
Abstract
Background
The aims of this study were to evaluate the current awareness of and implementation by pharmacists in Japan of adjustment of drug dosage according to renal function (ADDR) in patients with chronic kidney disease (CKD) and to clarify the factors influencing implementation of ADDR by community pharmacists.
Methods
We conducted a web-based questionnaire of Japanese community and hospital pharmacists. Responders were compared by characteristics, rate of implementation of ADDR, experience with adverse drug events, pharmacist awareness of implementation of ADDR, and obstacles to ADDR implementation experienced by pharmacists. Additionally, the factors influencing the implementation of ADDR by community pharmacists were investigated by logistic regression analysis.
Results
Fewer community pharmacists had implemented ADDR than hospital pharmacists. The community pharmacists had less experience with adverse drug events caused by an inappropriate dosage than the hospital pharmacists, while the hospital pharmacists had encountered more severe adverse drug events than the community pharmacists. The community pharmacists had less awareness of ADDR implementation, and believed that problems in implementing ADDR were caused by a lack of information on the renal function of patients. In the logistic regression analysis, the factors influencing implementation of ADDR were “Routinely receiving prescriptions from nephrologists”, “Experience with adverse drug events caused by inappropriate dosage for CKD patients”, and “Awareness of the need for pharmacists to check the dosage of renally excreted drugs”; they did not include “Lack of information on patient renal function”.
Conclusions
This study indicates that fewer Japanese community pharmacists than hospital pharmacists implement ADDR and that implementation of ADDR by community pharmacists is hindered by their limited awareness of the importance of patient renal function. We advocate that many countermeasures be introduced to prevent CKD patients from experiencing adverse drug events caused by inappropriate dosage. Such countermeasures would include a training program to educate pharmacists about the impact of impaired renal function on dosage of drugs that are excreted by the kidneys.
Similar content being viewed by others

Background
Chronic kidney disease (CKD) is, an important and common health problem. Its incidence and prevalence are increasing worldwide. The estimated overall prevalence of CKD (glomerular filtration rate <60 mL/min/1.73 m2) in adults (aged ≥18) is increasing exponentially in the older population in Japan [1]. Pharmacokinetics are often altered in CKD patients [2]. In particular, the optimal dosages of renally excreted drugs are strongly affected by renal impairment. Dosages that do not take renal function into account are a major cause of increases in drug blood concentrations that lead to adverse drug events [3],[4]. Appropriate dosages of renally excreted drugs can be calculated on the basis of renal function using creatinine clearance. Thus, dosage adjustment based on renal function contributes to a reduction in the incidence of adverse drug events in older patients and others with renal impairment [5]-[7].
Adjustment of the drug dosage according to renal function (ADDR) by pharmacists, as a result of checking renal function and recommending alterations in their prescriptions, can prevent inappropriate dosages and thus reduce the incidence of the resulting adverse drug events [8],[9]. Hassan et al. [6] reported that hospital pharmacists can contribute to a reduction in the incidence of adverse drug events in patients with renal impairment. Conversely, the contribution of community pharmacists to ADDR seems limited in Japan [10] and in other countries [11]. Although hospital pharmacists can easily obtain information on patient renal function from medical records, community pharmacists may find it difficult. We might expect that the limited contribution to the implementation of ADDR by community pharmacists might be because of the unavailability of information on patient renal function in community pharmacies. However, the practical reasons remain unclear. We conducted a questionnaire-based survey to evaluate the current awareness of community pharmacists of ADDR for CKD patients in Japan and to compare the responses of community pharmacists with those of hospital pharmacists. Additionally, to clarify why community pharmacists are not implementing ADDR, we explored factors influencing its implementation.
Methods
Study design
A web-based survey was developed to investigate various factors relating to the pharmacotherapy of CKD patients. A web-based questionnaire has advantages that include access to individuals in distant locations, the ability to reach difficult-to-contact participants, and the convenience of having automated data collection, which reduces researcher time and effort [12]. The survey was conducted via the Internet using “Google Forms”, a questionnaire-style information-collecting system for efficiently administering questionnaires [13]. The items in the survey are listed in Table 1. Pharmacists were invited to participate via the relevant pharmacist association’s mailing lists in each geographical area and via pharmacists’ groups on social networking sites. Because the URL of the survey website consisted of a random character string, general surfers of the Internet could not access the site. The timeframe for responding was 1 month (from May 1st to 31st, 2013). We did not send any reminders. The survey data were compared with Japanese national statistics on pharmacists from the Survey of Physicians, Dentists and Pharmacists 2012 by the Ministry of Health, Labour and Welfare [14]. We had estimated the percentage of pharmacists with <5 years working experience by the age distribution from the national statistics. The Ethics Committee of Kumamoto University approved the study (no. 788).
