consumed for the implementation and delivery of remote genetic services. Separately, we will examine costs from the health system perspective that can inform decisions about the provision and reimbursement of services, and ultimately will influence the effective dissemination and implementation of remote telegenetic services beyond the study. Cost-effectiveness will be estimated as the incremental cost per (1) additional survivor who receives genetic testing, and (2) additional mutations detected. The numerator of the incremental cost-effectiveness ratio (ICER) will include intervention costs and patient time and travel costs, estimated as described above. In the first analysis, the denominator will be defined by the primary trial endpoint of genetic testing received within 6 months. Because receipt of genetic testing is the measure of effectiveness in this case (i.e. the denominator of the ICER), neither the cost of testing nor the cost of related services provided after genetic testing will be included in the numerator. For the second analysis, the numerator of the ICER will include both genetic test costs and any related health care service costs (additional tests, visits, counseling) associated with genetic testing at 6 months. Incremental cost effectiveness will be estimated using standard methods, and sensitivity analysis will be used to assess the impact of assumptions and uncertainty on results and conclusions [109, 110].
Mixed-methods CFIR-informed implementation analysis (Aim 3)
We hypothesize that our CFIR-informed multi-stakeholder mixed-methods process evaluation will identify barriers to uptake and inform recommendations for future adaptation and sustainability. We will quantitatively characterize factors associated with uptake using T-tests (continuous predictors), chi- squared tests (categorical predictors), and multiple logistic regressions (multivariable models). We will control for randomization arm in multivariable models. Qualitative data will be analyzed using a deductive content analysis approach and CFIR as the coding framework [77, 82, 111]. The qualitative data will include patient surveys and key informant interviews, notes from the PCP Advisory Board and notes and debriefing from the telegenetics service and research team meetings. Guided by consensual qualitative methods [112, 113], two independent coders review notes and assign responses to CFIR constructs. Finally, using a convergent mixed-methods approach [114], we will merge the quantitative and qualitative data, organized by the 5 CFIR domains to evaluate which constructs were associated with, or more prevalent among: a) patients who had testing and those who did not and b) PCPs who registered and their patient completed testing, PCPs who registered and their patient did not complete testing, PCPs who never registered (were contacted by the patient but did not support testing through our model of remote telegenetic services). As in other studies [80,81,82], evaluation of CFIR components is expected to identify patient, provider and system barriers and enablers of our remote delivery interventions and increase future dissemination to increase access and adoption of genetic services.
Discussion
We hypothesize that our adapted in-home, collaborative PCP model of remote telegenetic services has the potential to provide a scalable model that will overcome existing access barriers to genetic services and support optimal patient outcomes in geographically diverse clinical populations, as the indications for genetic testing expand in the era of Precision Medicine. Further, we believe the CCSS provides an ideal “real-world’ population of socio-demographically and geographically diverse patients to empirically evaluate this novel delivery model.
Limitations and potential challenges
There are potential limitations we may encounter in this study. We are relying on the 6-month status survey to evaluate what occurs in the usual care arm. Loss to attrition for any of the surveys may result in some missing data. We plan to monitor completion and consider reducing survey burdens or increasing incentives to obtain generalizable data. While we have had strong PCP willingness to register with the Penn Telegenetics Program, we may find some PCP are not willing to collaborate to facilitate genetic services for patients in the intervention arms. Understanding these barriers, if they occur, could inform future interventions or modifications to optimize access to genetic services in the primary care setting. Some patients may not have coverage for testing or face high out-of-pocket costs. While we expect this to be limited, understanding real-world cost barriers to testing will be helpful to advancing equitable access to precision medicine.
Potential for impact and implications
The ENGAGE Study will provide critical empiric data on the effectiveness of an in-home, collaborative PCP telegenetic service model to increase the uptake of genetic testing and a theoretically-informed process evaluation which can inform modifications to enhance dissemination beyond this study population and to realize the benefits of precision medicine.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
- AYA:
-
Adolescent and young adult
- CCSS:
-
Childhood Cancer Survivor Study
- COG:
-
Children’s Oncology Group
- CFIR:
-
Consolidated Framework for Implementation Research
- ENGAGE:
-
Engaging and Activating Cancer Survivors in Genetic Services
- GC:
-
Genetic counselor
- HINTS:
-
Health Information National Trends Survey
- NCCN:
-
National Comprehensive Cancer Network
- PCP:
-
Primary care physician
- SMN:
-
Subsequent malignant neoplasms
- SRTHB:
-
Self-Regulation Theory of Health Behavior
References
The National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology [http://www.nccn.org/professionals/physician_gls/f_guidelines.asp]
Force USPST. Genetic risk assessment and BRCA mutation testing for breast and ovarian cancer susceptibility: recommendation statement. Ann Intern Med. 2005;143(5):355–61.
