
Abstract
Background
Stratified care approach involving use of the STarT-Back tool to optimise care for patients with low back pain is gaining widespread attention in western countries. However, adoption and implementation of this approach in low-and-middle-income countries will be restricted by context-specific factors that need to be addressed. This study aimed to develop with physiotherapists, tailored intervention strategies for the implementation of stratified care for patients with low back pain.
Methods
A two-round web-based Delphi survey was conducted among purposively sampled physiotherapists with a minimum of three years of clinical experience, with post-graduation certification or specialists. Thirty statements on barriers and enablers for implementation were extracted from the qualitative phase. Statements were rated by a Delphi panel with additional open-ended feedback. After each Delphi round, participants received feedback which informed their subsequent responses. Additional qualitative feedback were analysed using qualitative content analysis. The criteria for consensus and stability were pre-determined using percentage agreement (≥ 75%), median value (≥ 4), Inter-quartile range (≤ 1), and Wilcoxon matched-pairs test respectively.
Results
Participants in the first round were 139 and 125 of them completed the study, yielding a response rate of 90%. Participants were aged 35.2 (SD6.6) years, and 55 (39.6%) were female. Consensus was achieved in 25/30 statements. Wilcoxon’s test showed stability in responses after the 5 statements failed to reach consensus: ‘translate the STarT-Back Tool to pidgin language’ 71% (p = 0.76), ‘begin implementation with government hospitals’ 63% (p = 0.11), ‘share knowledge with traditional bone setters’ 35% (p = 0.67), ‘get second opinion on clinician’s advice’ 63% (p = 0.24) and ‘carry out online consultations’ 65% (p = 0.41). Four statements strengthened by additional qualitative data achieved the highest consensus: ‘patient education’ (96%), ‘quality improvement appraisals’ (96%), ‘undergraduate training on psychosocial care’ (96%) and ‘patient-clinician communication’ (95%).
Conclusion
There was concordance of opinion that patients should be educated to correct misplaced expectations and proper time for communication is vital to implementation. This communication should be learned at undergraduate level, and for already qualified clinicians, quality improvement appraisals are key to sustained and effective care. These recommendations provide a framework for future research on monitored implementation of stratified care in middle-income countries.
Similar content being viewed by others

Introduction
Low back pain (LBP) is highly prevalent and substantially increasing globally as the population ages. LBP cuts across national and socio-economic boundaries [1,2,3] and it is a leading cause of disability that has significant impact on productivity and personal life [1, 2]. Despite treatment efforts, many acute LBP cases turn chronic, and the prevalence and recurrence levels remain high, even exponentially increasing [3, 4]. Research shows that there is a presence of psychosocial risk factors in over 60% of patients with chronic non-specific LBP which further impedes outcome [5].
Research has shown that standardized risk-specific stratified treatment approaches could be superior to traditional physiotherapy approaches for patients with LBP [6,7,8]. These studies recognise the heterogeneous population of patients with LBP and recommend the creation of patient prognostic profiles based on potential individual responses to specific treatments [8]. Further recommendations on management strategies integrate physical and psychological treatment approaches to address psychosocial risk factors and reduce other obstacles to recovery [9, 10].
Stratified care (SC), is an approach that involves differentiating and targeting prognostic subgroups, aligning the risk of an unfavourable treatment outcome with specific evidence-based treatment procedures [11, 12]. It is described as best practice in multiple international guidelines [13, 14]. A comprehensively evaluated procedure is the Subgroups for Targeted Treatment (STarT-Back) approach. It has shown the potential to improve treatment outcomes, patient and clinician satisfaction and reduce the cost burden [15,16,17].
The STarT-Back tool (SBT) is one of several tools developed, translated and cross-culturally adapted to assist this prognostic profiling [18, 19]. The method of stratification using SBT is unique because it matches specific treatments to subgroups of patients with similar characteristics i.e. complex prognostic factors, categorising patients into low, medium or high risk subgroups [15]. Patients with LBP in the low-risk subgroup receive care involving reassurance, medication and self-management advice to discourage other speciality treatments including x-ray requests; patients in the medium-risk subgroup, receive support using evidence-based conservative treatments offered by physiotherapists, further preventive measures against future LBP related disability and for patients in the high-risk subgroup, psychologically informed physiotherapy treatment (PIP) [20]. The STarT-Back (SB) approach borrows these components of self-management and patient-centred approach principles in a bid to provide more tailored treatment and optimize LBP outcomes [20].
Identifying prognostic subgroups of patients and allocating specific treatment content as recommended is currently not utilized in low/medium resource countries like Nigeria when planning treatment [21]. There are well-known and available evidence-based treatment methods such as exercises, manual therapy and analgesic medications [22,23,24,25,26]. In spite of this, the general physiotherapy approach to the treatment of LBP in low-medium income countries involves a variety of largely non-evidence based modalities. One study reported heat therapy was most commonly used for 1 in every 2 cases, followed by exercise therapy and then education/advice which was not only significantly low in frequency but included education on the diagnosis of LBP and reducing activities for sufferers [27]. These methods are used in combination or separately to treat patients with LBP [28]. Treatment modality, intensity and duration are not influenced by prognostic factors and strict use of guidelines is not popular [29]. For a large percentage of the rural population, there is also the practice of traditional bone setting; a ‘method of traditional medicine’ learned by apprenticeship and using herbs and roots for treatment and pain relief. The reported high patronage (> 70%) is due to the immense faith placed on them by the people, its relatively low cost and easy access [30].
This might be in contrast to high-income countries where more advanced care options with broader applications are available as mainstream or adjunct care options for LBP and its complications or related comorbidities [31,32,33]. Since LBP is a complex multi-faceted phenomenon, it benefits from multimodal interventions some of which might be unavailable in low/medium resource countries [25].
