
Abstract
Objectives
The purpose of this study was to investigate fatigue, mental workload, and burnout among health care workers (HCWs) and explore the possible underlying factors.
Materials and methods
An online cross-sectional survey design was used to collect data from HCWs in Chongqing, China. The online survey included the Fatigue Severity Scale, NASA Task Load Index, and Chinese version of the Maslach Burnout Inventory-General Survey to assess fatigue, mental workload, and burnout, respectively, and was conducted from February 1 to March 1, 2023.
Results
In this study, the incidence of fatigue and burnout among HCWs was 76.40% and 89.14%, respectively, and the incidence of moderate to intolerable mental workloads was 90.26%. Work–family conflict, current symptoms, number of days of COVID-19 positivity, mental workload, burnout and reduced personal accomplishment were significantly associated with fatigue. Mental workload was affected by fatigue and reduced personal accomplishment. Furthermore, burnout was influenced by marital status and fatigue. Moreover, there was a correlation among mental workload, fatigue, and burnout.
Conclusions
Fatigue, mental workload and burnout had a high incidence and were influenced by multiple factors during COVID-19 public emergencies in China.
Similar content being viewed by others


Introduction
Public health emergencies often trigger psychological distress among individuals and communities due to their sudden, urgent, and serious nature, as well as the high level of uncertainty they cause [1]. Due to their unique work environment, high levels of stress, and increased risk of infection, frontline healthcare workers (HCWs) who provide care and services to sick people often experience mental health issues during public health emergencies [2, 3]. They may experience symptoms such as fatigue, high mental workload, and burnout, which have negative consequences such as medical errors, poor quality of care, and increased patient mortality [4,5,6].
Fatigue primarily manifests as physical and mental exhaustion, including reduced concentration and motivation [7, 8]. Fatigue has become common among HCWs during the COVID-19 pandemic, with a moderate to high prevalence of 35.06–72.2% [9, 10]. Cardiopulmonary symptoms, psychiatric symptoms, and muscle weakness may also occur following COVID-19 infection [11], facilitating the physical exhaustion of HCWs. In addition, limited social interactions due to isolation measures and different viral transmission routes have led to mental fatigue among HCWs. All of these factors exacerbate their symptoms of fatigue, resulting in declines in work quality and poor patient outcomes [12, 13].
Moreover, previous studies have shown that the occurrence of an epidemic adversely affects the mental health of HCWs, including the loss of self-confidence and inability to make decisions [14, 15]. The occurrence of these factors affects the mental workload of HCWs. Mental workload is defined as the weight, cost, and quantity of effort needed to complete occupational tasks, referring to the ability to process information, make clinical decisions, and communicate with patients and their families [16,17,18]. A high mental workload contributes to fatigue, decreased efficiency, poor performance, and increased patient mortality [19,20,21].
Furthermore, more than 50% of HCWs experience severe fatigue and have a heavy mental workload, which can lead to burnout [22]. Maslach and Jackson defined burnout as a reaction to chronic and long-term stress in the workplace characterized by three aspects: emotional exhaustion (EE), depersonalization (DP), and reduced personal accomplishment (RPA) [23]. Notably, burnout generally increases over time [24]. From the peak of the Wuhan COVID-19 epidemic to the strict zero-COVID-19 policy period, the overall incidence of burnout decreased slightly from 51.7 to 50.4% [22, 25], indicating that the overall incidence of burnout among HCWs remained high. Chronic burnout can lead to physical or psychological issues, poor quality of care, medical malpractice, and increased organizational costs [26,27,28]. However, the incidence of burnout after the strict zero-COVID-19 policies were relaxed is not known, but the reality is not promising.
We hypothesized that the incidence of fatigue, mental workload, and burnout among HCWs was high and that HCWs were strongly affected by the COVID-19 pandemic. Therefore, this study aimed to investigate fatigue, mental workload, and burnout among HCWs and explore their interrelationships. Understanding the mental health of HCWs in this ongoing situation will help us develop better coping mechanisms.
Materials and methods
Study design and participants
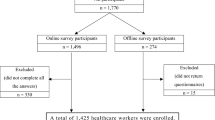
An online cross-sectional study of HCWs was conducted from February 1 to March 1, 2023. The inclusion criteria were as follows: (1) individuals who provided consent to participate in this study and (2) HCWs, including registered doctors, nurses, and technicians. HCWs who were unwilling to participate in this study were excluded.
Materials
Demographic data questionnaires
Individual and occupational characteristic data were self-reported by the participants and included age, sex, marital status, education level, profession, hospital level, hospital department, work year, intensity of work, work pressure, and work-family conflict. The following data related to personal virus infection were collected: COVID-19 infection status, current symptoms, number of days of COVID-19 positivity, and number of days until recovery from COVID-19.
