
Abstract
Background
The prevalence of multi-morbidity is increasing globally. Integrated models of care present a potential intervention to improve patient and health system outcomes. However, the intervention components and concepts within different models of care vary widely and their effectiveness remains unclear. We aimed to describe and map the definitions, characteristics, components, and reported effects of integrated models of care in systematic reviews (SRs).
Methods
We conducted a scoping review of SRs according to pre-specified methods (PROSPERO 2019 CRD42019119265). Eligible SRs assessed integrated models of care at primary health care level for adults and children with multi-morbidity. We searched in PubMed (MEDLINE), Embase, Cochrane Database of Systematic Reviews, Epistemonikos, and Health Systems Evidence up to 3 May 2022. Two authors independently assessed eligibility of SRs and extracted data. We identified and described common components of integrated care across SRs. We extracted findings of the SRs as presented in the conclusions and reported on these verbatim.
Results
We included 22 SRs, examining data from randomised controlled trials and observational studies conducted across the world. Definitions and descriptions of models of integrated care varied considerably. However, across SRs, we identified and described six common components of integrated care: (1) chronic conditions addressed, (2) where services were provided, (3) the type of services provided, (4) healthcare professionals involved in care, (5) coordination and organisation of care and (6) patient involvement in care. We observed differences in the components of integrated care according to the income setting of the included studies. Some SRs reported that integrated care was beneficial for health and process outcomes, while others found no difference in effect when comparing integrated care to other models of care.
Conclusions
Integrated models of care were heterogeneous within and across SRs. Information that allows the identification of effective components of integrated care was lacking. Detailed, standardised and transparent reporting of the intervention components and their effectiveness on health and process outcomes is needed.
Similar content being viewed by others

Background
Globally, the prevalence and burden of multi-morbidity, the existence of two or more chronic health conditions in one individual [1], is increasing [2]. Multi-morbidity refers to people with multiple non-communicable diseases (NCDs) such as cardiovascular diseases, cancers, chronic respiratory diseases and diabetes, [3] mental health conditions and communicable diseases. Although NCDs are a global problem, low-and middle-income countries (LMICs) are hit the hardest, where more than 75% of global deaths due to NCDs occur [3]. In LMICs, the burden of multi-morbidity may be exacerbated by emerging infections such as COVID-19 and the double burden of NCDs and chronic communicable diseases, such as Human immunodeficiency virus (HIV) infection and tuberculosis (TB). The prevalence of multi-morbidity in LMICs ranges from 13 to 87% and is expected to increase over time if there are no drastic measures for preventing and controlling chronic diseases [4, 5]. Life expectancy of people living in LMICs has improved over the past two decades and a considerable number of people are reaching middle and older ages when NCDs such as cardiovascular diseases, type 2 diabetes mellitus, and cancers, among others are increasing. Furthermore, people living in LMICs are also experiencing a change in lifestyle and environmental exposures which contribute to NCDs.
Management of and care for patients with multi-morbidity is often fragmented, as specialised care is needed to address each individual condition. This often involves both primary and multiple secondary care specialists who may not be communicating and coordinating care effectively with resultant impact on health outcomes and impact on households [6]. To respond to the growing burden caused by multi-morbidity and to meet international health targets, models of care that enhance the continuum of care, adherence to care, reduce number of health visits and multidisciplinary management should be prioritised [7].
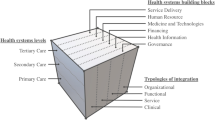
Integrated approaches or models of care are described as providing patients with holistic options centred on health needs of people and communities and thereby enhancing community self-reliance [8,9,10,11,12]. Various approaches, models of care and frameworks, aiming to improve health outcomes and strengthen health systems, have been described [13]. As an example, the WHO framework on ‘integrated, people-centred health services’ [14] and the ‘conceptual and analytical framework on integrated care for health programs’ developed by Atun et al. 2010 [8] provide an analytical approach that helps researchers to apply the framework when conducting evaluative and formative studies on ‘integration’ in order to generate useful evidence to inform policy and practice in different health setting [8, 12].
Integrated care has been widely promoted to help provide services for people with multi-morbidity assuming that they achieve more appropriate, better-quality as well as less resource-intensive and therefore more cost-effective care. However, many evidence gaps related to the prevention and management of multi-morbidity remain [15]. Many different definitions and models of integrated care exist, and it is often difficult to unpack the components and mechanisms of action of these complex interventions [16]. Furthermore, it is still unclear which components and characteristics of integrated care render it more effective than other models of care.
