
Abstract
Background
Screening for colorectal cancer (CRC) is suboptimal, particularly for vulnerable populations. Effective intervention programs are needed to increase screening rates. We used a discrete choice experiment (DCE) to learn about how vulnerable individuals in North Carolina value different aspects of CRC screening programs.
Methods
We enrolled English-speaking adults ages 50–75 at average risk of CRC from rural North Carolina communities with low rates of CRC screening, targeting those with public or no insurance and low incomes. Participants received basic information about CRC screening and potential program features, then completed a 16 task DCE and survey questions that examined preferences for four attributes of screening programs: testing options available; travel time required; money paid for screening or rewards for completing screening; and the portion of the cost of follow-up care paid out of pocket. We used Hierarchical Bayesian methods to calculate individual-level utilities for the 4 attributes’ levels and individual-level attribute importance scores. For each individual, the attribute with the highest importance score was considered the most important attribute. Individual utilities were then aggregated to produce mean utilities for each attribute. We also compared DCE-based results with those from direct questions in a post-DCE survey.
Results
We enrolled 150 adults. Mean age was 57.8 (range 50–74); 55% were women; 76% White and 19% African-American; 87% annual household income under $30,000; and 51% were uninsured. Individuals preferred shorter travel; rewards or small copayments compared with large copayments; programs that included stool testing as an option; and greater coverage of follow-up costs. Follow-up cost coverage was most frequently found to be the most important attribute from the DCE (47%); followed by test reward/copayment (33%). From the survey, proportion of follow-up costs paid was most frequently cited as most important (42% of participants), followed by testing options (32%). There was moderate agreement (45%) in attribute importance between the DCE and the single question in the post-DCE survey.
Conclusions
Screening test copayments and follow-up care coverage costs are important program characteristics in this vulnerable, rural population.
Similar content being viewed by others


Background
Screening reduces colorectal cancer (CRC) incidence and mortality, and is cost-effective [1],[2]. Unfortunately, CRC screening is underutilized, particularly in vulnerable populations, defined as those with low incomes, inadequate or no health insurance, or those who live far from health care facilities [3]-[6]. Data from national surveys suggest that over a third of US adults ages 50–75 are not up to date with CRC screening; levels are even lower for vulnerable populations: for example, fewer than 50% of those with no insurance report being up to date with CRC screening [6].
The US government’s Healthy People 2020 goals set a target of having 70.5% of eligible adults up to date with CRC screening by 2020 [7]. Effective programs to reach vulnerable populations (and increase their rates of CRC screening) are essential to bring the benefits of CRC screening to the full US population and reach national objectives. Increasing CRC screening is also an important part of payer-based healthcare quality improvement and pay for performance efforts.
Several types of interventions, including small media, patient and provider reminders, and possibly financial incentives are effective in increasing screening, and some of these interventions have been tested in vulnerable populations [8]. However, these effective interventions have not been widely disseminated [6]. Reasons for failure of dissemination may include intervention complexity, costs of intervention, challenges in scaling, or difficulty in choosing among potentially effective interventions. Policy makers and payers may need to decide among potential options for programs to increase CRC screening among vulnerable populations, including the option of maintaining the status quo.
For a screening program to be effective, it must be acceptable to the targeted population, easily accessible, and readily available at an acceptable price. Information on the public's preferences between types of screening programs will aid policy makers in designing, implementing and disseminating effective programs. One method for informing decisions about potential options for increasing CRC screening among vulnerable populations is to elicit feedback from members of vulnerable groups about the features of potential programs.
Discrete choice experiment (DCE) is one potentially valuable method for eliciting such feedback. DCE presupposes that a “product” like a screening promotion program can be described in terms of its features or “attributes” and that by understanding the different features and how people value them, effective programs can be designed and implemented to address the needs of the population [9]. Although stated preference methods, including DCE, have been used to understand patient preferences for different CRC screening tests [10]-[12], to our knowledge, DCE has not been used in the design of programs to increase CRC screening among vulnerable populations in the US, such as those with low income or those who are under- or uninsured. As such, we designed and performed a DCE among members of vulnerable populations in North Carolina to provide information to assist policymakers in the design and implementation of programs to promote CRC screening.
