
Abstract
Background
Using management competency-based frameworks to guide developing and delivering training and formal education to managers has been increasingly recognized as a key strategy in building management capacity. Hence, interest in identifying and confirming the competency requirements in various contexts have been witnessed. Therefore, learnings from how competency studies were designed and conducted, how competencies were identified, and strategies in ensuring success in competency identification are of great value to researchers planning and conducting competency studies in their own country.
Methods
A scoping review was conducted guided by the Arksey and O’Malley framework and reported according to the PRISMA Extension for Scoping Reviews (PRISMA-ScR). All papers that published empirical studies aiming at identifying and assessing manager’s competencies at the peer-reviewed journals were identified from Web of sciences, PubMed, Scopus and Emerald Management between 2000 and 2021. In order to maximize learning, studies focusing on health and non-health sectors are all included.
Results
In total, 186 studies were included in the review including slightly more than half of the studies conducted in health sector (54.5%). 60% of the studies focused on mid to senior level managers. Surveys and Interviews were the two most commonly used methods either solely or as part of the mix-method in the studies. Half of the studies used mixed methods approach (51.1%). Large proportion of the papers failed to include all information that is necessary to contribute to learning and improvement in future study design. Based on the results of the scoping review a four steps framework was developed that can guide designing and implementing management competency studies in specific country vs. sector context and to ensure benefits of the studies are maximised.
Conclusion
The review confirmed the increasing trend in investing in management competency studies and that the management competency identification and development process varied substantially, in the choice of methods and processes. The identification of missing information in majority of the published studies calls for the development of more rigorous guidelines for the peer-review process of journal publications. The proposed framework of improving the quality and impact of the future management competency study provides clear guidance to management competency identification and development that promotes the functional alignment of methods and strategies with intended uses and contexts.
Similar content being viewed by others

Background
In recent decades developing a competent health service management workforce has been well recognized as one of the means to improving health service effectiveness and efficiencies [1,2,3] which is critical to the sustainability of health systems in order to meeting the increasingly complex health needs and demands. Therefore, global movement in developing better understanding of the competencies required by health service managers in different healthcare context (countries vs. settings vs. management positions) has been witnessed [4,5,6,7,8]. The importance of adopting a competency-based approach in designing and developing training and educational programs in health management has been recognized as the means to building health system management capacity and improving effectiveness and quality of health service delivery [2, 9,10,11,12], making the understanding of management competency requirements for health service management fundamental [2, 13].
Management competencies are context-sensitive and influenced by the complexity of management levels, nature of management positions, and the team, organization and system in which these competencies to be demonstrated. No one healthcare system is the same, differing healthcare environment and health policy of different countries may affect the competency requirements of their managers differently. Hence, management competencies cannot be adopted without considering the differing healthcare context [14,15,16,17]. In the past two decades, increasing number of management competency studies have been undertaken in the developed countries such as Australia, USA, UK, Canada, Switzerland and Finland [1, 5, 8, 11, 18, 19]. There has also been increasing reinforcement of the importance of health management competency in developing countries such as Iran, Thailand, Vietnam, South Africa, Bhutan, and Indonesia [4, 7, 9, 20,21,22]. Although efforts in developing country-based understanding of the management competency requirements have been continuous and increasing, in comparison with the efforts in non-health sector, management competency development in health sectors is still in its infancy, hence learning the experience of management competency identification from both health and non-health sectors are beneficial.
In addition to overcoming common challenges facing any research projects, the identification of management competency requirements have its own hurdles to overcome and can be a complex process. Firstly, the concept and role of management competency have been interpreted differently between researchers and managers. Bridging such understanding is critical to ensuring the relevance and validity of the competency identified. Secondly, health service management has not be universally accepted as a certified profession and represents a large number of different positions varied by management level, functionality and settings [2] which makes creating a ‘blanket competency framework’ less straightorward. Thirdly, the recruitment and involvement of health service managers in management competency studies are challenging because of the busy nature and associating high pressure of the management roles, often resulting in low response [2]. Fourthly, the validity of the process of identifying management competency is important to ensuring that the competency framework developed can guide formulation of management training curriculum. Such process is also important to confirm the context in which the developed management competency framework can be used to guide application.
While no guidance is currently available on what specific methods to use, and when and how to use to identify management competencies, there is consensus that in order to increase the validity and utility of competency frameworks developed, a combination of approaches may be necessary, akin to a process of triangulation [23]. However, consideration of the feasibility of the study, complexity of practice, and ease of access to appropriate stakeholders may prompt research designers to prioritise aspects of the competency development and validation process differently [23, 24]. These challenges may result in variable or uncertain study outcomes that may limit the validity and applicability of the research output as a result [23, 24]. Therefore, experience and lessons learnt from previous management competency studies would be beneficial in guiding future management competency studies in determining research resign and data collection methods and processes. Such learning will contribute to the successful implementation and completion of the studies by incorporating tested strategies in the study design. In addition, such learnings can also provide guidance to increase the applicability and validity of the management competency framework or management competency tool developed. It is also reasonable to assume that using tested methods can decrease the time and cost associating with new competency framework development and maximize the research efforts.
With such purposes in mind, a scoping review on empirical management competency studies was conducted in 2021 in order to answer the following questions:
-
1)
What are the commonly used methods in identifying management competencies? Are there specific considerations on how different methods could achieve competency identification purposes?
-
2)
What are the key learnings and specific strategies adopted that can contribute to the success in management competency studies?
The findings of the review provide guidance for determining the design and implementation of the management competency studies and the application of the identified management competencies.
Methods
Study Design
The scoping review was completed following the five-step process described by Arksey and O’Malley [25] and Levac et al. [26] and reported according to the PRISMA Extension for Scoping Reviews (PRISMA-ScR) [27] and conducted by the authors EK and ZL, and a colleague AH. The review includes studies in both health and non-health context for broader learning.
Paper inclusion criteria
-
Presented results of empirical studies and systematic / scoping / rapid review;
-
Are published in English language since 2000 considering the commencement some major management competency reviews and studies since 2000, and.
-
Are published in a peer-reviewed journal that focus on management competency identification and management competency assessment.
Paper exclusion criteria
-
Opinion pieces and commentaries without linking to empirical evidence,
-
Are not published in English,
-
Are not published in peer reviewed journals, and.