Initially, we set out to conduct an overview of systematic reviews on the effects of integrated models of care. However, during the process of identifying studies for inclusion, the author team realised that the complexity and heterogenous nature of integrated models of care would make it difficult to compare effects across SRs. We decided that it was important to understand the various ways integrated care has been defined and reported in SRs as a first step to then inform further work on effects. We therefore conducted a scoping review, which is better suited for this objective [17], and aimed to describe and map the definitions, characteristics, components and effects of integrated models of care as reported in SRs.
Methods
We developed a protocol for an overview of SRs (PROSPERO: CRD42019119265), which we adapted for this scoping review. We followed the pre-specified methods linked to eligibility criteria, identification of reviews including the search strategy, and selection of reviews, but adapted the methods linked to data extraction and analysis to fit with the objectives of this scoping review. We used the PRISMA Extension for Scoping Reviews to guide reporting [18].
Eligibility criteria
We included SRs on integrated models of care at either primary health care (PHC) level only or both PHC and specialized health settings for adults and children with multi-morbidity. We focused on PHC, as effective management of chronic conditions requires a shift from curative to preventative, and from inpatient to outpatient care [14]. We were therefore not interested in treatment of acute complications in a hospital setting, but in long-term management of chronic conditions. Multi-morbidity was defined as having two or more chronic conditions. We considered the following NCDs and communicable diseases to be chronic conditions: Diabetes mellitus, cardiovascular diseases, cancers, chronic respiratory diseases, mental diseases (e.g. depression), musculoskeletal disorders (e.g. Arthritis), chronic kidney disease, HIV, and TB. The key characteristics of SRs were defined as having a clearly stated set of objectives with an explicit and reproducible methodology; a systematic search that attempts to identify all studies that would meet the eligibility criteria; an assessment of the validity of the findings of the included studies (e.g., assessment of risk of bias and confidence in cumulative estimates); and systematic presentation, and synthesis of the characteristics and findings of the included studies [19]. We therefore considered a review to be a SR if it included (1) pre-specified objectives and eligibility criteria of studies; (2) a search of at least two electronic databases to identify studies; and (3) assessment of risk of bias of included studies.
We included interventions that comprised fully integrated care or partially integrated care. Full integration of care referred to models where patients (primarily treated for one condition) receive the full package of care (prevention, diagnosis and treatment) for another condition at the same point of care by one or more health care professionals. Partial integration of care was defined as models where patients treated for one condition receive part of the package of care (either prevention, diagnosis, or treatment) for another condition (Fig. 1). As a minimum, patients had to receive preventative measures such as health education or be screened (and referred if they received a positive test result) for another specific condition for the intervention to be classified as integrated care. Studies that did not adequately define their intervention were included if it was clear that the intervention aimed to integrate care for two or more chronic conditions.

Logic model of integrated care [20]
Information sources and search
We conducted a comprehensive search of PubMed (MEDLINE), Embase, Cochrane Database of Systematic Reviews, Epistemonikos, and Health Systems Evidence up to 3 May 2022. Keywords included ‘Chronic diseases’, ‘Integrated health care’, ‘Systematic review’ and their synonyms. We did not apply restrictions based on language or date of publication. The full search strategies for all databases are provided in Additional file 1.
Selection of systematic reviews
A pair of authors (AR, IT, JLZN, JUN, JBN) independently screened titles and abstracts in duplicate, using Covidence software and obtained full texts of potentially relevant articles. A pair of authors (AR, IT, JLZN, JUN, JBN) independently screened full texts according to the pre-specified eligibility criteria and provided reasons for excluding studies. Discrepancies were resolved through discussion with another member of the author team.
Data extraction and analysis
A pair of authors (AR, JUN, IT, JBN, AA, JLZN) independently extracted data using a pre-piloted data extraction form set up in Covidence. We extracted descriptive characteristics of included SRs, comprising objectives of the SR; characteristics of included participants, interventions and comparisons; how integrated care was defined; key features of integrated care; the outcomes addressed; eligible study designs and actual number and type of studies included; country and setting where included studies were conducted; databases searched and the date of the last search. Discrepancies were resolved through discussions with the author team.
We summarised descriptive characteristics of included SRs narratively. We mapped available evidence in table format, focussing on the characteristics of various models of integrated care included in the SRs. We extracted information on main components and sub-components of models of integrated care across SRs and tabulated these to compare models. We identified common components of integrated models of care through iterative discussions within the author team. We extracted findings of the SRs as presented in the conclusions and reported on these verbatim.