Fatigue severity scale (FSS)
The FSS, which was developed in 1989 by Krupp [29, 30], is mainly used to assess the severity of fatigue. The scale consists of 9 items scored using a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). The total score ranges from 9 to 63 points, with higher scores indicating greater fatigue. A score of 36 points is the threshold, with a score < 36 points indicating no fatigue and a score ≥ 36 points indicating the presence of fatigue [31]. The Cronbach’s α for the FSS in the present study was 0.940.
NASA Task load index (NASA-TLX)
Mental workload was assessed with the NASA-TLX. The NASA-TLX, which was designed in the 1970s, was originally developed to measure workload stress among aerospace workers and consists of six dimensions: mental demand, physical demand, temporal demand, performance, effort and frustration [32, 33]. Each dimension is represented by a straight line on a 20-point scale ranging from 0 to 100, and a higher score indicates a greater mental workload [34]. Mental workload was classified based on the NASA-TLX score as follows: scores of 0–20, low; scores of 21–40, mild; scores of 41–60, moderate; scores of 61–80, high; and scores of 81–100, intolerable [35]. The Cronbach’s α in this study was 0.826.
The Chinese version of the Maslach Burnout Inventory-General Survey (MBI-GS)
The Chinese version of the MBI-GS was used to measure burnout and has three dimensions: the EE, DP and RPA [36]. The RPA items are reverse scored. Each item is rated on a 7-point Likert scale ranging from 0 (never) to 6 (every day). According to the evaluation criteria of Li et al., burnout was classified as no burnout (all 3 dimension scores below the threshold), mild burnout (any 1 dimension score above the threshold), moderate burnout (any 2 dimension scores above the threshold), or high burnout (all 3 dimension scores above the threshold), using an EE score > 25 points, a DP score > 11 points, and an RPA score > 16 points as the thresholds [37]. The MBI-GS had a Cronbach’s α of 0.863 for burnout in this study.
Data collection
Owing to the rapid spread of the virus since the relaxation of restrictions, an online questionnaire was created and distributed to HCWs via WeChat, one of the most widely used social media platforms in China. The survey was conducted from February 1 to March 1, 2023. Each phone IP address could be used only once to open and complete the survey to avoid duplication.
Data analysis
The data were analyzed using IBM SPSS software version 24.0. Quantitative data are presented as the mean ± standard deviation (SD), and qualitative data are presented as frequencies and percentages. Demographic and personal viral infection characteristics associated with fatigue, mental workload, and burnout were examined using t tests and one-way analysis of variance (ANOVA). Pearson’s correlation analysis was used to investigate the relationships among burnout, fatigue, and mental workload. The independent variables with statistical significance (P < 0.05) in the univariate analysis and Pearson correlation analysis were included in the multiple linear regression analysis, with fatigue, mental workload, and burnout as the dependent variables. In multiple regression analysis, independence was tested with the Derbin-Watson (D-W) residual test, homogeneity of variance was tested by a scatter plot, and normality was checked with a histogram combined with a normal P-P plot. A p value < 0.05 was considered to indicate a significant difference.
Ethical consideration
Ethics approval for this study was obtained from the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (Approval number: K2023-061). Participants read and signed an informed consent form before they started filling out the questionnaire.
Results
Descriptive characteristics
A total of 267 completed questionnaires were collected in this study. The majority of participants were female (92.13%), were married (59.18%), were nurses (87.26%), had an undergraduate degree or above (86.14%), came from Grade A hospitals (90.64%), worked in surgical units (47.19%), and had worked for less than 5 years (40.82%). Most participants experienced moderate or higher levels of work intensity (94.38%), work pressure (93.63%), and work-family conflict (75.66%). Regarding personal COVID-19 infection characteristics, most participants had a COVID-19 positivity period of 1–10 days (83.00%) and a recovery period of 11 days or more (84.69%). Moreover, most participants had one or more symptoms (69.66%). More detailed information about the individual, occupational, and COVID-19 infection characteristics of the participants is shown in Tables 1 and 2.
Univariate analysis results
Fatigue
Our results indicated that the prevalence of fatigue was 76.40%, and the mean (SD) fatigue score was 43.79 ± 13.26, as shown in Table 3. Tables 1 and 2 show that profession, intensity of work, work pressure, work-family conflict, current symptoms, number of days of COVID-19 positivity, and number of days until recovery from COVID-19 were correlated with fatigue (P < 0.05). As hypothesized, the incidence of fatigue was high and affected by COVID-19 infection.