-
Were published prior to year 2000.
-
Papers presented results of systematic / scoping / rapid reviews were excluded from data extraction.
Data source and search strategy
The search strategies were developed by the authors who have both content knowledge and experience in conducting scoping review. Searches in databases were conducted in December 2019 using the following key words or combination of the key words: “competenc*”, “leader*” “head nurses”, “charge nurses”, “directors”, “executives” and “manage*”, including literature from both the health and non-health sectors. Electronic databases such as PubMed, Scopus, Web of Science and Emerald where majority of the management studies are published were initially accessed. An additional snowball search technique such as scanning reference lists to identifying relevant papers was also applied to compliment the search. Details of the search strategies using terms and combination of terms were explained in “Supplementary 1”.
Screening
Search results were imported into the EndNote software (V.X8) with duplications removed. Titles and abstracts of the articles generated by the searches were screened independently by EK and AH leading to the confirmation of potentially relevant articles. Once agreement was reached between EK and AH, full-text review of the articles were performed by EK in accordance with the inclusion criteria. The final decision on papers to be included in data extraction was made on the basis of agreement between EK and AH. Views from ZL were sought to resolve disagreement.
Selection of studies and data extraction
Data were extracted independently by EK and AH from the selected studies using data extraction form developed and pilot tested for each study design. The following information were extracted and entered into the excel spreadsheet prior to the analysis: (A) surname of the first author, (B) year of publication, (C) country of origin, (D) period of data collection, (E) study aims; (F) methods used to develop and identify management competency (G) settings in which studies were conducted, and (H) main findings.
Critical appraisal
In line with the scoping review framework, we did not conduct a critical appraisal on the papers [25].
Data charting and analysis
A data extraction form was developed to organize information, confirm relevance, and to extract study characteristics from included articles. Information collected included study characteristics, objectives of studies, and citations. Relevance was confirmed by sampling population and objectives. Characteristics collected via this form included: author (year), country; sampling population; objective/aim of studies; setting (health sector or non-health sector); methods used; management level. All data were compiled into a single spreadsheet in Microsoft Excel 2013 (Microsoft, Redmond, WA) for coding and analysis.
Results
Study selection
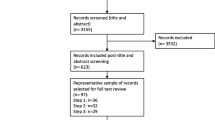
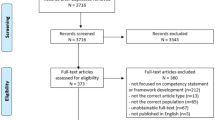
The review process and search results are presented in Fig. 1. In the initial search, 5936 articles were found in the four selected databases by keyword search as explained earlier. Abstract screening resulted in 226 studies being included for full-text review. As a result, 173 studies (excluding 13 review papers) published between 2001 and 2021 were included in data extraction and analysis.

Search and review strategy (PRISMA flow diagram)
Study location
Location of the studies conducted is presented in Fig. 2: 41.4% of the studies were conducted in Asia (n = 77), followed by Europe (19.9%, n = 37) and North America (16.7%, n = 31).

Study location and number of studies
Most of the 186 studies were published in 2019 and 2020. Figure 3 shows an increasing trend in the publication of management competency study, in particular the significant increase since 2019.

Published year and number of studies
Sectors and target population
Amongst the 173 empirical studies, 88 vs. 85 papers presented the studies that were conducted in health and non-health sectors respectively. Target population varied between management levels, management positions and sectors. For studies in the health sectors, close to half of them focused solely on senior or middle management levels or both levels (n = 44); 27 of them on junior or both middle and junior levels, and 17 of them targeted various management levels. On the other hand, for studies conducted in the non-health sectors, 66 out of 85 studies (77%) solely focused on senior and middle management level. The rest were on junior levels and all management levels.
Methods used to identify management competency
Half of the studies (n = 92) adopted mix-methods for data collection. The other 84 studies adopted single-method. Amongst the single-method studies, 45 vs. 36 used quantitative and qualitative approach respectively. Table 1 details the frequency of the eight methods used by the 173 papers (excluding the 13 review papers). The commonest methods used were survey and interviews.
Variation in application of methods/ strategies
Considering the popularity of ‘surveys’ and ‘interviews’ which dominated majority of the management competency studies both in health and non-health sectors, the paper focuses on the actual learnings from these two methods. Learnings include the considerations and preparation put into designing and conducting the studies, and whether different study outcomes in terms of competency identification and development were expected as a result.
To achieve such purposes, the second round of data extraction was performed from studies adopted surveys and interviews as part of the research methods. The data extracted included.
-
Justification of methods chosen;
-
Sampling frame, sampling methods and recruitment strategies;
-
Sampling power, and.
-
Discussions of the generalisibity of results and/or results implications.
Learnings from surveys
Survey was the commonest method used by 110 out of 173 identified studies as either sole method for 44 studies or part of the mix-methods for 66 studies for four main purposes:
-
1)
To confirm competencies identified in other studies and/or test the applicability in their own context;
-
2)
To assess competency level of managers within specific context;
-
3)
To identify core competencies for specific management positions, and.
-
4)
To obtain feedback during the competency identification and competency framework development process.
Overall, 46% of surveys were conducted paper-based (n = 51) and 39% was conducted electronically either using an online platform or via email (n = 43). Ten surveys were conducted both online and face to face [9, 28,29,30,31,32,33,34,35,36]. Six articles did not mention how survey was conducted. Few students opted to conduct the survey on paper because of the concern of low response for online method.
Slightly more than half of the identified studies (n = 59) did not mention methods used to recruit survey participants. Thirty-six studies invited the whole target population for participation and the rest of study selected study participants using two main techniques namely probability sampling (n = 24) and non-probability sampling (n = 23). Random sampling (n = 16) and convenient sampling (n = 11) are the two commonly used sampling methods. Purposeful and snowball sampling was mentioned by 13 studies. Two studies used Census approach and plausibility sampling. One study used two methods purposeful and stratified sampling simultaneously.
All surveys included closed and structured questions to construct questionnaires. Most of the questionnaires used Likert scale with 5-point scale being the commonest (n = 65 or 59.1%). Studies did not normally provide clear justifications of how questionnaire was constructed, why certain Likert scale was used and whether such scale has been validated in studies with similar nature. Survey instrument was pilot tested in 37 of the studies prior to the commencement of the survey.