Results
Results of search and description of included studies
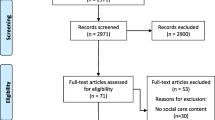
After removal of duplicates, we screened titles and abstracts of 10,040 records and assessed eligibility of 72 full texts. We included 22 SRs and excluded 50 reviews with reasons (Additional file 2). The PRISMA flow-diagram is depicted in Fig. 2.

PRISMA Flow diagram of included studies
The included SRs [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42] were published between 2011 and 2022, with the dates of the last search ranging from September 2010 to October 2021 (Table 1). Primary studies included in the SRs were exclusively conducted in high income countries (HICs) in twelve SRs [21, 25,26,27,28, 30,31,32,33, 37, 39, 42] and exclusively in LMICs in six SRs [23, 29, 34, 36, 40, 41]. Four SRs included studies from LMICs and HICs [22, 24, 35, 38] (Fig. 3). Overall, the included SRs examined data from randomised controlled trials (RCTs), controlled before-after studies, non-randomised intervention studies, interrupted time series, cohort studies, case series, cross-sectional studies, retrospective record reviews, mixed-methods studies, quasi-experimental studies, and qualitative studies. Data was also derived from program descriptions in one SR. Ten SRs included RCTs only [21, 26, 28, 30,31,32,33, 35, 37, 42].
The included SRs (Table 1) looked at a wide array of medical conditions that were addressed with collaborative care or integrated care approaches. These included HIV, TB, NCDs, diabetes, hypertension, cardiovascular disease, cancer, depression and other mental health conditions. Some reviews reported that they considered multiple conditions or patients with multi-morbidity.

Heatmap of primary studies included in the SRs
Included SRs provided various definitions for integrated care, ranging from very simple to very comprehensive definitions (Additional file 3). The different models for delivering care and offering health services were described as integrated care [22,23,24, 27, 29, 30, 34, 36, 40, 41] or collaborative care [21, 26, 28, 31, 32, 39], with a few SRs reporting the models of care as comprehensive care [25, 33], a multi-professional approach to patient care [37], interprofessional collaboration practice [38] and patient-centered medical home [35].
Characteristics and components of models of integrated care
Models of care evaluated in primary studies were heterogenous within and across SRs. We identified six common components across included SRs, related to (1) chronic conditions addressed, (2) where services were provided (3) types of services provided (4) healthcare professionals involved in care (5) coordination and organisation of care and (6) patient involvement in care. Within each of these components, we identified various sub-components reported across included SRs (Table 2). Additional file 4 provides additional details for each included review.
Specific chronic conditions addressed in systematic reviews included HIV, TB, diabetes mellitus, hypertension, cardiovascular disease, cancer and mental health (mostly depression). Some reviews only referred to NCDs or multiple conditions collectively.
(Where) Services were provided at a single facility, multiple facilities, and at home or in the community. Where services were provided at a single facility, these were described as ‘within clinic’ or as ‘co-location’. Services offered within the same clinic were referred to as a ‘one-stop-shop’, where services related to all conditions were provided at the same time, by the same healthcare professional. In contrast, ‘co-location’ referred to services provided in different clinics, by different healthcare professionals, but at the same facility.
Types of services provided included health education and counselling, screening, diagnosis, linkage to care, treatment and management of conditions, referral, appointment reminders and telephonic follow-up. Healthcare professionals involved in care included primary care nurses, general physicians, specialists, other healthcare professionals such as physiotherapists, psychologists or pharmacists, a multi-disciplinary team, peers, or a combination of these.
We identified various sub-components for coordination and organisation of care. The sub-component coordination of care described internal and external referral systems, scheduled follow-ups, and continuity of care. Interprofessional communication comprised regular team meetings, case discussions, enhanced communication, joint consultations, and shared medical records. Case management referred to appointment of case managers. Clinical management support comprised clinical practice guidelines, algorithms and decision-aids. Structured treatment plans referred to individual treatment plans or a stepped care approach. Staff support comprised training of healthcare professionals, supervision, additional staff and expanded prescribing provisions for nurses. Facility reorganisation referred to the physical space at clinics and how this was reorganised to accommodate integrated care.
Patient involvement in care was described as patient engagement and self-management support. Patient engagement referred to engaging with patients and considering their views in decision-making and treatment plans. Self-management support included problem-solving, goal setting, self-monitoring and self-care education.
Although components and sub-components differed considerably between and within SRs, we observed some similarities related to where studies included in the SRs were conducted: in LMICs, in LMICs and HICs, or in HIC only. Reviews in each of these categories reported similar subcomponents, whereas we observed differences in the reported sub-components across these categories (Fig. 4).