Mental workload
Seven participants (2.62%) had a low mental workload, 19 participants (7.12%) had a light mental workload, 63 participants (23.60%) had a moderate mental workload, 133 participants (49.81%) had a high mental workload, and 45 participants (16.85%) had an intolerable mental workload. The mean (SD) mental workload score was 65.52 ± 17.46, as shown in Table 3. The highest to lowest scores were obtained for the dimensions of effort, temporal demand, physical demand, mental demand, perceived performance and frustration, respectively. Profession, hospital department, intensity of work, work pressure, work-family conflict, current symptoms, and number of days until recovery from COVID-19 were significantly associated with mental workload (P < 0.05), as shown in Tables 1 and 2. As assumed, mental workload was significantly prevalent and impacted by contracting COVID-19.
Burnout
Of the 267 participants, 29 (10.86%) had no burnout, 238 (89.14%) had burnout, 154 (57.68%) had mild burnout, 76 (28.46%) had moderate burnout, and 8 (3.00%) had severe burnout. As hypothesized, the incidence of burnout was high. Moreover, the percentages of participants with EE, DP, and RPA scores above the cut-offs were 17.98%, 85.00%, and 20.22%, respectively, as shown in Table 3.
We analyzed the features of burnout, which are summarized in Tables 1 and 2. We found that age, marital status, education level, profession, hospital department, work year, intensity of work, work pressure, and work-family conflict were significantly associated with burnout (P < 0.05). Contrary to the hypothesis, burnout was not affected by COVID-19 infection. Furthermore, age, marital status, education level, profession, hospital department, intensity of work, work pressure, and work-family conflict were significantly correlated with EE (P < 0.05). Age, marital status, profession, hospital department, work year, intensity of work, work pressure, work-family conflict and the number of days until recovery from COVID-19 were associated with the DP score (P < 0.05). Additionally, marital status, work year, and work-family conflict were related to RPA (P < 0.05).
Relationships among fatigue, mental workload and burnout
As shown in Table 4, the correlation analysis revealed that fatigue and mental workload were associated with burnout (overall: r = 0.514, P < 0.01; overall: r = 0.264, P < 0.01).
Multiple linear regression analysis results
The model including fatigue had an R2 of 0.471 and an adjusted R2 of 0.440. Variables that were significantly associated with greater fatigue included experiencing more frequent work-family conflict (t = 2.044, P = 0.042), having a greater number of current symptoms (t = 1.991, P = 0.048), having a greater number of days of COVID-19 positivity (t = 2.412, P = 0.017), having a greater mental workload (t = 2.340, P = 0.020), and experiencing increased burnout (t = 2.886, P = 0.004). Decreased fatigue was significantly associated with RPA (t=-2.435, P = 0.016).
The mental workload model had an R2 of 0.333 and an adjusted R2 of 0.293. These variables were significantly associated with more fatigue (t = 2.070, P = 0.040). Decreased mental workload was significantly associated with RPA (t=-2.118, P = 0.036).
The model of burnout had an R2 of 0.389 and an adjusted R2 of 0.352. Variables that were significantly associated with marital status were unmarried status (t = 3.160, P = 0.002) and increased fatigue (t = 6.128, P = 0.000).
Discussion
This study surveyed 267 HCWs after the strict zero-COVID-19 policies were relaxed and found that they experienced high levels of fatigue, mental workload, and burnout. Our analysis showed that many factors affected the fatigue, mental workload, and burnout of HCWs, and that these variables are correlated.
Our 76.40% fatigue incidence rate was higher than that in a previous study, which reported an incidence ranging from 26.6 to 41.2% at the start of the COVID-19 pandemic [38, 39]. Our mean (SD) fatigue score was 43.79 ± 13.26. The reason for the high prevalence of fatigue is that the HCWs were both patients and health caregivers. Our study corroborated the previously discussed associations among work-family conflict, mental workload, burnout and fatigue,as shown in Table 5. Notably, we found that greater numbers of current symptoms and days of COVID-19 positivity were significantly associated with fatigue [40,41,42]. Patients with acute COVID-19 can develop neurological and psychiatric symptoms during and after the acute phase of illness [43,44,45]. These chronic symptoms made the HCWs more prone to fatigue. Therefore, it is necessary to pay attention to changes in HCWs’ physical condition caused by COVID-19 through methods such as electrocardiography and CT. In addition, in a previous study, one-third of HCWs experienced residual symptoms even after returning to work, with persistent fatigue being a common symptom [46, 47]. This prompted HCWs to rationalize their work in accordance with their physical status, especially the presence of current symptoms and number of days of COVID-19 positivity. Moreover, fatigue is not only a state but also a process that can gradually lead to worsening fatigue symptoms [9]. This could increase the risk of poor clinical decision-making and compromise patient safety [26]. Therefore, early identification of fatigue and timely intervention are necessary Table 5.