Sample size greatly varied between studies. Table 2 details the number of studies falls into different sample size ranges.
However, studies generally did not discuss how sample size affected the applicability and generalizability of the results, even the five studies with a response rate lower than 20%. Amongst the 92 studies using survey as one of the mix-methods, 1/3 of them did not report actual response rate. For the rest of the studies, the mean response rate is 69% ranging from 8% [37] to 100% [38,39,40,41,42,43,44] including.
-
25 studies achieved a response rate of 90% or higher [4, 7, 9, 28, 34, 35, 38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56].
-
33 studies achieved a response rate between 50 and 89.9% [2, 30, 57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87], and.
-
6 studies with a response rate less than 20% [37, 88,89,90,91,92].
Only 25% of the papers (n = 27) mentioned or discussed recruitment strategies as the following:
-
Be flexible allowing paper-based survey to supplement the online survey when online survey response rate is lower than planned;
-
Having senior leader to reinforce the importance of the study and encourage participation from their staff;
-
Having the survey open for longer period ( 4 weeks or longer) with multiple reminders via emails or phone calls;
-
Identifying a contact person from each participating organization to assist with the recruitment of survey participants and survey distribution. The contact person usually are senior manager or director of human resources;
-
Minimizing the complexity and length of the questionnaire used for the survey;
-
Mobilizing own professional and social network to recruit additional eligible participants;
-
Recruiting and training clinical staff such as nurses to assist with the implementation of paper-based survey including distribution of questionnaires and collection of the completed questionnaires, and.
-
Reinforcing the anonymous and confidential nature of the survey.
Learning from interviews
In total, 59 out of the 173 studies (34%) used interview as a sole method or part of the mixed method for data collection for the following key purposes:
-
To develop rich understanding of management behavior and performance [4, 9, 20, 29, 36, 37, 39, 54, 58, 61, 63, 66, 74, 79, 80, 86, 93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109];
-
To identify managerial competencies and behaviors that can predict job performance [10,11,12, 20, 39, 54, 58, 61, 66, 74, 80, 94, 98, 104, 106, 108, 110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130];
-
To develop rich understanding of the findings generated from the previous step(s) of the same study [29, 36, 63, 86, 96, 97, 99,100,101,102, 107, 109], and.
-
To gain insight into actual management practices from both managers and stakeholders’ perspectives [4, 9, 37, 79, 93, 95, 103, 105, 131, 132].
Interviews were most commonly designed as in-depth and semi-structured [9,10,11, 36, 37, 39, 58, 61, 93,94,95,96, 100, 101, 103, 106, 109, 111, 114, 120,121,122,123,124, 128,129,130, 132]. Critical incident interviews [80, 102, 112, 113, 128] and behavioral event interviews [12, 86, 105, 116, 127, 131] were also performed. Interviews were conducted online [115], by telephone [63, 98, 115], and face-to-face [10, 11, 39, 58, 79, 86, 109, 114, 120, 125], both online and face-to-face [9, 129], or both telephone and face-to-face [36, 122]. Nine studies did not explicitly outline the form of interviews [20, 66, 74, 97, 103, 104, 107, 108, 126]. Online interviews were conducted in the studies published in 2012, 2019 and 2021.
Several studies (n = 16 studies) mentioned that protocol including pre-determined open questions was developed to guide the interview process. Less than 40% of the studies (23 out of 69) provided adequate details on how interview questions were developed [11, 12, 29, 61, 86, 93,94,95,96, 98, 99, 103, 109, 111, 115, 117, 121, 123, 124, 129, 131, 132]. The following common methods were used to develop interview questions:
-
Adopted an interview guide from other studies, then validated with representatives of target group and made adjustment before implementation, and.
-
Conducting document analysis on policy and government documents and reports;
-
Conducting literature review to identify competencies from other studies;
-
Developed by investigators, then input sought from professional institutions that provide training to the target population;
-
Developing questions with inputs from representatives from target population;
-
Informed by findings of the quantitative data collected in the first phase of the study, and.
-
Using the critical incident technique to gather information about effective and ineffective individual behaviors.
The number of interview participants varied between studies. Forty-two studies interviewed between 10 and 35 participants. Five studies involved more than 35 interviewees (n = 36, 42, 45, 110 and 120 participants) [11, 111, 115, 124, 128]. Eight studies conducted interviews with less than 10 participants [9, 29, 54, 61, 102, 103, 107, 129] including three studies only interviewed three or four participants [9, 54, 129]. Most of the studies did not provide justification of why specific number of interviewees were recruited for the interviews. However, theoretical saturation was one justification mentioned in eight studies.
Discussion
The increasing interest and investment in management competency studies in the past five years confirms the value of the development management competency framework which can serve as valuable resources for guiding the design of training and education curriculum, outlining requirements of a competent workforce and professional development needs, evaluation or assessment of professional expertise [2, 133,134,135,136]. It also confirms that ongoing efforts in refreshing and modifying management competency-based frameworks are required in order to respond to the changing environment or professional needs, minimize lapses in knowledge and skill sets, and ultimately transform education for professions [137]. The increasing interests in management competency studies align with the increasing reinforcement of the role of management competency in service quality and efficiency improvement. The sudden surge of publications in 2020 at the peak of COVID-19 pandemic reinforced the importance of ensuring management competency and capacity development being responsive to the pressing needs of improving health service quality and efficiency.
The aging of the health workforce and the changing healthcare needs and complexity making the delay in effective health workforce development in terms of current workforce upskilling and producing ‘new blood’ impossible [138]. It has been recognised that, in addition to playing a key role in improving service quality and efficiency, managers is critical to leading and managing healthcare transition, and the adoption of innovation is no longer an option, but a most, in order to creating a sustainable healthcare system [139]. The drastic increase in the number of management competency studies conducted in developing countries, in particularly in Asia in the past 10 years proven the necessity of considering learning from past management competency studies, in particularly in the healthcare sectors, when designing its own management competency studies to improve efficiency.