Overview of components and sub-components of integrated models of care
In the six SRs that only included studies from LMICs [23, 29, 34, 36, 40, 41], integrated models of care were mainly described in terms of the conditions addressed, where services were provided and the types of services that were offered. All but one SR included studies that integrated services for HIV with other conditions, and four of the six studies included studies that integrated services for TB. Three of the SRs in this category also reported that services were offered in a one-stop-shop, a term that was not used for studies conducted in HICs. Services offered mostly included screening and treatment of the condition. SRs in this category also reported on linkage to care, a service that was not reported in SRs that included studies from HICs. Furthermore, only one SR reported that specialists were part of the team providing care, while coordination of care was only reported in two SRs. Patient involvement in care was not reported in any of the SRs that only included studies from LMICs.
The four SRs that included studies from LMICs and HICs generally reported on few subcomponents [22, 24, 35, 38]. All reviews reported on how care was coordinated and interprofessional communication, as well as patient engagement in care.
In the twelve SRs that only included studies from HICs [21, 25,26,27,28, 30,31,32,33, 37, 39, 42], integrated models of care were generally described in terms of who provided care, how care was coordinated and patient involvement in care. These SRs mainly addressed multiple conditions including, cancer, diabetes, hypertension, mental health and NCDs. Services reported for this category related mostly to health education and counselling and treatment and management of the condition. A wide range of healthcare professionals provided care, and most SRs reported that a multi-disciplinary team was involved in care. SRs in this category described a wide range of sub-components related to how care was coordinated and organised. Indeed, this was the focus of most SRs included in this category. Furthermore, all but two reviews reported on patient involvement in care, and all but three reviews described subcomponents related to self-management.
Effectiveness of integrated models of care
The findings on the effectiveness of integrated models of care, as reported in the conclusions of included SRs, are summarised in Additional file 5. Reported conclusions on the effectiveness of integrated models of care were heterogenous for health and process outcomes.
Of the SRs that included studies from LMICs, four reported findings on health outcomes. One SR [34] found that integrated care for HIV and other conditions had health benefits for HIV and other conditions. The other three SRs [36, 40, 41] did not find that integrated care improved health outcomes. Three SRs reported findings on process outcomes and reported an increase in the uptake of services for integrated models of care [23, 29, 34].
Two SRs that included studies from both LMICs and HICs, reported improved health outcomes for the patient-centered medical home [35] and interprofessional collaborative practice model [38]. The other two SRs in this category reported that integrated care had positive effects on process outcomes [22, 24].
All SRs that included studies from HICs reported findings on health outcomes. Eight SRs found that collaborative or coordinated care had significant benefits for depression [21, 26,27,28, 30, 32, 33, 37]. The other four SRs reported that although there might be small improvements in health outcomes [31], the current evidence was insufficient [25] and inconsistent [39], and uncertainties about the effectiveness of interventions for peoples with multi-morbidity remained [42]. Three SRs reported findings on access to health services. One SR reported that integrated models of care may make little or no difference to health services use [30], one SR reported that the intervention significantly increased the use of mental health services [27], and another reported that there was no evidence that comprehensive care reduced the number of primary care visits or costs [25].
Discussion
We conducted a scoping review to describe the characteristics, components and reported effects of models of integrated care included in systematic reviews on the effectiveness of integrated care for people with multiple chronic conditions. We included 22 SRs investigating various forms of integrated care for a wide range of conditions. Definitions of integrated care varied between SRs. Some referred to integrated care as integration of services, while others only used the terms collaborative or coordinated care. As these models all aimed to treat patients with more than one chronic condition in a more or less integrated manner, we decided within our team, that we would include these under the umbrella term of integrated care.
Integrated models of care were complex and heterogenous, both within and across included SRs, and were poorly reported. Only two SRs used the Template for Intervention Description and Replication (TIDieR) checklist [43] to describe included interventions. This presented a challenge in synthesising and comparing models of care in a meaningful way. However, we identified some similarities in the components of integrated care and summarised these in terms of chronic conditions addressed, where services were provided, the type of services provided, healthcare professionals involved in care, coordination and organisation of care and patient involvement. Furthermore, we identified sub-components within each of the components and described the models of care of included SRs accordingly. Individual SRs did not report on all components and sub-components varied considerably between SRs.
We observed a difference in the reported components and sub-components of interventions based on the income setting of included studies. The different approaches to integrated care in the various income settings might be attributed to the differences in the disease profile of the population and the aims of the intervention. While the main aim in LMICs has been to increase access to care, improve uptake of priority services and increasing efficiency, HICs have focused on shifting care from in-patient care to primary care, and improving quality of care [44].