We also found that RPA was related to a reduction in fatigue and mental workload. RPA is characterized by feelings of incompetence and a lack of achievement and productivity at work [23]. Kakemam reported that RPA was associated with the risk of medical errors and verbal abuse by patients and their families [48]. Alleviation of RPA reduced the occurrence of adverse events and reduced work and psychological stress among HCWs, which may be one of the reasons why RPA was related to fatigue and mental workload in our study. Therefore, skills training, further education, and professional development to improve professional achievement at work are essential.
In our study, the incidence of a moderate to intolerable mental workload was 90.26%, higher than the pooled incidence of 54% reported in the study of Yuan et al. [49]. This was due to the suspension of medical activities to treat patients infected with COVID-19, exposing medical and surgical staff to a new complex work environment, causing them to face new challenges. A total of 23.9% of the respondents in the study by González-Gil et al. noted greater clinical autonomy in decision-making during the COVID-19 pandemic than before the pandemic [50]. This placed greater demands on HCWs and increased the burden of their mental workload. Costin et al. reported flexible working, time management, and team support increased efficiency, productivity, and creativity [51]. Telehealth utilization was used to provide healthcare services during the pandemic [52]. Flexible working arrangements and clinical support, including remote technologies, are effective ways to alleviate HCWs’ mental workload.
In our study, the mean mental workload score was 65.52 ± 17.46. Additionally, effort and frustration had the highest and lowest scores, respectively, which was consistent with the study of Sarsangi et al. [53]. Nikeghbal et al. reported that nurses who were assessed for mental workload by the NASA-TLX had the highest perceived performance scores and the lowest frustration scores [54]. In Liu et al.’s study, nurses considered physical demand to be the most important part of their mental workload, while mental demand was considered the least important [40]. Overall, we found that the scores for mental demand and frustration were the lowest, indicating that the HCWs responded in a positive manner to the pandemic.
A total of 89.14% of the participants in our study reported experiencing burnout, 31.46% of whom had moderate to high burnout. Previous studies have shown that the incidence of burnout among HCWs was up to 84.44% [55] and that the incidence of moderate to high burnout was 50.13% [56]. Burnout during the full relaxation of COVID-19 restrictions was much more prevalent but less severe among HCWs than before their relaxation. The incidence of burnout increased due to the increase in the number of infections caused by the full relaxation of the pandemic restrictions, but the reduction in severity was due to the improvement in the associated complementary supplies.
Burnout was associated with more adverse changes in physical and psychological health, quality of care and cost of care among HCWs. Therefore, early identification of the risk factors for burnout is essential. Increased fatigue can lead to burnout, as previous studies have confirmed [42]. Some studies have shown that an unmarried status is a protective factor against burnout [57]. However, married people had a lower risk of burnout in our study. Research from Çevik H and Ungan M suggested that this is due to improved social support [58]. In addition, Hu et al. noted that unmarried people had higher RPA scores [59], meaning that they may have higher expectations of their job and less experience, increasing their vulnerability to burnout.
The percentages of patients with EE, DP, and RPA scores above the cut-offs were 17.98%, 85.00%, and 20.22%, respectively. In the study by Galanis et al., the overall prevalence of EE was 34.1%, that of DP was 12.6%, and that of RPA was 15.2% [60]. Parola et al. reported that the prevalence of EE, DP, and RPA was 19.5%, 8.2%, and 9.3%, respectively [61]. In our research, the incidence of DP was much greater than that in previous studies. A high DP means an increased emotional gap between patients and HCWs, which is not conducive to establishing good professional relationships. However, the use of some isolation policies made high DP scores unavoidable. Studies have shown that some contact restrictions cause HCWs to become more isolated and emotionally distressed [62].
Previous studies have shown an association between fatigue and mental workload [39] and between burnout and mental workload [63]. In this study, we quantified the relationships among fatigue, mental workload, and burnout, which indicated that these factors could affect each other. This finding might alert managers to pay attention to all of these factors. That is, when assessing burnout among HCWs, fatigue and mental workload should also be accounted for.
This study has several limitations. First, this study investigated only the fatigue, mental workload and burnout of HCWs after the relaxation of strict zero-COVID-19 policies and failed to perform comparisons with the pre-epidemic and early epidemic phases to dynamically assess their changes. Second, although we explored the influences of fatigue, mental workload and burnout, we might have failed to identify all contributing factors. Third, we collected data mainly from HCWs in the surgery department. A broader sample may reveal differences among different departments and regions or beyond.
Conclusion
Our study revealed a high prevalence of fatigue, mental workload, and burnout after the relaxation of the strict zero-COVID-19 policies. Fatigue, mental workload and burnout in HCWs were influenced by different factors, and these three factors were interrelated. This implies that when facing large-scale public emergencies, while the importance of comprehensive medical support cannot be overlooked, ultimately, attention needs to be given to the inner feelings of HCWs.
