
Abstract
Background
Although knowledge of the barriers and motivators to physical activity participation among nurses is increasing, the factors influencing motivation methods’ effectiveness are not completely defined. This study aimed to identify the methods that support increasing the level of daily physical activity and the factors that influence the effectiveness of motivation methods among nurses.
Methods
This study was based on an intervention study protocol. All registered nurses in clinical settings were invited to participate in the study. The study involved 71 professionally active nurses. A self-reported questionnaire was used to collect sociodemographic and employment data. The level of physical activity was assessed using the International Physical Activity Questionnaire, and the daily number of steps was assessed using a pedometer. Body composition was measured using a bioimpedance method, and the 5-year risk of cardiovascular events was assessed using the Harvard Score. The intervention included self-monitoring daily steps using a pedometer and completing a diary daily for one month. Additionally, a few-minute speech was sent to each participant via email on the intervention’s 7th, 14th, and 21st days.
Results
The analysis revealed a higher value of physical activity recorded in the follow-up compared to the initial and final measurement in the Recreation domain [Met] (p < 0.001) and a higher value of daily steps in the follow-up compared to the final measurement (p = 0.005). Participants with a higher Harvard Score were more likely to increase their daily number of steps (OR = 6.025; 95% CI = 1.70-21.41), and nurses working in hospital wards were less likely to do so (OR = 0.002; 95% CI = 0.00-0.41).
Conclusions
Recommendations for physical activity in the nursing population should focus on increasing leisure time physical activity and regular risk assessment of cardiovascular events. A mixed methods approach, such as feedback enhanced by health coaching, effectively achieves long-term physical activity changes in nurses.
Similar content being viewed by others


Background
The benefits of regular physical activity are well-documented and include improved cardiovascular function and musculoskeletal strength, reduced morbidity and mortality risk due to chronic disease, and decreased risk of mental health problems [1, 2]. Additionally, performing physical activity can reduce work-related stress and incidence of burnout [3,4,5] and positively affect emotional intelligence and resilience [6, 7]. Moreover, the health-related behaviors of medical professionals are associated with their quality of life [8].These benefits are increasingly emphasized in research on healthcare worker populations [9]. Despite being aware of the benefits, many nurses have low levels of physical activity [10,11,12,13], placing them at an increased risk for chronic diseases [14] andleading to increased absences and decreased work capacity, potentially increasing the workload for other nurses on the unit [15, 16]. Furthermore over 30% of registered nurses are overweight or obese [9, 17, 18], which may result from stressful work conditions. Such a relationship has previously been found among nurses [19]. Moreover, rotating night shift work is related with unhealthy lifestyles and both are involved in increasing the risk of type 2 diabetes. Rotating night shift work alters sleep and circadian rhythms that play important roles in daily normal metabolic function. Disruption of sleep and circadian rhythms are involved in lifestyle behaviors such as smoking, diet, physical activity, they also could disrupt the intestinal microbiota, which has the role in development of metabolic diseases. Some researchers suggest that most cases of type 2 diabetes could be prevented by adherence to a healthy lifestyle, and the benefits would be larger in rotating night shift workers [20]. Although nurses have the highest rates of obesity and overweight, they have the lowest participation in workplace health promotion activities among all healthcare professional groups working in hospitals [21]. As such, nurses should be a target group for health promotion initiatives [22].
Several methods have been identified to promote physical activity andthe workplace is an ideal setting to implement health promotion initiatives to reduce noncommunicable disease risk factors, according to the World Health Organization [23]. On the other hand, theresults of interventions regarding physical activity promotion in nurses, especially workplace initiatives, are inconsistent [14]. The quality of studies assessing the impact of such interventions is mostly low to moderate, and results should be interpreted cautiously [14]. Moreover assessing the physical activity using one method– only subjective or objective one may have discrepancy. Self-reported measures tend to overestimate physical activity levels when compared with objective assessments [22, 24]. Effective methods in increasing nurses’ physical activity include self-monitoring using the accelerometer or physical activity challenges, but the rate of change decreases over time [5, 25]. Visual triggers and health coaching with texting have also increased physical activity levels [26]. Based on replicable behavior change techniques, self-monitoring behavior and subsequent feedback are typically an effective combination of methods to improve nurses’ physical activity [27]. One recommendation to increase the level of physical activity is to remove barriers that discourage or prevent nurses from engaging in physical activity. These barriers include lack of time, excessive work, irregular shifts, stress, exhaustion, and fear of pain after exercise, which results from the physically demanding nature of the nursing profession [28,29,30]. The nursing profession has long been considered physically demanding [31] and is associated with a very high prevalence of musculoskeletal disorders [32]. Previous studies have confirmed that one of the biggest barrier to motivating nurses to increase their physical activity is the fear of pain that may occur after exercise [22]. In the nursing population, high fear-avoidance beliefs regarding physical activity have been significantly associated with experiencing chronic, disabling low back pain [33].