Statistical analysis
All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Japan), which is a graphical user interface for R [15] (The R Foundation for Statistical Computing, Vienna, Austria). More precisely, EZR is a modified version of R Commander designed to add statistical functions frequently used in biostatistics [16]. Univariate analyses to compare community and hospital pharmacists were performed using the chi-square or Mann–Whitney U tests. Logistic regression analysis was used to identify the factors influencing implementation of ADDR by community pharmacists. Logistic regression was performed using stepwise model selection according to the Akaike information criterion [17]. Significance values were set at p <0.05 for interpreting the final multivariate logistic regression model.
Results
Relevant characteristics of responders
Relevant characteristics of responders are shown in Table 2. Two hundred eighty-four pharmacists responded to the survey, including 190 community pharmacists (66.9%) and 94 hospital pharmacists (33.1%). Forty-five (15.8%), 73 (25.7%), 101 (35.6%), and 65 (22.9%) pharmacists had worked for <5, 5–9, 10–20, and >20 years, respectively. The community pharmacists routinely dispensed prescriptions for a median of three hospital departments. Eighty pharmacists (39.2%) routinely dispensed prescriptions from nephrologists. The community pharmacists routinely dispensed prescriptions from significantly fewer departments and dispensed significantly fewer prescriptions from nephrologists than the hospital pharmacists. The responding pharmacists were distributed throughout Japan (40/47 prefectures). The ratios of community to hospital pharmacists in the national statistics and in our data set were 2.5:1 and 3:1, respectively. The estimated percentage of pharmacists with <5 years of working experience in the national statistics was approximately 15.4%; the percentage with <5 years working experience in our dataset was similar (15.8%).
Implementation of ADDR for CKD patients in Japan
We investigated the implementation of ADDR for CKD patients in Japan. Most hospital pharmacists (n = 86, 91.5%) implemented ADDR. In contrast, only about half of the community pharmacists (n = 103, 54.2%) had implemented ADDR (Table 3).
Experience with adverse drug events caused by inappropriate dosage for CKD patients
We investigated the pharmacists’ experience with adverse drug events caused by an inappropriate dosage for CKD patients. As shown in Table 3, significantly fewer community pharmacists (n = 22, 11.6%) than hospital pharmacists (n = 47, 50.0%) had experienced such adverse drug events. We also investigated which drugs had caused these adverse drug events. The drugs most frequently cited by hospital and community pharmacists were antivirals and pregabalin, respectively. We also identified other differences between community and hospital pharmacists in terms of their experience with such adverse drug events (Figure 1).

Renally-excreted drugs cited by pharmacists as having caused ADRs. aNSAIDs:Non-steroidal anti-Inflammatory drugs.
Awareness of pharmacotherapy for CKD patients
We examined the participating pharmacists’ awareness of pharmacotherapy for CKD patients. Significantly fewer community pharmacists than hospital pharmacists were aware of the need for “Checking of dosage of renally excreted drugs”, “Recommending dosage of renally excreted drugs to doctors”, and “Monitoring of drug-induced renal dysfunction” (Median Likert scale (IQR) = 4 (1) to 5 (0), 4 (1) to 5 (1), and 4 (1) to 5 (1)). The score distributions are shown in Figure 2.

Pharmacists’ awareness of pharmacotherapy for CKD in Japanese patients. The awareness score is the median score on the Likert scale for each item.
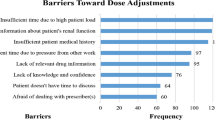
Obstacles to ADDR implementation reported by pharmacists
As shown in Table 4, more community pharmacists (n = 168, 88.4%) than hospital pharmacists (n = 13, 13.8%) responded that “Difficulty in obtaining information on patient renal function” was an obstacle to implementation of ADDR.
Factors influencing implementation of ADDR for CKD patients by community pharmacists
The final model of the logistic regression identified that the factors influencing implementation of ADDR by community pharmacists were “Routinely receiving prescriptions from nephrologists” (OR: 3.12, CI: 1.16–8.44), “Experience with adverse drug events caused by inappropriate dosage for CKD patients” (OR: 3.92, CI: 1.00–15.3), and “Awareness of need for pharmacists to check dosage of renally excreted drugs” (OR: 4.29, CI: 2.45–7.49) (Table 5).
