
Abstract
Background
Cultural competence is considered a core qualification for dealing with socio-cultural diversity and balancing disparities in health care.
Objectives
To explore features supporting and inhibiting cultural competence in the hospital at both organisational and staff levels.
Design
Cross-sectional online survey in the form of a full census from May to November 2018.
Setting
Two organisations that run a total of 22 hospitals in Germany.
Participants
Eight hundred nursing and medical professionals [nurses: n = 557; doctors: n = 243].
Methods
Using the Short Form Cultural Intelligence SCALE (SFCQ), cultural competence was measured and its relation to potential influencing factors at staff level and organisational level examined, using bivariate (t-Test, one-way ANOVA, Pearson and Spearman correlations) and multivariate (multiple linear regression) approaches. Model 1 examined features at organisational level, Model 2 at individual level and Model 3 included organisational and individual features.
Results
The mean cultural competence measured was 3.49 [min.: 1.3; max.: 5.0]. In the bivariate and isolated multivariate models [Models 1 and 2], factors on both organisational and individual levels were significantly related to the hospital staff’s cultural competence. The multivariate overview [Model 3], however, revealed that individual features at staff level were the statistically relevant predictors. Positive influencing features included staff’s assessment of the importance of cultural competence in their professional context [B: 0.368, 95% confidence interval 0.307; 0.429], participation in competence training [B: 0.193; 95% confidence interval 0.112; 0.276] and having a migration background [B: 0.175; 95% confidence interval 0.074; 0.278], while negative features included length of medical service [B: -0.004; 95% confidence interval -0.007; -0.001].
Conclusions
The development and practice of cultural competence appear to be determined less by organisational features and more on the level of individual actors. In addition to staff development, adequate organisational structures and an economic incentive system are required to promote sociocultural diversity in hospitals.
Similar content being viewed by others


Introduction
Global migration reached a peak of an estimated 272 million people in 2019 [1].
The “refugee crisis “ in 2015 gave a fresh boost to migration to Germany, too. Currently, 13.7 million people, 16.7% of the total population of Germany, have personal experience of migration [2]. Nevertheless, being a migrant or having ethnic minority status is linked to unequal access to the health system and sometimes to higher risk of illness [3]. The discussion of ways to effectively counter migrants’ health inequality is still ongoing. Cultural competence is seen as one strategy to rebalance inequalities in nursing and medical care and to promote immigrants’ chances of participation in healthcare [4,5,6,7,8]. Two aspects shown to have a positive impact in this context are a solution-oriented working approach, and empathy and tolerance when dealing with cultural diversity. These factors are reflected in improved treatment quality and patient satisfaction, as well as economic efficiency [9,10,11,12,13,14]. Cultural competence also has the potential to increase healthcare staff’s professional satisfaction and to protect them from perceived time pressure, stress, sleep problems or burnout [15,16,17].
Pluralisation processes in the health care system are accelerated not only by its users, but also by the employment of (post-)migrant healthcare staff. According to OECD figures, the number of trained healthcare staff in almost all European countries increased in the last decade, yet more are still needed [18]. The WHO predicts a lack of about 14.5 million trained nursing staff by 2030 [19]. One reaction is to recruit trained nurses from abroad [20]. In addition, German policy is to integrate refugees into the healthcare professions [21].
Consequently, healthcare is experiencing more multicultural teams of nurses and doctors and increasing cultural diversity of patients. In other words, immigration impacts the nursing and medical care field in a variety of ways. This diversity can be a challenge that particularly affects communication when actors have different sociocultural backgrounds.
The concept of cultural competence
Communication is based on internalised patterns of action and interpretation that people acquire during their lives. In our context, the key agent of socialisation is the cultural system ‘medicine’ which has differing cultural and social features in each country. This results in a range of ideas about illness and health, concepts of healthcare and healing, and specific notions of the hierarchies, skills and fields of responsibility of the nursing and medical professions. The fewer experiences interacting persons have in common, the more difficult it is to correctly grasp, much less intuitively interpret, the intention behind others’ words, gestures and emotions. Although interactions are therefore seldom conflict-free as diversity increases, little attention has been paid so far—in Europe—to sociocultural and migration-related aspects in care or organisational concepts [22,23,24,25,26,27,28,29].