Recent studies reveal that using the SC model enhances practice and garnered a positive perception among clinicians, patients and general practitioners. It also reveals contextual concerns that might serve as barriers to implementation such as time constraints, treatment expectations held by patients regarding the method and success of approach and the incentivised tradition of practice. These studies reveal potential facilitators like communication, patients’ trust and socio-cultural factors with the potential to accentuate implementation [17, 34].
There still exists the need for developing consensus on strategies that can be adopted for a tailored implementation of SC for LBP among physiotherapists in low-medium income countries. Studies have recommended that for tailoring interventions, a stepwise process should be adopted [35, 36]. This involves first identifying the determinants affecting implementation, then developing strategies for utilising facilitators and overcoming barriers by consensus [35]. This study aims to identify tailored strategies, approaches and adaptations to address barriers and promote enablers to the implementation of SC with Nigerian physiotherapists.
Materials and methods
The Web-based Delphi technique chosen for this study is a structured iterative process that provides an accurate synthesis of opinions gathered from panellists through multiple rounds aiming for group consensus [37, 38]. The key components are anonymity and iterative feedback to participants [39]. This procedure was chosen because of the comparative advantage it offers in gathering subjective information from a group of panellists on a particular subject and is especially reliable when they are not physically present [40]. This Delphi study took place from November 2021 to July 2022.
Participants
The participants were a panel of physiotherapists sampled following the criteria for panellists described by Hora [41] and Trevelyan [42]. Based on this, the inclusion criteria allowed physiotherapists with a minimum of 3 years of clinical experience, with postgraduate degrees or Continuous Professional Development courses (CPDs) and available and willing to participate in the study throughout its entire duration. All participants were physiotherapists licenced, registered above 18 years and practicing in Nigeria. Physiotherapists who did not meet any of the panellist requirements in this study were excluded. An expected sample size of 60 participants was planned for this study providing sufficiently representative data for the targeted heterogeneous population [37], fitting to the aim of the study and allowing for attrition as exemplified by similar research studies [43, 44].
Potential participants who met the baseline inclusion criteria were contacted via email. These physiotherapists were registered with the regulatory board of physiotherapists, had completed a recognised training programme, and working in Nigeria. Potential participants received a recruitment link, explaining the Delphi process and its objectives [37]. They were also informed about the study, anonymity and requested to confirm their qualification on each of the inclusion criteria before consenting to the study. An incentive of 2 Euro worth of phone credit vouchers was provided to reduce the attrition rate as recommended in the literature [45].
Data collection
Procedure
Potential participants were invited to a nationwide interactive physiotherapy webinar on stratified care to stimulate their interest. They were further informed about stratified care via tailored interactive videos before participation. This included the rationale for SB approach, psychosocial barriers to recovery, using and scoring the SB Tool and matched treatments, scientific underpinning of the approach, clinical and economic benefits of the SB approach obtained from literature [11, 12, 15].
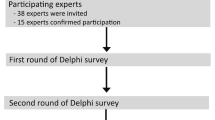
A preliminary round (see Fig. 1) was carried out as recommended in the literature as a feature of Delphi studies when sufficient content is not available from previous studies as it improves responses and reduces dropout [38, 46, 47]. It was a semi-structured telephone interview, exploring barriers and enablers to implementation of stratified care. Interviews were audio recorded, transcribed and analysed using Grounded theory [48] generating categories and sub-categories used in the Delphi rounds (Additional file 1). This preliminary round was described in detail in a published manuscript [34].

Data collection procedure. Legend: SC: Stratified Care; IQR: Inter-quartile range
Round 1:After a recruitment phase, round 1 was carried out. The aim of this round was to investigate the level of agreement on statements derived from the qualitative preliminary round. Participants who responded to the recruitment email were contacted for this round. The survey was presented to participants via an online link for rating according to their level of agreement. Qualitative feedback options were provided for participants to give additional strategies.
Round 2:After analysis of round 1 data, round 2 questionnaire was developed and distributed. This round aimed to investigate the level of agreement between the participants regarding the aspects of the previous phase. This was sent only to participants who responded to the first round [49]. Participants were urged to reconsider their original responses and rate the statements in the light of the feedback from the first round and grade again. At each stage, participants were free to change their opinions if they wish and were given the possibility to explain the reasons if any. The criteria for Stability and consensus were considered.
In both rounds, non-responders were reminded via email one week and 2 days before the deadline. Participants were blinded to each other but known to the researcher, however, contact was provided for private feedback and participants were given 5 weeks to complete this round. There was a period of 4 weeks interval between rounds.
Questionnaire design
The questionnaire was derived from perceived barriers and enablers to implementing stratified care identified in the preliminary round with additional opinions provided by participants (Fig. 1). Terminologies from the preliminary round were maintained as closely as possible to reflect the original content suggested by participants [37]. To fulfil the criteria for an acceptable validation process in a Delphi study [50], statements selected to make up the questionnaire were structured following the recommendations for word count and complexity [51].
These statements were further prepared for grading on a 5-point Likert scale (from ‘strongly disagree’ to ‘strongly agree’) with a neutral midpoint option, ascending response options, fully labelled response options, response options in a horizontal format provided to participants as recommended and merged with open-ended questions allowing the participants freedom to bring fresh views [45].
To ease comprehension, statements with similar ideas making up the questionnaire were classed together forming three categories; i) strategies to best modify stratified care management to fit the National context, ii) views on how training and education can best be done to help the implementation of stratified care, iii) ideas on conditions necessary to enhance the implementation of stratified care nationally. The questionnaire was then reviewed for language, content and sequencing by the research team consisting of physiotherapists with experience in SC and Delphi methodology.
The final resulting questionnaire made up of 30 statements hosted on an online survey platform [52] was pilot-tested with five individuals using the Think-aloud method [53]. During this piloting process, the participants were asked to have feasibility and importance in mind while responding to the questions. Hence the questionnaire was further modified to contain these components before presentation to the panellists in Round 1 of the Delphi process.