Our findings regarding heterogeneity in the definition, complexity and context-specific nature of integrated models of care resonate with previous findings [13, 16]. The WHO framework on integrated, people-centered health services [14] recognises the complexity of integrated models of care and proposes five interdependent strategies that should be adopted in a context-sensitive manner, rather than used as a static framework. These are (1) empowering and engaging people and communities, (2) strengthening governance and accountability, (3) reorienting the model of care, (4) coordinating services within and across sectors, and (5) creating an enabling environment. The components that we identified describe integrated care at the level of service delivery and fit under strategy 1 (involvement of patients in care), strategy 3 (conditions, where services were provided, types of services provided, health professionals involved in care) and strategy 4 (coordination and organisation of care).
A recent scoping review that summarised the characteristics of integrated care for NCDs and mental health in LMICs [45] also found that models of care were complex and heterogenous. Authors described the models of care according to pre-specified dimensions, of which the following mirror components that we identified: the condition, type of service, health care provider and health system level (where care was provided).
It is important to have a comprehensive understanding of the components of models of care when planning, implementing and evaluating integrated care interventions, and to report the approaches in a transparent way. Unique aspects linked to the management of specific diseases makes it difficult to synthesise evidence on a broad range of conditions.
We did not aim to evaluate the effectiveness of integrated models of care in this scoping review but extracted a verbatim summary of conclusions of included SRs, which provide an indication of the potential benefit and direction of effects of integrated care and its individual components, both in terms of health and process outcomes. However, this needs to be interpreted with caution, since we did not assess the quality and did not evaluate findings of included SRs. Other studies have found that provision of integrated care has potential benefits on health systems, notable —addressing poor care coordination which is often the main problem cited by patients with multi-morbidity when describing their experiences of health and social care services [46]. Additionally, the literature has suggested that integrated care has a positive effect on the quality [8, 47] and efficiency [24, 48, 49] of services. However, there is still uncertainty about which model of integrated care is most effective, for which conditions, and how these models should be implemented alongside persistent questions over whether the aims of integration are ultimately achievable in any meaningful way [50].
Strengths and limitations
We followed a rigorous and systematic process to conduct our scoping review. We pre-specified our eligibility criteria and conducted a comprehensive search to identify the available evidence. To minimise bias, two authors independently selected studies and extracted data.
We set out to conduct an overview of SRs, focussing on the effectiveness of integration of care. However, during study selection and data extraction, we realised that included interventions were very complex and heterogenous, which made it difficult to compare models of care across SR. Furthermore, we found that we needed a better understanding of the available models of care before evaluating their effectiveness. We therefore revised our strategy to conduct a scoping review, focussing on the characteristics of various models of integrated care as a first step. Although we provide a summary of verbatim conclusions from included SRs, this needs to be interpreted with caution, as we did not assess the quality of included SRs.
Even though our search was comprehensive, we acknowledge that including a wider range of studies and not restricting it to SRs would have been useful to get a good understanding of integrated models of care. Our findings are based on how authors of included SRs reported the interventions and we did not review primary studies. Poor reporting of primary studies in SRs was limiting.
Our logic model describing integrated models of care (Fig. 1) depicts our conceptualisation of fully integrated models of care and partially integrated models of care, which mainly refers to the services that are being offered, ideally in a one-stop-shop setting. However, we found that it was difficult to categorise models of care using these categories, mainly because services offered as part of the interventions were poorly described. If reported, most SRs only described services offered for one condition, which we assumed to be the ‘add-on’ condition. The other components of integrated care that we described in our scoping review are not depicted in the logic model. Our model might be too simplistic to describe the range of interventions considered as part of integrated care in various contexts and health systems. An expansion of this model is therefore warranted.
Conclusion
Integrated models of care were heterogenous within and across included SRs. Although there was a lack of a common definition of integrated care, there were some common components of integrated care reported across included SRs. We observed a difference in the conceptualisation and description of integrated care according to the income setting of the included studies, and information that allows the identification of effective components of integrated care was lacking. There is a need to develop a structured framework to compare the effectiveness of integrated models of care that can be used in future primary research studies and evidence syntheses. Detailed, standardised and transparent reporting of the intervention components and their effectiveness on patient-relevant and health system outcomes is needed. We encourage authors of primary and secondary research to use the TIDieR checklist when reporting on integrated models of care.
Data Availability
All data generated or analysed during this study are included in this published article and its supplementary information files.