Cultural competence is seen as a potential tool for shaping effective, appropriate communication and interaction, regardless of the participants’ sociocultural background [30, 31]. “Cultural competence” is usually described as a multidimensional set of cognitive orientations, culture-related knowledge, skills, sensitivities and attitudes [32, 33]. In this context, (self-)critical reflection is considered particularly important; this includes among other things the individual’s ties to their cultural location, internalised prejudices and value hierarchies.
Factors that influence cultural competence
It is generally accepted that cultural competence can be learnt [34, 35]. Several literature reviews confirm that coaching is an effective factor in strengthening all, or at least some, dimensions of cultural competence [36,37,38,39,40,41]. It is less clear how sociodemographic factors such as age, educational level, country of origin, religion and ethnicity are related to cultural competence. While a number of studies show no links [42, 43], several indicate age as an influencing factor [44, 45]. Almutairi et al. (2017) attributed this to the accumulated professional experience of the nurses examined that had a positive effect on their cultural competence, while also showing that cultural competence varied in relation to the nurses’ country of origin [44]. Finally, a Swiss study indicated that doctors have more cultural competence than nursing staff [46].
The analyses in these studies focused primarily on individual factors at staff level. Looking at actions intended to promote cultural competence, they also focused on strategies that aim at staff development and training [35, 47, 48]. Organisational factors (e.g. organisational readiness and commitment, audit and quality improvement approaches, workforce diversity, diversity climate) intended as innovations to promote cultural competence in the healthcare system were measured for their effectiveness in relation to patient-oriented outcomes or at system level [47, 49]; the studies reveal no overall impact. The direct effect of these factors on healthcare staff’s cultural competence was not the focus of this research, however.
Logic model and study aim
Our concept starts with the assumption that while an organisation‘s institutional framework does not determine its members’ actions, it does influence them. To that extent, organisations can strengthen or inhibit active cultural competence. This article examines how both staff-related and institution-related factors are linked to the cultural competence of healthcare staff, both nurses and doctors, in hospital.
Methods
Data collection
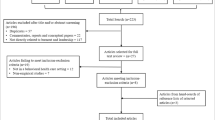
Data collection lasted from May to November 2018. Active healthcare workers in 22 hospitals run by two organisations (Organisations A and B) were invited by email to participate in an online survey via a personalised link (Organisation A: approx. 2,500 doctors, approx. 4,000 nursing staff; Organisation B: approx. 1,200 doctors, approx. 5,800 nursing staff). Because some potential respondent groups did not have their own email accounts, they received their invitations, including a QR code, sent with the pay slip. The survey was administered using the EFS software Unipark. The data collected were saved on an external server protected by QuestBack, a Unipark provider. In order to increase the response rate, we sent reminders and an additional survey was carried out later among the doctors in organisation B.
Measuring “cultural competence”, the target variable
To measure cultural competence, a multidimensional construct, we applied Thomas et al.’s short scale (Short Form Cultural Intelligence SCALE, SFCQ) which provided evidence for construct-related and criterion-related validity and is internet-enabled [50]. This instrument already existed in five languages and was translated from the English original into German (Cronbachs α = 0.87, total value). Several scientists worked in parallel to translate the text and the translation was finalised in a joint sitting [51]. The instrument includes ten items: two measure cultural knowledge, five measure cultural skills and three measure cultural metacognition. Higher scores indicate greater cultural competence. The arithmetic mean was determined across all ten items; cases with two or more missing items (n = 6) were excluded. Where one item was missing (n = 14), the arithmetic mean of nine items was determined.