Discussion
We demonstrated that community pharmacists had less awareness of and less frequently implemented ADDR for CKD patients than did hospital pharmacists. The less frequent implementation of ADDR by community pharmacists was attributable to differences in “Awareness of need for pharmacists to check dosage of renally excreted drugs”, “Routinely dispensing prescriptions from nephrologists”, and “Experience with adverse drug events caused by inappropriate dosage for CKD patients”.
Prescription errors, including inappropriate dosage for CKD patients, are associated with adverse drug events [18]-[21], and seem to be common. Via-Sosa et al. [11] and Joosten et al. [22] reported that community pharmacists sometimes dispense inappropriate dosages for CKD patients. In our study, half the participating community pharmacists had never implemented ADDR, and fewer community pharmacists than hospital pharmacists had implemented ADDR (Table 3). These findings suggest that community pharmacists sometimes dispense inappropriate dosages of drugs to CKD patients. Health care professionals’ awareness is influenced by their experience with clinical problems such as adverse drug events. In turn, the awareness of health care professionals, including pharmacists, greatly influences their behavior [23]-[25]. In our study, more hospital than community pharmacists had experienced adverse drug events (Table 3). Additionally, the hospital pharmacists had experienced more severe adverse drug events such as hospitalization and/or death than the community pharmacists (e.g., neurotoxicity of antivirals [26], digoxin intoxication [27]) (Figure 1). Fewer community pharmacists than hospital pharmacists were aware of the need to check and recommend appropriate dosages of renally excreted drugs and to monitor drug-induced renal dysfunction (Figure 2). Furthermore, in this study, pharmacists’ experience with adverse drug events was related to awareness of the need for checking and recommending appropriate dosages (data not shown). These findings suggest that hospital pharmacists have more experience with adverse drug events and that this results in them having more awareness of the need for ADDR. Thus, hospital pharmacists are more careful and are able to implement ADDR. In contrast, although many community pharmacists responded that checking the dosage was “important”, half of community pharmacists had not implemented ADDR. We believe there is a considerable gap between “important” and “very important”. Hence, we performed a subgroup analysis of the community pharmacists to compare awareness of the need for pharmacists to check dosage of renally excreted drugs and implementation of ADDR. Significantly more community pharmacists that had implemented ADDR responded that checking the dosage was “very important” rather than “important” (Additional file 1: Table S1). These results suggest a need for greater awareness among community pharmacists for implementing ADDR.
Most community pharmacists indicated that the most frequent obstacle to implementing ADDR was “Difficulty in obtaining information on patient renal function” whereas for most hospital pharmacists it was “Failure to check prescriptions because of pressure of other work” (Table 4). In Japan, community pharmacists generally do not have access to patient medical records, unlike hospital pharmacists. Thus, community pharmacists believe that their failure to implement ADDR is caused by a lack of information on patient renal function. However, about half the community pharmacists had implemented ADDR (Table 3). We therefore conclude that lack of information on renal function is not a critical factor in the failure of community pharmacists to implement ADDR.