Data availability
The datasets generated and/or analysed during the current study are not publicly avaliable due the ethic of this study, but are available from the corresponding author upon reasonable request.
References
Li J, Zheng W, Liu L, Li S. The effect of medical staff’s professional identity on psychological stress during public health emergencies: The role of intolerance of uncertainty and adversity appraisal. Acta Psychol (Amst). 2022;227:103605. https://doi.org/10.1016/j.actpsy.2022.103605. Epub 2022 May 4. PMID: 35523081.
Lin TK, Werner K, Witter S, Alluhidan M, Alghaith T, Hamza MM, Herbst CH, Alazemi N. Individual performance-based incentives for health care workers in Organisation for Economic Co-operation and Development member countries: a systematic literature review. Health Policy. 2022;126(6):512–521. doi: 10.1016/j.healthpol.2022.03.016. Epub 2022 Apr 3. PMID: 35422364.
Wang XM, Chen BZ, Li XF, et al. Investigation and intervention of mental health status of nursing staff in isolation Ward during COVID-19 epidemic. Chin Remedies Clin. 2020;20(24):4083–4. https://doi.org/10.11655/zgywylc2020.24.008.
Guillén- Astete C, Penedo- Alonso R, Gallego- Rodríguez P. Levels of anxiety and depression among emergency physicians in Madrid during the SARS- Co V- 2 pandemic. Niveles De ansiedad Y depresión en médicos de urgencias de Madrid durante La pandemia POR El virus SARS- Co V- 2. Emergencias. 2020;32:369–71.
O’Callaghan EL, Lam L, Cant R, Moss C. Compassion satisfaction and compassion fatigue in Australian emergency nurses: a descriptive cross-sectional study. Int Emerg Nurs. 2020;48:100785. https://doi.org/10.1016/j.ienj.2019.06.008. Epub 2019 Jul 19. PMID: 31331839.
Stehman CR, Testo Z, Gershaw RS, Kellogg AR, Burnout, Drop Out, Suicide: Physician Loss in Emergency Medicine, Part I., West. J Emerg Med. 2019;20(3):485–494. https://doi.org/10.5811/westjem.2019.4.40970. Epub 2019 Apr 23. Erratum in: West J Emerg Med. 2019;20(5):840–841. PMID: 31123550; PMCID: PMC6526882.
Labrague LJ, Ballad CA. Lockdown fatigue among college students during the COVID-19 pandemic: predictive role of personal resilience, coping behaviors, and health. Perspect Psychiatr Care. 2021;57(4):1905–12. https://doi.org/10.1111/ppc.12765.
Majumdar P, Biswas A, Sahu S. COVID-19 pandemic and lockdown: cause of sleep disruption, depression, somatic pain, and increased screen exposure of office workers and students of India. Chronobiol Int. 2020;37(8):1191–200. https://doi.org/10.1080/07420528.2020.1786107.
Zhan YX, Zhao SY, Yuan J, Liu H, Liu YF, Gui LL, Zheng H, Zhou YM, Qiu LH, Chen JH, Yu JH, Li SY. Prevalence and influencing factors on fatigue of first-line nurses combating with COVID-19 in China: a descriptive cross-sectional study. Curr Med Sci. 2020;40(4):625–35. https://doi.org/10.1007/s11596-020-2226-9. Epub 2020 Aug 29. PMID: 32767264; PMCID: PMC7412774.
Zou X, Liu S, Li J, Chen W, Ye J, Yang Y, Zhou F, Ling L. Factors Associated with Healthcare workers’ insomnia symptoms and fatigue in the fight against COVID-19, and the role of Organizational Support. Front Psychiatry. 2021;12:652717. https://doi.org/10.3389/fpsyt.2021.652717. PMID: 33841214; PMCID: PMC8032945.
Montani D, Savale L, Noel N, et al. Post-acute COVID-19 syndrome. Eur Respir Rev. 2022;31(163):210185. https://doi.org/10.1183/16000617.0185-2021.
Giménez-Espert MDC, Prado-Gascó V, Soto-Rubio A, Psychosocial, Risks. Work Engagement, and job satisfaction of nurses during COVID-19 pandemic. Front Public Health. 2020;8:566896. https://doi.org/10.3389/fpubh.2020.566896.
Labrague LJ, de Los Santos JAA. Fear of COVID-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J Nurs Manag. 2021;29(3):395–403. https://doi.org/10.1111/jonm.13168.
Nickell LA. Psychosocial effects of SARS on hospital staff: survey of a large tertiary care institution. Can Med Assoc J. 2004;170(5):793–8. https://doi.org/10.1503/cmaj.1031077.
Tham KY, Tan YH, Loh OH, Tan WL, Ong MK, Tang HK. Psychiatric morbidity among emergency department doctors and nurses after the SARS outbreak. Ann Acad Med Singap. 2004;33(5 Suppl):S78–79.