Independent variables at the individual level
Independent variables at individual level were sociodemographic factors and features of respondents’ professional biographies: gender, migration background, occupational category [nursing, medicine], duration of career and respondents’ assessment of how well their training prepared them for working with immigrant patients [well, fairly well, fairly poorly, poorly] and the importance assigned to cultural competence in the professional context [very important, important, slightly important, not important]. Finally, respondents were asked whether they had completed a training course on cultural competence. Data on respondents’ migration background was based on the country of (the parents’) birth and differentiated between whether one or both parents are immigrants [52]. Respondents born in Germany but one of whose parents were born abroad have a “migration background on one side”. Respondents who are themselves immigrants and/or both parents are immigrants have a “migration background on both sides”.
Independent variables at organisational level
Institutional factors were registered by differentiating between the two organisations [A and B] that run the hospitals, the (estimated) proportion of staff and patients with migration backgrounds on each ward, and regular employer encouragement to take part in intercultural coaching. The latter item was dichotomised by combining the options “don’t know” and “no”.
Statistical analyses
SPSS Statistics 25 was used to carry out the statistical analysis, including mean comparison tests (t-test, one-way ANOVA), correlation analysis (Pearson, Spearman) and multiple regression in which potential influencing factors were related to cultural competence. Three models were calculated in total: first, effects on the organisational level were examined; second, effects at individual level and third, all variables were examined in a joint model. The model was tested for multicollinearity. We set the significance level for all analyses to α = 0.05.
Results
Institution-related and staff-related sample characteristics
A total of 800 active hospital staff participated in the online survey, a response rate of about 6%. Table 1 shows the main characteristics of the organisational and staff samples and how they relate to cultural competence. In the bivariate test, both organisational features (organisation, provision and encouragement of coaching on intercultural topics, proportion of staff and patients with migration background) and individual features (occupational category, migration background, mother tongue, relevance, preparation through training, participation in intercultural competence coaching, career duration) show a significant correlation with the degree of cultural competence.
The average cultural competence measured is 3.49. The sub-dimension Cultural Metacognition has a statistically significantly lower mean value than that of Cultural Skills (Table 2). However, this is not relevant for the following analyses, since the Short-Scale SFCQ was designed as a reflexive model in which the three sub-dimensions are not compensatory, but in which cultural competence is reflected as a latent construct in all three sub-dimensions [50].
Multiple regression models
Table 3 shows the results of the three regression models. The regressors included on the organisational level (Model 1) explain 3.4% of the variance of the target variable “cultural competence”; the regressors on the personnel level (Model 2) explain 29.9% of this variance and those on both organisational and individual levels (Model 3) explain 29.7%.
Model 1: predictors at organisational level
Two factors with a significant positive effect on the cultural competence of hospital staff are estimated proportion of patients with a migration background and employer encourages staff to participate in coaching on intercultural topics. As the proportion of patients with a migration background grows, respondents’ cultural competence also increases, though only very slightly, by 0.003 points. The greatest effect on respondents’ cultural competence at organisational level was achieved by regularly encouraging staff to participate in relevant training.
Model 2: predictors at individual level
Respondents’ occupational category or gender is not significantly linked to their cultural competence. Factors positively associated with cultural competence are staff’s assessment that cultural competence is very important in the professional context and that their training prepared them well for working with migrant patients. Participation in relevant coaching courses also has a positive effect on the competence measured. The cultural competence of people who had attended such coaching was 0.204 points higher than that of respondents who had not. There is also a significant difference in cultural competence between respondents with a migration background on both sides and those with no migration background. Staff with a migration background on both sides show cultural competence that is 0.183 points higher than those with no migration background. No significant effect could be seen in people with a migration background on one side. Career duration is negatively associated with cultural competence, which sinks very slightly, but still significantly, by 0.004 points per career year. The strongest effect on the individual level, i.e., hospital staff, reflects how relevant they consider cultural competence to be.
Model 3: institutional and person-related predictors
If factors on the organisational and individual levels are examined simultaneously in one model, only the staff-related effects are significant. The largest effect is still produced by the importance assigned to cultural competence, followed by participation in coaching and a migration background on both sides. Professional training and career duration also have significant influence.