Methods
Overview
We identified rural North Carolina counties with low CRC screening rates and elevated CRC mortality by linking North Carolina Cancer registry data to Medicare and Medicaid claims data using demonstrated methods [13],[14]. Three counties in western North Carolina were selected for further study. We then recruited and surveyed English-speaking, adults ages 50–75 at average risk for CRC about their preferences and values regarding possible CRC screening programs.
Ethical considerations
This study was approved by the Institutional Review Board at the University of North Carolina at Chapel Hill.
Survey content
The study team designed a paper-based survey based on our prior research [10],[11], existing literature [15]-[19], and pre-testing feedback (See Additional file 1). The survey began with general information about colon cancer and features of colon cancer screening programs and asked participants to complete a DCE, a rating task and several additional questions. We used the term “colon cancer” rather than “colorectal cancer” to ensure understanding among the target population.
Discrete choice experiments
In a DCE, individuals are asked to choose between hypothetical alternatives described by a set of attributes and levels. The levels of the attributes are varied systematically in a series of choice tasks where participants are asked to select an option that they most prefer. Responses to the choices are modeled to provide quantitative information about the relative value participants attach to different levels of the attributes being considered [20].
Selection of key attributes and levels
We developed four key attributes of CRC screening programs from the literature and prior research, which include, testing options, travel time, money paid for screening, and the portion of the cost of follow-up care paid out of pocket [10],[11],[16]-[19].
We developed a plausible range of levels for each attribute. We framed the testing options attribute by employing four levels: two without a choice (stool test only; colonoscopy only) and two options with a choice (choice of stool test or colonoscopy; choice of stool test, colonoscopy, or CT colonography).We did not include sigmoidoscopy as one of the testing options within a program because our formative research suggested it was not readily available in the study area.
Travel time options ranging from “no travel” to “1 hour + .” were based on distances to nearest endoscopy facilities from our formative work [13]. These times are suitable for the rural geographic region where the study occurred and allowed individuals who may have difficulty conceptualizing distance (e.g. individuals who do not drive) to state their preference.
Money paid for screening was framed to include rewards and costs (copayments) within the same attribute, ranging from a $100 reward to a $1000 cost, with the highest amount of cost designed to simulate the cost of colonoscopy screening without insurance coverage. [21].
We represented out-of-pocket follow-up costs using percentages rather than absolute costs because it is impossible to know what the out-of-pocket follow-up costs might be with the selection of any given screening test. The outcome of the initial screening test and subsequent testing or treatment utilized, factor into the total out-of-pocket costs, and will differ for each individual. Given the uncertainty and difficulty in making a choice among these levels, we decided to frame the levels in a way that is likely to be familiar to individuals - as insurance coverage. The levels ranged from no coverage (100% paid by the person) to a 20% copayment, to full coverage (0% out of pocket expense).
Development of the DCE
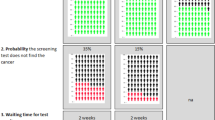
We used Sawtooth Software Version 8 to design a balanced and efficient set of 16 choice tasks (with 1 dominant task): this number of questions has been shown in past work to be feasible for participants to complete [10],[11]. Each choice was comprised of two active screening options and a fixed “opt-out” option (“Given these options, I would not get screened”). A sample choice task is included in Figure 1. Our study followed the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Guidelines [22] for DCE design.

An example discrete choice experiment task.
Post-DCE questions
Following the DCE, participants completed a rating task where they were asked to rate screening program attributes (on a scale from 0, meaning not important at all, to 5, very important, which were converted to a 1 to 6 scale for analysis). Participants were then asked to answer which single program attribute was most important- we called this the “directly selected most important attribute”.
Pretesting
The survey was pre-tested with 53 individuals in 6 gender-stratified focus groups held in 2 eastern North Carolina counties and 3 western North Carolina counties, from March 28, 2012 to September 7, 2012. Based on participant feedback, the survey was modified to include a table of pictograms comparing CRC screening options, and bulleted, condensed text to improve readability and comprehension. The table of pictograms illustrating screening test options was drawn from evidence-based materials from the National Cancer Institute (http://gutcheck.cancer.gov/screenings/index.html) and from clip art (See Additional file 1).