To clarify the critical factors that influence implementation of ADDR by community pharmacists, we used logistic regression analysis. The final model of the logistic regression indicated that the influential factors were “Routinely dispensing prescriptions from nephrologists”, “Experience with adverse drug events caused by inappropriate dosage”, “Awareness of the need for pharmacists to check dosage of renally excreted drugs” (Table 5). However, “Difficulty in obtaining information about renal function” was not identified as a contributory factor. Additionally, in this study, dispensing prescriptions from nephrologists (i.e., participation in pharmacotherapy of CKD) tended to be related to awareness of the need for checking and recommending appropriate dosages (data not shown). These results are consistent with our argument that pharmacists’ experience with adverse drug events with CKD patients make them more likely to check prescriptions associated with ADDR policy. In contrast, in the Netherlands, the serum creatinine concentration is printed on prescriptions for designated drugs including renally excreted drugs (e.g., acyclovir) [28]. Recently, attempts to implement this policy have been made more frequently in Japan. However, although the serum creatinine concentration is generally an accurate indicator of renal function, this measure is less reliable in older people and those with malnutrition because of the loss of muscle mass [29]-[31]. Renal impairment is frequently overlooked in patients with such concealed renal impairment (normal serum creatinine concentrations and reduced estimated glomerular filtration rate), resulting in the prescription of inappropriate dosages [32]. Wong et al. [33] stressed that awareness that renal impairment can be accompanied by normal serum creatinine concentrations is important in preventing adverse drug events in older patients. These findings suggest that implementation of ADDR by community pharmacists would be best supported by not only providing information about serum creatinine concentrations, but also by the strategy of bringing renal impairment to the attention of pharmacists when they check prescriptions, by means, for example, of a computerized system that alerts the pharmacist to renal impairment. Joosten et al. [22] have demonstrated that a computer-based renal impairment alert system is effective. However, it would be difficult to introduce a computerized alert system for all community pharmacists. Conversely, training programs for physicians [7], medical staff [34], and community pharmacists [11] seem to reduce the percentage of inappropriate dosage prescriptions. Thus, training programs to educate community pharmacists on the risk of adverse drug events caused by inappropriate dosages for CKD patients and encouraging them to pay attention to renal impairment may be effective in increasing the rate of implementation of ADDR.
This study has some limitations. Data validation in this survey was not sufficient. Although we compared our data with national statistics, this survey data lacks some demographic characteristics of respondents, such as gender, age, and qualifications of the pharmacist. Furthermore, the questionnaire invitation was sent via a closed social network group and relevant pharmacist associations’ mailing lists. Because the exact number of invitees was unknown, we were not able to calculate a response rate and sample size. Additionally, this study has a sampling bias, which is a disadvantage of the survey method. A web-based questionnaire also has a self-selection/volunteer bias [35]. This survey might have been biased toward pharmacists who are concerned with or have an interest in ADDR. Thus, this study might have overestimated the percentage of pharmacists who have implemented ADDR. Conversely, a web-based survey is easier for participants to respond to because pharmacists who have not implemented ADDR might feel stigmatized if the survey were public [12]. Therefore, we chose the web-based approach as a means of obtaining more responses from pharmacists in Japan. Although further study will be needed, the results suggest the importance of awareness among pharmacists in implementing ADDR.
Conclusions
In summary, we have investigated the awareness and implementation of ADDR for CKD patients by community pharmacists. We found that community pharmacists commonly adjust inappropriate dosages of drugs for CKD patients. However, there is insufficient implementation of ADDR by community pharmacists and insufficient awareness of the need for community pharmacists to check prescriptions for patients with renal impairment and to implement ADDR. We believe that immediate measures such as training programs for community pharmacists are necessary to improve the current status of ADDR implementation in Japan by drawing their attention to the need to check prescriptions for patients with renal impairment.
Additional file
Change history
29 June 2021
A Correction to this paper has been published: https://doi.org/10.1186/s12913-021-06631-w
Abbreviations
- CKD:
-
Chronic kidney disease
- ADDR:
-
Adjustment of drug dosage according to renal function
References
Imai E, Horio M, Iseki K, Yamagata K, Watanabe T, Hara S, Ura N, Kiyohara Y, Hirakata H, Moriyama T, Ando Y, Nitta K, Inaguma D, Narita I, Iso H, Wakai K, Yasuda Y, Tsukamoto Y, Ito S, Makino H, Hishida A, Matsuo S: Prevalence of chronic kidney disease (CKD) in the Japanese general population predicted by the MDRD equation modified by a Japanese coefficient. Clin Exp Nephrol. 2007, 11: 156-163. 10.1007/s10157-007-0463-x.
Kappel J, Piera C: Safe drug prescribing for patients with renal insufficiency. Can Med Assoc J. 2002, 166: 473-477.
Manley HJ, Drayer DK, Muther RS: Medication-related problem type and appearance rate in ambulatory hemodialysis patients. BMC Nephrol. 2003, 4: 10-10.1186/1471-2369-4-10.
Manley HJ, Cannella CA, Bailie GR, St. Peter WL: Medication-related problems in ambulatory hemodialysis patients: a pooled analysis. Am J Kidney Dis. 2005, 46: 669-680. 10.1053/j.ajkd.2005.07.001.
Patel HR, Pruchnicki MC, Hall LE: Assessment for chronic kidney disease service in high-risk patients at community health clinics. Ann Pharmacother. 2005, 39: 22-27. 10.1345/aph.1E269.