Many authors report the necessity to investigate personal and occupational factors that could help nurses sustain physical activity levels in the long term [22, 25]. This study aims to identify the methods that support increasing the level of daily physical activity and the sociodemographic, occupational, and health-related factors that influence the effectiveness of motivation methods in increasing daily physical activity among nurses.
Methods
Design and settings
This study was based on an intervention study protocol, and data were collected over 10 months, from September 2021 to June 2022. The inclusion process was continuous and intentionally included different seasons to account for the variability of the daily number of steps depending on the season, which is confirmed in the literature [34]. All registered nurses in clinical settings were invited to participate in the study. Detailed information about the study was disseminated in hospitals and outpatient clinics in Warsaw, and a full list of participating institutions is included in Appendix 1. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement was used to report data [35], along with the Page et al. statement about improving the reporting of therapeutic exercise interventions in rehabilitation research [36].
Sample
The inclusion criteria for this study were being a professionally active nurse working in a clinical setting, being able to walk unassisted, being willing to wear a monitoring device on the wrist, and having access to the Internet and an email address. Criteria for exclusion from participation in the study were dysfunction or disability affecting gait locomotion, pregnancy, medical contraindications to exercise, or implanted pacemakers or other devices contraindicated for body composition assessment using the bioimpedance method. Sample size analysis was performed using G*Power 3.1.9.4 software. Based on analysis of variance (ANOVA) results for a moderate effect size (f = 0.25), alpha = 0.05, and test power at 0.95, the sample size required was 43 participants for repeated measures.
Data sources and measurements
The study was divided into three phases: inclusion, intervention with final assessment, and follow-up measurements. During the inclusion process, all participants consented to participate in the study. A self-reported questionnaire was used to collect sociodemographic data such as sex, age, and place of residence, as well as professional activity-related data such as education, clinical specialization, management position, number and type of workplace(s), total monthly workload, type of shift, and work experience.
Body composition, including Body Mass Index (BMI) [kg/m2], the absolute value of Fat Mass (Fat) in kg, and the absolute value of Free Fat Mass (FFM) in kg, was measured using a bioimpedance method (Body Composition Analyzer Maltron Bioscan 920, UK). The measurement was taken during rest in the supine position after measuring the participant’s body weight in kg. Blood pressure was measured once in the supine position using an upper arm automatic blood pressure monitor (Omron M4). On average, each examination lasted up to 10 min for each person.
The 5-year risk of cardiovascular events was assessed using the Harvard Score (Score), a non-laboratory method shown to predict cardiovascular events as accurately as the Framingham Coronary Heart Disease Risk Score, which requires laboratory-based values. The Harvard Score utilized non-laboratory-based risk factors such as age, sex, diabetes status (no diabetes or diabetes), current smoking status (non-smoker or smoker), systolic blood pressure, and Body Mass Index to determine 5-year cardiovascular disease risk categories: <5% (low), 5–10% (low), > 10–20% (moderate), > 20–30% (high), or > 30% (high). Cardiovascular risk scores were not calculated for participants younger than 35 [37].
The level of daily physical activity was assessed using a Polish version of the long form of the International Physical Activity Questionnaire (IPAQ). The questionnaire was structured to provide separate domain-specific scores for walking (total walking MET), moderate-intensity activity (total moderate MET), and vigorous-intensity activity (total vigorous MET) within each of the work (Occupational activity [MET]), active transportation (Active locomotion [MET]), domestic chores (Domestic chores [MET]), and leisure-time domains (Recreation [MET]). Total time engaged in walking, moderate physical activity, and vigorous physical activity, as well as the total level of weekly activity (total physical activity score - TPAS), were computed according to the guidelines [38].
