
Abstract
Background
Trustful relationships play a vital role in successful organisations and well-functioning hospitals. While the trust relationship between patients and providers has been widely studied, trust relations between healthcare professionals and their supervisors have not been emphasised. A systematic literature review was conducted to map and provide an overview of the characteristics of trustworthy management in a hospital setting.
Methods
We searched Web of Science, Embase, MEDLINE, APA PsycInfo, CINAHL, Scopus, EconLit, Taylor & Francis Online, SAGE Journals and Springer Link from database inception up until Aug 9, 2021. Empirical studies written in English undertaken in a hospital or similar setting and addressed trust relationships between healthcare professionals and their supervisors were included, without date restrictions. Records were independently screened for eligibility by two researchers. One researcher extracted the data and another one checked the correctness. A narrative approach, which involves textual and tabular summaries of findings, was undertaken in synthesising and analysing the data. Risk of bias was assessed independently by two researchers using two critical appraisal tools. Most of the included studies were assessed as acceptable, with some associated risk of bias.
Results
Of 7414 records identified, 18 were included. 12 were quantitative papers and 6 were qualitative. The findings were conceptualised in two categories that were associated with trust in management, namely leadership behaviours and organisational factors. Most studies (n = 15) explored the former, while the rest (n = 3) additionally explored the latter. Leadership behaviours most commonly associated with employee’s trust in their supervisors include (a) different facets of ethical leadership, such as integrity, moral leadership and fairness; (b) caring for employee’s well-being conceptualised as benevolence, supportiveness and showing concern and (c) the manager’s availability measured as being accessible and approachable. Additionally, four studies found that leaders’ competence were related to perceptions of trust. Empowering work environments were most commonly associated with trust in management.
Conclusions
Ethical leadership, caring for employees’ well-being, manager’s availability, competence and an empowering work environment are characteristics associated with trustworthy management. Future research could explore the interplay between leadership behaviours and organisational factors in eliciting trust in management.
Similar content being viewed by others


Background
Trustful relationships between professionals are an important quality of both successful organisations and well-functioning hospitals [1, 2]. Professional workers in high-trust organisations are happier, more productive, have more energy, collaborate better, and are more loyal to their organisations than people working in low-trust companies [2]. Studies in hospital settings seem to indicate similar findings. In Taylor & al.’s [1] systematic review study of factors and strategies associated with high performing hospitals, trustful relationships was found to be one of the more important factors. High performing hospitals demonstrated respectful and valued relations between staff members [3, 4].
The phenomenon of trust has been widely studied. A commonly used definition is Mayer, Davis and Schoorman’s (1995) definition of trust as the “willingness of a party to be vulnerable to the action of another party based on the expectation that the other will perform a particular action important to the trustor, irrespective of the ability to monitor or control that other party” [5]. Within the healthcare sector, the published literature has explored many facets of trust, such as trust in healthcare in general [6,7,8], trust between patients and providers [9,10,11], trust between healthcare providers [12, 13] and trust between healthcare providers and their supervisors [14, 15].
Studies have showed that trust is important in relations between healthcare professionals and patients. Patient trust has an impact on patient satisfaction, adherence, and continued enrolment [16,17,18,19]. Trust is also highly important for the level of openness in communication between doctors and patient [20]. According to many theoretical approaches to the study of trust, a central aspect of trust relationships is the trustor’s lack of precautionary measures against the trustee [21,22,23]. Patients are vulnerable because of their illness, and the asymmetrical knowledge of medicine [24,25,26].
McCabe and Sambrook [27] studied the antecedents, attributes and consequences of trust between nurses and nurse managers. In terms of consequences, when trust was “high” there were positive outcomes such as professionalism, efficiency and a high quality patient care delivered; while the contexts where trust was low or lacking, led to negative effects such as conflict, absenteeism and turnover; reduced levels of teamwork, patient care quality, support, delegation and efficiency; and increased levels of work-related stress and surveillance [27].
These very different studies point in divergent directions. We understand that trust is often associated with positive outcomes for both patients and healthcare professionals. But we lack a systematic review of trust between healthcare providers and their supervisors. A handful of systematic literature reviews focused on patients’ trust in their healthcare providers [10, 28, 29], and one reviewed literature on healthcare professionals’ trust in patients [11]. In terms of trust relations between healthcare professionals and their supervisors, one systematic review explored how motivation is influenced by such relationships [13]. However, there is a lack in the overview of the published literature on what characterises this trust relationship between employees and their supervisors within a hospital setting.
Given this gap in knowledge, we aim to study the trust relationships, or lack thereof, between healthcare staff and their supervisors by conducting a systematic review that will map and provide an overview of the published literature on this topic. We want to study:
What are the characteristics of trustworthy and/or untrustworthy management, be it culture of sharing, management style and tools, manager characteristics, etc; in a hospital or a similar setting such as wards or large general/family practices?
Methods
Search strategy
Seven databases (Web of Science, Embase, MEDLINE, APA PsycInfo, CINAHL, Scopus and EconLit) and three publisher platforms (Taylor & Francis Online, SAGE Journals and Springer Link) were searched systematically to find eligible records. These sources were searched based on the relevance of the fields they covered to the subject of this review, such as medicine, social sciences, nursing and allied health and healthcare policy and management.