Abbreviations
- BMBF:
-
German Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung)
- CEBHA+:
-
Collaboration for Evidence-based Healthcare and Public Health in Africa
- HICs:
-
High income countries
- HIV:
-
Human immunodeficiency virus
- LMICs:
-
Low - Middle- Income Countries
- NCDs:
-
Non-communicable diseases
- PHC:
-
Primary Healthcare
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PROSPERO:
-
Prospective Register of Systematic Reviews
- RCTs:
-
Randomised controlled trials
- SRs:
-
Systematic Reviews
- TB:
-
Tuberculosis
- TIDieR:
-
Template for Intervention Description and Replication
- WHO:
-
World Health Organisation
References
Bernell S, Howard SW. Use your words carefully: what is a chronic disease? Front Public Health. 2016;4:159.
Nguyen H, Manolova G, Daskalopoulou C, Vitoratou S, Prince M, Prina AM. Prevalence of multimorbidity in community settings: a systematic review and meta-analysis of observational studies. J Comorb. 2019;9:2235042X19870934.
World Health Organization. Noncommunicable diseases 2021 [Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
Asogwa OA, Boateng D, Marza-Florensa A, Peters S, Levitt N, van Olmen J, Klipstein-Grobusch K. Multimorbidity of non-communicable diseases in low-income and middle-income countries: a systematic review and meta-analysis. BMJ Open. 2022;12(1):e049133.
Kaluvu L, Asogwa OA, Marza-Florensa A, Kyobutungi C, Levitt NS, Boateng D, Klipstein-Grobusch K. Multimorbidity of communicable and non-communicable diseases in low- and middle-income countries: a systematic review. J Multimorb Comorb. 2022;12:26335565221112593.
Uwimana J, Jackson D, Hausler H, Zarowsky C. Health system barriers to implementation of collaborative TB and HIV activities including prevention of mother to child transmission in South Africa. Trop Med Int Health. 2012;17(5):658–65.
Hurst JR, Dickhaus J, Maulik PK, Miranda JJ, Pastakia SD, Soriano JB, Siddharthan T, Vedanthan R, Agarwal G, Aguilar-Salinas CA, Bloomfield GS, Chavannes NH, Daivadanam M, Gómez-Olivé FX, Gorre C, Levitt NS, Lotrean LM, Norris SA, Owolabi M, Parker G, Postma MJ, Sheikh A, Siddiqi K, Stratev V, Trofor AC, van Boven JF, van der Kleij RM. Global Alliance for Chronic Disease researchers’ statement on multimorbidity. The Lancet Global Health. 2018;6(12):e1270–e1.
Atun R, de Jongh T, Secci F, Ohiri K, Adeyi O. Integration of targeted health interventions into health systems: a conceptual framework for analysis. Health Policy Plan. 2010;25(2):104–11.
Curry N, Ham C. Clinical and service integration: the route to improved outcomes. London, UK: The King’s Fund; 2010.
Shigayeva A, Atun R, McKee M, Coker R. Health systems, communicable diseases and integration. Health Policy Plan. 2010;25(Suppl 1):i4–20.
Valentijn PP, Schepman SM, Opheij W, Bruijnzeels MA. Understanding integrated care: a comprehensive conceptual framework based on the integrative functions of primary care. Int J Integr Care. 2013;13:e010.
WHO Study Group on Integration of Health Care Delivery. Integration of health care delivery: report of a WHO study group. Geneva, Switzerland: World Health Organization; 1996.
WHO. Integrated care models: an overview. Health Services Delivery Programme. Division of Health Systems and Public Health; 2016.
WHO. Framework on integrated, people-centered health services. 2016.
Sciences TAoM. Multimorbidity: a priority for global health research. 2018.
Armitage GD, Suter E, Oelke ND, Adair CE. Health systems integration: state of the evidence. Int J Integr Care. 2009;9:e82.
Peters MDJ, Marnie C, Colquhoun H, Garritty CM, Hempel S, Horsley T, Langlois EV, Lillie E, O’Brien KK, Tuncalp, Wilson MG, Zarin W, Tricco AC. Scoping reviews: reinforcing and advancing the methodology and application. Syst Rev. 2021;10(1):263.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, Moher D, Peters MDJ, Horsley T, Weeks L, Hempel S, Akl EA, Chang C, McGowan J, Stewart L, Hartling L, Aldcroft A, Wilson MG, Garritty C, Lewin S, Godfrey CM, Macdonald MT, Langlois EV, Soares-Weiser K, Moriarty J, Clifford T, Tuncalp O, Straus SE. PRISMA Extension for scoping reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467–73.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Group P-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1.