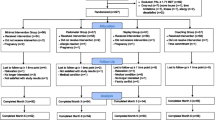
The average daily number of steps was measured using a pedometer Health Manager App Beurer AS 80 (model 2016/2017) for 7 consecutive days before the intervention phase. The nurses were instructed to wear the activity monitor from waking to bedtime (except during water activities) and to complete a diary of their daily number of steps. The pedometers had a memory function and researchers cross-checked the data stored in the pedometer’s memory with the participant’s diaries. A flow chart depicting the measures taken in each study phase is presented in Fig. 1.

A flow chart depicting the measures taken in each study phase
Intervention
All participants wore the pedometer for one month and had to complete a diary of their daily number of steps. In addition, on the intervention’s 7th, 14th, and 21st days, motivation for physical activity participation was enhanced through a few-minute speech recorded and sent to each participant’s email. The researchers have checked if each participant has read the email. The speeches covered topics such as guidelines for daily physical activity, the impact of physical activity on health, the health effects of physical inactivity, and tips on gradually increasing daily physical activity. During the speeches, participants were encouraged to achieve the goal of 10,000 steps per day, but goal achievement was not the purpose of the study. At the end of the intervention phase, final measurements were conducted, including the level of daily physical activity measure, the average daily number of steps, body composition, and Harvard Score.
Follow-up
The follow-up assessments were conducted after 3 months of final measurements and included the level of daily physical activity measure and the average daily number of steps.
Statistical methods
All data were analyzed using IBM SPSS Statistics, version 28.0. Descriptive statistics were used to assess sample characteristics. The Shapiro-Wilk test was used to assess the consistency of the quantitative variable with a normal distribution. For the comparison of two related samples and quantitative variables, the t-test was performed, and for more than two measurements, the Friedman test or the analysis of variance for repeated measures was used (e.g., comparison of the level of daily physical activity measure and Steps values between each study phase). To determine which of the analyzed variables were predictors of the decrease/increase in the average daily number of steps (Steps), a logistic regression analysis was performed using the backward elimination method with maximum likelihood estimation. The model explained a total of 21.9% of the variance of the dependent variable (Cox and Snell R2 = 0.219) and was well fitted to the data, χ2 [8] = 3.90; p = 0.866 (Hosmer-Lemeshow test). Spearman’s rho correlation analysis determined the relationships between quantitative variables. The significance level was set at α = 0.05.
Results
Participant characteristic
A total of 106 professionally active Polish nurses were included in the study, and 71 completed all stages. One participant was excluded during the intervention due to a leg fracture, 11 were excluded due to upper respiratory tract infections, and 23 withdrew without reason. The detailed characteristics of the study participants are summarized in Table 1. Participants were predominantly middle-aged (mean 35.65 ± 10.40 [years]), female (85.9%), residing in a city (91.5%), and had a master’s degree (59.2%) without clinical specialization (69%). Most of the participants were employed in hospital settings (90.1%), working overtime (62%) on mixed shifts (81.7%). The average work experience of participants was 12.3 ± 9.28 [years].
Physical activity before and after intervention
There were no significant differences in the Total Physical Activity Score (TPAS [MET]) assessed by IPAQ between study points, but a detailed analysis revealed significant differences in the Recreation domain [MET]. The follow-up recorded a higher value than the initial and final measurements. However, the differences between the initial and final measurements were not significant. The analysis showed significant differences between the measurements for ‘Domestic chores’ but post hoc analysis using the Dunn test with Bonferroni correction of the significance level did not show significant differences between the groups.
The average daily number of steps (Steps) was significantly higher in the follow-up compared to the final measurement, but there were no differences between the initial and final measurements. The comparisons of the results of IPAQ and Steps between each study phase are presented in Table 2 and in Figs. 2 and 3.

The results of Recreation domain [MET] in all phases of the study

The results of the average daily number of steps [Steps] in all phases of the study
The trend analysis of the Step number revealed that the average daily number of steps was similar during each of the 30 days of the intervention. A slight decrease from the average was observed on the 6th, 14th, 17th, and 20th day of the study, while a higher activity level was observed on the 25th day of the study. Figure 4 depicts the trend of the daily number of steps. In this figure, the whiskers represent the standard deviation, the solid line indicates the average number of steps for each measurement day, and the dashed line represents the average daily number of steps over the entire analyzed period.