Data collection
Participants were recruited from community-based organizations in the region from October 23, 2012 to March 23, 2013. Eligibility criteria included residing in the area of interest (in an identified county or in an adjacent county), being 50 – 75 years of age, having average risk for CRC (i.e. no personal or family history of CRC and no history of inflammatory bowel disease), having a life expectancy of 2+ years, and being able to read English.
Participants were identified and screened for eligibility by one of two methods. Most commonly, individuals learned of the study and called a dedicated phone number, were screened by study personnel, and scheduled an appointment to be surveyed at survey sites, including flea markets, senior centers, discount stores, public housing authorities and medical clinics. Additionally, participants were recruited in-person at survey sites and were screened and administered surveys on a walk-in basis.
To ensure sufficient representation of vulnerable populations within the sample, the study team adopted a purposeful sampling approach for recruitment. We sought to enroll uninsured individuals (at least 50%) or publicly insured individuals (Medicare, Medicaid, Veterans benefits); individuals who were not up-to-date with screening (colonoscopy more than 10 years ago, sigmoidoscopy more than 5 years ago, Fecal Occult Blood Test (FOBT) or Fecal Immunochemical Test (FIT) more than one year ago); individuals who have a low annual household income (< $45,000); and minority groups (African-American and Hispanic participants).
Participants provided consent and were asked to take the survey in semi-private areas. The survey was administered on paper. Each individual was given the option of having the entire survey read aloud by a study team member. Study team members carefully explained how to complete the survey and took the time to explain the DCE process, and went through a practice DCE task to help reduce concerns and uncertainties about how to answer DCE questions. Upon completion of the survey, participants received a $35 gift card.
Study outcomes
The primary outcomes of interest were the mean utility levels for the four attributes, and the DCE-calculated most important attributes for each individual, based on their individual utility levels. Secondary outcomes of interest include the directly reported single most important attribute and the agreement between the DCE-generated and directly selected most important attribute.
Sample size determination
Because there is no optimal method for determining the sample size for DCE, we used the method suggested by Johnson to determine that a sample size of 150 participants would yield reasonably precise estimates of utility levels, given the use of 16 choice tasks, two active alternatives, and a maximum number of levels within a single attribute of six [23]. We continued recruitment until we reached this goal.
Statistical analysis
We performed descriptive analyses with means and proportions using Stata version 12.
The DCE survey responses were analyzed using Choice Based Conjoint (CBC) Hierarchical Bayesian (HB) module in Sawtooth Software to obtain individual-level preferences. The CBC/HB module uses data from the DCE in a mixed effects multivariate, multinomial logit model to estimate the value or “utility” each participant attaches to the different levels of the 4 attributes. The value associated with the “opt-out” choice is expressed as a constant [24].
The Hierarchical Bayesian process used in Sawtooth Software is a two-step process to determine individual-level utilities. First, average utilities are calculated for the full sample of participants, and how much each individual’s responses differ from the average. Secondly, individual utilities are adjusted to an optimal mix of average sample utilities and individual utilities, based on the amount of information provided by participants and the variance in the sample average (Markov Chain Monte Carlo). These individual-level utility estimates are then averaged to give the population mean utilities [24].
Utilities are arbitrarily-scaled, zero-centered values that represent the relative desirability of the levels within each attribute in numerical form: the higher the number the more desirable it is to participants and conversely, the lower (more negative) the number, the less desirable it is to participants [20]. Each participant’s utilities are then used to calculate individual-level attribute importance scores. Attribute importance scores represent the relative importance of the four attributes, given the range of levels employed [20]. Attribute importance scores were calculated for each individual separately and then averaged for mean importance scores.
For each individual, the attribute with the highest importance score from the DCE is considered to be “most important” for that individual. We compared the DCE-based most important attribute with the most important attribute based on a single post-DCE survey question to determine if they represented different information.