Schoenenberger S, Moulin P, Brangier E et al. Patients’ characteristics and healthcare providers’ perceived workload in French hospital emergency wards. Int J Occup Saf Ergon. 2014;20(4):551-9. https://doi.org/10.1080/10803548.2014.11077071. PMID: 25513791.
Amin SG, Fredericks TK, Butt SE et al. Measuring mental workload in a hospital unit using EEG - A pilot study. IIE Annual Conference and Expo 2014.Institute of Industrial Engineers, 2014.
Restuputri DP, Pangesti AK, Garside AK. The measure-ment of physical workload and mental workload level of medical per-sonnel. Jurnal Teknik Industri. 2019;20(1):34–44.
Sarboozi Hosein Abadi T, Askari M, Miri K, Namazi Nia M. Depression, stress and anxiety of nurses in COVID-19 pandemic in Torbat Heydariyeh Hospital, Iran. J Mil Med. 2020;22(6). https://doi.org/10.30491/JMM.22.6.526.
Zamanian Z, Nikravesh A, Monazzam MR, Hassanzadeh J, Fararouei M. Short-term exposure with vibration and its effect on attention. J Environ Health Sci Eng. 2014;12(1):135. https://doi.org/10.1186/s40201-014-0135-1.
Spence Laschinger HK, Leiter M, Day A, Gilin D. Workplace empowerment, incivility, and burnout: impact on staff nurse recruitment and retention outcomes. Journal of Nursing Management. 2009;17(3):302–311. https://doi.org/10.1111/j.1365-2834. 2009.00999.x.
Zhu H, Xie S, Liu X, Yang X, Zhou J. Influencing factors of burnout and its dimensions among mental health workers during the COVID-19 pandemic. Nurs Open. 2022;9(4):2013–23. https://doi.org/10.1002/nop2.1211.
Maslach C, Jackson SE. The measurement of experienced burnout. J Organ Behav. 1981;2:99–113.
Teo I, Chay J, Cheung YB et al. Wang J, ed. 2021 Healthcare worker stress, anxiety and burnout during the COVID-19 pandemic in Singapore: a 6-month multi-centre prospective study. PLoS ONE 16 10 e0258866 https://doi.org/10.1371/journal.pone.0258866.
Zhang Y, Wang C, Pan W et al. Stress, Burnout, and Coping Strategies of Frontline Nurses During the COVID-19 Epidemic in Wuhan and Shanghai, China. Front Psychiatry. 2020;11:565520. Published 2020 Oct 26. https://doi.org/10.3389/fpsyt.2020.565520.
Al Ma’mari Q, Sharour LA, Al Omari O. Fatigue, burnout, work environment, workload and perceived patient safety culture among critical care nurses. Br J Nurs. 2020;29(1):28–34. https://doi.org/10.12968/bjon.2020.29.1.28.
Ma C, Park SH. Hospital Magnet Status, Unit Work Environment, and pressure ulcers: work environment and pressure ulcers. J Nurs Scholarsh. 2015;47(6):565–73. https://doi.org/10.1111/jnu.12173.
Salvagioni DAJ, Melanda FN, Mesas AE, González AD, Gabani FL, Andrade SMD. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. Van Wouwe JP, ed. PLoS ONE. 2017;12(10):e0185781. https://doi.org/10.1371/journal.pone.0185781.
Wang MY, Liu IC, Chiu CH, Tsai PS. Cultural adaptation and validation of the Chinese version of the fatigue severity scale in patients with major depressive disorder and nondepressive people. Qual Life Res. 2016;25(1):89–99. https://doi.org/10.1007/s11136-015-1056-x.
Krupp LB. The fatigue severity scale: application to patients with multiple sclerosis and systemic Lupus Erythematosus. Arch Neurol. 1989;46(10):1121. https://doi.org/10.1001/archneur.1989.00520460115022.
Wilson N, Wynter K, Fisher J, Bei B. Postpartum fatigue: assessing and improving the psychometric properties of the fatigue severity scale. Arch Womens Ment Health. 2018;21(4):471–4. https://doi.org/10.1007/s00737-018-0818-1.
Hart S, Staveland L. Development of NASA-TLX (Task load index): results of empirical and theoretical research. Hum Mental Workload. 1988;52:139–83.
Nasirizad Moghadam K, Chehrzad MM, Reza Masouleh S, et al. Nursing physical workload and mental workload in intensive care units: are they related? Nurs Open. 2021;8(4):1625–33. https://doi.org/10.1002/nop2.785.
Hoonakker P, Carayon P, Gurses AP, et al. Measuring workload of ICU nurses with a questionnaire survey: the NASA Task load index (TLX). IIE Trans Healthc Syst Eng. 2011;1(2):131–43. https://doi.org/10.1080/19488300. 2011.609524.