Uwimana Nicol J, Rohwer A, Young T, Bavuma CM, Meerpohl JJ. Integrated models of care for diabetes and hypertension in low- and middle-income countries (LMICs): protocol for a systematic review. Syst Rev. 2018;7(1):203.
Atlantis E, Fahey P, Foster J. Collaborative care for comorbid depression and diabetes: a systematic review and meta-analysis. BMJ Open. 2014;4(4):e004706.
Chuah FLH, Haldane VE, Cervero-Liceras F, Ong SE, Sigfrid LA, Murphy G, Watt N, Balabanova D, Hogarth S, Maimaris W, Otero L, Buse K, McKee M, Piot P, Perel P, Legido-Quigley H. Interventions and approaches to integrating HIV and mental health services: a systematic review. Health Policy Plann. 2017;32(4 Supplement).
Dudley L, Garner P. Strategies for integrating primary health services in low- and middle-income countries at the point of delivery. Cochrane Database Syst Rev. 2011(7):Cd003318.
Haldane V, Legido-Quigley H, Chuah FLH, Sigfrid L, Murphy G, Ong SE, Cervero-Liceras F, Watt N, Balabanova D, Hogarth S, Maimaris W, Buse K, McKee M, Piot P, Perel P. Integrating cardiovascular diseases, hypertension, and diabetes with HIV services: a systematic review. AIDS Care. 2018;30(1):103–15.
Hopman P, de Bruin SR, Forjaz MJ, Rodriguez-Blazquez C, Tonnara G, Lemmens LC, Onder G, Baan CA, Rijken M. Effectiveness of comprehensive care programs for patients with multiple chronic conditions or frailty: a systematic literature review. Health Policy. 2016;120(7):818–32.
Huang Y, Wei X, Wu T, Chen R, Guo A. Collaborative care for patients with depression and diabetes mellitus: a systematic review and meta-analysis. BMC Psychiatry. 2013;13:260.
Kastner M, Cardoso R, Lai Y, Treister V, Hamid JS, Hayden L, Wong G, Ivers NM, Liu B, Marr S, Holroyd-Leduc J, Straus SE. Effectiveness of interventions for managing multiple high-burden chronic diseases in older adults: a systematic review and meta-analysis. CMAJ. 2018;190(34):E1004–E12.
Li M, Kennedy EB, Byrne N, Gerin-Lajoie C, Katz MR, Keshavarz H, Sellick S, Green E. Systematic review and meta-analysis of collaborative care interventions for depression in patients with cancer. Psycho-oncology. 2017;26(5):573–87.
Sigfrid L, Murphy G, Haldane V, Chuah FLH, Ong SE, Cervero-Liceras F, Watt N, Alvaro A, Otero-Garcia L, Balabanova D, Hogarth S, Maimaris W, Buse K, McKee M, Piot P, Perel P, Legido-Quigley H. Integrating cervical cancer with HIV healthcare services: a systematic review. PLoS ONE. 2017;12(7):e0181156.
Smith SM, Wallace E, O’Dowd T, Fortin M. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst Rev. 2021;1(1):Cd006560.
Tully PJ, Baumeister H. Collaborative care for comorbid depression and coronary heart disease: a systematic review and meta-analysis of randomised controlled trials. BMJ Open. 2015;5(12):e009128.
van Eck JF, Castelijns H, Eijsbroek V, Rijnders CAT, van Marwijk HWJ, van der Feltz-Cornelis CM. Illness burden and physical outcomes associated with collaborative care in patients with comorbid depressive disorder in chronic medical conditions: a systematic review and meta-analysis. Gen Hosp Psychiatry. 2018;50:1–14.
Watson LC, Amick HR, Gaynes BN, Brownley KA, Thaker S, Viswanathan M, Jonas DE. Practice-based interventions addressing concomitant depression and chronic medical conditions in the primary care setting: a systematic review and meta-analysis. J Prim care community health. 2013;4(4):294–306.
Bulstra CA, Hontelez JAC, Otto M, Stepanova A, Lamontagne E, Yakusik A, El-Sadr WM, Apollo T, Rabkin M, Atun R, Bärnighausen T. Integrating HIV services and other health services: a systematic review and meta-analysis. PLoS Med. 2021;18(11):e1003836.
John JR, Jani H, Peters K, Agho K, Tannous WK. The effectiveness of patient-centred medical home-based models of care versus standard primary care in chronic disease management: a systematic review and meta-analysis of randomised and non-randomised controlled trials. Int J Environ Res Public Health. 2020;17(18):1–50.