Disregard whether study adopts a single method or mix-methods or using surveys and interviews in data collection, ‘validating’ findings (identified management competencies) from previous studies should be considered to avoid duplication or ‘reinventing the wheel to create something new’. This is backed up by ‘the existence of core management competencies across management levels and sectors’ as suggested in the management literature [13]. The review of previous studies confirmed that ‘validation’ can be considered by both qualitative and quantitative method such interviews and surveys. Questions in survey can be drawn from the findings of management competency studies whilst interview questions were often developed based on prior knowledge which can be gained from literature review, document analysis and validated interview questions from previous studies. Key stakeholder engagement and consultation was also one key strategy in seeking input from target group and professional bodies.
The review confirms the importance of adopting a flexible approach for conducting management competency studies considering the time constraint and high workload demands of health managers. These include the mixture of conducing the questionnaire survey both online and on paper creating flexibility for busy health managers in completing the questionnaire whenever they have a spare moment. COVID-pandemic has changed how health services are provided and how works are completed bounded by the constraint of travel restriction, cross-infection prevention and maintaining social distancing [140]. E-Health, online consultation, holding meetings via online platforms such as zoom have become regular part of our lives [141]. Therefore, it can be predicted that online interviews, online focus groups etc. would be considered as a common process for research data collection. This posted a question of whether qualitative researchers have been equipped with the relevant skills to conduct qualitative studies via online platform where body language was hard to observe and participant engagement is harder to be effective.
Learning from previous studies, survey and interview can contribute to achieving the purposes of the studies differently. Surveys can be used to validate and identify management competency requirements, whilst interviews placed focus on linking management competencies to actual demonstration and performance. Interviews also helped developing understanding of the context in which that management competencies are applied. Management competencies are context sensitive [134, 135], competencies identified via quantitative methods are helpful in developing a guiding framework for understanding competency requirements and development needs. But it is the qualitative method that helps to understand the context in which the competency framework is most applicable to and in what ways that the framework should be used to guide competency development. The popularity of mix-methods used by the identified studies confirms the multiple purposes.
One of the key challenges for conducting management competency studies using quantitative method is successful participant recruitment in achieving a response rate allowing the generalization of result. The identified studies confirmed two important strategies: getting support/buy in from participating organisations and adopting a flexible approach as discussed above. Identifying a liaison person who has credibility and good access to targeted management positions, senior management’s openly providing support to the study, and training nursing staff in providing actual assistance in administering the questionnaire survey are three key strategies. The validity and reliability of the chosen method, the practicability and acceptability to relevant stakeholders including potential research participants are also the considered factors [142]. All of these require advanced planning and relationship building.
Based on the results of the scoping review and the health management competency identification process validated by Liang et al. (2018) [5], the below framework (Fig. 4) is developed that can guide designing and implementing management competency studies in specific country vs. sector context and to ensure benefits of the studies are maximised.

Competency framework development of management in healthcare
The first step in a competency modeling effort is to define the scope and objectives of the study, which includes considering the opportunities to be pursued through the development and application of a competency model. This step is also informed by ‘prior learning (step two) and informs the determination of research design and method for data collection (step three). It is important to consider how will the identified competencies and competency framework be used to guide strategic workforce planning, employee selection, performance management, training and development, succession planning, rewards and recognition, or career planning. The success of management competency studies also rely on the participation and active contribution make by the managers. Therefore, it is important that the ‘two key considerations’ (Step four) are incorporating into the research project design and implementation. Competency requirement for health managers continues to revolve as a response to the rapid transformation of the healthcare system. Efforts in regularly review and update the competency requirements is necessary to ensure the relevance and applicability of the management competency frameworks developed.
The review also identified information critical to study success and accessing the validity and reliability of the study are consistently missing inform the published management competency studies. The information, such as process of constructing survey questions and selecting target population, and recruitment strategies, should be included in research reports and published journal articles as they can allow learning from others to improve future research efficiency and success.
The review found that discussion on how sample size affected the applicability and generalizability of the results and the context in which management competencies are applicable were also often missing. This calls for the review and development of more rigorous guidelines for article peer-reviewed process by journals acting as gate keeper for quality publications and allowing not only the sharing of research results and discussing implications of the studies, but also encouraging lessons to be shared and leant contributing to better research design and research efficiency.
Strengths and Limitations
A strength of this scoping review is that the search strategy was comprehensive with assistance of a skilled research librarian. In addition, a rigorous process was used to determine which articles should be included in the final review. The review was conducted according to PRISMA-ScR guidance. However, there are some limitations of our research that may affect the results and should be addressed. First, quality of the articles was not assessed. Second, this review was restricted to peer-reviewed English papers and did not including books, grey literature, or any documents published in a foreign language. As a result, some evidence might have been excluded. However, this does not inherently bias a review [143].
Conclusions
The development and the use of competency is a complex endeavor. This review identified and explored publications sharing results of management competency identification and management competency framework development in both health and non-health sectors. The review confirmed an increasing trend in investing in management competency study and that the management competency identification and development process varied substantially, in the choice of methods and reporting of the process. Despite the expectations of comprehensive presentation and discussion of study design, implementation strategies and applicability of the research results, some important information are missing from large number of the identified studies limited the learning from experience that is important to improve future research design and research quality. The proposed framework of improving the quality and impact of future management competency studies provides a clear guidance to the process of management competency identification and development that promotes the functional alignment of methods and strategies with intended use and context. In addition, such guidance will assist researchers in determining approaches better-positioned studies to overcome challenges associated with competency framework development.
Data Availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- PRISMA-ScR:
-
PRISMA Extension for Scoping Reviews
References
Howard PF, Liang Z, Leggat S, Karimi L. Validation of a management competency assessment tool for health service managers. J Health Organ Manag. 2018;32(1):113–34.
Liang Z, Blackstock FC, Howard PF, Briggs DS, Leggat SG, Wollersheim D, et al. An evidence-based approach to understanding the competency development needs of the health service management workforce in Australia. BMC Health Serv Res. 2018;18(1):976.
Walston SL, Khaliq AA. The importance and use of continuing education: findings of a national survey of hospital executives. J Health Adm Educ. 2010;27(2):113–25.
Kitreerawutiwong K, Sriruecha C, Laohasiriwong W. Development of the competency scale for primary care managers in Thailand: Scale development. BMC Fam Pract. 2015;16(1):174.
Liang Z, Howard PF, Leggat S, Bartram T. Development and validation of health service management competencies. J Health Organ Manag. 2018;32(2):157–75.