Teng M, Yuan Z, He H, Wang J. Levels and influencing factors of mental workload among intensive care unit nurses: A systematic review and meta-analysis. Int J Nurs Pract. 2023 May 31:e13167. https://doi.org/10.1111/ijn.13167. Epub ahead of print. PMID: 37259643.
Li CP, Shi K. The influence of distributive justice and procedural justice on job burnout. Acta Physiol Sinica. 2003;35(5):677–84.
Li Y, Li Y. Developing the diagnostic ctiterion of job burnout. Psychol Sci. 2006;29(1):148–50.
Chew NWS, Lee GKH, Tan BYQ, et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun. 2020;88:559–65. https://doi.org/10.1016/j.bbi.2020.04.049.
Salazar de Pablo G, Vaquerizo-Serrano J, Catalan A, et al. Impact of coronavirus syndromes on physical and mental health of health care workers: systematic review and meta-analysis. J Affect Disord. 2020;275:48–57. https://doi.org/10.1016/j.jad.2020.06.022.
Liu Y, Xian JS, Wang R, et al. Factoring and correlation in sleep, fatigue and mental workload of clinical first-line nurses in the post-pandemic era of COVID-19: a multi-center cross-sectional study. Front Psychiatry. 2022;13:963419. https://doi.org/10.3389/fpsyt.2022.963419.
Ismail KM, Malak MZ, Alamer RM. Psychosocial correlates of work-related fatigue among Jordanian emergency department nurses. Perspect Psychiatr Care. 2019;55(3):486–93. https://doi.org/10.1111/ppc.12354. Epub 2019 Feb 6. PMID: 30729538.
Van Dam A, Keijsers G, Verbraak M, Eling P, Becker E. Level and appraisal of fatigue are not specific in burnout. Clin Psychol Psychother. 2015 Mar-Apr;22(2):133 – 41. https://doi.org/10.1002/cpp.1869. Epub 2013 Sep 11. PMID: 24022877.
Klein R, Soung A, Sissoko C, et al. COVID-19 induces neuroinflammation and loss of hippocampal neurogenesis. Preprint Res Sq. 2021. https://doi.org/10.21203/rs.3.rs-1031824/v1. rs.3.rs-1031824.
Divani AA, Andalib S, Biller J, et al. Central Nervous System manifestations Associated with COVID-19. Curr Neurol Neurosci Rep. 2020;20(12):60. https://doi.org/10.1007/s11910-020-01079-7.
Méndez R, Balanzá-Martínez V, Luperdi SC, et al. Short-term neuropsychiatric outcomes and quality of life in COVID-19 survivors. J Intern Med. 2021;290(3):621–31. https://doi.org/10.1111/joim.13262.
Tempany M, Leonard A, Prior AR, et al. The potential impact of post-COVID symptoms in the healthcare sector. Occup Med (Lond). 2021;71(6–7):284–9. https://doi.org/10.1093/occmed/kqab109.
Grazzini M, Lulli LG, Mucci N, et al. Return to Work of Healthcare Workers after SARS-CoV-2 infection: determinants of physical and Mental Health. Int J Environ Res Public Health. 2022;19(11):6811. https://doi.org/10.3390/ijerph19116811. Published 2022 Jun 2.
Kakemam E, Chegini Z, Rouhi A, Ahmadi F, Majidi S. Burnout and its relationship to self-reported quality of patient care and adverse events during COVID-19: a cross-sectional online survey among nurses. J Nurs Manag. 2021;29(7):1974–82. https://doi.org/10.1111/jonm.13359. Epub 2021 May 24. PMID: 33966312; PMCID: PMC8237033.
Yuan Z, Wang J, Feng F, Jin M, Xie W, He H, Teng M. The levels and related factors of mental workload among nurses: a systematic review and meta-analysis. Int J Nurs Pract. 2023;29(5):e13148. https://doi.org/10.1111/ijn.13148. Epub 2023 Mar 23. PMID: 36950781.
González-Gil MT, González-Blázquez C, Parro-Moreno AI, et al. Nurses’ perceptions and demands regarding COVID-19 care delivery in critical care units and hospital emergency services. Intensive Crit Care Nurs. 2021;62:102966. https://doi.org/10.1016/j.iccn.2020.102966.
Costin A, Roman AF, Balica RS. Remote work burnout, professional job stress, and employee emotional exhaustion during the COVID-19 pandemic. Front Psychol. 2023;14:1193854. https://doi.org/10.3389/fpsyg.2023.1193854. PMID: 37325768; PMCID: PMC10267312.