Nelson HD, Huffman LH, Fu R, Harris EL. Genetic risk assessment and BRCA mutation testing for breast and ovarian cancer susceptibility: systematic evidence review for the U.S. Preventive services task force. Ann Intern Med. 2005;143(5):362–79.
Robson M, Offit K. Clinical practice. Management of an inherited predisposition to breast cancer. N Engl J Med. 2007;357(2):154–62.
Armstrong K, Micco E, Carney A, Stopfer J, Putt M. Racial differences in the use of BRCA1/2 testing among women with a family history of breast or ovarian cancer. JAMA, J Am Med Assoc. 2005;293(14):1729–36.
Godard B, Pratte A, Dumont M, Simard-Lebrun A, Simard J. Factors associated with an individual’s decision to withdraw from genetic testing for breast and ovarian cancer susceptibility: implications for counseling. Genet Test. 2007;11(1):45–54.
Lea DH, Johnson JL, Ellingwood S, Allan W, Patel A, Smith R. Telegenetics in Maine: Successful clinical and educational service delivery model developed from a 3-year pilot project. Genet Med. 2005;7(1):21–7.
Forman AD, Hall MJ. Influence of race/ethnicity on genetic counseling and testing for hereditary breast and ovarian cancer. Breast J. 2009;15(Suppl 1):S56–62.
Hawkins AK, Hayden MR. A grand challenge: providing benefits of clinical genetics to those in need. Genet Med. 2011;13(3):197–200.
Armstrong J, Toscano M, Kotchko N, Friedman S, Schwartz MD, Virgo KS, Lynch K, Andrews JE, Aguado Loi CX, Bauer JE, et al. Utilization and outcomes of BRCA genetic testing and counseling in a national commercially insured population: the ABOUT study. JAMA Oncol. 2015;1(9):1251–60.
Cohen SA, Marvin ML, Riley BD, Vig HS, Rousseau JA, Gustafson SL. Identification of genetic counseling service delivery models in practice: a report from the NSGC service delivery model task force. J Genet Couns. 2013;22(4):411–21.
Anderson B, McLosky J, Wasilevich E, Lyon-Callo S, Duquette D, Copeland G. Barriers and facilitators for utilization of genetic counseling and risk assessment services in young female breast cancer survivors. J Cancer Epidemiol. 2012;2012:298745.
Katz SJ, Ward KC, Hamilton AS, McLeod MC, Wallner LP, Morrow M, Jagsi R, Hawley ST, Kurian AW. Gaps in receipt of clinically indicated genetic counseling after diagnosis of breast cancer. J Clin Oncol. 2018;36(12):1218–24.
Mackenzie A, Patrick-Miller L, Bradbury AR. Controversies in communication of genetic risk for hereditary breast cancer. Breast J. 2009;15(Suppl 1):S25–32.
Sivell S, Iredale R, Gray J, Coles B. Cancer genetic risk assessment for individuals at risk of familial breast cancer. Cochrane Database Syst Rev. 2007;2:CD003721.
McBride CM, Rimer BK. Using the telephone to improve health behavior and health service delivery. Patient Educ Couns. 1999;37(1):3–18.
Ndiaye K, Krieger JR, Warren JR, Hecht ML, Okuyemi K. Health disparities and discrimination: three perspectives. J Health Dispar Res Pract. 2008;2(3):51–71.
Phillips SM, Padgett LS, Leisenring WM, Stratton KK, Bishop K, Krull KR, Alfano CM, Gibson TM, de Moor JS, Hartigan DB, et al. Survivors of childhood cancer in the United States: prevalence and burden of morbidity. Cancer Epidemiol Biomarkers Prev. 2015;24(4):653–63.
Mirabello L, Yeager M, Mai PL, Gastier-Foster JM, Gorlick R, Khanna C, Patino-Garcia A, Sierrasesumaga L, Lecanda F, Andrulis IL, et al. Germline TP53 variants and susceptibility to osteosarcoma. J Natl Cancer Inst. 2015;107(7):djv101.