The search strategy used to identify relevant records was developed over the course of nine months. The final structure of the search strategy was the product of an iterative process which involved testing of different variations of the search strategy, and discussions among the authors and experts on systematic reviews. The input of an expert in running searches, a university librarian, was sought in order to reach a sound search strategy.
The search strategy has three components and has the following structure: 1) “hospital(s)” OR “ward(s)” AND 2) “health care professional(s)” OR “doctor(s)” OR “nurse(s)” OR “leader(s)” OR “manager(s)” AND 3) “trust” OR “reliance” OR “credibility”. The first component filters by the setting this review is focused on, namely hospitals. The second component establishes the actors/stakeholders within a hospital and is captured by the terms listed above and their synonyms. The third component represents the interaction or relationship between the actors and is linked to the search strategy with a proximity operator. Proximity operators were also used for some of the terms in the second component of the search strategy in order to make the strategy more specific, like “(healthcare NEAR/x professional$)”. Where applicable, the searches were limited to English language.
The detailed search strategy can be found in an additional file [see Additional file 1]. The final search was carried out on the 9th of August 2021.
Eligibility criteria
For records to be included in this review, several inclusion criteria were applied. Firstly, in terms of context and participants, eligible studies had to be undertaken in a hospital setting or similar settings where healthcare professionals and managers are present and patients are being treated. Secondly, related to topic, studies should have addressed and explored aspects relevant to the relationship of trust / trustworthiness of subordinates with their higher-ups. Thirdly, eligible records should be of empirical nature. Initially there was no exclusion based on study design; this criterion was later changed in the full-text screening review, as systematic reviews were excluded. However, this criterion remained broad as this review aimed to identify studies of qualitative, quantitative and mixed designs. This was motivated by our purpose to capture, on one hand, the objectiveness that quantitative studies offer on the topic, and on the other to capture the in-depth understanding that qualitative studies provide. Lastly, articles should be written in English. No limit on the year of publication was imposed.
Record selection
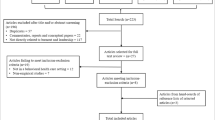
The processes of identification, screening and inclusion are depicted in Fig. 1. Flow diagram.

Flow diagram. * The Ovid platform provided the option of removing duplicates from the records identified before downloading the citations, as the search was performed in multiple databases at once. Adapted from Page, McKenzie [30]
The search resulted in a total of 16,766 records, 15,970 from databases searches and 796 from publisher platforms. Then 9352 duplicate records were removed before the screening process. More specifically, 2851 duplicates were removed before the citations were downloaded. These come from the search conducted in the Ovid platform, which allowed deduplication for the search performed in multiple databases (Embase, MEDLINE and APA PsycInfo) at once.
After the citations were downloaded and imported in the EndNote X9 reference manager, 5462 duplicates were automatically identified by the reference manager. An additional 1039 duplicates were identified manually and removed. Thus, after all duplicates were removed, a total of 7414 records were screened.
The first half and second half were independently screened by two researchers. IS and AIV screened the first half, while HS and AIV screened the second half. The screening comprised of scanning the titles and abstracts. A total of 7380 records were removed; 7289 did not meet the inclusion criteria, based on title and abstract, 5 records were not written in English and an additional 86 duplicate records were found. The 47 remaining publications were discussed by all three researchers, with a focus on the ones that we were in disagreement over. The discussions resulted in 2 records out of the 15 previously agreed upon to be excluded and 21 publications out of the 32 were agreed to be included in the full-text review. Thus, a total of 34 publications were sought for retrieval.
30 records were retrieved. For four records, a full-text version could not be retrieved. The authors of these papers were contacted through Research Gate, but no reply was given. An additional number of 6 papers were identified through reference check of the included records. These were retrieved, and a final number of 36 full-text articles were assessed for eligibility.
The full-text review was performed independently by all authors, and 18 articles met the inclusion criteria. The rest (n = 18) were excluded based on the reasons listed in Fig. 1. The list of the excluded papers can be found under Additional file 2.
Data analysis and synthesis
Given the descriptive nature of this review’s research question, and the inclusion of papers with different research designs (both qualitative and quantitative), a narrative approach to data analysis and synthesis was adopted. This entailed developing textual and tabular summaries of findings, which were then used to synthesise the findings under two separate sets of factors.
Data extraction was performed by one researcher (AIV) and checked for correctness by another (IS), and comprised of three categories. The first one relates to details about the included studies: author(s), year of publication, aim(s), methodology (design, setting, participants and sample, instrument and measured concepts, data analysis) and country. The detailed summary of included studies can be found under Additional file 3. The second category comprises of results relevant to the research question and the concept of trust extracted from quantitative studies, such as hypotheses and whether they were supported or not. The extracted data for the second category is available under Additional file 4. And the third category similarly gathered results pertinent to the research question from qualitative studies, such as themes identified by the authors of the included studies and their interpretations of supporting evidence quoted from interviews. The extracted data included in this category can be found under Additional file 5.
Once all the data was extracted, based on his experience in the field of leadership, management and organisations, IS observed patterns in the results. More specifically, characteristics of trustworthy management were noticed to fit under two categories, namely leadership behaviours and organisational factors. IS then summarised and categorised the results into the two classifications. These summaries were presented and discussed with the two other authors during the process. All authors agreed that the summaries were representative of the original findings. The summaries were presented as tables in the results section.
The results section firstly described the study characteristics, then laid out common aspects identified between the qualitative and quantitative studies included in the review. The common aspects related to trust and ethics, trust and well-being, trust and availability and trust and competence. Aspects not common between the quantitative and qualitative studies were presented separately.