Mohd-Shamsudin F, Chuttipattana N. Determinants of managerial competencies for primary care managers in Southern Thailand. J Health Organ Manag. 2012;26(2):258–80.
Dorji K, Tejativaddhana P, Siripornpibul T, Cruickshank M, Briggs D. Leadership and management competencies required for bhutanese primary health care managers in reforming the district health system. J Healthc Leadersh. 2019;11:13.
Pihlainen V, Kivinen T, Lammintakanen J. Experts’ perceptions of management and leadership competence in finnish hospitals in 2030. Leadersh Health Serv. 2019;32(2):280–95.
Gunawan J, Aungsuroch Y, Fisher ML, McDaniel AM. Development and psychometric properties of managerial competence scale for first-line nurse managers in Indonesia. SAGE Open Nursing. 2019;5:2377960819831468.
Luo WY, Shen NP, Lou JH, He PP, Sun JW. Exploring competencies: a qualitative study of chinese nurse managers. J Nurs Adm Manag. 2016;24(1):E87–E94.
Sherman RO, Bishop M, Eggenberger T, Karden R. Development of a leadership competency model. JONA: The Journal of Nursing Administration. 2007;37(2):85–94.
Sudirman I, Siswanto J, Monang J, Aisha AN. Competencies for effective public middle managers.Journal of Management Development. 2019.
Isouard G, Martins JM, Friedman LH. Competency in innovation, creative and innovative thinking: challenges within the health management course curriculum. J Health Adm Educ. 2015;32(3):257–69.
Brownell J. Leading on land and sea: competencies and context. Int J Hospitality Manage. 2008;27(2):137–50.
Pye A. Management competence in the public sector. Public Money & Management. 1988;8(4):62–4.
Robotham D, Jubb R. Competences: measuring the unmeasurable. Manage Dev Rev. 1996;9(5):25–9.
Epstein RM, Hundert EM. Defining and assessing professional competence. JAMA. 2002;287(2):226–35.
Çitaku F, Violato C, Beran T, Donnon T, Hecker K, Cawthorpe D. Leadership competencies for medical education and healthcare professions: population-based study. BMJ open. 2012;2(2):e000812.
Moaveni A, Gallinaro A, Conn LG, Callahan S, Hammond M, Oandasan I. A Delphi approach to developing a core competency framework for family practice registered nurses in Ontario. Nurs Leadersh. 2010;23(4):45–60.
Barati O, Sadeghi A, Khammarnia M, Siavashi E, Oskrochi G. A qualitative study to identify skills and competency required for hospital managers. Electron physician. 2016;8(6):2458.
Pillay R. Defining competencies for hospital management: a comparative analysis of the public and private sectors. Leadersh Health Serv. 2008;21(2):99–110.
Van Tuong P, Thanh ND. A Leadership and Managerial Competency Framework for Public Hospital Managers in Vietnam. AIMS public health. 2017;4(4):418.
Marrelli AF, Tondora J, Hoge MA. Strategies for developing competency models. Adm Policy Mental Health Mental Health Serv Res. 2005;32(5–6):533–61.
Batt AM, Tavares W, Williams B. The development of competency frameworks in healthcare professions: a scoping review. Adv Health Sci Educ. 2019;25:913–87.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):69.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
Liang Z, Howard P, Wang J, Xu M, Zhao M. Developing senior hospital managers: does ‘one size fit all’?–evidence from the evolving chinese health system. BMC Health Serv Res. 2020;20:1–14.
Abdullah AH, Yaman SK, Mohammad H, Hassan PF. Construction manager’s technical competencies in malaysian construction projects. Eng Constr Architectural Manage. 2018;25(2):153–77.
Khadka DK, Gurung M, Chaulagain N. Managerial competencies–A survey of hospital managers’ working in Kathmandu valley. Nepal J Hosp Adm. 2014;3(1):62–72.
Koenigsfeld JP, Kim S, Cha J, Perdue J, Cichy RF. Developing a competency model for private club managers. Int J Hospitality Manage. 2012;31(3):633–41.
Marneros S, Papageorgiou G, Efstathiades A. Identifying key success competencies for the hospitality industry: the perspectives of professionals.Journal of Teaching in Travel & Tourism. 2020:1–25.
Shah MN, Prakash A. Developing generic competencies for infrastructure managers in India. Int J Managing Projects Bus. 2018;11(2):366–81.
Suh E, West JJ, Shin J. Important competency requirements for managers in the hospitality industry. J hospitality leisure sport tourism Educ. 2012;11(2):101–12.
Liang Z, Howard P, Wang J, Xu M. A call for leadership and management competency development for directors of medical services—evidence from the chinese public hospital system. Int J Environ Res Public Health. 2020;17(18):6913.
Dey R, Subramanian V, Pereira A. Competencies required for Channel sales executives in the Present indian FMCG & consumer durables Sector. Manage Quest. 2020;3(1):50–70.
Burgess C. Managerial competencies for UK Hotel Financial Controllers: are they hospitality managers or Accountants? J Hospitality Financial Manage. 2017;25(1):27–43.
Al Ansari H, al Khadher O. Developing a leadership competency model for library and information professionals in Kuwait. Libri. 2011;61(3):239–46.
Anh DVP, Hung TH. Building competence frameworks for Vietnam Middle Management in the Hotel industry. VNU J Science: Econ Bus. 2019;35(2):62–74.
AwadAllah M, Salem G. Managerial competencies of primary Health Care Managers. Egypt J Occup Med. 2021;45(1):35–46.
Gonçalves FHL, Batista RCS, Piffer V. Essential Managerial Skills for Brazilian Micro and Small Business Managers.International Journal of Business Administration. 2020;11(3).
Lopes AG, Narattharaksa K, Siripornpibul T, Briggs D. An assessment of management competencies for primary health care managers in Timor-Leste. Int J Health Plann Manag. 2020;35(2):520–31.
Tabassi AA, Roufechaei KM, Ramli M, Bakar AHA, Ismail R, Pakir AHK. Leadership competences of sustainable construction project managers. J Clean Prod. 2016;124:339–49.