For the second Delphi round, the questionnaire from round 1 was further modified based on the previous responses. This contained all thirty questions in the same classification as the previous phase and a statistical summary of answers with the possibility to provide further comments. This was based on recommendations from literature to ‘help motivate panel’ as they see that the process actually worked also giving participants the opportunity to reflect on their previous judgement [37, 42].
Data analysis
Rounds 1 and 2: Descriptive statistics were employed to present participants' sociodemographic data. For participants responses to statements, pre-set measures of central tendency (median) and measures of dispersion (Interquartile range-IQR) were employed. To calculate the median and IQR, the response options were assigned numerical values. For the options 1 to 6 in ascending order, the numerical values were; ‘strongly disagree’ (1), ‘disagree’ (2), ‘neutral’ (3), ‘agree’ (4), ‘strongly agree’ (5), ‘no opinion’ (0). Wilcoxon matched-pairs signed rank test was used to determine the degree of stability for each round [54]. Statistical results of each phase were fed back to participants. Qualitative data from the additional opinions were analysed using qualitative content analysis [55].
Inter-round stability and consensus were considered suitable termination criteria as recommended in literature [56]. Inter-round stability was considered based on recommendations by Dajani et al. [57]. Inter-round stability of statements reveals the degree to which participants' responses are changing or not changing. Statements were considered stable if the median and interquartile range of responses from all participants did not change significantly between rounds [57, 58]. Wilcoxon matched-pairs signed-ranks test was used to assess the stability of the responses between stages as used in a previous Delphi study [54].
The consensus was determined using IQR (≤ 1) and median (≥ 4) [59]. In addition, percentage agreement was described as the percentage of panellists who respond “agree or strongly agree” to an individual statement. Each statement that receives ≥ 75% agreement was considered as having reached a consensus [60]. Statements were further described by level of agreement, this means that consensus statements in the top 5% with the highest percentage of agreement was considered the most important [29]. Following these pre-defined criteria, two rounds were sufficient as exemplified in a study [49]. The study report was prepared following the recent guidelines for reporting Delphi techniques in Health Science research [61].
Results
A total of 1,097 emails were sent to participants meeting the minimum criteria. Feedback was received from 209 participants. Due to relocation out of the country or stopping practice 12 participants were ineligible. Therapists meeting the inclusion criteria were 197. Of those, 139 completed the first round and 125 (90%) completed the second round after receiving the link to the questionnaire as seen in Fig. 2.

Study flowchart
Table 1 below shows further details on participants demographics. Their mean age was 35.2 (SD 6.6), 39.6% were female and 1 participant was diverse. The majority 47 (33.8%) had above 5 and below 10 years of clinical experience, 76 (54.7%) had BSc as their highest educational level, and 80 (57.6%) had musculoskeletal area of interest. Participants who worked in the teaching hospital and federal medical centres made up 54 (38.8%).
Round 1: In this round, participants completed the rating of 30 statements and responded to the open-ended questions put forward. Of these 30 statements, 25 reached the criteria for consensus as seen in Table 2. There were 5 statements that failed to reach consensus; statement 5 (72%), statement 9 (61%), statement 15 (35%), statement 26 (73%) and statement 28 (70%) with the IQR ≥ 2 for each of the 5 statements.
Round 2: In this round, the same 5 statements as in round 1 failed to reach consensus; statement 5 (71%), statement 9 (63.7%), statement 15 (35.4%), statement 26 (63%) and statement 28(65.3%). The IQR remained at ≥ 2 for each of the 5 statements. The Wilcoxon’s matched-pairs signed-rank test shows no significant difference in the 5 statements between round 1 and round 2 with alpha level set at p < 0.05. Table 2 displays all 30 statements including the results from Wilcoxon’s matched-pairs signed-rank test, percentage agreement, median and inter-quartile range. Further details on individual item responses are shown in Additional file 2.
When arranged in order of importance, the top 5% of the items reaching consensus ranked by percentage of agreement were 4 statements, these statements had the highest levels of agreement (> 95%). These statements were; Modify patients’ expectations by education (96% agreement), Holding quality improvement meetings to review successes and adherence of the approach (96% agreement), Psychosocial care training for physiotherapists at undergraduate levels (96% agreement) and allocating time for patient communication (95% agreement) as shown on Table 3.
Qualitative responses
The responses and additional suggestions from rounds 1 and 2 fit well into the scope of categories previously derived (14 already identified categories in the preliminary round giving rise to the initial questionnaire), hence it was not necessary to add any new suggestions/questions to the questionnaire. They were re-classified under the 3 major existing categories of the questionnaire with accompanying definitions arising from participants’ responses (Additional file 3); Strategies to best modify stratified care management to fit the national context, Strategies on how training and education can best be done to help the implementation of stratified care, and Strategies related to conditions necessary to sustain the implementation (Table 4).
Strategies to best modify stratified care management to fit the National context
This category describes the unique challenges facing the national Health Care context, advantages which can be harnessed for the implementation of SC and peculiar ways of modifying the approach and tool to enhance suitability.
Here some participants commented on several issues they felt could help with contextual adaptation. A vital aspect was the suggestion on pilot implementation through the senior colleagues, Heads of departments and intermittent meetings/quality improvement monitoring how the approach progresses. This form of hierarchal implementation was seen by some responders as a viable means for implementation. In addition, some suggested ways to optimise the tool and approach by automation, using electronic versions of the tool and creating more translations.
‘High level PT mentorship needed’ *(F/ < 5/MSc/TeachHosp). [*Format: Quote (Gender/Qualification/Years of experience/Work)]
‘Periodic review of the approach should be done per time and encourage PTs in using the strategy’ (M/BSc/5–10/GenHosp).
‘Other language version of the SB tool should be made available for easy application because of the illiteracy level of many patients around the country’ (F/Msc/15–20/TeachHosp).
Training and education to aid the implementation of stratified care
This category relates to how education and training can be best carried out for stakeholders to aid the implementation of SC in clinical practice.