All included studies were critically appraised by two researchers. The qualitative studies (n = 6) were assessed by HS and AIV using the JBI Critical appraisal checklist for qualitative research [31] and the quantitative studies were appraised by IS and AIV using an adapted checklist by the National Institute for Health and Clinical Excellence (NICE) for a questionnaire study [32]. The NICE checklist did not provide response options, and in order to be consistent, we decided to use the ones from the JBI checklist (Yes, No, Unclear and Not applicable). The overall appraisal scale published by Roever [33] was used to rate the overall methodological quality of the studies included in this review. The results of the critical appraisal were used to provide an overall picture over the quality of the included studies and to determine whether there were any papers of poor quality, with significant flaws that would determine their exclusion from this review.
Results
Research methods, setting and participants, journals and countries
Tables 1 and 2 lay out the summaries of the quantitative and qualitative included studies in a concise manner. The majority of the studies used a quantitative research design (n = 12), in which surveys (n = 5) and questionnaires (n = 7) were self-administered. With two exceptions, studies (n = 11) collected the data at one point in time. The first exception is a study in which the data was gathered sequentially; with two weeks between the collection of demographic, independent and dependent variables. And the second exception is a study that had a three-week follow-up, but no details are presented. The rest of the included studies had a qualitative design (n = 6); two of which solely collected data through interviews, while the rest (n = 4) used a combination of interviews, focus groups, document reviews or observations such as participant observations, facility audits and research memos.
In terms of setting, studies took place in hospitals (n = 12), hospitals and clinics (n = 3), cancer treatment facilities (n = 1), primary health centres that include inpatient departments (n = 1) and an early psychosis intervention (EPI) clinic (n = 1). Some of the quantitative studies were conducted from the perspective of healthcare employees (nurses and nursing staff) (n = 6), other studies focused on the perspective of employees in management, specialist or administrative positions (n = 3) and three studies included both perspectives. Similarly, one qualitative study captured the perspective of healthcare workers and key-informants, two studies described the management perspective and the rest (n = 3) included both.
Several studies (n = 6) were published in journals that include the healthcare field, such as leadership and management-oriented journals (n = 2), human resources journals (n = 2), industrial psychology (n = 1) and social behaviour (n = 1). While the rest (n = 12) were published in journals covering the healthcare area specifically. The journals were related to management (n = 2), policy and planning (n = 1), leadership (n = 3) and social science and medicine (n = 1) in a general sense, while a handful of studies were published in journals related to nursing specifically (administration and management) (n = 6).
Most of the studies were conducted in the Americas, namely USA (n = 3), Canada (n = 3) and Brazil (n = 1). Then other studies were conducted in European countries, more specifically Italy (n = 2), Poland (n = 1), Portugal (n = 1) and Sweden (n = 1) and the UK (n = 1). Four studies were conducted in countries on the African continent such as South Africa (n = 2), Nigeria (n = 1) and Zambia (n = 1); and one study was conducted in China.
Common aspects
This section firstly describes the two categories that were found to be associated with trust in management, namely leadership behaviours and organisational factors. Then, under the first category, four common aspects across both quantitative and qualitative papers are presented and can be seen under Table 3.
Most of the studies explored leadership behaviours associated with trust in management only (n = 10)[15, 34,35,36,37,38,39,40,41,42]. While five studies described characteristics related to both leadership behaviours and organisational factors that were associated with trust in management [27, 43,44,45,46]. Additionally, three studies explored organisational factors exclusively [47,48,49].
The common aspects are: trust and ethics, trust and well-being, trust and availability and trust and competence and were informed by the following leadership behaviours most commonly related to employees’ trust in their supervisor: different facets of ethical leadership (n = 5), caring for employees’ well-being (n = 5), the manager’s availability (n = 4) and leaders’ competence (n = 4). Each aspect and the studies that informed them are presented below.
Trust and ethics
This first aspect was informed by five studies, two qualitative papers [15, 41] and three quantitative studies [34, 36, 37]. The different aspects of ethical leadership that were addressed included integrity [15, 37], moral leadership [34], fairness [41], and ethical leadership, specifically [36].
Cregård and Eriksson investigated physician-managers’ and nurse-managers’ perceptions of other physicians’ trust in them; and revealed that trust is strengthened by physician-managers’ understanding of “healthcare issues from various perspectives”, but can decrease when physician-managers are “unable to prioritize both managerial and medical issues” or “fulfil professional demands” ([15], Table I. p.287).
In Topp and Chipukuma’s interview study [41], healthcare workers perceived their supervisors in charge of overall or departmental sites to be unfair and inconsistent, for example when selecting staff for workshops or trainings; which contributed to weak trust.
Results from survey studies showed that employee’s affective trust in their direct leaders was positively related to their moral leadership [34]; and that staff nurses’ trust in their ward/unit leader or immediate supervisor was in a positive relationship with ethical leadership [36].
Trust and well-being
One qualitative study [15] and four survey studies [37, 43, 44, 46] informed the second aspect. Caring for employees’ well-being included measures of benevolence [15, 37], supportiveness [46] and showing concern (one of five dimensions of empowering leadership in Bobbio et al.’s [44] study). In Araujo and Figueiredo’s study, trust was measured with five items, including: “The superiors care about my well-being at work” ([43], Table II.).