Van Vo B, Sunantiwat M, Pumtong S, Vo TQ, Anuratpanich L. Perceptions of managerial competency among Pharmacy Department heads in vietnamese hospitals. Syst Reviews Pharm. 2020;11(2):422–6.
Dikic M, Nikolic D, Todorovic J, Terzic-Supic Z, Kostadinovic M, Babic U, et al. editors. Alignment of Perceived Competencies and Perceived Job Tasks among primary care managers. Healthcare: Multidisciplinary Digital Publishing Institute; 2020.
Gunawan J, Aungsuroch Y, Fisher ML, McDaniel AM, Marzilli C. Perceived Managerial Competence of First-Line Nurse Managers: A Comparative Analysis Among Public Hospitals. Policy, Politics, & Nursing Practice. 2020:1527154420926616.
Hamze M, Keshkar S. Investigating the managers’ competency of Sports and Youth offices in Alborz. J New Stud Sport Manage. 2020;1(1):22–9.
Howard PF, Liang Z, Leggat S, Karimi L. Validation of a management competency assessment tool for health service managers.Journal of Health Organization and Management. 2018.
Liang Z, Howard PF, Leggat SG. 360° management competency assessment: is our understanding adequate? Asia Pac J Hum Resour. 2017;55(2):213–33.
Munyewende PO, Levin J, Rispel LC. An evaluation of the competencies of primary health care clinic nursing managers in two south african provinces. Global health action. 2016;9(1):32486.
Ofei AMA, Paarima Y, Barnes T. Management competencies of nurse managers in Greater Accra.International Journal of Africa Nursing Sciences. 2020:100248.
Paarima Y, Kwashie AA, Ofei AMA. Financial management skills of nurse managers in the Eastern Region of Ghana. Int J Afr Nurs Sci. 2021;14:100269.
Sharma P, Pandher JS. Competences desired among educational leaders of technical education degree institutions. J Workplace Learn. 2019;31(6):377–90.
Tongmuangtunyatep K, Kunaviktikul W, Nantsupawat R, Akkadechanunt T. Development of a competency in Community Hospitals. Pac Rim Int J Nurs Res. 2015;19(2):122–34.
Varajão J, Silva H, Pejic-Bach M. Key competences of Information Systems Project Managers. Int J Inform Technol Project Manage (IJITPM). 2019;10(3):73–90.
Yang L, Cui D, Zhu X, Zhao Q, Xiao N, Shen X. Perspectives from nurse managers on informatics competencies.The Scientific World Journal. 2014;2014.
Abou-Hafs H, Boutora F, Smaili N. Identification and classification of the key competencies for social project managers in Agadir, Morocco.Archives of Business Research. 2019;7(5).
Agut S, Grau R, Peiró JM. Competency needs among managers from spanish hotels and restaurants and their training demands. Int J Hospitality Manage. 2003;22(3):281–95.
Ahadzie D, Proverbs D, Sarkodie-Poku I. Competencies required of project managers at the design phase of mass house building projects. Int J Project Manage. 2014;32(6):958–69.
Arditi D, Gluch P, Holmdahl M. Managerial competencies of female and male managers in the swedish construction industry. Constr Manage Econ. 2013;31(9):979–90.
Blixt C, Kirytopoulos K. Challenges and competencies for project management in the australian public service. Int J Public Sector Manag. 2017;30(3):286–300.
Cha J, Maytorena-Sanchez E. Prioritising project management competences across the software project life cycle.International Journal of Managing Projects in Business. 2019.
Chan B, Coleman M. Skills and competencies needed for the Hong Kong hotel industry: the perspective of the hotel human resources manager. J Hum Resour Hospitality Tourism. 2004;3(1):3–18.
Gunawan J, Aungsuroch Y, Fisher ML, McDaniel AM. Comparison of managerial competence of indonesian first-line nurse managers: a two-generational analysis. J Res Nurs. 2020;25(1):5–19.
Gunawan J, Aungsuroch Y, Fisher ML, McDaniel AM, Marzilli C. Managerial competence of first-line nurse managers in Public Hospitals in Indonesia. J Multidisciplinary Healthc. 2020;13:1017.
Horch H-D, Schütte N. Competencies of sport managers in german sport clubs and sport federations. Managing Leisure. 2003;8(2):70–84.
Jo Dolasinski M, Reynolds J. Hotel leader competencies: industry practitioner perspectives. J Hum Resour Hospitality Tourism. 2019;18(3):349–67.
Kakemam E, Dargahi H. Competencies gap in Hospital Management in Tehran, Iran: a cross-sectional survey. J Health Manage. 2019;21(4):451–64.
Kalhor R, Tajnesaei M, Kakemam E, Keykaleh MS, Kalhor L. Perceived hospital managerial competency in Tehran, Iran: is there a difference between public and private hospitals? J Egypt Public Health Assoc. 2016;91(4):157–62.
Kantanen K, Kaunonen M, Helminen M, Suominen T. The development and pilot of an instrument for measuring nurse managers’ leadership and management competencies. J Res Nurs. 2015;20(8):667–77.
Karathanasi K, Prezerakos P, Maria M, Siskou O, Kaitelidou D. Operating room nurse manager competencies in greek hospitals. Clin Nurs Stud. 2014;2(2):16–29.
Kwofie TE, Adinyira E, Botchway EA. Identification of the critical project management competencies of architects in the ghanaian construction industry. Int J Constr Manage. 2015;15(4):288–98.
Lakshminarayanan S, Pai YP, Ramaprasad BS. Competency need assessment: a gap analytic approach.Industrial and Commercial Training. 2016.
MacKinnon NJ, Chow C, Kennedy PL, Persaud DD, Metge CJ, Sketris I, editors. Management competencies for canadian health executives: views from the field. Healthcare Management Forum. Los Angeles, CA: SAGE Publications Sage CA; 2004.
Maraouch F. Professional profile and management competencies in the lodging industry. J Hum Resour Hospitality Tourism. 2020;19(4):496–519.
Moradi S, Kähkönen K, Klakegg OJ, Aaltonen K. A competency model for the selection and performance improvement of Project Managers in Collaborative Construction Projects: behavioral studies in Norway and Finland. Buildings. 2021;11(1):4.
Pillay R. Defining competencies for hospital management. Leadersh Health Serv. 2008;21(2):99–110.