Discussion
Sociocultural diversity is a typical feature of the everyday medical and nursing context in hospital. This creates challenges both in dealing with patients and where staff cooperate in a multicultural environment. The initial thesis behind our analysis was that in addition to individual skills at staff level, the institutional context can promote or inhibit cultural competence in action. Therefore the analytical viewpoint includes both individual and institution-related factors.
First, our findings show that cultural competence in action seems to increase with everyday practice in an intercultural context – the proportion of immigrant patients reported in the hospitals we examined indicates this. Equally, the institutional context has a positive effect if the organisation is aware of the importance of intercultural care and, for example, actively encourages its staff to participate in relevant coaching. In the overview of the influencing factors analysed, however, it is the individual resources that produce an effect on cultural competence. In particular, the significance staff allocate to this topic in professional activity produces a positive effect; actually attending relevant coaching is also beneficial. A migration background on both sides and intercultural content in professional training are also associated with greater cultural competence. Longer duration of respondents’ professional careers had a negative impact. The development and practice of cultural competence thus appears to be not so much anchored in the institutional structure as linked to the level of individual actors.
Factors at organisational level
A staff development strategy focused on cultural diversity has been discussed as an effective institutional instrument for driving cultural competence development [47, 49]. Our isolated examination of organisational factors clearly showed that cultural competence is boosted when the proportion of staff with a migration background increases, even though this effect was slightly below a statistically significant level. This indicates that working in culturally diverse teams is linked to increased demands for culturally competent behaviour. The proportion of patients with a migration background had a greater influence – intercultural care practice may be concomitant with more pressure to improve qualifications. The greatest effect, however, was seen when the institution encourages staff to participate in intercultural coaching; we assess this as indicating a management that actively promotes the development of relevant skills. Studies that identify diversity-sensitive organisational development as the institutional framework for cultural competence in practice point to the same conclusion. This includes factors such as a diversity-sensitive organisational climate, defining cultural competence development as a mark of quality, and coordinated controlling [53, 54].
Factors at individual level
The positive relationship between staff members’ participation in intercultural coaching and their level of cultural competence tallies with the findings of previous studies. For example, several systematic reviews confirm that coaching increases healthcare workers’ cultural competence [48]. This applies to both intercultural knowledge and culture-sensitive characteristics and attitudes. Despite intercultural education, nevertheless, an in-depth understanding of cross-cultural healthcare (e.g., power imbalances, biases, and self-reflexivity) often seems to be lacking [55].
In their study of doctors and psychotherapists in training, Bernhard et al. (2015) determined that both cultural competence training and a migration background had a significant influence on some dimensions of cultural competence. The results of this online survey confirm that a migration background on both sides has positive effects for the respondents. In particular, potential and resources such as speaking more than one language, specific cultural knowledge and the experience of moving in different sociocultural contexts seem to have a beneficial impact on culture-sensitive patient care. Staff with migration backgrounds also more often take on the role of cultural mediators, interpreters or people of trust in their everyday work context.
Unlike the findings of a Swiss study [46], our survey showed no indications of differences between nurses and doctors related to their professional category.
While some studies show that cultural competence increases with age and professional experience, [44, 45] we observed the opposite effect. We suspect that a generational effect lies behind the negative association between career duration and the level of cultural competence: on the one hand, younger staff may benefit from changes to training content, which increasingly takes culturally sensitive and migration-related topics into account, though not always to the same extent. The effect of career duration still shows up, however, regardless of how their training was oriented, as we were able to show. On the other hand, intercultural contacts both at work and in private life may be taken more for granted by younger staff members and socialisation in contexts of diversity may be more common. Studies show that cultural competence increases with the frequency of intercultural encounters in private and professional contexts [10, 56, 57]. Topics like cultural competence that are relatively new in Germany may therefore be less accessible to older staff members. Finally, however, another explanation could be that where working routines become ossified, cultural competence that may initially have been present may gradually fade.