The qualitative study informing this aspect showcases that physician- and nurse-managers perceive that other physician’s trust in them is increased when the physician-manager shows care towards “patients, colleagues and other healthcare professionals” ([15], Table I. p.287).
In Wong and Cummings’s study [46], clinical (such as nurses, pharmacists, doctors and other professionals) and non-clinical employees (administrative, support and research staff) completed a survey with regards to trust in management; and the results were reported separately for the two samples. Supportiveness, as part of the leadership behaviour latent concept developed for the model that was tested in the study, had a significant indirect effect on trust in management among the clinical sample of employees ([46], p.14).
Trust and availability
This third aspect was developed based on two qualitative papers [27, 38] and two quantitative papers [43, 46]. The manager’s availability was measured as being accessible [43] and approachable [46]. McCabe and Sambrook [27] found that nurse managers who were considered accessible, approachable and involved were more likely to be trusted by nurses. The opposite was true for managers who were “perceived as ‘inaccessible’, ‘removed’ or those managers higher up within the organisational hierarchy” ([27], p. 821). In Freysteinson et al.’s [38] study, availability relates to leaders’ efforts to maintain a visible and accessible leadership presence (with emphasis on face-to-face interaction with the staff).
In Araujo and Figueiredo’s study, another one of the five items that measured trust relates to: “My superiors are accessible and open to dialogue” ([43], Table II.). In Wong and Cummings’s study [46], another of the leadership behaviours, relational transparency, had a direct and significant influence on perceptions of trust in management, but only among the non-clinical sample of employees. There were no other direct significant effects between leadership behaviours and trust in management ([46], p. 14 and 16); making this study the only one included in this review that found mixed or no results for relationships between leadership behaviours and trust.
Trust and competence
Three qualitative papers [15, 27, 41] and one quantitative study [37] informed this last aspect. The studies found that leaders’ competence, in terms of knowledge [37], medical competence [15] and decision making skills [27, 41], were related to perceptions of trust.
The physician-manager’s medical competence, on one side, was deemed “valuable when managerial healthcare decisions are required” and the participants (physician- and nurse-managers) perceived this as a factor that increased trust in the physician-manager ([15], Table I. p.287). On the other side, the participants also perceived that “physician-managers should have extensive involvement in medical practice” in order to maintain competence in daily medical work ([15], Table I. p.287).
Organisational factors
One qualitative study [27] and seven quantitative studies [43,44,45,46,47,48,49] studied organisational factors associated with trust. Work environments in which employees experienced empowerment (n = 4) [43, 45, 47, 48] were most commonly associated with trust in management. Salary, workload and administrative support was also related to trust in one study [46]. In the qualitative study [27], the authors found that antecedents of trust converged mainly on organisational factors such as immediate work environment, communication systems and new management practices.
Quantitative studies
The quantitative studies had different conceptualisations and measures of trust. Some studies measured trust as a one-dimensional concept, e.g. “trust in leader” [36] and “trust in supervisor” [49]. Other studies measured trust as a multi-dimensional concept. For example, in da Costa Freire and Azevedo’s [47] study, trust was operationalised as “perceptions of trustworthiness in the supervisor”, and measured on three dimensions (integrity, benevolence and ability). Laschinger, Finegan [48] separated trust into subscales measuring faith in the intentions of managers and confidence in managers’ actions. One study [43] conceptualised trust as one of nine dimensions related to internal climate at work.
Variations in the type of trust relationships investigated were also observed. For example, Bai et al. [34] studied general employees’ affective trust in their direct leaders. Bobbio et al. [44] and Bobbio and Manganelli [45] focused on nursing staff’s trust in leader (nurse manager in this case) and trust in the organisation; and similarly, another study [36] specified that nursing staff’s trust in leaders was understood as trust in their ward/unit leader or immediate supervisor. Additionally, one study [35] investigated workplace trust which was comprised of trust in organisation, trust in immediate supervisor and trust in co-workers.
Qualitative studies
Among the six qualitative studies, four studies explored trust explicitly in the research aim [15, 27, 40, 41], while two studies identified trust as an emerging factor in the data analysis [38, 42].
In two of the qualitative studies [15, 38], trust was explored through managers’ own perspectives. Cregard and Eriksson [15] interviewed and conducted focus groups with physician managers and nurse-managers, with the aim of exploring trust in relation to physicians’ dual roles as managers and clinicians. According to the managers, aspects related to competence, benevolence, and integrity could influence physician employees’ trust in physician-managers. Difficulties related to combining the managerial and medical role was also described as a common reason for decreased trust. Freysteinson and colleagues [38] interviewed nursing leaders in American hospitals about their leadership experiences under the COVID-19 pandemic. The authors describe how the leaders became aware of face-to-face interaction as crucial to earning the trust of the employees, and that “leaders felt transparency increased trust” (p.1539). While the findings from these two studies were gathered from the lens of managers themselves, they are consistent with findings from other studies in our review.
Critical appraisal
Table 4 presents the assessment of risk of bias for each paper included in the review.
Out of the six qualitative papers assessed, most of them (n = 4) were rated as acceptable; while one paper was rated between acceptable and low quality and one paper as high quality. The majority of the quantitative papers (n = 10) were rated as acceptable and the rest (n = 2) were rated as high quality. Thus, most papers included in this study were assessed as acceptable. No study was excluded based on quality, as none were rated as poor (0).