The trend of the daily number of steps during the intervention phase
Body composition and cardiovascular disease risk before and after intervention
The study revealed a significant decrease in Body Mass Index and the absolute value of Fat Mass at [kg] in the final measurement compared to the initial measurement (t = 2.09; p = 0.04 and t = 2.22; p = 0.03, respectively). The comparisons of the results of blood pressure, body composition, and Harvard Score between each study phase are summarized in Table 3.
Factors influencing the increase in the average daily number of steps after the intervention were examined in the present study. The results showed that 43.7% of participants had increased the Steps number at the final measure and 63.4% at the follow-up. Logistic regression analysis revealed that the odds for an increase in the Steps number decreased with higher systolic blood pressure (SBP) [mmHg] (OR = 0.92; 95% CI = 0.85-1.00) and with working in a hospital ward (OR = 0.002; 95% CI = 0.00-0.41). On the other hand, the odds for an increase in the Steps number increased with a higher Harvard Score (OR = 6.025; 95% CI = 1.70-21.41) and Free Fat Mass (FFM) [kg] (OR = 1.451; 95% CI = 1.07–1.96) measures. None of the other sociodemographic orvocational variables, were significant predictors of an increase or decrease in the participants’ number of steps. The model explained a total of 21.9% of the variance in the explained variable (Cox and Snell R2 = 0.219) and was a good fitted to the data, χ2 [8] = 3.90; p = 0.866 (Hosmer-Lemeshow test). The detailed results of analysis are presented in Table 4.
Discussion
A mixed method approach, using a pedometer and 3 motivational speeches did not influence the Total Physical Activity Score (TPAS [MET]) assessed by IPAQ, but a detailed analysis revealed a significant increase in the Recreation domain [MET], where a significantly higher value was recorded in the follow-up compared to the initial and final measurements. Furthermore, the average daily number of steps was significantly higher in the follow-up compared to the final measurement, suggesting that the intervention had a long-lasting effect that persisted after the completion of the intervention phase. This finding is inconsistent with previous studies that reported short-lived increases in physical activity after web-based interventions providing feedback and physical activity challenges [39]. The results suggest that other motivation methods, such as health coaching, should enhance interventions with feedback and physical activity challenges [26]. The good match of health coaching applied in the present study, which occurred just after the decrease in the daily number of steps, supports this hypothesis. Drawing on evidence-based behavior change techniques, such as coaching, social support, feedback, barrier identification, follow-up prompts, and health checks may help reinforce long-term physical activity changes [40].
Our findings suggest that the Recreation domain of daily physical activity is the most susceptible to change. This aligns with our previous research, which demonstrated that nurses who are more motivated to be active engagement in a higher level of leisure-time physical activity than those who are less motivated [22]. Research has also shown that engaging in moderate- to vigorous-intensity physical activity before a morning shift is associated with increased sedentary time and decreased physical activity during work hours [41]. Henwood et al. found that nurses who engaged in ≥ 30 min/day of moderate workplace activity were not healthier than those who found the same amount of physical activity during their leisure time. They concluded that workplace activity does not positively affect health and well-being [42]. Parker et al. suggested that occupational physical activity may not provide the same health benefits as leisure-time physical activity for nurses [43]. Furthermore, Richard et al. reported that leisure-time physical activity is inversely associated with all-cause mortality, whereas occupational physical activity does not have clear associations [44]. These observations support the effectiveness of intervention programs that promote physical activity, particularly in the leisure-time domain, which is most recommended for health benefits. Providing sufficient time for recovery after work and ensuring compliance with ergonomic principles are crucial to enable nurses to engage in leisure-time physical activity. Our study also revealed a significant change in participants’ Body Mass Index, which may indicate that the motivational strategies employed during the intervention phase influenced other healthy behaviors besides physical activity. In our study strength of the effect is low, but other authors have also confirmed the effectiveness of health coaching in promoting behavior changes for improved health, including body weight loss, increased physical activity, mental health status, enhanced medication adherence, better social support, and improved physical health status, including HbA1c. Health coaching is also a low-cost tool [45].