Pillay R. Managerial competencies of hospital managers in South Africa: a survey of managers in the public and private sectors. Hum Resour Health. 2008;6(1):4.
Priyangika K, Perera B, Wickremanayake Karunaratne TL. Facilities Management Roles in the Hotel industry: the Skills and Competencies required. J Qual Assur Hospitality Tourism. 2020;21(4):454–73.
Qiao JX, Wang W. Managerial competencies for middle managers: some empirical findings from China.Journal of European Industrial Training. 2009.
Shum C, Gatling A, Shoemaker S. A model of hospitality leadership competency for frontline and director-level managers: which competencies matter more? Int J Hospitality Manage. 2018;74:57–66.
Skytt B, Carlsson M, Ljunggren B, Engström M. Psychometric testing of the Leadership and Management Inventory: a tool to measure the skills and abilities of first-line nurse managers. J Nurs Adm Manag. 2008;16(7):784–94.
Tuong P, Thanh ND. A Leadership and Managerial Competency Framework for Public Hospital Managers in Vietnam. AIMS public health. 2017;4(4):418.
Wang Y-F. Constructing career competency model of hospitality industry employees for career success.International Journal of Contemporary Hospitality Management. 2013.
Wisittigars B, Siengthai S. Crisis leadership competencies: the facility management sector in Thailand. Facilities. 2019;37(13/14): 881 – 96.
Wong SC, Lee PC. Competencies of training professionals in the Hong Kong hotel industry. J Hum Resour Hospitality Tourism. 2017;16(4):384–400.
Zhang F, Zuo J, Zillante G. Identification and evaluation of the key social competencies for chinese construction project managers. Int J Project Manage. 2013;31(5):748–59.
Fjelstul J, Tesone DV. Golf and club entry level management competencies.International Journal of Contemporary Hospitality Management. 2008.
Gilgeous V, Parveen K. Core competency requirements for manufacturing effectiveness.Integrated Manufacturing Systems. 2001.
Lehtonen M-R, Roos M, Kantanen K, Suominen T. International nursing: nurse managers’ Leadership and Management Competencies assessed by nursing personnel in a finnish hospital. Nurs Adm Q. 2018;42(2):164–74.
Sisson LG, Adams AR. Essential hospitality management competencies: the importance of soft skills. J Hospitality Tourism Educ. 2013;25(3):131–45.
Thai V, Ibrahim KB, Ramani V, Husng H-Y. Competency profile of managers in the Singapore logistics industry. Asian J Shipping Logistics. 2012;28(2):161–82.
Alberton A, Kieling AP, Lyra FR, Hoffmann EM, Lopez MPV, Stefano SR. Competencies for sustainability in hotels: insights from Brazil.Employee Relations: The International Journal. 2020.
Carstens JG, De Kock FS. Firm-level diversity management competencies: development and initial validation of a measure. Int J Hum Resource Manage. 2017;28(15):2109–35.
Erjavec K, Starc J. Competencies of nurse managers in Slovenia: a qualitative and quantitative study. Cent Eur J Nurs Midwifery. 2017;8(2):632–40.
Esser A, Kahrens M, Mouzughi Y, Eomois E. A female leadership competency framework from the perspective of male leaders.Gender in Management: An International Journal. 2018.
Lan MT, Hung TH. The Leadership Competency in Vietnam Public Administration. Organ Markets Emerg Economies. 2018;9(1):8–20.
Liang Z, Howard PF. Competencies required by senior health executives in New South Wales, 1990–1999. Aust Health Rev. 2010;34(1):52–8.
Lockhart W, Backman A, editors. Health care management competencies: identifying the gaps. Healthcare Management Forum. Los Angeles, CA: SAGE Publications Sage CA; 2009.
Melaia S, Abratt R, Bick G. Competencies of marketing managers in South Africa. J Mark Theory Pract. 2008;16(3):233–46.
Moradi S, Kähkönen K, Aaltonen K. Project managers’ Competencies in Collaborative Construction Projects. Buildings. 2020;10(3):50.
Oberländer M, Beinicke A, Bipp T. Digital competencies: a review of the literature and applications in the workplace. Comput Educ. 2020;146:103752.
Okonkwo U, Ekpeyoung B, Ndep A. Perceived important managerial competencies for healthcare managers at a tertiary healthcare institution in Calabar, Cross River State, Nigeria.Journal of Hospital Administration. 2020;9(1).
Sohmen VS, Dimitriou CK. Ten core competencies of program managers: an empirical study. Int J Health Economic Dev. 2015;1(1):1.
Wang X, Gao J, Xie X. A study to develop a competency model for chinese EHS managers. Front Bus Res China. 2011;5(4):580–96.
Yarbrough Landry A, Stowe M, Haefner J. Competency assessment and development among health-care leaders: results of a cross-sectional survey. Health Serv Manage Res. 2012;25(2):78–86.
Koustelios A. Identifying important management competencies in fitness centres in Greece. Managing Leisure. 2003;8(3):145–53.
Pihlainen V, Kivinen T, Lammintakanen J. Experts’ perceptions of management and leadership competence in Finnish hospitals in 2030.Leadership in Health Services. 2019.
Nuwan P, Perera B, Dewagoda K. Development of Core Competencies of Construction Managers: The Effect of Training and Education. Technology, Knowledge and Learning. 2020:1–40.
Brière S, Proulx D, Flores ON, Laporte M. Competencies of project managers in international NGOs: perceptions of practitioners. Int J Project Manage. 2015;33(1):116–25.
Connelly LM, Yoder UH, Miner-Williams D. A qualitative study of charge nurse competencies. Medsurg Nurs. 2003;12(5):299.
Darling SD, Cunningham JB. Underlying values and competencies of public and private sector managers. Asian Education and Development Studies; 2016.
Ekaterini G. A qualitative approach to middle managers’ competences.Management research review. 2011.
Naranjee N, Sibiya MN, Ngxongo TSP. Development of a financial management competency framework for nurse managers in public health care organisations in the province of KwaZulu-Natal, South Africa. Int J Afr Nurs Sci. 2019;11:100154.
Testa MR, Sipe L. Service-leadership competencies for hospitality and tourism management. Int J hospitality Manage. 2012;31(3):648–58.