Some participants felt that undergraduate training should be carried out in areas related to patient communication and psychologically informed physiotherapy. These ones felt such training should be compulsory for every physiotherapist in training as this was very important in equipping them handle patients’ expectations. It helped with their confidence, standard of practice and enhances their knowledge. For patients, others felt rural outreaches can be easily done where communities are given educational seminars which should contain pain beliefs.
‘There should be compulsory training for PTs on stratified care approach’ (F/MSc/5–10/SpecialHosp)
‘PT undergraduates should be allowed to experience SC during their internship when practiced by licensed PTs’ (F/BSc/5 > /TeachHosp).
‘Reaching to rural communities to deliver health talks’ (M/MSc/10–15/TeachHosp).
Strategies related to conditions necessary to sustain the implementation
This category deals with the criteria that therapists feel are necessary to be in place for a smooth and sustained delivery and utilisation of SC. These conditions need to be ongoing concurrently with implementation and should serve to prepare stakeholders to accept this approach.
In order to ensure smooth implementation, some physiotherapists reported that interprofessional collaborations have to be made. Also, hospital managements have to be involved, to ensure sufficient PTs are employed, and remunerated and ultimately reduce workload. This can ensure sufficient time for patient communication relevant for all prognostic risk groups in the STarT Back classification system. The treatment tradition and attitude of PTs will change gradually with good results stemming from the pilot use of SC in practice.
‘Traditional ways will improve and be refined gradually with use’ (F/BSc/5–10/SportCentr).
‘More PTs should be employed in hospitals to reduce the burden of work and thus enable PTs to have more time for assessment and treatment’ (M/PhD/10–15/TrainInst).
‘Careful involvement of other health personnel participating in the client care’ (F/Bsc/ < 5/PriHC).
Discussion
This study developed strategies for the implementation of stratified care in Nigeria after two rounds of Delphi survey. The aspects of undergraduate training, sufficient time for patient-clinician communication, modifying patients’ expectations by educating them on expected outcomes and quality improvement meetings received consensus by physiotherapists as the most important and feasible strategies.
In this study, participants rated the statements based on their level of importance and feasibility within the context of all statements [37]. Participants highlighted broad strategies for implementation of a stratified model of care for patients with low back pain. These areas include; Educating and sharing information with stakeholders, inter-disciplinary collaboration and good patient communication. Undergraduate competency training aimed to adjust physiotherapists' beliefs and hone their skills in managing psychosocial risk factors in patients with complex conditions. Internal appraisals of the approach should be carried out to ensure compliance. Time scheduling was highlighted and categorised to help participants and was seen to have achieved the highest consensus. These aspects were consistent with the literature [17]. However, findings from this study reveal that of these areas, four statements were considered contextually most critical and feasible for implementation.
Overcoming patient expectations using education
Delphi panellists agreed that implementation needed physiotherapists to modify patients’ expectations by educating them on expected outcomes. Evidence from research shows that patients’ expectations when drawn from an inaccurate understanding of pain, could impede outcome if used as indices to measure satisfaction and a guide to treatment choices [62, 63]. For patients classified by the SB approach into low risk and high risk sub-categories, this strategy is of particular importance due to the recommended one-off treatment session, extended consultation and advice components. An understanding of the rationale and quality of the SB intervention will help patients trust the outcomes (e.g. that the one-off session for low risk sub-group is sufficient or that staying active in spite of pain is the right approach), establish reasonable expectations and re-focuses the patients’ attention on the treatment goals [64, 65]. For the delivery of education, participants in this study suggested that organising community seminars/outreaches and the use of social media platforms are effective as they reach individuals before they become patients and translate into amenable and co-operative patients [66, 67].
Quality improvement meetings
Delphi participants affirmed that physiotherapists should hold quality improvement meetings among themselves to review successes and adherence. This is in tandem with the Consolidated Framework for Implementation Research (CFIR) framework which expounds this further by asserting that the process of implementation should be supported by engaging users, opinion leaders through a process of self-reflection, evaluation and re-evaluating of the success and areas to improve. Such appraisals are not only key to implementation, but they also ensure the sustainability of the intervention [65]. A recent study shows that implementation using quality improvement strategies have better outcomes when established as routines in clinical practice, and executed with peer assessment workshops and support systems [68]. In the global implementation of stratified care, a research work by Sowden et al. suggests that stakeholder engagement can be done through various mechanisms including quality improvement meetings and mentorship [67]. This has a bearing not only on hierarchal implementation, where the seniors physiotherapists instigate these appraisals and systematically monitor the progress, it also involves their full participation and cooperation in convincing junior physiotherapy practitioners [34].
Undergraduate training
The Delphi survey received reasonable input from early graduates up to 5 years of clinical practice making up nearly one-fifth of the study population. Their opinions contributed to the strong consensus regarding the need for universities to include training on psychosocial care for physiotherapists at the undergraduate level. Studies testing the skills and capacity of fresh graduates in communications strategies and other aspects of cognitive behavioural treatment shows deficiencies with potential to be translated into practice. Revealing that training on psychosocial aspects including communication needs improvement [69, 70]. This important aspect of physiotherapy education is grossly limited within physiotherapy curriculum, due to limited patient contact and experiential teaching in training [70].
Therefore, undergraduate and entry-level physiotherapists should be targeted with sufficient practical components. This should be introduced early into their curriculum with adequate patient contact and close mentorship to ensure effective and sustained use of stratified care in practice and in this way to facilitate implementation [65, 71].