Results
There were 360 individuals who expressed interest in the study and 175 potential participants were found eligible. Twenty-four participants declined participation, 1 did not complete, and 150 individuals completed the survey (85.7%).
Participant characteristics are shown in Table 1. Mean age was 58 years, and 55% were female. Most (76%) were White and 40% had a high school education or less. Participants had low household incomes (87% reported less than $30,000 per year) and 51% were uninsured. Most (76%) had never been screened for CRC.
Mean utility levels are shown in Table 2. The negative constant associated with “Given these options, I would not get screened” suggests a strong overall preference for participation in CRC screening programs. Over 80% of respondents answered the dominant question correctly, suggesting good understanding and engagement in the survey.
As predicted, participants preferred no or shorter travel times compared with longer travel times. They also exhibited strong preferences for the larger ($100) reward for screening and against the highest screening test copayment of $1000. Interestingly, they had few differences in utility among small ($10) rewards, small-moderate copayments ($25- $100), or the lack of a reward or copayment. These findings suggest that individuals would be more likely to be screened if given a large reward (small rewards and copayments are less likely to have a significant impact) and would be discouraged from participating in a program where they had to bear large costs for screening.
The proportion of follow-up costs covered by the screening program was also important: participants strongly preferred full or nearly full coverage of follow-up costs compared with programs in which they would be responsible for 50 or 100% of these costs.
Utility levels for test choices available within the hypothetical screening programs had a less consistent pattern. In general, participants appeared to value having the option of stool test screening, whether as the only testing option or as part of a suite of options that included CT colonography and colonoscopy. In contrast, programs offering colonoscopy as the only option or offering a choice of stool test or colonoscopy were relatively less popular.
Mean attribute importance scores, which reflect the relative importance of the four attributes compared to one another, given the levels of the attributes employed, suggested that the cost variables were relatively more important than testing options or travel time: follow-up care cost had a 34% importance score, followed by money paid for screening (reward or copayment) at 33%. The other attributes, testing options (17%) and travel time (16%), were somewhat less important given the ranges of levels tested.
Post-DCE survey
In the post-DCE survey, participants’ ratings of the importance of the attributes had some similarities to the DCE results: the cost of follow-up care was rated to be very important (mean 5.5, SD 1.1 on a 1–6 scale), while travel time was rated to be of lower importance (mean 3.4, SD 1.8). In contrast, testing options were considered to be quite important (mean 5.3, SD 1.2), and out of pocket costs or rewards somewhat less so (mean 4.6, SD 1.8).
The most important attribute, based on a single question, was most frequently found to be the costs of follow-up care (42%), followed by testing options (32%), and out of pocket screening test costs or rewards (23%). Only 1.3% of participants considered travel time to be most important.
Agreement between DCE and survey results
Table 3 shows the agreement between participants’ most important attribute as calculated from the DCE in comparison with their responses to the single question from the post-DCE survey. Overall, 66 of 148 (45%) participants had agreement between these two methods for assessing attribute importance, with most differences coming from differences between methods in the value attributed to testing options compared with costs.
Discussion
In our survey of vulnerable adults in North Carolina, we found strong overall interest in programs to promote CRC screening. Program costs, both those associated with screening and those related to follow-up costs after initial screening, strongly influenced participants’ preferences. Participants’ responses also seemed to favor programs that included the option of stool testing, which may also reflect concerns about the costs of screening colonoscopy. Somewhat surprisingly, travel time appeared relatively much less important, perhaps reflecting the rural setting for our survey; residents of rural areas may be more accustomed to traveling relatively long distances and times to obtain health care, and hence attribute less relative importance to it.
Our study is the first, to our knowledge, to use DCE to examine features of potential CRC screening programs in the United States (US). Our findings have several potential implications for US health policy and for future research. First, they suggest that in order to maximize uptake and effectiveness, policymakers could encourage the development of programs that account for both initial screening costs and subsequent costs for additional testing (e.g. diagnostic and surveillance colonoscopy) and cancer treatment. The uncertainty associated with the magnitude of the follow-up costs may be a particularly important barrier to overcome.