Strengths and limitations
The significance of our data is limited by restricted controllability of the survey conditions. The links to the survey were passed on via mediators in each institution for data protection reasons. At the same time, however, coverage problems were reduced because the base population was known and a lack of internet access at the place of work could be compensated by the QR code on the payslip. Online surveys are generally considered to be less successful in motivating respondents to participate, a problem reinforced by the lack of time available during everyday hospital work. This is reflected in the low response rate. In Organisation A the nurses were harder to reach; in Organisation B the doctors were less accessible. The sample nevertheless adequately reflects the overall distribution of the professional categories. Further, we cannot exclude the possibility that respondents who were motivated to take part were those who were more interested in the topic anyway and therefore have more cultural competence. Moreover, information on how to correctly interpret our finding that cultural competence decreases with career length can only be provided by a longitudinal study. Data on organisation-related characteristics were collected through a self-report survey. In order to ensure anonymity, it was not possible to assign survey participants to a particular hospital. Nevertheless, the decisive aspect for the actions of professional actors is how they perceive their organisation and its services. Finally, we subsumed several hospitals in two units run under the auspices of Organisations A and B. This leads to a simplification because individual hospitals run by one organisation may still differ. However, the hospitals present themselves as being linked by a common philosophy which includes addressing sociocultural diversity.
Conclusion
On balance, our findings suggest that culturally competent action is not promoted systematically through the organisational contexts but is primarily supported by the staff’s individual resources. As diversity increases, in-patient care institutions are coming under increasing pressure to change. This includes promoting organisational structures and an organisational culture that accepts apparent cultural idiosyncrasies as variations in ways of thinking and acting that anchor intergenerational and cultural learning and encourage their staff to consistently apply the cultural competence they have gained. Last but not least, this requires economic incentive systems that reward culturally competent care. In order to optimise care quality in the long term in the context of sociocultural diversity and to ensure the satisfaction of both patients and staff, the process of intercultural opening must include structural development on the organisational level, alongside personnel development.
Availability of data and materials
The datasets generated and analysed during the current study are not publicly available due to data protection concerns, particularly on the part of the participating hospital organisations, but are available from the corresponding author on reasonable request.
Abbreviations
- OECD:
-
Organisation for Economic Co-operation and Development
- SFCQ:
-
Short Form Cultural Intelligence SCALE
- WHO:
-
World Health Organization
References
IOM. World Migration Report 2020. https://publications.iom.int/books/world-migration-report-2020. Accessed 20 July 2021.
Statistisches Bundeamt. Bevölkerung nach Migrationshintergrund und Geschlecht 2021. https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Migration-Integration/Tabellen/liste-migrationshintergrund-geschlecht.html. Accessed 14 July 2021.
Rechel B, Mladovsky P, Ingleby D, Mackenbach JP, McKee M. Migration and health in an increasingly diverse Europe. Lancet. 2013;381:1235–45.
Weech-Maldonado R, Elliott M, Pradhan R, Schiller C, Hall A, Hays RD. Can hospital cultural competency reduce disparities in patient experiences with care? Med Care. 2012;50:48–55.
Slean GR, Jacobs EA, Lahiff M, Fisher L, Fernandez A. Aspects of culturally competent care are associated with less emotional burden among patients with diabetes. Med Care. 2012;50:69–73.
McGregor B, Belton A, Henry TL, Wrenn G, Holden KB. Improving behavioral health equity through cultural competence training of health care providers. Ethn Dis. 2019;29:359–64.
Marek E, Nemeth T. Intercultural competence in healthcare. Orv Hetil. 2020;161:1322–30.
Kraft-Todd GT, Reinero DA, Kelley JM, Heberlein AS, Baer L, Riess H. Empathic nonverbal behavior increases ratings of both warmth and competence in a medical context. PLoS ONE. 2017;12: e0177758.