The presented study identified several factors predisposing individuals to increase their daily number of steps. Participants with higher Harvard Scores were likelier to increase their Steps number, which contradicts the belief that fear arousal induced by threat (future punishment) is likely counterproductive when self-efficacy is low [27]. This suggests that nurses with higher knowledge about the consequences of chronic diseases may be more motivated to change their health behaviors because of the fear of threat (future punishment), such as the 5-year risk of cardiovascular events. Conversely, participants with higher Free Fat Mass [kg] are more vulnerable to applied motivation, suggesting that naturally active individuals in good physical condition are more willing to engage in physical activity. Nurses who agree that physical activity positively affects their mental and physical condition were more motivated to engage in physical activity and showed a higher level of leisure-time physical activity [22]. However, working in a hospital ward harmed the increase in the number of steps after the applied intervention. Although the type of hospital ward was not distinguished in the study, other research has shown that the average number of steps and distance traveled was greatest for nurses working in the emergency room, followed by the intensive care unit, surgical ward, and medical ward [46]. Working in a hospital ward and engaging in direct patient care is considered the most demanding [41, 47], and nurses not involved in direct patient care are more sedentary [47]. Nurses working in rotating shifts showed a significantly higher level of general physical activity than nurses working only in daily shifts [22, 48]. Furthermore, nurses who are highly active during work hours are less likely to engage in leisure-time physical activity, as confirmed by Chappel et al., who revealed that occupational walking time was associated with lower activity levels during leisure time [41]. Although working in a hospital ward is difficult to modify, ensuring appropriate time for recovery and compliance with ergonomic principles is necessary to enable nurses to increase their leisure-time physical activity.
Limitations
One limitation of the presented study is the possibility that participants may have adopted a healthier lifestyle during the observation period than they normally would have, knowing that their physical activity was being recorded. Therefore, an observer effect cannot be ruled out, a common limitation in similar studies [49]. For the same reasons, a control group was not included in the study. Another limitation is self-selection, meaning nurses not interested in increasing their physical activity may have chosen not to participate in the study. Moreover, the adherence to listening to a few-minute speeches was not assessed by a reliable method and it was based solely on participant’s self-reporting. Researchers only confirmed whether each participant had read the email.
Strengths
One strength of the study was the utilization of both objective and subjective methods to assess daily physical activity. The study utilized the IPAQ questionnaire, allowing for a comprehensive analysis of physical activity. This analysis included not only fundamental calculations derived from the assessment but also additional domains such as recreation, household duties, and duties related to professional work. The sample size was well-matched to the intervention. Moreover, the recommended bio-psycho-social model was used in the logistic regression analysis, taking into account metric, professional, social and health-related factors influencing the increase/decrease of daly physical activity.
Conclusions
To reinforce long-term changes in nurses’ physical activity, employing mixed methods, such as using a pedometer and delivering motivational speeches, seems a promising way to proceed. Feedback and physical activity challenges should be supplemented by other motivational techniques, such as health coaching, effectively promoting behavior changes for improved health. It should be highly recommended because leisure-time physical activity is the most susceptible to change according to motivational techniques. Participants with higher Harvard Scores were more likely to increase their daily number of steps; therefore, regular evaluation of this indicator among nurses is warranted. Working in a hospital ward had the most negative impact on increasing the daily number of steps, and this factor is difficult to modify. Therefore, ensuring appropriate time for recovery and compliance with ergonomic principles is necessary to enable nurses to increase their leisure-time physical activity.
Data availability
The datasets used and/or analysed during the current study are available from.
the corresponding author on reasonable request.