Vathanophas V. Competency requirements for effective job performance in thai public sector. Contemp Manage Res. 2007;3(1):45.
Wongprasit N. The leadership competencies model of private hospital directors in Thailand. HRD J. 2014;4(1):72–85.
Xiao Y, Liu J, Pang Y. Development of a competency model for real-estate project managers: case study of China. Int J Constr Manage. 2019;19(4):317–28.
Som RM, Omar Z, Ismail IA, Alias SN. Understanding leadership roles and competencies for public-private partnership. J Asia Bus Stud. 2020;14(4):541–60.
Moradi F, Ziapour A, Abbas J, Baharirad N. Hospital managers skills required and onward challenges: a qualitative study. Journal of Education and Health Promotion; 2020.
Kainuma M, Kikukawa M, Nagata M, Yoshida M. Competencies necessary for becoming a leader in the field of community medicine: a Japanese qualitative interview study.BMJ open. 2018;8(4).
Harrison R, Meyer L, Chauhan A, Agaliotis M. What qualities are required for globally-relevant health service managers? An exploratory analysis of health systems internationally. Globalization and health. 2019;15(1):1–8.
Barkhordari-Sharifabad M, Ashktorab T, Atashzadeh-Shoorideh F. Ethical competency of nurse leaders: a qualitative study. Nurs Ethics. 2016;25(1):20–36.
Cappellen T, Janssens M. Global managers’ career competencies. Career Dev Int. 2008;13(6):514–37.
Tironi NM, Bernardino E, Haddad MdCL, Nimtz MA, Torres DG, Peres AM. Assignments and competencies of nursing managers: a descriptive exploratory research. Online Brazilian Journal of Nursing. 2017;16(2):130–9.
Ab Wahab M, Awang M, Mohsin A, Anthony Jiram WR, Adawiyah SR, Abdul Rahman MS. Competencies framework for the property manager of shopping malls. Int J Sci Technol Res. 2020;9(1):2246–9.
Dreyfus CR. Identifying competencies that predict effectiveness of R&D managers. J Manage Dev. 2008;27(1):76.
Daouk-Öyry L, Sahakian T, van de Vijver F. Evidence‐Based Management Competency Model for Managers in Hospital Settings.British Journal of Management. 2020.
Marques I, Serrasqueiro Z, Nogueira F. Managers’ Competences in private hospitals for investment decisions during the COVID-19 pandemic. Sustainability. 2021;13(4):1757.
Mojar AKS, Depositario DPT. An exploratory study on the Managerial Competencies of First-Line managers in a Philippine University. J Econ Manage Agricultural Dev. 2020;6(2390–2021–960):17–34.
Kim DH, Fitchett G, Anderson JL, Garman AN. Management and leadership competencies among spiritual care managers.Journal of Health Care Chaplaincy. 2020:1–10.
Mahbanooee B, Gholipour A, Aboyee AM. A competency model for general health managers (case: Iran medical of health and education). Iran J Manage Stud. 2016;9(2):217–41.
Janke KK, Traynor AP, Boyle CJ. Competencies for student leadership development in doctor of pharmacy curricula to assist curriculum committees and leadership instructors. Am J Pharm Educ. 2013;77(10):222.
Campion MA, Fink AA, Ruggeberg BJ, Carr L, Phillips GM, Odman RB. Doing competencies well: best practices in competency modeling. Pers Psychol. 2011;64(1):225–62.
Graafland M, Ten Cate O, van Seventer J-P, Schraagen JMC, Schijven MP. Mapping the demand for serious games in postgraduate medical education using the entrustable professional activities framework. Games for health journal. 2015;4(5):381–6.
Mann JE, Amerine LB, Waldron K, Wolcott MD, McLaughlin JE. Pharmacist perceptions of competency: identifying priority areas for a competency program development at an academic medical center. Res Social Administrative Pharm. 2018;14(6):595–602.
Miller BM, Moore DE Jr, Stead WW, Balser JR. Beyond Flexner: a new model for continuous learning in the health professions. Acad Med. 2010;85(2):266–72.
Strudwick G, Nagle LM, Morgan A, Kennedy MA, Currie LM, Lo B, et al. Adapting and validating informatics competencies for senior nurse leaders in the canadian context: results of a Delphi study. Int J Med Informatics. 2019;129:211–8.
Lee P, Abernethy A, Shaywitz D, Gundlapalli AV, Weinstein J, Doraiswamy PM, et al. Digital Health COVID-19 Impact Assessment: Lessons learned and compelling needs. NAM Perspect. 2022;2022:1–34.
Sheikhbardsiri H, Raeisi AR, Nekoei-Moghadam M, Rezaei F. Surge capacity of hospitals in emergencies and disasters with a preparedness approach: a systematic review. Disaster Med public health preparedness. 2017;11(5):612–20.
Kun A, Shaer O, Iqbal S. The future of work: COVID-19 and Beyond. IEEE Pervasive Comput. 2021;20(04):7–8.
Nuwan P, Perera B, Dewagoda K. Development of Core Competencies of Construction Managers: The Effect of Training and Education. Technology, Knowledge Learning. 2021;26(4):945 – 84.
Morrison A, Polisena J, Husereau D, Moulton K, Clark M, Fiander M, et al. The effect of English-language restriction on systematic review-based meta-analyses: a systematic review of empirical studies. Int J Technol Assess Health Care. 2012;28(2):138–44.
Acknowledgements
The authors would like to thank Dr Alireza Hajizadeh (PhD Candidate, Tehran University of Medical Sciences) for assistance with search consulting.
Funding
This study did received any form of funding.
Author information
Authors and Affiliations
Contributions
ZL and EK were responsible for the conception and design of the study. EK was responsible for the search, screening, inclusion of relevant articles, data extraction of eligible studies with assistance from colleague mentioned in the acknowledgement. EK was responsible for the initial drafting of the introduction, method and result sections of the manuscript. ZL was responsible for developing the discussion section, providing substantial revision and editing of, and the proof read the complete manuscript. Both EK and ZL approved the final version before submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kakemam, E., Liang, Z. Guidance for management competency identification and development in the health context: a systematic scoping review. BMC Health Serv Res 23, 421 (2023). https://doi.org/10.1186/s12913-023-09404-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09404-9