Discussion
Summary of findings
This systematic literature review aimed to provide an overview of the published literature over the characteristics of the trust relationship between employees and their supervisors within a hospital setting. Based on the included studies, these characteristics were categorised under two aspects: leadership behaviours and organisational factors associated with trust in management. Most studies explored leadership behaviours, and thus some common aspects emerged between the qualitative and quantitative papers. The common aspects are: trust and ethics, trust and well-being, trust and availability and trust and competence. These are discussed below.
Trust and ethics
Five included articles emphasised different aspects of ethical leadership for trust relationships to grow between employee and manager. Integrity, moral leadership, fairness and ethical leadership are mentioned specifically. In clinical studies on relationships between healthcare professionals and patients, it is more common to thematise reciprocity and “being taken seriously as a human being” [20]. Brown [50] has claimed that doctors’ standing as caring and competent now depends to a great degree on communication and involvement with the patient before trust can be earned. Showing reciprocal humanity creates common ground with the patient, and this review shows that similar effects play a role between leader and healthcare professionals.
Studies from other industries have also marked the impact ethical leadership has on trust in leader. For example, Newman et al. [51] showed that in a sample of n = 184 pairs of employees-supervisors from three Chinese firms, ethical leadership lead to higher levels of trust in leader (both cognitive and affective). Similarly, Dadhich and Bhal [52] found that ethical leadership predicted affective and cognitive trust in a sample of post-graduate engineering students in India.
Trust and well-being
Several included studies showed a connection between managers’ care for the employees’ well-being and trust relationships. Being available when concerns are voiced, and listening to employees’ worries is important. A survey study on 107 white-collar employees working in various organisations in Malaysia [53] highlighted that when employees perceived their supervisor to show benevolence, integrity and ability, trust in them was predicted both directly and indirectly. Studies on the trust relationship between healthcare professionals and patients emphasise this characteristic even more clearly, as many studies have focused on how trust is built [20], and we can see some similarities to how trust is built between healthcare staff and managers. E.g., Skirbekk & al. have shown how relationships between healthcare professionals and patients based on “open mandates of trust” are more resilient [19]. The findings from the studies included in our study show that managers’ care for employees’ well-being lead to more caring and empowering trust relationships.
Trust and availability
Manager’s availability was another leadership characteristic associated with trust in management, as shown by four papers included in this review; and had to do with managers being perceived as accessible and approachable. While there are few studies directly exploring the relationship between a supervisor’s availability and employees’ trust towards the supervisor, some studies from other organisational contexts have indicated that a supervisor’s availability might improve the quality of relations between supervisors and employees, both in physical [54] and remote work settings [55].
Trust and competence
Four included studies found the leaders’ competence to be an important characteristic for trust relationships. Employees need to be assured that the leaders know what they are doing, or at least that they have a plan for how the hospital should be run. Similarly, Manderson and Warren [56] have shown how competence is often the most important dimension of trust relations with healthcare professionals. Studies on the doctor-patient relationship in different medical contexts have shown that the better a patient feels informed about the treatment process, the greater trust he or she will experience [57,58,59,60]. This trust in competence makes it possible for the patients to bridge the knowledge gap [24] through a “leap of faith” [25, 26]. There might be a similar “leap of faith” by health professionals towards their supervisors. Employees can rarely be expected to have knowledge on how hospitals should be run, but it is important for them to be able to trust that the leaders have this competence.
In terms of supervisors’ trustworthiness and competence, hospitals and related settings might place emphasis both on managerial and clinical competence. Studies of healthcare managers have found that doctors in management positions attempt to maintain their clinical competence. For example, Spehar & al. [61] found that Norwegian doctors in management positions in hospitals placed importance on “being perceived as a competent clinician in order to be taken seriously by the medical staff.“ The authors also found that clinical knowledge was important for “winning” arguments with the staff. This is in line with arguments by other authors on how doctors in management seek to maintain their clinical knowledge in order to sustain legitimacy among their staff, especially their professional colleagues [62, 63].
Trust and culture
Studies have shown that there might be cultural differences in leader expectations and trust. Indeed, words such as «paternalistic», «feminine» and «masculine» are sometimes used to differentiate cultural expectations towards management [64, 65]. For example, employees in Western countries might expect a more «feminine», or empowering leadership style, whereas employees in Asian countries might expect a more paternalistic leadership style [66]. But studies have also shown similarities in expectations across different countries. For example, most employees want managers who are perceived as inspirational, competent and fair [67].
We have not observed explicit cultural differences in our included studies in terms of trust, although the number of studies included in our analysis might not be conducive to a comprehensive comparison of cultural differences. However, the study by Bai et al. [34], included in our study, found that authoritarian leadership of direct leaders had positive impacts on employees’ personal initiative. We can therefore not rule out that cultural differences might influence perceptions of trustworthiness.
Methodological considerations
The fact that only one author extracted the data and no standardised data extraction form was used, could pose as a risk of error. This risk was reduced, as another author checked the correctness of the extracted data. Another drawback of this systematic literature review is that it was not registered and a formal review protocol was not used in guiding how this review was conducted. However, we did follow strict guidelines developed throughout years of experience and discussions with experienced reviewers. The expert knowledge of a librarian was also sought in the process of developing the search strategy. We also discussed conducting a more in-depth synthesis of the 6 qualitative papers, but we decided against it since we found the research questions in the included studies were not homogenous enough. This might be considered a missed opportunity.