References
Warburton DER, Bredin SSD. Health benefits of physical activity: a systematic review of current systematic reviews. Curr Opin Cardiol. 2017;32(5):541–56. https://doi.org/10.1097/hco.0000000000000437
Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, Stubbs B. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. 2019;107:525–39. https://doi.org/10.1016/j.neubiorev.2019.09.040
Merces MC, Coelho JM, Lua I, Silva DD, Gomes AM, Erdmann AL, et al. Prevalence and Factors Associated with Burnout Syndrome among Primary Health Care nursing professionals: a cross-sectional study. Int J Environ Res Public Health. 2020;17(2). https://doi.org/10.3390/ijerph17020474
Naczenski LM, de Vries JD, van Hooff MLM, Kompier MAJ. Systematic review of the association between physical activity and burnout. J Occup Health. 2017;59(6):477–94. https://doi.org/10.1539/joh.17-0050-RA
Murphy CA, Staffileno BA, Hand M, Bruen CP, Hermsen M, Johnson L, et al. Feasibility and impact of physical activity on Compassion fatigue and Burnout among Ambulatory Care Oncology nurses. Clin J Oncol Nurs. 2022;26(5):519–27. https://doi.org/10.1188/22.Cjon.519-527
Wu R, Jing L, Liu Y, Wang H, Yang J. Effects of physical activity on regulatory emotional self-efficacy, resilience, and emotional intelligence of nurses during the COVID-19 pandemic. Front Psychol. 2022;13:1059786. https://doi.org/10.3389/fpsyg.2022.1059786
Yu F, Cavadino A, Mackay L, Ward K, King A, Smith M. Physical activity and personal factors associated with nurse resilience in intensive care units. J Clin Nurs. 2020;29(17–18):3246–62. https://doi.org/10.1111/jocn.15338
Niestrój-Jaworska M, Dębska-Janus M, Polechoński J, Tomik R. Health behaviors and Health-Related Quality of Life in Female Medical Staff. Int J Environ Res Public Health. 2022;19(7):3896. https://doi.org/10.3390/ijerph19073896
Ortega-Campos E, Cañadas-De la Fuente GA, Albendín-García L, Gómez-Urquiza JL, Monsalve-Reyes C, de la Fuente-Solana EI. A Multicentre study of psychological variables and the prevalence of burnout among primary Health Care nurses. Int J Environ Res Public Health. 2019;16(18). https://doi.org/10.3390/ijerph16183242
Ross A, Bevans M, Brooks AT, Gibbons S, Wallen GR. Nurses and health-promoting behaviors: knowledge may not translate into self-care. Aorn j. 2017;105(3):267–75. https://doi.org/10.1016/j.aorn.2016.12.018
Blake H, Malik S, Mo PK, Pisano C. Do as say, but not as I do’: are next generation nurses role models for health? Perspect Public Health. 2011;131(5):231–9. https://doi.org/10.1177/1757913911402547
Reed JL, Prince SA, Pipe AL, Attallah S, Adamo KB, Tulloch HE, et al. Influence of the workplace on physical activity and cardiometabolic health: results of the multi-centre cross-sectional Champlain nurses’ study. Int J Nurs Stud. 2018;81:49–60. https://doi.org/10.1016/j.ijnurstu.2018.02.001
Priano SM, Hong OS, Chen JL. Lifestyles and Health-related outcomes of U.S. Hospital nurses: a systematic review. Nurs Outlook. 2018;66(1):66–76. https://doi.org/10.1016/j.outlook.2017.08.013
Torquati L, Pavey T, Kolbe-Alexander T, Leveritt M. Promoting Diet and physical activity in nurses. Am J Health Promot. 2017;31(1):19–27. https://doi.org/10.4278/ajhp.141107-LIT-562
Letvak S. We cannot ignore nurses’ health anymore: a synthesis of the literature on evidence-based strategies to improve nurse health. Nurs Adm Q. 2013;37(4):295–308. https://doi.org/10.1097/NAQ.0b013e3182a2f99a
While AE. Promoting healthy behaviours - do we need to practice what we preach? Lond J Prim Care (Abingdon). 2015;7(6):112–4. https://doi.org/10.1080/17571472.2015.1113716
Chin DL, Nam S, Lee SJ. Occupational factors associated with obesity and leisure-time physical activity among nurses: a cross sectional study. Int J Nurs Stud. 2016;57:60–9. https://doi.org/10.1016/j.ijnurstu.2016.01.009
Fang L, Hsiao LP, Fang SH, Chen BC. The associations with work stress, social support and overweight/obesity among hospital nurses: a cross-sectional study. Contemp Nurse. 2018;54(2):182–94. https://doi.org/10.1080/10376178.2018.1476166
Caruso CC. Negative impacts of shiftwork and long work hours. Rehabil Nurs. 2014;39(1):16–25. https://doi.org/10.1002/rnj.107
Shan Z, Li Y, Zong G, Guo Y, Li J, Manson JE, et al. Rotating night shift work and adherence to unhealthy lifestyle in predicting risk of type 2 diabetes: results from two large US cohorts of female nurses. BMJ. 2018;363:k4641. https://doi.org/10.1136/bmj.k4641
Chiou ST, Chiang JH, Huang N, Chien LY. Health behaviors and participation in health promotion activities among hospital staff: which occupational group performs better? BMC Health Serv Res. 2014;14:474. https://doi.org/10.1186/1472-6963-14-474
Wesołowska-Górniak K, Nerek A, Serafin L, Czarkowska-Pączek B. The relationship between Sociodemographic, Professional, and incentive factors and self-reported level of physical activity in the Nurse Population: a cross-sectional study. Int J Environ Res Public Health. 2022;19(12). https://doi.org/10.3390/ijerph19127221
Quintiliani L, Sattelmair J, Sorensen G. The workplace as a setting for interventions to improve diet and promote physical activity. World Health Organ. 2007:1–36.