Hassan Y, Al-Ramahi RJ, Aziz NA, Ghazali R: Impact of a renal drug dosing service on dose adjustment in hospitalized patients with chronic kidney disease. Ann Pharmacother. 2009, 43: 1598-605. 10.1345/aph.1M187.
Falconnier AD, Haefeli WE, Schoenenberger RA, Surber C, Martin-Facklam M: Drug dosage in patients with renal failure optimized by immediate concurrent feedback. J Gen Intern Med. 2001, 16: 369-75. 10.1046/j.1525-1497.2001.016006369.x.
Bhardwaja B, Carroll NM, Raebel MA, Chester EA, Korner EJ, Rocho BE, Brand DW, Magid DJ: Improving prescribing safety in patients with renal insufficiency in the ambulatory setting: the drug renal alert pharmacy (DRAP) program. Pharmacother J Hum Pharmacol Drug Ther. 2011, 31: 346-356. 10.1592/phco.31.4.346.
Erler A, Beyer M, Petersen JJ, Saal K, Rath T, Rochon J, Haefeli WE, Gerlach FM: How to improve drug dosing for patients with renal impairment in primary care - a cluster-randomized controlled trial. BMC Fam Pract. 2012, 13: 91-10.1186/1471-2296-13-91.
Tachi T, Kato M, Osawa T, Koda A, Fukuta M, Tanaka K, Aoyama S, Yasuda M, Mizui T, Goto C, Teramachi H: Economic evaluation of adjustments of levofloxacin dosage by dispensing pharmacists for patients with renal dysfunction. Yakugaku Zasshi. 2013, 133: 1223-1233. 10.1248/yakushi.13-00194.
Via-Sosa MA, Lopes N, March M: Effectiveness of a drug dosing service provided by community pharmacists in polymedicated elderly patients with renal impairment–a comparative study. BMC Fam Pract. 2013, 14: 96-10.1186/1471-2296-14-96.
Wright KB: Researching internet-based populations: advantages and disadvantages of online survey research, online questionnaire authoring software packages, and web survey services. J Comput-Mediat Commun. 2005, 10: 00-00. 10.1111/j.1083-6101.2005.tb00259.x.
Rayhan RU, Zheng Y, Uddin E, Timbol C, Adewuyi O, Baraniuk JN: Administer and collect medical questionnaires with Google documents: a simple, safe, and free system. Appl Med Inform. 2013, 33: 12.
Survey of Physicians, Dentists and Pharmacists in 2012. [], [http://www.mhlw.go.jp/toukei/saikin/hw/ishi/12/dl/kekka_3.pdf]
R Core Team: R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria, 2012. ISBN 3-900051-07-0; 2012.
Kanda Y: Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2012, 48: 452-458. 10.1038/bmt.2012.244.
Akaike H: Information theory and an extension of the maximum likelihood principle. Breakthr Stat. Edited by: Kotz S, Johnson NL. 1992, Springer, New York, 610-624. 10.1007/978-1-4612-0919-5_38. [Springer Series in Statistics]
Bates DW, Boyle DL, Vander Vliet MB, Schneider J, Leape L: Relationship between medication errors and adverse drug events. J Gen Intern Med. 1995, 10: 199-205. 10.1007/BF02600255.
Lesar TS, Briceland L, Stein DS: Factors related to errors in medication prescribing. JAMA J Am Med Assoc. 1997, 277: 312-317. 10.1001/jama.1997.03540280050033.
Beardsley JR, Schomberg RH, Heatherly SJ, Williams BS: Implementation of a standardized discharge time-out process to reduce prescribing errors at discharge. Hosp Pharm. 2013, 48: 39-47. 10.1310/hpj4801-39.
Basey AJ, Krska J, Kennedy TD, Mackridge AJ: Prescribing errors on admission to hospital and their potential impact: a mixed-methods study. BMJ Qual Saf. 2014, 23: 17-25. 10.1136/bmjqs-2013-001978.
Joosten H, Drion I, Boogerd KJ, Pijl EV Van D, Slingerland RJ, Slaets JPJ, Jansen TJ, Schwantje O, Gans ROB, Bilo HJG: Optimising drug prescribing and dispensing in subjects at risk for drug errors due to renal impairment: improving drug safety in primary healthcare by low eGFR alerts. BMJ Open. 2013, 3: e002068-10.1136/bmjopen-2012-002068.