Wang Z, Wilson CL, Easton J, Thrasher A, Mulder H, Liu Q, Hedges DJ, Wang S, Rusch MC, Edmonson MN, et al. Genetic risk for subsequent neoplasms among long-term survivors of childhood cancer. J Clin Oncol. 2018;36(20):2078–87.
Landier W, Bhatia S, Eshelman DA, Forte KJ, Sweeney T, Hester AL, Darling J, Armstrong FD, Blatt J, Constine LS, et al. Development of risk-based guidelines for pediatric cancer survivors: the children’s oncology group long-term follow-up guidelines from the children’s oncology group late effects committee and nursing discipline. J Clin Oncol. 2004;22(24):4979–90.
Nathan PC, Greenberg ML, Ness KK, Hudson MM, Mertens AC, Mahoney MC, Gurney JG, Donaldson SS, Leisenring WM, Robison LL, et al. Medical care in long-term survivors of childhood cancer: a report from the childhood cancer survivor study. J Clin Oncol. 2008;26(27):4401–9.
Suh E, Daugherty CK, Wroblewski K, Lee H, Kigin ML, Rasinski KA, Ford JS, Tonorezos ES, Nathan PC, Oeffinger KC, et al. General internists’ preferences and knowledge about the care of adult survivors of childhood cancer: a cross-sectional survey. Ann Intern Med. 2014;160(1):11–7.
Nathan PC, Ness KK, Mahoney MC, Li Z, Hudson MM, Ford JS, Landier W, Stovall M, Armstrong GT, Henderson TO, et al. Screening and surveillance for second malignant neoplasms in adult survivors of childhood cancer: a report from the childhood cancer survivor study. Ann Intern Med. 2010;153(7):442–51.
Oeffinger KC, Ford JS, Moskowitz CS, Diller LR, Hudson MM, Chou JF, Smith SM, Mertens AC, Henderson TO, Friedman DL, et al. Breast cancer surveillance practices among women previously treated with chest radiation for a childhood cancer. JAMA. 2009;301(4):404–14.
Kadan-Lottick NS, Robison LL, Gurney JG, Neglia JP, Yasui Y, Hayashi R, Hudson M, Greenberg M, Mertens AC. Childhood cancer survivors’ knowledge about their past diagnosis and treatment: childhood cancer survivor study. JAMA. 2002;287(14):1832–9.
Schwartz MD, Valdimarsdottir HB, Peshkin BN, Mandelblatt J, Nusbaum R, Huang AT, Chang Y, Graves K, Isaacs C, Wood M, et al. Randomized noninferiority trial of telephone versus in-person genetic counseling for hereditary breast and ovarian cancer. J Clin Oncol. 2014;32(7):618–26.
Kinney AY, Butler KM, Schwartz MD, Mandelblatt JS, Boucher KM, Pappas LM, Gammon A, Kohlmann W, Edwards SL, Stroup AM, et al. Expanding access to BRCA1/2 genetic counseling with telephone delivery: a cluster randomized trial. J Natl Cancer Inst. 2014;106(12):dju328.
Kinney AY, Steffen LE, Brumbach BH, Kohlmann W, Du R, Lee JH, Gammon A, Butler K, Buys SS, Stroup AM, et al. Randomized noninferiority trial of telephone delivery of BRCA1/2 genetic counseling compared with in-person counseling: 1-year follow-up. J Clin Oncol. 2016;34(24):2914–24.
Bradbury AR, Patrick-Miller LJ, Egleston BL, Hall MJ, Domchek SM, Daly MB, Ganschow P, Grana G, Olopade OI, Fetzer D, et al. Randomized noninferiority trial of telephone vs in-person disclosure of germline cancer genetic test results. J Natl Cancer Inst. 2018;110(9):985–93.
Ekeland AG, Bowes A, Flottorp S. Effectiveness of telemedicine: a systematic review of reviews. Int J Med Inform. 2010;79(11):736–71.
Agboola SO, Ju W, Elfiky A, Kvedar JC, Jethwani K. The effect of technology-based interventions on pain, depression, and quality of life in patients with cancer: a systematic review of randomized controlled trials. J Med Internet Res. 2015;17(3): e65.
Doraiswamy S, Abraham A, Mamtani R, Cheema S. Use of telehealth during the COVID-19 pandemic: scoping review. J Med Internet Res. 2020;22(12):e24087.