Niestrój-Jaworska M, Polechoński J, Nawrocka A. Subjective and Objective Assessment of recommended physical activity in female Healthcare professionals. Appl Sci. 2023;13(15):8569. https://doi.org/10.3390/app13158569
Brunet J, Tulloch HE, Wolfe Phillips E, Reid RD, Pipe AL, Reed JL. Motivation predicts Change in nurses’ physical activity levels during a web-based worksite intervention: results from a Randomized Trial. J Med Internet Res. 2020;22(9):e11543. https://doi.org/10.2196/11543
Melnyk BM, Kelly SA, Stephens J, Dhakal K, McGovern C, Tucker S, et al. Interventions to Improve Mental Health, Well-Being, Physical Health, and Lifestyle Behaviors in Physicians and nurses: a systematic review. Am J Health Promot. 2020;34(8):929–41. https://doi.org/10.1177/0890117120920451
Power BT, Kiezebrink K, Allan JL, Campbell MK. Development of a behaviour change workplace-based intervention to improve nurses’ eating and physical activity. Pilot Feasibility Stud. 2021;7(1):53. https://doi.org/10.1186/s40814-021-00789-0
George LS, Lais H, Chacko M, Retnakumar C, Krishnapillai V. Motivators and barriers for physical activity among Health-Care professionals: a qualitative study. Indian J Community Med. 2021;46(1):66–9. https://doi.org/10.4103/ijcm.IJCM_200_20
Saridi M, Filippopoulou T, Tzitzikos G, Sarafis P, Souliotis K, Karakatsani D. Correlating physical activity and quality of life of healthcare workers. BMC Res Notes. 2019;12(1):208. https://doi.org/10.1186/s13104-019-4240-1
Philbrick G, Sheridan NF, McCauley K. An exploration of New Zealand mental health nurses’ personal physical activities. Int J Ment Health Nurs. 2022. https://doi.org/10.1111/inm.12981
Van der Heijden B, Brown Mahoney C, Xu Y. Impact of Job Demands and Resources on Nurses’ Burnout and Occupational Turnover Intention Towards an Age-Moderated Mediation Model for the Nursing Profession. Int J Environ Res Public Health. 2019;16(11). https://doi.org/10.3390/ijerph16112011
Sun W, Yin L, Zhang T, Zhang H, Zhang R, Cai W. Prevalence of work-related Musculoskeletal disorders among nurses: a Meta-analysis. Iran J Public Health. 2023;52(3):463–75. https://doi.org/10.18502/ijph.v52i3.12130
Fujii T, Oka H, Takano K, Asada F, Nomura T, Kawamata K, et al. Association between high fear-avoidance beliefs about physical activity and chronic disabling low back pain in nurses in Japan. BMC Musculoskelet Disord. 2019;20(1):572. https://doi.org/10.1186/s12891-019-2965-6
Wesolowska K, Czarkowska-Paczek B. Activity of daily living on non-working and working days in Polish urban society. Int J Occup Med Environ Health. 2018;31(1):47–54. https://doi.org/10.13075/ijomeh.1896.01076
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of Observational studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–9. https://doi.org/10.1016/j.ijsu.2014.07.013
Page P, Hoogenboom B, Voight M, IMPROVING THE REPORTING OF THERAPEUTIC, EXERCISE INTERVENTIONS IN REHABILITATION RESEARCH. Int J Sports Phys Ther. 2017;12(2):297–304.
Gaziano TA, Young CR, Fitzmaurice G, Atwood S, Gaziano JM. Laboratory-based versus non-laboratory-based method for assessment of cardiovascular disease risk: the NHANES I follow-up study cohort. Lancet. 2008;371(9616):923–31. https://doi.org/10.1016/s0140-6736(08)60418-3
Guidelines for Data Processing and Analysis of the International. Physical Activity Questionnaire (IPAQ)– Short and Long Forms 2005.