Houtz JC, Ponterotto JG, Burger C, Marino C. Problem-solving style and multicultural personality dispositions: a study of construct validity. Psychol Rep. 2010;106:927–38.
Korol LD. Is the association between multicultural personality and ethnic tolerance explained by cross-group friendship? J Gen Psychol. 2017;144:264–82.
Yakar HK, Alpar. Intercultural communication competence of nurses providing care for patients from different cultures. Int J Caring Sci. 2018;11:1743–55.
Hagqvist P, Oikarainen A, Tuomikoski AM, Juntunen J, Mikkonen K. Clinical mentors’ experiences of their intercultural communication competence in mentoring culturally and linguistically diverse nursing students: a qualitative study. Nurse Educ Today. 2020;87:104348.
Betancourt JR, Green AR, Carrillo JE, Park ER. Cultural competence and health care disparities: key perspectives and trends. Health Aff. 2005;24:499–505.
Govere L, Govere EM. How effective is cultural competence training of healthcare providers on improving patient satisfaction of minority groups? a systematic review of literature. Worldviews Evid Based Nurs. 2016;13:402–10.
Allensworth-Davies D, Leigh J, Pukstas K, Geron SM, Hardt E, Brandeis G, et al. Country of origin and racio-ethnicity: are there differences in perceived organizational cultural competency and job satisfaction among nursing assistants in long-term care? Health Care Manage Rev. 2007;32:321–9.
Wesolowska K, Hietapakka L, Elovainio M, Aalto AM, Kaihlanen AM, Heponiemi T. The association between cross-cultural competence and well-being among registered native and foreign-born nurses in Finland. PLoS One. 2018;13:e0208761.
Choi, SY, Kim K. The Effects of Work Characteristics, Supervision, and Cultural Competence on Nurses' Burnout. BSBT. 2014;6(4):187-200. https://doi.org/10.14257/IJBSBT.2014.6.4.18.
OECD/European Union. Health at a Glance: Europe 2020: State of Health in the EU Cycle. Paris: OECD Publishing; 2020. https://doi.org/10.1787/82129230-en.
WHO. The World Health Report 2006. Geneva: Working together for health; 2006.
OECD. Foreign-trained doctors and nurses. 2017.
Khan-Gökkaya S, Mösko M. Labour market integration of refugee health professionals in Germany: challenges and strategies. Int Migr. 2021;59:105–26.
Narayanasamy A, White E. A review of transcultural nursing. Nurse Educ Today. 2005;25:102–11.
Schouten BC, Meeuwesen L. Cultural differences in medical communication: a review of the literature. Patient Educ Couns. 2006;64:21–34.
Marshall JK, Cooper LA, Green AR, Bertram A, Wright L, Matusko N, et al. Residents’ attitude, knowledge, and perceived preparedness toward caring for patients from diverse sociocultural backgrounds. Health Equity. 2017;1:43–9.
Karger AM, Lindtner-Rudolph H, Mroczynski R, Ziem A. Joksimovic L [’How strange is the patient to me?’]. Z Psychosom Med Psychother. 2017;63:280–96.
Brzoska P. Disparities in health care outcomes between immigrants and the majority population in Germany: a trend analysis, 2006–2014. PLoS One. 2018;13:e0191732.
Weech-Maldonado R, Dreachslin JL, Epane JP, Gail J, Gupta S, Wainio JA. Hospital cultural competency as a systematic organizational intervention: Key findings from the national center for healthcare leadership diversity demonstration project. Health Care Manage Rev. 2018;43:30–41.
Markey K, Tilki M, Taylor G. Understanding nurses’ concerns when caring for patients from diverse cultural and ethnic backgrounds. J Clin Nurs. 2018;27:e259–68.
Bradby H, Lindenmeyer A, Phillimore J, Padilla B, Brand T. “If there were doctors who could understand our problems, I would already be better”: dissatisfactory health care and marginalisation in superdiverse neighbourhoods. Sociol Health Illn. 2020;42:739–57.