Quality of the included papers
14 of the 18 included articles have an acceptable quality. According to the rating scale we used [33], this means that most criteria were met but there are “some flaws in the study with an associated risk of bias”. For the qualitative studies rated as acceptable (n = 4), the associated risk of bias mostly arises from studies not locating the researcher culturally or theoretically, and not addressing the influence of the researcher on the research. For the quantitative studies rated as acceptable (n = 10), the associated risk of bias arose mostly from studies being unclear regarding whether the sampling frame was sufficiently large and representative; and somewhat from studies not discussing potential response biases. One qualitative paper was evaluated as having a quality between acceptable and low. An associated risk of bias stemmed from the study not locating the researcher culturally or theoretically and not discussing his/her influence on the research. The reason for leaning towards rating this paper low quality is the study failing to provide a statement on whether ethical approval by an appropriate body was granted.
Although the quality of the included quantitative papers was acceptable, and high in two cases, the use of surveys and questionnaires to capture an abstract concept such as trust can be viewed as a limitation. However, claims for the validity and reliability of the instruments used have been made and were justified in all papers, except for three, where the claims related to validity were unclear.
Conclusion and future research
The aim of our study was to provide an overview of the existing literature related to characteristics of trustworthy management. We found that most of the studies explored leadership behaviours associated with trust in management. Leadership behaviours related to ethical leadership and caring for employees’ well-being were the most prominent in these studies. Based on our review, we present the following main suggestions for future research.
Firstly, based on the findings from the included studies, both leadership behaviours and organisational factors appear to be related to trust in management. However, these are not clearly distinct dimensions. For example, individual managers might positively or negatively influence employees’ perceptions of the work environment. Likewise, the work environment or organisational culture might influence individual leaders’ behaviours. Therefore, there is likely an interplay between factors in the work environment and individual leadership behaviours. More research is needed to untangle these relationships.
Secondly, we did not seek to explore whether certain leadership behaviours or organisational factors were more or less important in eliciting trust in management. The included studies did not explicitly aim to delineate such “hierarchies”. Future systematic review studies could explore possible causal relationships between leadership behaviours and organisational factors on employees’ trust in management.
Thirdly, the studies in our review explored characteristics of trustworthiness in formal managers. Informal leaders may also have a prominent role in some healthcare settings, but we cannot infer that the same characteristics will be relevant for understanding perceptions of trustworthiness in informal leaders. This is an aspect that could be researched further.
Lastly, only one study in our review reported results from two different samples (clinical and non-clinical workers). Future studies could investigate differences and similarities in how different employees in a medical setting (such as clinicians and non-clinicians) or healthcare professionals (such as nurses compared to physicians) view trustworthy management.
Data availability
All relevant data are within the paper and its attached Additional files.
Abbreviations
- OsloMet:
-
Oslo Metropolitan University
- UiO:
-
University of Oslo
- NICE:
-
National Institute for Health and Care Excellence
- EPI:
-
Early Psychosis Intervention
- SEM:
-
structural equation modelling
References
Taylor N, Clay-Williams R, Hogden E, Braithwaite J, Groene O. High performing hospitals: a qualitative systematic review of associated factors and practical strategies for improvement. BMC Health Serv Res. 2015;15(1):244.
Zak PJ. The neuroscience of Trust. Management behaviors that foster employee engagement. Harvard Business Rev. 2017(Jan-Feb).
Bradley EH, Curry LA, Webster TR, Mattera JA, Roumanis SA, Radford MJ, et al. Achieving rapid door-to-balloon times: how top hospitals improve complex clinical systems. Circulation. 2006;113(8):1079–85.
Landman AB, Spatz ES, Cherlin EJ, Krumholz HM, Bradley EH, Curry LA. Hospital collaboration with emergency medical services in the care of patients with acute myocardial infarction: perspectives from key hospital staff. Ann Emerg Med. 2013;61(3):185–95.
Mayer RC, Davis JH, Schoorman FD. An integrative model of organizational trust. Acad Manage Rev. 1995;20(3):709–34.
Calnan M, Rowe R. Trust and Health Care. Sociol Compass. 2007;1(1):283–308.
Calnan MW, Sanford E. Public trust in health care: the system or the doctor? Qual Saf Health Care. 2004;13(2):92–7.
Gilson L. Trust in health care: theoretical perspectives and research needs. J Health Organ Manag. 2006;20(5):359–75.
Murray B, McCrone S. An integrative review of promoting trust in the patient–primary care provider relationship. J Adv Nurs. 2015;71(1):3–23.
Brennan N, Barnes R, Calnan M, Corrigan O, Dieppe P, Entwistle V. Trust in the health-care provider–patient relationship: a systematic mapping review of the evidence base. Int J Qual Health Care. 2013;25(6):682–8.
Sousa-Duarte F, Brown P, Mendes AM. Healthcare professionals’ trust in patients: a review of the empirical and theoretical literatures. Sociol Compass. 2020;14(10):e12828.
Sutherland BL, Pecanac K, LaBorde TM, Bartels CM, Brennan MB. Good working relationships: how healthcare system proximity influences trust between healthcare workers. J Interprof Care. 2021:1–9.
Okello DRO, Gilson L. Exploring the influence of trust relationships on motivation in the health sector: a systematic review. Hum Resour Health. 2015;13(1):16.
Mullarkey M, Duffy A, Timmins F. Trust between nursing management and staff in critical care: a literature review. Nurs Crit Care. 2011;16(2):85–91.