Guan F, Xie J, Wang G-L, Wang J-H, Wang J-S, Yu J-M, Hu D-Y: Community-wide survey of physicians’ knowledge of cholesterol management. Chin Med J (Engl). 2010, 123: 884-889.
Adams OP, Carter AO: Knowledge, attitudes, practices, and barriers reported by patients receiving diabetes and hypertension primary health care in Barbados: a focus group study. BMC Fam Pract. 2011, 12: 135-10.1186/1471-2296-12-135.
Puspitasari HP, Aslani P, Krass I: Australian community pharmacists’ awareness and practice in supporting secondary prevention of cardiovascular disease. Int J Clin Pharm. 2013, 35: 1218-1228. 10.1007/s11096-013-9854-0.
Haefeli WE, Schoenenberger RAZ, Weiss P, Ritz RF: Acyclovir-induced neurotoxicity: concentration-side effect relationship in acyclovir overdose. Am J Med. 1993, 94: 212-215. 10.1016/0002-9343(93)90186-S.
Hirata S, Izumi S, Furukubo T, Ota M, Fujita M, Yamakawa T, Hasegawa I, Ohtani H, Sawada Y: Interactions between clarithromycin and digoxin in patients with end-stage renal disease. Int J Clin Pharmacol Ther. 2005, 43: 30-36. 10.5414/CPP43030.
Voortgang wijziging regeling “Reden van voorschrijven op recept en uitwisseling labwaarden” — knmp.nl. [], [http://knmg.artsennet.nl/Nieuws/Overzicht-nieuws/Nieuwsbericht/134105/Reden-van-voorschrijven-op-recept-en-labwaarden-uitwisselen.htm]
Lindeman RD: Assessment of renal function in the old. Special considerations. Clin Lab Med. 1993, 13: 269-277.
Corsonello A, Pedone C, Corica F, Mazzei B, Di Iorio A, Carbonin P, Incalzi RA: Concealed renal failure and adverse drug reactions in older patients with type 2 diabetes mellitus. J Gerontol A Biol Sci Med Sci. 2005, 60: 1147-1151. 10.1093/gerona/60.9.1147.
Corsonello A, Pedone C, Corica F, Mussi C, Carbonin P, Antonelli Incalzi R: Concealed renal insufficiency and adverse drug reactions in elderly hospitalized patients. Arch Intern Med. 2005, 165: 790-10.1001/archinte.165.7.790.
Kalender-Rich JL, Mahnken JD, Wetmore JB, Rigler SK: Transient impact of automated glomerular filtration rate reporting on drug dosing for hospitalized older adults with concealed renal insufficiency. Am J Geriatr Pharmacother. 2011, 9: 320-327. 10.1016/j.amjopharm.2011.08.003.
Wong NA, Jones HW: An analysis of discharge drug prescribing amongst elderly patients with renal impairment. Postgrad Med J. 1998, 74: 420-422. 10.1136/pgmj.74.873.420.
Baum S, Harder S: Appropriate dosing in patients with impaired renal function on medical wards before and after an educational intervention. Int J Clin Pharmacol Ther. 2010, 48: 29-35. 10.5414/CPP48029.
Eysenbach G, Wyatt J: Using the internet for surveys and health research. J Med Internet Res. 2002, 4: E13-10.2196/jmir.4.2.e13.
Acknowledgments
The authors are grateful to the participating pharmacists. We also thank the faculty of the Pharmaceutics Department of Kumamoto University for their constructive discussions and comments. This work was supported in Grants-in-Aid for Research from the OTC Self-Medication Promotion Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
YK designed this study. YK, ES, and TM performed the research. YK, YI, MI and TI analyzed the data. YK, YI, DK, SH and TI drafted the manuscript. All authors have read and approved the final manuscript.
The original version of this article was revised: Table 5 has been revised.
Electronic supplementary material
12913_2014_615_MOESM1_ESM.docx
Additional file 1: Table S1.: Relationship between awareness of need for pharmacists to check the dosage of renally excreted drugs and implementation of ADDR by community pharmacists. (DOCX 43 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

{kind=link}
{kind=link}
Cite this article
Kondo, Y., Ishitsuka, Y., Shigemori, E. et al. Awareness and current implementation of drug dosage adjustment by pharmacists in patients with chronic kidney disease in Japan: a web-based survey. BMC Health Serv Res 14, 615 (2014). https://doi.org/10.1186/s12913-014-0615-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-014-0615-0