Proussaloglou EM, Koelliker EL, Laprise J, Wilbur JS, Robison K, Stuckey A, Crawford K. The impact of converting to telehealth for cancer genetic counseling and testing during the COVID-19 pandemic. J Genet Couns. 2023. https://doi.org/10.1002/jgc4.1792. Online ahead of print.
Mair F, Whitten P. Systematic review of studies of patient satisfaction with telemedicine. BMJ. 2000;320(7248):1517–20.
Robinson DF, Savage GT, Campbell KS. Organizational learning, diffusion of innovation, and international collaboration in telemedicine. Health Care Manage Rev. 2003;28(1):68–78.
Hilgart JS, Hayward JA, Coles B, Iredale R. Telegenetics: a systematic review of telemedicine in genetics services. Genet Med. 2012;14(9):765–76.
Buchanan AH, Datta SK, Skinner CS, Hollowell GP, Beresford HF, Freeland T, Rogers B, Boling J, Marcom PK, Adams MB. Randomized trial of telegenetics vs. in-person cancer genetic counseling: cost, patient satisfaction and attendance. J Genet Couns. 2015;24(6):961–70.
Solomons NM, Lamb AE, Lucas FL, McDonald EF, Miesfeldt S. Examination of the patient-focused impact of cancer telegenetics among a rural population: comparison with traditional in-person services. Telemed J E Health. 2018;24(2):130–8.
Williams S, Ebrahimzadeh JE, Clay D, Constantino G, Heiman J, Wangensteen KJ, Valverde K, Mahmud N, Katona BW. Comparing telemedicine and in-person gastrointestinal cancer genetic appointment outcomes during the COVID-19 pandemic. Hered Cancer Clin Pract. 2023;21(1):6.
Costanzo S, De Summa S, Maurmo L, Digennaro M, Patruno M, Paradiso A. Remote vs in-person BRCA1/2 non-carriers test disclosure: patients’ choice during Covid-19 pandemic restriction. Fam Cancer. 2023;22(1):43–8.
Bombard Y, Hayeems RZ. How digital tools can advance quality and equity in genomic medicine. Nat Rev Genet. 2020;21(9):505–6.
Pingree S, Hawkins R, Baker T, duBenske L, Roberts LJ, Gustafson DH. The value of theory for enhancing and understanding e-health interventions. Am J Prev Med. 2010;38(1):103–9.
Cacioppo CN, Egleston BL, Fetzer D, Burke Sands C, Raza SA, Reddy Malleda N, McCarty Wood E, Rittenburg I, Childs J, Cho D, et al. Randomized study of remote telehealth genetic services versus usual care in oncology practices without genetic counselors. Cancer Med. 2021;10(13):4532–41.
Robison LL, Armstrong GT, Boice JD, Chow EJ, Davies SM, Donaldson SS, Green DM, Hammond S, Meadows AT, Mertens AC, et al. The childhood cancer survivor study: a national cancer institute-supported resource for outcome and intervention research. J Clin Oncol. 2009;27(14):2308–18.
Oeffinger KC, Mertens AC, Hudson MM, Gurney JG, Casillas J, Chen H, Whitton J, Yeazel M, Yasui Y, Robison LL. Health care of young adult survivors of childhood cancer: a report from the childhood cancer survivor study. Ann Fam Med. 2004;2(1):61–70.
Nathan PC, Ford JS, Henderson TO, Hudson MM, Emmons KM, Casillas JN, Lown EA, Ness KK, Oeffinger KC. Health behaviors, medical care, and interventions to promote healthy living in the childhood cancer survivor study cohort. J Clin Oncol. 2009;27(14):2363–73.
Casillas J, Oeffinger KC, Hudson MM, Greenberg ML, Yeazel MW, Ness KK, Henderson TO, Robison LL, Armstrong GT, Liu Q, et al. Identifying predictors of longitudinal decline in the level of medical care received by adult survivors of childhood cancer: a report from the childhood cancer survivor study. Health Serv Res. 2015;50(4):1021–42.
Bradbury A, Patrick-Miller L, Harris D, Stevens E, Egleston B, Smith K, Mueller R, Brandt A, Stopfer J, Rauch S, et al. Utilizing remote real-time videoconferencing to expand access to cancer genetic services in community practices: a multicenter feasibility study. J Med Internet Res. 2016;18(2): e23.