Secondly, such programs could include the option of stool testing, which can be performed at home and has lower “up-front” effort and costs required compared with screening colonoscopy. Along these lines, Inadomi and colleagues found that uptake of CRC screening in a vulnerable urban population was higher when patients were offered FOBT alone or the option of FOBT or colonoscopy compared with only offering screening colonoscopy [25].
Our work suggests that DCE is a feasible technique for eliciting preferences of vulnerable individuals about potential health promotion policies. Based on prior behavioral economics research [26],[27], we expected to see stronger negative preferences for the modest copayments and more strongly positive preferences for the modest reward levels; the lack of such effects suggests that the relatively small monetary copayments or rewards may have little effect themselves on program uptake, at least in comparison with the extreme levels (e.g. those associated with having to pay for screening colonoscopy completely out of pocket). Also, our DCE results differed somewhat from our direct question results, with the DCE suggesting a great deal of importance attached to costs whereas the direct questions also found considerable importance attached to testing options. These results suggest that the different techniques (DCE and direct questions) may have complementary value [10],[11].
Our findings should be considered in light of several limitations. Foremost, we examined participants’ stated preferences; their actual behaviors (e.g. actual participation in screening programs) may differ. Secondly, we were only able to test a limited number of attributes and levels while maintaining a feasible and valid survey design; including other attributes or different levels within attributes, may have produced somewhat different results. That said, we believe that the attributes and levels we chose are relevant and well supported in the literature. The participants’ responses about the choice of screening tests available within the screening program were somewhat complex and hard to interpret: they reflected participants’ feeling about the specific tests as well as about the value of having options. It appears participants attached particular value to having stool testing as one of the options, but did not necessarily value more choice simply for the sake of having more options. Moreover, participants received brief, high-quality, evidence-based information about the testing options, but because we were studying preferences for screening programs, we did not evaluate their understanding of the nuances of each test.
We chose to represent out of pocket follow-up costs with percentages rather than absolute amounts because the amounts of out of pocket follow-up costs vary so much according to whether the person always screens negative (and hence has no additional costs), requires diagnostic colonoscopy with or without polypectomy, or is diagnosed with cancer and requires treatment. Given this uncertainty, we sought to simulate how insurance programs address costs, ranging from no coverage (100% paid by the person) to a 20% copayment, to full coverage (0% out of pocket expense). Not surprisingly, this attribute was considered very important, and reinforces the need for policymakers to consider follow-up care costs when designing screening programs.
Our sample size of 150 was sufficient, based on expert opinion, to examine appropriately differentiate overall preferences for the levels tested. However, we cannot exclude that a larger sample may not be able to further differentiate small degrees of difference in preferences. Finally, we collected information from one (rural) region of North Carolina; results from other parts of the state or from other states, may differ.
Conclusions
Despite these limitations, our results suggest that programs to encourage CRC screening among vulnerable individuals are likely to be most effective if they account for both the direct costs of screening as well as the follow-up costs of additional testing and treatment and if they include a stool test option. In our future work, we will use these findings to compare the cost-effectiveness of different means to increase CRC screening at the state level through organized programs, to help provide information and guidance about efficiency as well as potential effectiveness.
Additional files
Abbreviations
- CT:
-
Computerized tomography
- CRC:
-
Colorectal cancer
- DCE:
-
Discrete choice experiment
- FIT:
-
Fecal immunochemical test
- FOBT:
-
Fecal occult blood test
- ISPOR:
-
International Society for Pharmacoeconomics and Outcomes Research
- SD:
-
Standard deviation
References
Pignone M, Rich M, Teutsch SM, Berg AO, Lohr KN: Screening for colorectal cancer in adults at average risk: a summary of the evidence for the U.S. preventive services task force. Ann Intern Med. 2002, 137 (2): 132-141. 10.7326/0003-4819-137-2-200207160-00015.
Pignone M, Saha S, Hoerger T, Mandelblatt J: Cost-effectiveness analyses of colorectal cancer screening: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2002, 137 (2): 96-104. 10.7326/0003-4819-137-2-200207160-00007.