Reed JL, Cole CA, Ziss MC, Tulloch HE, Brunet J, Sherrard H, et al. The impact of web-based feedback on physical activity and Cardiovascular Health of Nurses Working in a Cardiovascular setting: a Randomized Trial. Front Physiol. 2018;9:142. https://doi.org/10.3389/fphys.2018.00142
Michie S, Ashford S, Sniehotta FF, Dombrowski SU, Bishop A, French DP. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychol Health. 2011;26(11):1479–98. https://doi.org/10.1080/08870446.2010.540664
Chappel SE, Aisbett B, Considine J, Ridgers ND. Bidirectional associations between emergency nurses’ occupational and leisure physical activity: an observational study. J Sports Sci. 2021;39(6):705–13. https://doi.org/10.1080/02640414.2020.1841921
Henwood T, Tuckett A, Turner C. What makes a healthier nurse, workplace or leisure physical activity? Informed by the Australian and New Zealand e-Cohort study. J Clin Nurs. 2012;21(11–12):1746–54. https://doi.org/10.1111/j.1365-2702.2011.03994.x
Parker HM, Gallagher R, Duffield C, Ding D, Sibbritt D, Perry L. Occupational and leisure-time physical activity have different relationships with Health: a cross-sectional Survey Study of Working nurses. J Phys Act Health. 2021;18(12):1495–502. https://doi.org/10.1123/jpah.2020-0415
Richard A, Martin B, Wanner M, Eichholzer M, Rohrmann S. Effects of leisure-time and occupational physical activity on total mortality risk in NHANES III according to sex, ethnicity, central obesity, and age. J Phys Act Health. 2015;12(2):184–92. https://doi.org/10.1123/jpah.2013-0198
Malecki HL, Gollie JM, Scholten J. Physical activity, Exercise, Whole Health, and Integrative Health Coaching. Phys Med Rehabil Clin N Am. 2020;31(4):649–63. https://doi.org/10.1016/j.pmr.2020.06.001
Chang HE, Cho SH. Nurses’ steps, distance traveled, and perceived physical demands in a three-shift schedule. Hum Resour Health. 2022;20(1):72. https://doi.org/10.1186/s12960-022-00768-3
Ross A, Yang L, Wehrlen L, Perez A, Farmer N, Bevans M. Nurses and health-promoting self-care: do we practice what we preach? J Nurs Manag. 2019;27(3):599–608. https://doi.org/10.1111/jonm.12718
Peplonska B, Bukowska A, Sobala W. Rotating night shift work and physical activity of nurses and midwives in the cross-sectional study in Łódź. Pol Chronobiol Int. 2014;31(10):1152–9. https://doi.org/10.3109/07420528.2014.957296
Roskoden FC, Krüger J, Vogt LJ, Gärtner S, Hannich HJ, Steveling A, et al. Physical activity, Energy Expenditure, Nutritional habits, quality of sleep and stress levels in Shift-Working Health Care Personnel. PLoS ONE. 2017;12(1):e0169983. https://doi.org/10.1371/journal.pone.0169983
Acknowledgements
We are grateful to the nurses who participated in this study.
Funding
This research was as part of the project (grant number: MB/Z/10) implemented from 2020 to 2022 and financed by a subsidy allocated to science from the Medical University of Warsaw.
Author information
Authors and Affiliations
Contributions
Conceptualization, A.N. K.W.-G. and B.C.-P.; Data curation, A.N.; Funding acquisition, K.W.-G.; Investigation, A.N.; Methodology, K.W.-G., A.N. and B.C.-P.; Project administration, K.W.-G. and B.C.-P.; Supervision, B.C.-P.; Writing—original draft, K.W.-G. and A.N. Writing—review and editing, B.C.-P. and K.W.-G. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the Declaration of Helsinki, and was approved by Ethics Committee of Medical University of Warsaw (reference number: AK-BE/163/2020). Informed consent was obtained from all participants of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nerek, A., Wesołowska-Górniak, K. & Czarkowska-Pączek, B. Enhancing feedback by health coaching: the effectiveness of mixed methods approach to long-term physical activity changes in nurses. An intervention study. BMC Nurs 23, 196 (2024). https://doi.org/10.1186/s12912-024-01815-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-024-01815-1