Langlois CM, Bradbury A, Wood EM, Roberts JS, Kim SYH, Riviere ME, Liu F, Reiman EM, Tariot PN, Karlawish J, et al. Alzheimer’s prevention initiative generation program: development of an APOE genetic counseling and disclosure process in the context of clinical trials. Alzheimers Dement (N Y). 2019;5:705–16.
Roberts MC, Wood EM, Gaieski JB, Bradbury AR. Possible barriers for genetic counselors returning actionable genetic research results across state lines. Genet Med. 2017;19(11):1202–4.
Patrick-Miller LJ, Egleston BL, Fetzer D, Forman A, Bealin L, Rybak C, Peterson C, Corbman M, Albarracin J, Stevens E, et al. Development of a communication protocol for telephone disclosure of genetic test results for cancer predisposition. JMIR Res Protoc. 2014;3(4):e49.
Leventhal H, Benyamini Y, Brownlee S, Diefenbach M, Leventhal EA, Patrick-Miller L. Perceptions of Health and Illness: Current Research and Applications. In: Illness representations: theoretical foundations. 1st ed. Edited by Petrie KJ, Weinman JA. Amsterdam: Harwood; 1997. p. 19–46.
Shiloh S. Illness representations, self-regulation, and genetic counseling: a theoretical review. J Genet Couns. 2006;15:325–37.
Cameron L, Leventhal EA. H L: Symptom representations and affect as determinants of care seeking in a community-dwelling, adult sample population. Health Psychol. 1993;12:171–9.
Patrick-Miller L, Kelly K, Toppmeyer D, Leventhal H, Much J, Baron J, Schwalb M: Breast cancer screening behaviors and perceived control in individuals interested in testing for BRCA1/2 mutations [Abstract]. In: American Society of Clinical Oncology: 2001;2001.
Weinman J, Petrie K, Sharpe N. Causal attributions in patients and spouses following first-time myocardial infarction and subsequent lifestyle changes. Br J Health Psychol. 2000;5:263–73.
Zimmerman RS, Safer MA, Leventhal H, Baumann LJ. The effects of health information in a worksite hypertension screening program. Health Educ Q. 1986;13:261–80.
Kelly K, Leventhal H, Andrykowski M, Toppmeyer D, Much J, Dermody J, Marvin M, Baran J, Schwalb M. Using the common sense model to understand perceived cancer risk in individuals testing for BRCA1/2 mutations. Psychooncology. 2005;14(1):34–48.
Park D. Self-regulation and control of rheumatic disorders. New York: John Wiley & sons; 1994.
Kelly KM, Ferketich AK, Sturm AC, Porter K, Sweet K, Kemp K, Schwirian P, Westman JA. Cancer risk and risk communication in urban, lower-income neighborhoods. Prev Med. 2009;48(4):392–6.
Shiloh S, Drori E, Orr-Urtreger A, Friedman E. Being 'at-risk' for developing cancer: cognitive representations and psychological outcomes. J Behav Med. 2009;32(2):197–208.
Patrick-Miller L, Bradbury AR, Terry MB. Controversies in communication of genetic screening results for cancer: a report from the American Society of Preventive Oncology’s Screening Special Interest Group (ASPO’s 33rd Annual Meeting, March 8 to 10, 2009, Tampa, Florida). Cancer Epidemiol Biomarkers Prev. 2010;19(2):624–7.
Hamilton JG, Lobel M, Moyer A. Emotional distress following genetic testing for hereditary breast and ovarian cancer: a meta-analytic review. Health Psychol. 2009;28(4):510–8.
O’Neill SC, Rini C, Goldsmith RE, Valdimarsdottir H, Cohen LH, Schwartz MD. Distress among women receiving uninformative BRCA1/2 results: 12-month outcomes. Psychooncology. 2009;18(10):1088–96.
Bradbury AR, Patrick-Miller L, Fetzer D, Egleston B, Cummings SA, Forman A, Bealin L, Peterson C, Corbman M, O’Connell J, et al. Genetic counselor opinions of, and experiences with telephone communication of BRCA1/2 test results. Clin Genet. 2011;79(2):125–31.
Lynch HT, Snyder C, Lynch JF, Karatoprakli P, Trowonou A, Metcalfe K, Narod SA, Gong G. Patient responses to the disclosure of BRCA mutation tests in hereditary breast-ovarian cancer families. Cancer Genet Cytogenet. 2006;165(2):91–7.