Sufficient time for patient-clinician communication
Communication in this context refers to ongoing individualized dialogue to improve patient condition and foster therapeutic alliance [72]. These conversations should be aimed at learning patients’ needs, perspectives and experiences, convincing the patients on treatment options, discussing treatment goals, building rapport, trust, self-efficacy, motivation, validating patients' feelings and normalise their experiences [65, 67]. The panellists in this study agreed that such open communication between physiotherapists and patients should be given priority and more time. It was also interesting to see that strategies to save time and incur cost savings like ‘educate the patients while treating them to save time’ were not a top priority to panellists as seen in other settings. This might be due to the structured statutory cadre-based system of payment used nationwide since physiotherapists are not paid based on time spent treating patients or based on the number of patients seen, these issues could have been of little relevance giving the possibility of extended time-based care [17]. This is directly in line with the SB approach which allocates an extended 30 min consultation session for patients in low and medium-risk categories and 45 min for patients in high-risk categories. Damschroder et al. [58] further suggested that for implementation, a common ground could be used to initiate some form of ‘marketing’ to attract and involve appropriate individuals and overcome indifference or resistance. Since physiotherapists easily see the importance of quality time for communication and a reduced income from one-off consultations might be less of a challenge, this can be a starting point and highlight for introducing SB approach for implementation during nationwide advocacy programs.
Notable other statements reaching consensus were ideas cutting across broad areas essentially aimed to standardise practice, inter-disciplinary collaboration and introduction of systemic managerial changes such as revamping the health insurance and referral systems. These aspects are vital but were not among the top consensus items. One possibility could be explained by their feasibility. For instance, creating a standard framework for uniform understanding, classification and measuring of a patient's conditions was the idea behind the International Classification of Functioning, Disability and Health (ICF). Its core set for LBP represents the typical spectrum of problems in functioning for patients with LBP [73]. In a study by Kirschneck et al., physiotherapists from 32 countries largely supported the core set for low back pain relating to activities and participation, similar in concept to the SB approach [73]. However, studies show that though clinicians support it, some still find issues with feasibility and challenges in clinical practice [74].
Research shows that the healthcare systems in low-medium income countries possess unique complexities and the possibilities are few due to poor funding and dire workforce shortages. There is also the issue of health care options for patients as inequalities exist between traditional, public and private Sects. [74]. These findings reveal that physiotherapists are aware of these issues and strategies using these statements would potentially receive good support.
Strengths and limitations
In the initial sampling, there was a response from one-fifth of the total number of contacted individuals. This implies that caution be taken in generalising the results of this study since the response rates might not represent the opinions of the entirety of the population. Further, there are some possible reasons to explain this level of response. Recent nationwide studies show a similar response ratio among healthcare workers especially when further expert criteria are required [75,76,77]. This may be due to the level of expertise, time and resource demands of online Delphi surveys [78,79,80]. Nonetheless, the recommended use of incentives, reasonable deadlines and personalised reminders in this study ensured high consistent response rates through rounds [78, 79].
The obtained demographics in this study were representative of the national physiotherapy workforce as the data shows that four-fifths of participants were less than 40 years, the majority were male with Bachelor’s degree, and working in tertiary health care institutions. This distribution can be corroborated by data from the World Physiotherapy database and demographics from recent studies [81,82,83].
This Delphi study was based on thorough qualitative data collected rigorously and analysed. One recent review and one methodological study concluded that concise statements lead to better quality responses and results since more than half of the Delphi studies reviewed had a maximum of 50 statements [37, 79]. There is evidence that a thorough first round based on systematically data extraction and analysis could produce shorter survey rounds [49, 79]. This was further reiterated by the qualitative data obtained from the rounds. Though the majority consisted of closed questions, the responses and suggestions after analysis resulted in sub-categories and quotes that fit into and strengthened pre-derived categories.
In this study, the questionnaire did not specify participants to respond either based on the feasibility or importance of statements. While this might be seen as a limitation, during the piloting process, the questions were cleverly modified to inherently imply feasibility. This was again checked from the pre-tests how they understood it so that while participants rated the level of importance they equally had feasibility in mind. This was piloted severally and reviewed to ensure the desired optimal outcome.
Conclusion
The Delphi method successfully elicited key recommendations on strategies with good potential to achieve sustained implementation of the stratified model of care. Educating patients with co-developed resources aimed at modifying expectations and focusing on patient communication to normalise their experiences and facilitate self-efficacy achieved consensus as the most feasible and important strategies. Additionally, undergraduate training on communication and psychosocial factors inherent in musculoskeletal conditions provide a framework for managing these subgroups. Quality improvement meetings for clinicians can ensure sustainability of stratified care in clinical practice. How the impact of these approaches incorporated into routine practices can be objectively quantified and reflected in patient well-being might be interesting for future research.
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Abbreviations
- STarT:
-
Subgrouping for Targeted Treatment
- SBT:
-
STarT Back Tool
- MSK:
-
Musculoskeletal
- LBP:
-
Low back pain
- IQR:
-
Interquartile range
- PIP:
-
Psychologically Informed Physiotherapy
- SC:
-
Stratified Care
- PT:
-
Physiotherapist
- TBS:
-
Traditional bone setters
References
Bello B, Bello AH. A systematic review on the prevalence of low back pain in Nigeria. Middle East J Rehabil Health. 2017;4(2):1–5.
Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. The Lancet. 2018;391(10137):2356–67.
Vos T, Abajobir AA, Abbafati C, Abbas KM, Abate KH, Abd-Allah F, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the global burden of disease study 2016. The Lancet. 2017;390(10100):1211–59.
Akodu AK, Kareem RO, Faniyi OR. Management of low back pain: knowledge and adherence to clinical practice guidelines amongst physiotherapists in selected hospitals in lagos state. Res J Health Sci. 2016;4(3):203.
Igwesi-Chidobe CN, Coker B, Onwasigwe CN, Sorinola IO, Godfrey EL. Biopsychosocial factors associated with chronic low back pain disability in rural Nigeria: a population-based cross-sectional study. BMJ Glob Health. 2017;2(3):e000284.
Protheroe J, Saunders B, Bartlam B, Dunn KM, Cooper V, Campbell P, et al. Matching treatment options for risk sub-groups in musculoskeletal pain: a consensus groups study. BMC Musculoskelet Disord. 2019;20(1):1–10.
Ogbeivor C, Elsabbagh L. Management approach combining prognostic screening and targeted treatment for patients with low back pain compared with standard physiotherapy: a systematic review & meta-analysis. Musculoskelet Care. 2021;19:436 (Epub ahead of print).