Beyer KM, Comstock S, Seagren R, Rushton G: Explaining place-based colorectal cancer health disparities: evidence from a rural context. Soc Sci Med. 2011, 72 (3): 373-382. 10.1016/j.socscimed.2010.09.017.
Cole AM, Jackson JE, Doescher M: Colorectal Cancer Screening Disparities for Rural Minorities in the United States. J Prim Care Community Health. 2012, 4 (2): 106-111. 10.1177/2150131912463244.
Stanley SL, King JB, Thomas CC, Richardson LC: Factors associated with never being screened for colorectal cancer. J Community Health. 2013, 38 (1): 31-39. 10.1007/s10900-012-9600-x.
Vital signs: colorectal cancer screening test use — United States, 2012. MMWR. 2013, 62 (44): 881-888.
Healthy People 2020 Disparities in Clinical Preventive Services [], [http://www.healthypeople.gov/2020/LHI/clinicalPreventive.aspx?tab=data]
The Community Guide: Cancer Prevention and Control [], [http://www.thecommunityguide.org/cancer/index.html]
Viney R, Lancsar E, Louviere J: Discrete choice experiments to measure consumer preferences for health and healthcare. Expert Rev Pharmacoecon Outcomes Res. 2002, 2 (4): 319-326. 10.1586/14737167.2.4.319.
Pignone MP, Brenner AT, Hawley S, Sheridan SL, Lewis CL, Jonas DE, Howard K: Conjoint analysis versus rating and ranking for values elicitation and clarification in colorectal cancer screening. J Gen Intern Med. 2012, 27 (1): 45-50. 10.1007/s11606-011-1837-z.
Brenner A, Howard K, Lewis C, Sheridan S, Crutchfield T, Hawley S, Reuland D, Kistler C, Pignone M: Comparing 3 values clarification methods for colorectal cancer screening decision-making: a randomized trial in the US and Australia. J Gen Intern Med. 2014, 29 (3): 507-513. 10.1007/s11606-013-2701-0.
Wortley S, Wong G, Kieu A, Howard K: Assessing stated preferences for colorectal cancer screening: a critical systematic review of discrete choice experiments. Patient. 2014, 7 (3): 271-282. 10.1007/s40271-014-0054-3.
Wheeler SB, Kuo TM, Goyal RK, Meyer AM, Hassmiller Lich K, Gillen EM, Tyree S, Lewis CL, Crutchfield TM, Martens CE, Tangka F, Richardson LC, Pignone MP: Regional variation in colorectal cancer testing and geographic availability of care in a publicly insured population. Health Place. 2014, 29: 114-123. 10.1016/j.healthplace.2014.07.001.
Meyer AM, Olshan AF, Green L, Meyer A, Wheeler SB, Basch E, Carpenter WR: Big data for population-based cancer research: the integrated cancer information and surveillance system. N C Med J. 2014, 75 (4): 265-269.
Van Dam L, Hol L, De Bekker-Grob EW, Steyerberg EW, Kuipers EJ, Habbema JD, Essink-Bot ML, Van Leerdam ME: What determines individuals’ preferences for colorectal cancer screening programmes? A discrete choice experiment. Eur J Cancer. 2010, 46 (1): 150-159. 10.1016/j.ejca.2009.07.014.
Marshall DA, Johnson FR, Kulin NA, Özdemir S, Walsh JME, Marshall JK, Van Bebber S, Phillips KA: How do physician assessments of patient preferences for colorectal cancer screening tests differ from actual preferences? A comparison in Canada and the United States using a stated-choice survey. Health Econ. 2009, 18 (12): 1420-1439. 10.1002/hec.1437.
Howard K, Salkeld G: Does attribute framing in discrete choice experiments influence willingness to pay? Results from a discrete choice experiment in screening for colorectal cancer. Value Health. 2009, 12 (2): 354-363. 10.1111/j.1524-4733.2008.00417.x.
Nayaradou M, Berchi C, Dejardin O, Launoy G: Eliciting population preferences for mass colorectal cancer screening organization. Med Decis Making. 2010, 30 (2): 224-233. 10.1177/0272989X09342747.