Schlich-Bakker KJ, ten Kroode HF, Ausems MG. A literature review of the psychological impact of genetic testing on breast cancer patients. Patient Educ Couns. 2006;62(1):13–20.
Halbert C, Kessler L, Collier A, Paul Wileyto E, Brewster K, Weathers B. Psychological functioning in African American women at an increased risk of hereditary breast and ovarian cancer. Clin Genet. 2005;68(3):222–7.
Kinney AY, Bloor LE, Mandal D, Simonsen SE, Baty BJ, Holubkov R, Seggar K, Neuhausen S, Smith K. The impact of receiving genetic test results on general and cancer-specific psychologic distress among members of an African-American kindred with a BRCA1 mutation. Cancer. 2005;104(11):2508–16.
Kinney AY, Simonsen SE, Baty BJ, Mandal D, Neuhausen SL, Seggar K, Holubkov R, Bloor L, Smith K. Risk reduction behaviors and provider communication following genetic counseling and BRCA1 mutation testing in an African American kindred. J Genet Couns. 2006;15(4):293–305.
Kaphingst KA, Blanchard M, Milam L, Pokharel M, Elrick A, Goodman MS. Relationships between health literacy and genomics-related knowledge, self-efficacy, perceived importance, and communication in a medically underserved population. J Health Commun. 2016;21(Suppl 1):58–68.
Oldach BR, Katz ML. Health literacy and cancer screening: a systematic review. Patient Educ Couns. 2014;94(2):149–57.
Lea DH, Kaphingst KA, Bowen D, Lipkus I, Hadley DW. Communicating genetic and genomic information: health literacy and numeracy considerations. Public Health Genomics. 2011;14(4–5):279–89.
Jimbo M, Sen A, Plegue MA, Hawley ST, Kelly-Blake K, Rapai M, Zhang M, Zhang Y. Ruffin MTt: correlates of patient intent and preference on colorectal cancer screening. Am J Prev Med. 2017;52(4):443–50.
Hendy J, Lyons E, Breakwell GM. Genetic testing and the relationship between specific and general self-efficacy. Br J Health Psychol. 2006;11(Pt 2):221–33.
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4:50.
Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. In. Washington D.C.: National Academies Press; 2001.
Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217–26.
Stevenson L, Ball S, Haverhals LM, Aron DC, Lowery J. Evaluation of a national telemedicine initiative in the Veterans Health Administration: Factors associated with successful implementation. J Telemed Telecare. 2018;24(3):168–78.
Kirk MA, Kelley C, Yankey N, Birken SA, Abadie B, Damschroder L. A systematic review of the use of the consolidated framework for implementation research. Implement Sci. 2016;11:72.
Damschroder LJ, Lowery JC. Evaluation of a large-scale weight management program using the consolidated framework for implementation research (CFIR). Implement Sci. 2013;8:51.
Underhill-Blazey M, Stopfer J, Chittenden A, Nayak MM, Lansang K, Lederman R, Garber J, Gundersen DA. Development and testing of the KnowGene scale to assess general cancer genetic knowledge related to multigene panel testing. Patient Educ Couns. 2019;102(8):1558–64.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–70.
Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale an updated literature review. J Psychosomatic Res. 2002;52(2):69–77.
Geirdal AO, Reichelt JG, Dahl AA, Heimdal K, Maehle L, Stormorken A, Moller P. Psychological distress in women at risk of hereditary breast/ovarian or HNPCC cancers in the absence of demonstrated mutations. Fam Cancer. 2005;4(2):121–6.
Spiegel TN, Esplen MJ, Hill KA, Wong J, Causer PA, Warner E. Psychological impact of recall on women with BRCA mutations undergoing MRI surveillance. Breast. 2011;20(5):424–30.
Horowitz M, Wilner N, Alvarez W. Impact of event scale: a measure of subjective stress. Psychosom Med. 1979;41(3):209–18.
Sundin EC, Horowitz MJ. Impact of event Scale: psychometric properties. Bri J Psychiatry. 2002;180:205–9.
Bradbury AR, Patrick-Miller LJ, Egleston BL, DiGiovanni L, Brower J, Harris D, Stevens EM, Maxwell KN, Kulkarni A, Chavez T, et al. Patient feedback and early outcome data with a novel tiered-binned model for multiplex breast cancer susceptibility testing. Genet Med. 2016;18(1):25–33.