Foster NE, Hill JC, O’Sullivan P, Hancock M. Stratified models of care. Best Pract Res Clin Rheumatol. 2013;27(5):649–61.
O’Sullivan K, O’Sullivan P, Vibe Fersum K, Kent P. Better targeting care for individuals with low back pain: opportunities and obstacles. Br J Sports Med. 2017;51(6):489–90.
O’Sullivan K, O’Sullivan PB, O’Keeffe M. The Lancet series on low back pain: reflections and clinical implications. Br J Sports Med. 2019;53(7):392–3.
Main CJ, Sowden G, Hill JC, Watson PJ, Hay EM. Integrating physical and psychological approaches to treatment in low back pain: The development and content of the STarT Back trial’s ’high-risk’ intervention (StarT Back; ISRCTN 37113406). Physiotherapy. 2012;98(2):110–6.
Sowden G, Hill JC, Konstantinou K, Khanna M, Main CJ, Salmon P, et al. Targeted treatment in primary care for low back pain: The treatment system and clinical training programmes used in the impact back study. Fam Pract. 2012;29(1):50–62.
Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica: Summary of NICE guidance. BMJ (Online). 2017;356:10–3.
KNGF Clinical Practice Guideline for Physical Therapy in patients with low back pain 2013. Available from: URL: https://www.kngf.nl/binaries/content/assets/kennisplatform/onbeveiligd/guidelines/low-back-pain-2021/kngf_guide_on_low_back_pain_practice_guideline.pdf. Cited 2020 Jan 10.
Hill JC, Whitehurst DG, Lewis M, Bryan S, Dunn KM, Foster NE, et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): A randomised controlled trial. The Lancet. 2011;378(9802):1560–71.
Whitehurst DG, Bryan S, Lewis M, Hill J, Hay EM. Exploring the cost-utility of stratified primary care management for low back pain compared with current best practice within risk-defined subgroups. Ann Rheum Dis. 2012;71(11):1796–802.
Hill J, Try F, Agnew G, Saywell N. Perspectives and experiences of physiotherapists and general practitioners in the use of the STarT Back Tool: a review and meta-synthesis. J Prim Health Care. 2022;14(2):164–72.
Karstens S, Krug K, Hill JC, Stock C, Steinhaeuser J, Szecsenyi J, et al. Validation of the German version of the STarT-Back Tool (STarT-G): a cohort study with patients from primary care practices. BMC Musculoskelet Disord. 2015;16(1):1–8.
Hill JC, Garvin S, Chen Y, Cooper V, Wathall S, Saunders B, et al. Stratified primary care versus non-stratified care for musculoskeletal pain: findings from the STarT MSK feasibility and pilot cluster randomized controlled trial. BMC Fam Pract. 2020;21(1):30.
Foster NE, Mullis R, Hill JC, Lewis M, Whitehurst DG, Doyle C, et al. Effect of stratified care for low back pain in family practice (IMPaCT back): A prospective population-based sequential comparison. Ann Fam Med. 2014;12(2):102–11.
Akindele M, Rabiu M, Useh E. Assessment of the awareness, adherence, and barriers to low back pain clinical practice guidelines by practicing physiotherapists in a low-resourced country. Physiother Res Int. 2019;25(1):e1811.
Ulger O, Demirel A, Oz M, Tamer S. The effect of manual therapy and exercise in patients with chronic low back pain: Double blind randomized controlled trial. J Back Musculoskelet Rehabil. 2017;30(6):1303–9.
Lam OT, Strenger DM, Chan-Fee M, Pham PT, Preuss RA, Robbins SM. Effectiveness of the McKenzie method of mechanical diagnosis and therapy for treating low back pain: literature review with meta-analysis. J Orthop Sports Phys Ther. 2018;48(6):476–90.
Moretti A, de Sire A, Curci C, Toro G, Gimigliano F, Iolascon G. Effectiveness of denosumab on back pain-related disability and quality-of-life in patients with vertebral fragility fractures. Curr Med Res Opin. 2019;35(1):151–5.
Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. The Lancet. 2018;391(10137):2368–83.
Hayden JA, Wilson MN, Stewart S, Cartwright JL, Smith AO, Riley RD, et al. Exercise treatment effect modifiers in persistent low back pain: an individual participant data meta-analysis of 3514 participants from 27 randomised controlled trials. Br J Sports Med. 2020;54(21):1277–8.
Ogwumike OO, Bashir-Bello F, Kaka B. Patients’ experiences about exercise prescription and education in the physiotherapy management of nonspecific low-back pain. J Patient Exp. 2020;7(6):1458–65.
Ayanniyi O, Lasisi O, Adegoke B, Oni-Orisan M. Management of low back pain: - attitudes and treatment preferences of physiotherapists in Nigeria. Afr J Biomed Res. 2009;10(1):42–9.
Odebiyi DO, Aweto HA, Igbari TO, Tella BA. Factors influencing number of physiotherapy treatment sessions for patients with low back pain. Af Jrl Phys Rehab Sci. 2012;4(1–2):23.
Mbada CE, Ojoawo AO, Owoola SO, Okonji AM, Odetunde MO, Adigwe KC, et al. Knowledge and attitude about the practice of traditional bone setters and its use for musculoskeletal disorders in rural areas in Nigeria. Middle East J Rehabil Health Stud. 2020;7(2):e99973.
Roccuzzo A, Molinero-Mourelle P, Ferrillo M, Cobo-Vázquez C, Sanchez-Labrador L, Ammendolia A, et al. Type I collagen-based devices to treat nerve injuries after oral surgery procedures. Syst Rev Appl Sci. 2021;11(9):3927.
de Sire A, Marotta N, Ferrillo M, Agostini F, Sconza C, Lippi L, et al. Oxygen-ozone therapy for reducing pro-inflammatory cytokines serum levels in musculoskeletal and temporomandibular disorders: a comprehensive review. Int J Mol Sci. 2022;23(5):2528.