Cregård A, Eriksson N. Perceptions of trust in physician-managers. Leadersh Health Serv (Bradf Engl). 2015;28(4):281–97.
Anderson LA, Dederick RF. Development of the trust in physician scale: a measure to assess interpersonal trust in patient-physician relationships. Psychol Rep. 1990;67.
Hall MA, Dugan E, Zheng B, Mishra AK. Trust in physicians and medical institutions: what is it, can it be measured, and does it matter? Milbank Q. 2001;79(4).
Safran D, Kosinski M, Tarlov, Rogers, Taira L et al. The Primary Care Assessment Survey: tests of Data Quality and Measurement Performance. Med Care. 1998;36.
Thom DH, Hall MA, Pawlson LG. Measuring patient’s trust in physicians when assessing quality of care. Health Aff. 2004;23.
Skirbekk H, Middelthon A-L, Hjortdahl P, Finset A. Mandates of Trust in the doctor-patient relationship. Qual Health Res. 2011;21(9):1182.
Grimen H. Gode institusjoners betydning for tillit. In: Skirbekk H, Grimen H, editors. Tillit i Norge. Oslo: Res Publica; 2012.
Hertzberg L. On the attitude of Trust. Inquiry. 1988;31.
Skirbekk H. Presupposed or negotiated trust? Explicit & implicit interpretations of trust in a medical setting. Med Health Care Philos. 2009;12.
Calnan M, Rowe R. Trust relations in a changing health service. J Health Serv Res Policy. 2008;13(3suppl):97–103.
Möllering G. Trust: reason, routine. Reflexivity: Elsevier; 2006.
Simmel G. The philosophy of money. London: Routledge; 1978.
McCabe TJ, Sambrook S. The antecedents, attributes and consequences of trust among nurses and nurse managers: a concept analysis. Int J Nurs Stud. 2014;51(5):815–27.
Birkhäuer J, Gaab J, Kossowsky J, Hasler S, Krummenacher P, Werner C, et al. Trust in the health care professional and health outcome: a meta-analysis. PLoS ONE. 2017;12(2):e0170988.
Rørtveit K, Hansen BS, Leiknes I, Joa I, Testad I, Severinsson E. Patients’ experiences of trust in the patient-nurse relationship-a systematic review of qualitative studies. 2015.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
JBI. Checklist for qualitatie research. Critical appraisal tools for use in JBI Systematic Reviews. 2020.
NICE. Sickle cell Acute painful episode: management of an Acute painful sickle cell episode in Hospital. Guidelines NIfHaCE, editor. Manchester (UK): National Institute for Health and Clinical Excellence (NICE) copyright © 2012, National Institute for Health and Clinical Excellence.; 2012.
Roever L. Critical appraisal of a questionnaire study. Evid Based Med Pract. 2015;1(2):1–2.
Bai S, Lu F, Liu D. Subordinates’ responses to paternalistic leadership according to leader level. Social Behav Personality: Int J. 2019;47(11):1–14.
Coxen L, van der Vaart L, Stander MW. Authentic leadership and organisational citizenship behaviour in the public health care sector: The role of workplace trust. 2016. 2016;42(1).
Enwereuzor IK, Adeyemi BA, Onyishi IE. Trust in leader as a pathway between ethical leadership and safety compliance. Leadersh Health Serv. 2020;33(2):201–19.
Fleig-Palmer MM, Rathert C, Porter TH. Building trust: the influence of mentoring behaviors on perceptions of health care managers’ trustworthiness. Health Care Manage Rev. 2018;43(1):69–78.
Freysteinson WM, Celia T, Gilroy H, Gonzalez K. The experience of nursing Leadership in a Crisis: a hermeneutic phenomenological study. J Nurs Adm Manag. 2021;19.
Stander FW, de Beer LT, Stander MW. Authentic leadership as a source of optimism, trust in the organisation and work engagement in the public health care sector. Sa J Hum Resource Manage. 2015;13(1).
Stasiulis E, Gibson BE, Webster F, Boydell KM. Resisting governance and the production of trust in early psychosis intervention. Soc Sci Med. 2020;253.
Topp SM, Chipukuma JM. A qualitative study of the role of workplace and interpersonal trust in shaping service quality and responsiveness in zambian primary health centres. Health Policy Plan. 2016;31(2):192–204.
Weaver SH, Lindgren TG, Cadmus E, Flynn L, Thomas-Hawkins C. Report from the night shift: how administrative Supervisors achieve nurse and patient safety. Nurs Adm Q. 2017;41(4):328–36.
Araujo CAS, Figueiredo KF. Brazilian nursing professionals: leadership to generate positive attitudes and behaviours. Leadership in health services. (Bradford England). 2019;32(1):18–36.
Bobbio A, Bellan M, Manganelli AM. Empowering leadership, perceived organizational support, trust, and job burnout for nurses: a study in an italian general hospital. Health Care Manage Rev. 2012;37(1):77–87.
Bobbio A, Manganelli AM. Antecedents of hospital nurses’ intention to leave the organization: a cross sectional survey. Int J Nurs Stud. 2015;52(7):1180–92.
Wong CA, Cummings GG. The influence of authentic leadership behaviors on trust and work outcomes of health care staff. J Leadersh Stud. 2009;3(2):6–23.
da Costa Freire CMF, Azevedo RMM. Empowering and trustful leadership: impact on nurses’ commitment. Personnel Rev. 2015;44(5):702–19.