Patrick-Miller L, Egleston BL, Daly M, Stevens E, Fetzer D, Forman A, Bealin L, Rybak C, Peterson C, Corbman M, et al. Implementation and outcomes of telephone disclosure of clinical BRCA1/2 test results. Patient Educ Couns. 2013;93(3):413–9.
Bradbury AR, Patrick-Miller L, Egleston BL, Hall MJ, Domchek SM, Daly MB, Ganschow P, Grana G, Olopade OI, Fetzer D, et al. Randomized non-inferiority trial of telephone versus in-person disclosure of germline cancer genetic test results. J Natl Cancer Inst Monographs. 2018;110:985.
Vickberg SM, Bovbjerg DH, DuHamel KN, Currie V, Redd WH. Intrusive thoughts and psychological distress among breast cancer survivors: global meaning as a possible protective factor. Behav Med. 2000;25(4):152–60.
Croyle RT, Smith KR, Botkin JR, Baty B, Nash J. Psychological responses to BRCA1 mutation testing: preliminary findings. Health Psychol. 1997;16(1):63–72.
Lloyd S, Watson M, Waites B, Meyer L, Eeles R, Ebbs S, Tylee A. Familial breast cancer: a controlled study of risk perception, psychological morbidity and health beliefs in women attending for genetic counselling. Br J Cancer. 1996;74(3):482–7.
Meiser B, Butow PN, Barratt AL, Schnieden V, Gattas M, Kirk J, Gaff C, Suthers G, Tucker K. Long-term outcomes of genetic counseling in women at increased risk of developing hereditary breast cancer. Patient Educ Couns. 2001;44(3):215–25.
Dick PT, Filler R, Pavan A. Participant satisfaction and comfort with multidisciplinary pediatric telemedicine consultations. J Pediatr Surg. 1999;34(1):137–41.
Cella D, Hughes C, Peterman A, Chang CH, Peshkin BN, Schwartz MD, Wenzel L, Lemke A, Marcus AC, Lerman C. A brief assessment of concerns associated with genetic testing for cancer: the Multidimensional Impact of Cancer Risk Assessment (MICRA) questionnaire. Health Psychol. 2002;21(6):564–72.
Gray SW, Martins Y, Feuerman LZ, Bernhardt BA, Biesecker BB, Christensen KD, Joffe S, Rini C, Veenstra D, McGuire AL, et al. Social and behavioral research in genomic sequencing: approaches from the clinical sequencing exploratory research consortium outcomes and measures working group. Genet Med. 2014;16(10):727–35.
Brehaut JC, O’Connor AM, Wood TJ, Hack TF, Siminoff L, Gordon E, Feldman-Stewart D. Validation of a decision regret scale. Med Decis Making. 2003;23(4):281–92.
Chew LD, Griffin JM, Partin MR, Noorbaloochi S, Grill JP, Snyder A, Bradley KA, Nugent SM, Baines AD, Vanryn M. Validation of screening questions for limited health literacy in a large VA outpatient population. J Gen Intern Med. 2008;23(5):561–6.
Blake KD, Portnoy DB, Kaufman AR, Lin CJ, Lo SC, Backlund E, Cantor D, Hicks L, Lin A, Caporaso A, et al. Rationale, procedures, and response rates for the 2015 administration of NCI’s Health Information National Trends Survey: HINTS-FDA 2015. J Health Commun. 2016;21(12):1269–75.
Gruber-Baldini AL, Velozo C, Romero S, Shulman LM. Validation of the PROMIS((R)) measures of self-efficacy for managing chronic conditions. Qual Life Res. 2017;26(7):1915–24.
Prawitz A GET, Sorhaindo B, O’Neill B, Kim J, Drentea P. Incharge Financial Distress/Financial Well-Being Scale: Development, Administration, and Score Interpretation. J Financial Counsel Plan. 2006;17(1):34–50.
Krull KR, McDonald A, Goodman P, Vukadinovich C, Ford J, Leisenring WM, Chow EJ, Robison LL, Armstrong GT. Impact of COVID-19 pandemic on a large cohort of adult survivors of childhood cancer. Pediatr Blood Cancer. 2021;68(11):e29324.
Francis JJ, Johnston M, Robertson C, Glidewell L, Entwistle V, Eccles MP, Grimshaw JM. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–45.
Raghunathan TLJ, Van Hoewyk J, Solenberger P. A multivariate technique for multiply imputing missing values using a sequence of regression models. Surv Methodol. 2001;27(1):85–95.
Harrell F. Regression Modeling Strategies. New York, NY: Springer; 2001.