Bernetti A, Agostini F, de Sire A, Mangone M, Tognolo L, Di Cesare A, et al. Neuropathic pain and rehabilitation: a systematic review of international guidelines. Diagnostics (Basel). 2021;11(1):74.
Adje M, Steinhäuser J, Stevenson K, Mbada CE, Karstens S. Patients’ and physiotherapists’ perspectives on implementing a tailored stratified treatment approach for low back pain in Nigeria: a qualitative study. BMJ Open. 2022;12(6):e059736.
Wensing M, Bosch M, Grol R. Developing and selecting interventions for translating knowledge to action. CMAJ. 2010;182(2):E85–8.
Wensing M, Huntink E, van Lieshout J, Godycki-Cwirko M, Kowalczyk A, Jag̈er C, et al. Tailored implementation of evidence-based practice for patients with chronic diseases. PLoS ONE. 2014;9(7):1–8.
Keeney S, Hasson F, McKenna H. The Delphi Technique. Nursing and Health Research. Oxford: Wiley-Blackwell; 2010.
Niederberger M, Renn O. Das klassische Delphi-Verfahren: Konzept und Vorgehensweise. In: Niederberger M, Renn O, editors. Das Gruppendelphi-Verfahren: Vom Konzept bis zur Anwendung. Wiesbaden: Springer VS; 2018. p. 7–25.
Fletcher AJ, Marchildon GP. Using the Delphi method for qualitative, participatory action research in health leadership. Int J Qual Methods. 2014;13(1):1–18.
Cole ZD, Donohoe HM, Stellefson ML. Internet-based Delphi research: case based discussion. Environ Manage. 2013;51(3):511–23.
Hora SC. Expert Judgment. Wiley StatsRef: Statistics Reference Online. 2014;323(7):1-3.
Delphi methodology in health research. how to do it? Eur J Integr Med. 2015;7(4):423–8.
Mcilfatrick SJ, Keeney S. Identifying cancer nursing research priorities using the Delphi technique. J Adv Nurs. 2003;42(6):629–36.
Hung H-L, Altschuld JW, Lee Y-F. Methodological and conceptual issues confronting a cross-country Delphi study of educational program evaluation. Eval Program Plann. 2008;31(2):191–8.
CatalinToma IP. The Delphi Technique: methodological considerations and the need for reporting guidelines in medical journals. Int J Public Health. 2016;4(6):47–59.
Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32(4):1008–15.
Duffield C. The Delphi technique: a comparison of results obtained using two expert panels. Int J Nurs Stud. 1993;30(3):227–37.
Corbin JM, Strauss A. Grounded theory research: Procedures, canons, and evaluative criteria. Qual Sociol. 1990;13(1):3–21.
Schmalz U, Spinler S, Ringbeck J. Lessons learned from a two-round delphi-based scenario study. MethodsX. 2021;8:101179.
Dalkey N. An experimental study of group opinion. Futures. 1969;1(5):408–26.
Grabbe EM, Pyke DL. An evaluation of the forecasting of information processing technology and applications. Technological Forecasting and Social Change. 1972;4(2):143–150.
SoSci Survey ‣ the Professional Solution for Your Online Survey. Available from: URL: https://www.soscisurvey.de/. Cited 2020 Jan 13.
Pepper D, Hodgen J, Lamesoo K, Kõiv P, Tolboom J. Think aloud: using cognitive interviewing to validate the PISA assessment of student self-efficacy in mathematics. Int J Res Method Educ. 2018;41(1):3–16.
Von der Gracht. Consensus measurement in Delphi studies: Review and implications for future quality assurance. Technological Forecasting and Social Change. 2012;79(8):1525–1536.
Mayring P. Qualitative Content Analysis 2000. Available from: URL: http://www.qualitative-research.net/index.php/fqs/article/view/1089/2385. Cited 2014 Dec 20.
von Briel F. The future of omnichannel retail: a four-stage Delphi study. Technol Forecast Soc Chang. 2018;132:217–29.
Dajani JS, Michael Z, Sincoff MZ, Talley WK. Stability and agreement criteria for the termination of Delphi studies. Technol Forecast Soc Change. 1979;13:83–90.
Holey EA, Feeley JL, Dixon J, Whittaker VJ. An exploration of the use of simple statistics to measure consensus and stability in Delphi studies. BMC Med Res Methodol. 2007;7:52.
Courtenay M, Deslandes R, Harries-Huntley G, Hodson K, Morris G. Classic e-Delphi survey to provide national consensus and establish priorities with regards to the factors that promote the implementation and continued development of non-medical prescribing within health services in Wales. BMJ Open. 2018;8(9):e024161.
Keeney S, Hasson F, McKenna H. Consulting the oracle: ten lessons from using the Delphi technique in nursing research. J Adv Nurs. 2006;53(2):205–12.
Spranger J, Homberg A, Sonnberger M, Niederberger M. Reporting guidelines for Delphi techniques in health sciences: A methodological review. In Zeitschrift für Evidenz, Fortbildung und Qualität im Gesundheitswesen. 2022;172:1–11.
Odumodu IJ, Olufunlayo TF, Ogunnowo BE, Kalu ME. Satisfaction with services among attendees of physiotherapy outpatient clinics in tertiary hospitals in Lagos State. J Patient Exp. 2020;7(4):468–78.
Lim YZ, Chou L, Au RT, Seneviwickrama KMD, CicuttiniFM,Briggs AM, et al. People with low back pain want clear, consistent and personalised information on prognosis, treatment options and self-management strategies: a systematic review. J Physiother. 2019;65(3):124–35.
Butler D, Moseley G. Explain Pain (2nd ed.). Adelaide City West, South Australia: Noigroup Publications; 2013.
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50.
Traeger AC, Lee H, Hübscher M, Skinner IW, Moseley GL, Nicholas MK, et al. Effect of intensive patient education vs placebo patient education on outcomes in patients with acute low back pain: a randomized clinical trial. JAMA Neurol. 2019;76(2):161–9.