Hol L, De Bekker-Grob EW, Van Dam L, Donkers B, Kuipers EJ, Habbema JD, Steyerberg EW, Van Leerdam ME, Essink-Bot ML: Preferences for colorectal cancer screening strategies: a discrete choice experiment. Br J Cancer. 2010, 102 (6): 972-980. 10.1038/sj.bjc.6605566.
Orme B: Interpreting the Results of Conjoint Analysis. Getting Started with Conjoint Analyis: Strategies for Product Design and Pricing Research. 2010, Research Publishers, Madison, Wisc, 77-88. 2
Promberger M, Dolan P, Marteau TM: “Pay them if it works”: discrete choice experiments on the acceptability of financial incentives to change health related behaviour. Soc Sci Med. 2012, 75 (12): 2509-2514. 10.1016/j.socscimed.2012.09.033.
Bridges JF, Hauber AB, Marshall D, Lloyd A, Prosser LA, Regier DA, Johnson FR, Mauskopf J: Conjoint analysis applications in health–a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2011, 14 (4): 403-413. 10.1016/j.jval.2010.11.013.
Orme B: Sample Size Issues for Conjoint Analysis. Getting Started with Conjoint Analysis: Strategies for Product Design and Pricing Research. 2010, Research Publishers, Madison, Wisconsin, 57-66. 2
The CBC/HB System for Hierarchical Bayes Estimation Version 5.0. Sawtooth Software: Technical Paper Series. 2009, Sawtooth Software, Sequim, WA, 1-32. http://www.sawtoothsoftware.com/download/techpap/hbtech.pdf, [http://www.sawtoothsoftware.com/download/techpap/hbtech.pdf]
Inadomi JM, Vijan S, Janz NK, Fagerlin A, Thomas JP, Lin YV, Munoz R, Lau C, Somsouk M, El-Nachef N, Hayward RA: Adherence to colorectal cancer screening: a randomized clinical trial of competing strategies. Arch Intern Med. 2012, 172 (7): 575-582. 10.1001/archinternmed.2012.332.
Sutherland K, Christianson JB, Leatherman S: Impact of targeted financial incentives on personal health behavior: a review of the literature. Med Care Res Rev. 2008, 65 (6 Suppl): 36S-78S. 10.1177/1077558708324235.
Marteau TM, Ashcroft RE, Oliver A: Using financial incentives to achieve healthy behaviour. BMJ. 2009, 338: b1415-10.1136/bmj.b1415.
Acknowledgements
This publication is a product of a Prevention Research Center and MP, TC, PB, SH, JL, CL, KHL and SW were funded by the Centers for Disease Control and Prevention (CDC) Special Interest Project, “Behavioral economics of colorectal cancer screening in underserved populations” (CDC-SIP-11-041, Co-PIs: Pignone and Wheeler) SBW was further supported by the Agency for Healthcare Research and Quality (AHRQ), 1-K-12 HS019468-01 Mentored Clinical Scientists Comparative Effectiveness Development Award (PI: Weinberger; Scholar: Wheeler). LCR & FT were funded through their roles at the Centers for Disease Control and Prevention and were involved in the study design, data analysis, data interpretation, and writing of the manuscript. The authors thank Linda Block, Deborah Briggs, Sandra Diehl, and Marjorie Vestal for their assistance with data collection and the creators of gutcheck.cancer.gov for the images used in the survey instrument.
Disclaimer
The findings and conclusions in this paper are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All authors have made significant contributions to the published study. All were involved in the conception and design of the research study. TC and JL were involved in data collection. MP and TC carried out the analyses. All authors aided in interpretation of results and revision of the manuscript. All authors have read and approved the final manuscript.
Electronic supplementary material
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

{kind=link}
Cite this article
Pignone, M.P., Crutchfield, T.M., Brown, P.M. et al. Using a discrete choice experiment to inform the design of programs to promote colon cancer screening for vulnerable populations in North Carolina. BMC Health Serv Res 14, 611 (2014). https://doi.org/10.1186/s12913-014-0611-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-014-0611-4