Sanders GD, Neumann PJ, Basu A, Brock DW, Feeny D, Krahn M, Kuntz KM, Meltzer DO, Owens DK, Prosser LA, et al. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: second panel on cost-effectiveness in health and medicine. JAMA. 2016;316(10):1093–103.
Drummond M, Sculpher M. Common methodological flaws in economic evaluations. Med Care. 2005;43(7 Suppl):5–14.
Forman J, Damschroder LJ. Qualitative content analysis. In: Jacoby L, Siminoff L, editors. Empirical research for bioethics: a primer, Volume 11. Oxford, U.K: Elsevier Publishing; 2008. p. 39–62.
Hill CE, Thompson BJ, Williams EN. A guide to conducting consensual qualitative research. Couns Psychol. 1997;25(4):517–72.
Hill CE, Knox S, Thompson BJ, Williams EN, Hess S, Ladany N. Consensual qualitative research: an update. J Couns Psychol. 2005;52:196–205.
Cresswell JW. A concise introduction to mixed methods research. Los Angeles: Sage Publishing; 2015.
Acknowledgements
We would like to thank our Investigators and Event Monitoring Committee for their expert guidance and recommendations on the development and progression of the study.
Protocol version
Approval date: May 12, 2021.
Protocol version: June 26, 2023.
Authors: TH, AB, GA, KK, BE, LF, EE, KO, EW, CC, MW, SB, SH, BM, MA, DF, DO, AB, RM, and PT.
DMC
A Data and Event Monitoring Committee (DEMC) is required for this study. The project is considered to have “minimal risk” to participants. The IRB and DEMC will be notified of any unanticipated events.
Data sharing
The Childhood Cancer Survivor Study is a US National Cancer Institute funded resource (U24 CA55727) to promote and facilitate research among long-term survivors of cancer diagnosed during childhood and adolescence. CCSS data are publicly available on dbGaP at https://www.ncbi.nlm.nih.gov/gap/ through its accession number phs001327.v2.p1. and on the St Jude Survivorship Portal within the St. Jude Cloud at https://survivorship.stjude.cloud/. In addition, utilization of the CCSS data that leverages the expertise of CCSS Statistical and Survivorship research and resources will be considered on a case-by case basis. For this utilization, a research Application Of Intent followed by an Analysis Concept Proposal must be submitted for evaluation by the CCSS Publications Committee. Users interested in utilizing this resource are encouraged to visit http://ccss.stjude.org. Full analytical data sets associated with CCSS publications since January of 2023 are also available on the St. Jude Survivorship Portal at https://viz.stjude.cloud/community/cancer-survivorship-community~4/publications.
Funding
This work is supported through the National Cancer Institute [National Cancer Institute (R01CA237369, MPI: Henderson, Bradbury)], and (CA55727, G.T. Armstrong, Principal Investigator). Support to St. Jude Children’s Research Hospital also provided by the Cancer Center Support (CORE) grant (CA21765, C. Roberts, Principal Investigator) and the American Lebanese-Syrian Associated Charities (ALSAC).
Author information
Authors and Affiliations
Contributions
TH, BE, LF, EE, KO, KK, GA, AB conceived the study design. TH, AB, GA, KK, BE, LF, EE, KO, EW, CC, MW, SB, SH, BM, MA, DO, AB, HG, and RM developed the study methods and protocol. AM, CV, SA, DR developed study design and methods. TH, AB, MA, BE, GA, and EE drafted and edited the manuscript. All authors reviewed and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol for the study has been reviewed and approved by the University of Chicago Institutional Review Board (CIRB21-0176), St. Jude Children’s Research Hospital Institutional Review Board (IRB21-0803), and the University of Pennsylvania Institutional Review Board (IRB-848501). The University of Pennsylvania is the IRB of record. Participants electronically sign an informed consent form that is available on the CCSS Long-Term Follow Up study website. Project PIs, research staff, and staff at the CCSS Coordinating Center are available to participants for questions and concerns. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Henderson, T.O., Allen, M.A., Mim, R. et al. The ENGAGE study: a 3-arm randomized hybrid type 1 effectiveness and implementation study of an in-home, collaborative PCP model of remote telegenetic services to increase uptake of cancer genetic services in childhood cancer survivors. BMC Health Serv Res 24, 253 (2024). https://doi.org/10.1186/s12913-024-10586-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-024-10586-z