Douglas MK, Rosenkoetter M, Pacquiao DF, Callister LC, Hattar-Pollara M, Lauderdale J, et al. Guidelines for implementing culturally competent nursing care. J Transcult Nurs. 2014;25:109–21.
Sorensen J, Norredam M, Dogra N, Essink-Bot ML, Suurmond J, Krasnik A. Enhancing cultural competence in medical education. Int J Med Educ. 2017;8:28–30.
Mews C, Schuster S, Vajda C, Lindtner-Rudolph H, Schmidt LE, Bösner S, et al. Cultural competence and global health: perspectives for medical education - position paper of the GMA committee on cultural competence and global health. GMS J Med Educ. 2018;35(3):Doc28.
Sharifi N, Adib-Hajbaghery M, Najafi M. Cultural competence in nursing: a concept analysis. Int J Nurs Stud. 2019;99: 103386.
Campinha-Bacote J. The Process of Cultural Competence in the Delivery of Healthcare Services: a model of care. J Transcult Nurs. 2002;13:181–4.
Alizadeh S, Chavan M. Cultural competence dimensions and outcomes: a systematic review of the literature. Health Soc Care Community. 2016;24:e117–30.
Beach MC, Price EG, Gary TL, Robinson KA, Gozu A, Palacio A, et al. Cultural competence: a systematic review of health care provider educational interventions. Med Care. 2005;43:356–73.
Price EG, Beach MC, Gary TL, Robinson KA, Gozu A, Palacio A, et al. A systematic review of the methodological rigor of studies evaluating cultural competence training of health professionals. Acad Med. 2005;80:578–86.
Chipps JA, Simpson B, Brysiewicz P. The effectiveness of cultural-competence training for health professionals in community-based rehabilitation: a systematic review of literature. Worldviews Evid Based Nurs. 2008;5:85–94.
Lie DA, Lee-Rey E, Gomez A, Bereknyei S, Braddock CH 3rd. Does cultural competency training of health professionals improve patient outcomes? a systematic review and proposed algorithm for future research. J Gen Intern Med. 2011;26:317–25.
Schouler-Ocak M, Graef-Calliess IT, Tarricone I, Qureshi A, Kastrup MC, Bhugra D. EPA guidance on cultural competence training. Eur Psychiatry. 2015;30:431–40.
Park HS, Jang HJ, Jeong GH. Effects of a cultural nursing course to enhance the cultural competence of nursing students in Korea. J Educ Eval Health Prof. 2019;16:39.
Kohli Bagwe T, Haskollar E. Variables Impacting Intercultural Competence: a Systematic Literature Review. J Intercult Commun Res. 2020;49:346–71.
Suk MH, Oh WO, Im Y. Factors affecting the cultural competence of visiting nurses for rural multicultural family support in South Korea. BMC Nurs. 2018;17:1.
Almutairi AF, Adlan AA, Nasim M. Perceptions of the critical cultural competence of registered nurses in Canada. BMC Nurs. 2017;16:47.
Çınar F. Examining the cross-cultural competencies of healthcare professionals as a health management strategy. J Soc Hum Sci Res. 2020;7:1073–85.
Casillas A, Paroz S, Green AR, Wolff H, Weber O, Faucherre F, et al. Cultural competency of health-care providers in a Swiss University Hospital: self-assessed cross-cultural skillfulness in a cross-sectional study. BMC Med Educ. 2014;14:19.
McCalman J, Jongen C, Bainbridge R. Organisational systems’ approaches to improving cultural competence in healthcare: a systematic scoping review of the literature. Int J Equity Health. 2017;16:78.
Truong M, Paradies Y, Priest N. Interventions to improve cultural competency in healthcare: a systematic review of reviews. BMC Health Serv Res. 2014;14:99.
Handtke O, Schilgen B, Mösko M. Culturally competent healthcare - a scoping review of strategies implemented in healthcare organizations and a model of culturally competent healthcare provision. PLoS One. 2019;14:e0219971.