Sowden G, Hill JC, Morso L, Louw Q, Foster NE. Advancing practice for back pain through stratified care (STarT Back). Braz J Phys Ther. 2018;22(4):255–64.
Meerhoff GA, van Dulmen SA, Maas MJM, Heijblom K, Van der Nijhuis Sanden MWG, van der Wees PJ. Development and evaluation of an implementation strategy for collecting data in a national registry and the use of patient-reported outcome measures in physical therapist practices: quality improvement study. Phys Ther. 2017;97(8):837–51.
Ezenwankwo EF, Ezeukwu AO, Abaraogu UO, Manu GP, Mogbolu GA, Ezelioha RN, et al. Physiotherapy clinical education in the eastern Nigeria: students’ and interns’ views on clinical educator characteristics, opportunities and learning conditions. Eur J Physiother. 2019;21(3):153–63.
Abaraogu UO, Onah U, Abaraogu OD, Fawole HO, Kalu ME, Seenan CA. Knowledge, attitudes, and the practice of health promotion among physiotherapists in Nigeria. Physiother Can. 2019;71(1):92–100.
Parry RH, Brown K. Teaching and learning communication skills in physiotherapy: what is done and how should it be done? Physiotherapy. 2009;95(4):294–301.
Oliveira VC, Refshauge KM, Ferreira ML, Pinto RZ, Beckenkamp PR, NegraoFilho RF, et al. Communication that values patient autonomy is associated with satisfaction with care: a systematic review. J Physiother. 2012;58(4):215–29.
Kirschneck M, Kirchberger I, Amann E, Cieza A. Validation of the comprehensive ICF core set for low back pain: the perspective of physical therapists. Man Ther. 2011;16(4):364–72.
Rundell SD, Davenport TE, Wagner T. Physical therapist management of acute and chronic low back pain using the world health organization’s international classification of functioning. Disabil Health Phys Ther. 2009;89(1):82–90.
Odole AC, Oyewole OO, Akinpelu AO. A comparative survey of Nigerian physiotherapists’ familiarity with, knowledge of and utilisation of standard outcome measures: 10 years after initial survey. S Afr J Physiother. 2018;74(1):435.
Badru OA, Oloko KO, Hassan AO, Yusuf OB, Abdur-Razaq UA, Yakub S. Prevalence and correlates of psychological distress amongst healthcare workers during the COVID-19 pandemic: An online survey. S Afr J Psychiatr. 2021;27:1617.
Idris I, Awotidebe AW, Mukhtar NB, Ativie RN, Nuhu JM, Muhammad IC, et al. Expert consensus on the minimum clinical standards of practice for Nigerian physiotherapists working in intensive care units: A modified Delphi study. Afr J Thorac Crit Care Med. 2021;27(3):10.7196.
Cunningham CT, Quan H, Hemmelgarn B, Noseworthy T, Beck CA, Dixon E, et al. Exploring physician specialist response rates to web-based surveys. BMC Med Res Methodol. 2015;15:32.
Gargon E, Crew R, Burnside G, Williamson PR. Higher number of items associated with significantly lower response rates in COS Delphi surveys. J Clin Epidemiol. 2019;108:110–20.
Giannarou L, Zervas E. Using Delphi technique to build consensus in practice. Int J Bus Sci Appl Manage (IJBSAM). 2014;9(2):65–82.
Kalu ME, Vlachantoni A, Norman KE. Knowledge about risk factors for falls and practice about fall prevention in older adults among physiotherapists in Nigeria. Physiother Res Int. 2019;24(1):e1742.
World Physiotherapy. Nigeria: A profile of the profession in 2022. Available from: https://world.physio/membership/nigeria. Cited 11 Jul 2022.
Bello B, Hartley SE, Yeowell G. Nigerian physiotherapists’ knowledge, current practice and perceptions of their role for promoting physical activity: A cross-sectional survey. PLoS ONE. 2022;17(5):e0266765.
Acknowledgements
The authors express thanks to Caroline Schulte, Motunrayo Ojo and Abraham Uluocha for their help on survey instruments; Mortiz Scherer for his ideas on analysis.
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors declare that there is no external source of funding allocated to this project.
MA received personal funding from the German Academic Exchange Service (DAAD) and Petroleum Technology Development Fund (PTDF) for his doctoral project.
Author information
Authors and Affiliations
Contributions
MA: Designed the study, recruited participants, organised data collection, transcribed, analysed and interpreted the data and drafted the manuscript. JS: Designed the study, analysed and interpreted the data, critically revised the manuscript. KS: Designed the study, analysed and interpreted the data, critically revised the manuscript. CM: Designed the study, recruited participants, critically revised the manuscript. VA: Designed the study, analysed and interpreted the data, critically revised the manuscript. SK: Designed the study, analysed and interpreted the data, drafted the manuscript, critically revised the document. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study received ethical approval from the ethical committee of the Trier University of Applied sciences (03/2020 – 04/2020) and the ethical committee of the Obafemi Awolowo University Teaching Hospital, Ile-Ife Nigeria (06/2020–09-2020) (registration ID: IRB/IEC/0004553). This study was pre-registered on OSF Registries (Registration https://doi.org/10.17605/OSF.IO/8CNPV).
All methods were carried out in accordance with relevant guidelines and regulations. Informed consent (written) for were obtained from all participants before participating in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Qualitative Data from Preliminary PhaseInforming Round 1 Questionnaire Development.
Additional file 2.
Individual Item Responses in Round 1 and Round 2.
Additional file 3.
Qualitative data for Rounds 1 and 2. Common themes and indicative quotes.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Adje, M., Steinhäuser, J., Stevenson, K. et al. Developing tailored intervention strategies for implementation of stratified care to low back pain with physiotherapists in Nigeria: a Delphi study. BMC Health Serv Res 23, 134 (2023). https://doi.org/10.1186/s12913-023-09123-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09123-1