Garfan S, Alamoodi AH, Zaidan BB, Al-Zobbi M, Hamid RA, Alwan JK, Ahmaro IYY, Khalid ET, Jumaah FM, Albahri OS, Zaidan AA, Albahri AS, Al-Qaysi ZT, Ahmed MA, Shuwandy ML, Salih MM, Zughoul O, Mohammed KI, Momani F. Telehealth utilization during the Covid-19 pandemic: a systematic review. Comput Biol Med. 2021;138:104878. Epub 2021 Sep 20. PMID: 34592585; PMCID: PMC8450049.
Sarsangi V, Saberi H, Hannani M, et al. Mental workload and its affected factors among nurses in Kashan province during 2014. J Rafsanjan Univ Med Sci. 2015;14(1):25–36.
Nikeghbal K, Kouhnavard B, Shabani A, Zamanian Z. Covid-19 effects on the Mental workload and quality of Work Life in Iranian nurses. Ann Glob Health. 2021;87(1):79. https://doi.org/10.5334/aogh.3386.
Kapasa RL, Hannoun A, Rachidi S, et al. E´ valuation Du burn-outchez les professionnels de sante´ des unite´ s de veille sanitaire COVID-19 Au Maroc. Arch Mal Prof Envi-ron. 2021;82(5):524–34.
Zemni I, Dhouib W, Sakly S, et al. Burnout syndrome among health care workers during the COVID-19 pandemic. A cross sectional study in Monastir, Tunisia. PLoS ONE. 2023;18(3):e0282318. https://doi.org/10.1371/journal.pone.0282318.
Hosseini M, Soltanian M, Torabizadeh C, Shirazi ZH. Prevalence of burnout and related factors in nursing faculty members: a systematic review. J Educ Eval Health Prof. 2022;19:16. https://doi.org/10.3352/jeehp.2022.19.16. Epub 2022 Jul 14. PMID: 35843600; PMCID: PMC9534603.
Çevik H, Ungan M. The impacts of the COVID-19 pandemic on the mental health and residency training of family medicine residents: findings from a nationwide cross-sectional survey in Turkey. BMC Fam Pract. 2021;22(1):226. https://doi.org/10.1186/s12875-021-01576-9. PMID: 34781878; PMCID: PMC8591155.
Hu HX, Liu LT, Zhao FJ, Yao YY, Gao YX, Wang GR. Factors Related to Job Burnout Among Community Nurses in Changchun, China. J Nurs Res. 2015;23(3):172 – 80. https://doi.org/10.1097/jnr.0000000000000072. PMID: 25700278.
Galanis P, Vraka I, Fragkou D, Bilali A, Kaitelidou D. Nurses’ burnout and associated risk factors during the COVID-19 pandemic: a systematic review and meta-analysis. J Adv Nurs. 2021;77(8):3286–302. https://doi.org/10.1111/jan.14839. Epub 2021 Mar 25. PMID: 33764561; PMCID: PMC8250618.
Parola V, Coelho A, Cardoso D, Sandgren A, Apóstolo J. Prevalence of burnout in health professionals working in palliative care: a systematic review. JBI Database System Rev Implement Rep. 2017;15(7):1905–1933. https://doi.org/10.11124/JBISRIR-2016-003309. PMID: 28708752.
Rana W, Mukhtar S, Mukhtar S. Mental health of medical workers in Pakistan during the pandemic COVID-19 outbreak. Asian J Psychiatr. 2020;51:102080. https://doi.org/10.1016/j.ajp.2020.102080. Epub 2020 Apr 7. PMID: 32283512; PMCID: PMC7139243.
Abareshi F, Salimi F, Farnia F, Fallahi M, Rastaghi S. The impact of Mental workload, work-related and Socio-demographic factors on Job Burnout among Emergency Medical Staff. WOR. 2022;72(4):1269–77. https://doi.org/10.3233/WOR-210001.
Acknowledgements
Thanks to everyone who worked to combat the COVID-19 and to everyone who has contributed to this study.
Funding
Not Applicable.
Author information
Authors and Affiliations
Contributions
Q.X made contributions to acquisition of data, interpretation of data, analysis, and draft the manuscript. Feng Luo and Yue Chen made contributions to study design. Y.D, J.H, H.L, P.J, R.L made contributions to acquisition of data.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of the first Affiliated Hospital of Chongqing Medical University (Approval number: K2023-061). The study was conducted in accordance with the principles of the Declaration of Helsinki. Participants read and signed informed consent form as they started filling out the questionnaire.
Consent for publication
Not Applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xiong, Q., Luo, F., Chen, Y. et al. Factors influencing fatigue, mental workload and burnout among Chinese health care workers during public emergencies: an online cross-sectional study. BMC Nurs 23, 428 (2024). https://doi.org/10.1186/s12912-024-02070-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-024-02070-0