Thomas DC, Liao Y, Aycan Z, Cerdin J-L, Pekerti AA, Ravlin EC, et al. Cultural intelligence: a theory-based, short form measure. J Int Bus Stud. 2015;46:1099–118.
Behr D, Braun M, Dorer B. Measurement Instruments in Cross-National Surveys (Version 2.0). (GESIS Survey Guidelines). Mannheim: GESIS - Leibniz-Institut für Sozialwissenschaften. 2016. https://doi.org/10.15465/gesis-sg_en_006.
Schenk L, Bau AM, Borde T, Butler J, Lampert T, Neuhauser H, et al. [A basic set of indicators for mapping migrant status. Recommendations for epidemiological practice]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2006;49:853–60.
Dansky KH, Weech-Maldonado R, De Souza G, Dreachslin JL. Organizational strategy and diversity management: diversity-sensitive orientation as a moderating influence. Health Care Manage Rev. 2003;28:243–53.
Brzoska P, Razum O. Challenges of Diversity-Sensitive Care in Medical Rehabilitation. Rehabilitation (Stuttg). 2017;56:299–304.
Sheperd SM, Willis-Esqueda C, Newton D, Sivasubramaniam D, Paradies Y. The challenge of cultural competence in the workplace: perspectives of healthcare providers. BMC Health Serv Res. 2019;19:135. https://doi.org/10.1186/s12913-019-3959-7.
Bernhard G, Knibbe RA, von Wolff A, Dingoyan D, Schulz H, Mosko M. Development and Psychometric Evaluation of an Instrument to Assess Cross-Cultural Competence of Healthcare Professionals (CCCHP). PLoS One. 2015;10:e0144049.
Meleady R, Seger CR, Vermue M. Evidence of a dynamic association between intergroup contact and intercultural competence. GPIR. 2021;24(8):1427-47. https://doi.org/10.1177/1368430220940400.
Acknowledgements
Not applicable.
Funding
Open Access funding enabled and organized by Projekt DEAL. This research was funded by the Federal Ministry of Education and Research (BMBF), Germany, under the funding line "Migration and Institutional Change" (funding codes: 01UM1810AY; 01UM1810BY). The funding conditions allowed for independent design and realisation of the study.
Author information
Authors and Affiliations
Contributions
L.S. conceptualised the methodological design of the study, analysed and interpreted the data, wrote, reviewed, edited and supervised the text. P.-T.S. was a major contributor in the construction of the questionnaire and the implementation of the online survey as well as the data review and analysis and was involved in the drafting of the manuscript. P.B. and Z.K. were involved in conducting the online survey and drafting the manuscript. Authors L.P. and M.S.-O. were involved in the acquisition of funding and conceptualised and reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Hospitals distributed an online link or a QR code for the study survey to the clinical staff via email or pay slip. The invitation to participate in the anonymous online survey contained information on the procedure and objectives of the study, the voluntary nature of study participation and data protection. Since there was no direct contact with the respondents and the survey was anonymous, we were not able to obtain a "classic" personal consent form. If the addressees agreed to participate in the study, they could click on the link or scan the QR code. As usual in such anonymous surveys, participation after detailed information had been provided was interpreted as declaration of consent. All methods were carried out in accordance with relevant guidelines and regulations. The consent procedure was approved by the Ethics Commission of the Charité – Universitätsmedizin Berlin and the Data Protection Officer of the Charité – Universitätsmedizin Berlin.
This study received the approval both of the Ethics Commission of the Charité – Universitätsmedizin Berlin (EA1/062/18) and the Data Protection Officer of the Charité – Universitätsmedizin Berlin.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schenk, L., Sonntag, PT., Beck, P. et al. Organisational and staff-related effects on cultural competence in the hospital setting: a cross-sectional online survey of nursing and medical staff. BMC Health Serv Res 22, 644 (2022). https://doi.org/10.1186/s12913-022-07947-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-022-07947-x