Laschinger HKS, Finegan J, Shamian J, Casier S. Organizational Trust and empowerment in Restructured Healthcare Settings: Effects on Staff Nurse Commitment. JONA: The Journal of Nursing Administration. 2000;30(9):413–25.
Simha A, Stachowicz-Stanusch A. The effects of ethical climates on trust in supervisor and trust in organization in a polish context. Manag Decis. 2015;53(1):24–39.
Brown PR. Trusting in the new NHS: instrumental versus communicative action. Sociol Health Illn. 2008;30(3):349–63.
Newman A, Kiazad K, Miao Q, Cooper B. Examining the cognitive and affective trust-based mechanisms underlying the relationship between ethical leadership and organisational citizenship: a case of the head leading the heart? J Bus Ethics. 2014;123(1):113–23.
Dadhich A, Bhal KT. Ethical leader behaviour and leader-member exchange as predictors of subordinate behaviours. Vikalpa. 2008;33(4):15–26.
Poon JM. Effects of benevolence, integrity, and ability on trust-in‐supervisor. Empl Relations. 2013.
Werbel JD, Lopes Henriques P. Different views of trust and relational leadership: supervisor and subordinate perspectives. J Managerial Psychol. 2009;24(8):780–96.
Connaughton SL, Daly JA. Identification with leader. Corp Communications: Int J. 2004;9(2):89–103.
Manderson L, Warren N. The art of (re) learning to walk: trust on the rehabilitation ward. Qual Health Res. 2010;20(10):1418–32.
Nannenga MR, Montori VM, Weymiller AJ, Smith SA, Christianson TJ, Bryant SC, et al. A treatment decision aid may increase patient trust in the diabetes specialist. The statin choice randomized trial. Health Expect. 2009;12(1):38–44.
Nagrampa D, Bazargan-Hejazi S, Neelakanta G, Mojtahedzadeh M, Law A, Miller M. A survey of anesthesiologists’ role, trust in anesthesiologists, and knowledge and fears about anesthesia among predominantly hispanic patients from an inner-city county preoperative anesthesia clinic. J Clin Anesth. 2015;27(2):97–104.
Hillen MA, De Haes HC, Smets EM. Cancer patients’ trust in their physician—a review. Psycho-oncology. 2011;20(3):227–41.
Conradsen S, Lara-Cabrera ML, Skirbekk H. Patients’ knowledge and their trust in surgical doctors. A questionnaire-based study and a theoretical discussion from Norway. Social Theory & Health. 2021:1–18.
Spehar I, Frich JC, Kjekshus LE. Clinicians in management: a qualitative study of managers’ use of influence strategies in hospitals. BMC Health Serv Res. 2014;14(1):251.
Berg NL, Byrkjeflot H. Management in hospitals. Int J Public Sector Manag. 2014;27(5):379–94.
Mo OT. Doctors as managers: moving towards general management? J Health Organ Manag. 2008;22(4):400–15.
Chen H-Y, Kao HS-R. Chinese paternalistic leadership and non-chinese subordinates’ psychological health. Int J Hum resource Manage. 2009;20(12):2533–46.
Helgstrand KK, Stuhlmacher AF. National culture: an influence on leader evaluations? Int J Organizational Anal. 1999.
Ling W, Chia RC, Fang L. Chinese implicit leadership theory. J Soc Psychol. 2000;140(6):729–39.
Den Hartog DN, House RJ, Hanges PJ, Ruiz-Quintanilla SA, Dorfman PW, Abdalla IA, et al. Culture specific and cross-culturally generalizable implicit leadership theories: are attributes of charismatic/transformational leadership universally endorsed? Leadersh Q. 1999;10(2):219–56.
Acknowledgements
We are grateful for the help and friendly advice we have received from librarian Pål Magnus Lykkja (UiO) and researcher Marita Sporstøl Fønhus (NK LMH). We would also like to acknowledge the valuable contribution of professor Frode Veggeland (HInn, UiO), with whom we had long discussions that helped shape the research objectives of this review. We are also grateful for the support we have received from UiO and OsloMet for this study.
Funding
All authors´ salaries were funded by their host institution. No funding body was involved in preparing the manuscript or the decision to submit the manuscript for publication in BMC Health Services Research.
Author information
Authors and Affiliations
Contributions
Formulation/identification of the scientific problem and conceptual idea: HS had the conceptual idea. All three authors participated in the development and formulation of the scientific problems. Planning of the experiments and methodology design, including selection of methods and method development: All three authors participated in the development of the methodology. Involvement in data gathering/experimental work and interpretation/analysis: All three authors participated in the gathering and analyses of the data, and all papers were reviewed by at least two authors, but AIV contributed most substantially, as described in the manuscript. Presentation, and discussion of obtained data and work with the manuscript: All three authors participated in the discussion of data. All three authors contributed substantially to the work with the manuscript. AIV and HS wrote the Background section, the Methods section was written by AIV with a contribution by IS, the Results sections was written by AIV and IS with a contribution from HS, the Discussion section was written by all authors and IS wrote the Conclusion section. All authors read and approved the final manuscript. All authors contributed to the revised manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Varga, A.I., Spehar, I. & Skirbekk, H. Trustworthy management in hospital settings: a systematic review. BMC Health Serv Res 23, 662 (2023). https://doi.org/10.1186/s12913-023-09610-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09610-5