Kadia BM, Dimala CA, Fongwen NT, Smith AD. Barriers to and enablers of uptake of antiretroviral therapy in integrated HIV and tuberculosis treatment programmes in sub-saharan Africa: a systematic review and meta-analysis. AIDS Res Ther. 2021;18(1):85.
Kappelin C, Carlsson AC, Wachtler C. Specific content for collaborative care: a systematic review of collaborative care interventions for patients with multimorbidity involving depression and/or anxiety in primary care. Fam Pract. 2021.
Lee JK, McCutcheon LRM, Fazel MT, Cooley JH, Slack MK. Assessment of Interprofessional Collaborative Practices and Outcomes in adults with diabetes and hypertension in primary care: a systematic review and Meta-analysis. JAMA Netw Open. 2021;4(2):e2036725.
Martens N, Destoop M, Dom G. Organization of community mental health services for persons with a severe mental illness and comorbid somatic conditions: a systematic review on somatic outcomes and health related quality of life. Int J Environ Res Public Health. 2021;18(2):1–19.
Nyirenda JLZ, Bockey A, Wagner D, Lange B. Effect of tuberculosis (TB) and diabetes mellitus (DM) integrated healthcare on bidirectional screening and treatment outcomes among TB patients and people living with DM in developing countries: a systematic review. Pathogens and Global Health. 2022.
Rohwer A, Uwimana Nicol J, Toews I, Young T, Bavuma CM, Meerpohl J. E ffects of integrated models of care for diabetes and hypertension in low-income and middle-income countries: a systematic review and meta-analysis. BMJ Open. 2021;11(7):e043705.
Smith SM, Wallace E, Clyne B, Boland F, Fortin M. Interventions for improving outcomes in patients with multimorbidity in primary care and community setting: a systematic review. Syst Reviews. 2021;10(1):271.
Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, Altman DG, Barbour V, Macdonald H, Johnston M, Lamb SE, Dixon-Woods M, McCulloch P, Wyatt JC, Chan AW, Michie S. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687.
Mounier-Jack S, Mayhew SH, Mays N. Integrated care: learning between high-income, and low- and middle-income country health systems. Health Policy Plan. 2017;32(suppl4):iv6–iv12.
Adler AJ, Drown L, Boudreaux C, Coates MM, Marx A, Akala O, Waqanivalu T, Xu H, Bukhman G. Understanding integrated service delivery: a scoping review of models for noncommunicable disease and mental health interventions in low-and-middle income countries. BMC Health Serv Res. 2023;23(1):99.
Mastellos N, Gunn L, Harris M, Majeed A, Car J, Pappas Y. Assessing patients’ experience of integrated care: a survey of patient views in the North West London Integrated Care Pilot. Int J Integr Care. 2014;14:e015.
Ouwens M, Wollersheim H, Hermens R, Hulscher M, Grol R. Integrated care programmes for chronically ill patients: a review of systematic reviews. Int J Qual Health Care. 2005;17(2):141–6.
Goodwin N, Sonola L, Thiel V, Kodner D. Co-ordinated care for people with complex chronic conditions. Key lessons and markers for success. The King’s Fund; 2013.
Shaw S, Rosen R, Rumbold B. What is integrated care? Research Report. Nuffield Trust; 2011.
Bardsley M, Steventon A, Smith J, Dixon J. Evaluating integrated and community-based care. 2013.
Acknowledgements
We would like to thank Anel Schoonees for her assistance in conducting the searches for this scoping review.
Funding
This research was supported by the funding from the Collaboration for Evidence-based Healthcare and Public Health in Africa (CEBHA+) project which is funded by the German Federal Ministry of Education and Research (BMBF) as part of the Research Networks for Health Innovation in Sub-Saharan Africa Funding Initiative. The funder did not have any role in the review process.
Author information
Authors and Affiliations
Contributions
Conception or design of the work (AR, JUN, IT, JJM, TK, TY) acquisition, analysis, or interpretation of data (AR, JUN, IT, ARA, CMB, TY, JBN, JJM, TK, JLZN), drafting the work (AR, IT, JUN, ARA, CMB, TY, JBN, JJM, TK, JLZN) or revising it critically (AR, IT, JUN, TY, JBN, JJM, TK), final approval of the version to be published (all authors), agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved (all authors).
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rohwer, A., Toews, I., Uwimana-Nicol, J. et al. Models of integrated care for multi-morbidity assessed in systematic reviews: a scoping review. BMC Health Serv Res 23, 894 (2023). https://doi.org/10.1186/s12913-023-09894-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09894-7