
Abstract
Background
This study aimed to assess the knowledge and current practice of using the airway pressure release ventilation (APRV) mode with acute respiratory distress syndrome (ARDS) patients and identify barriers to not using this mode of ventilation among nurses who work in critical areas in Saudi Arabia.
Methods
Between December 2022 and April 2023, a cross-sectional online survey was disseminated to nurses working in critical care areas in Saudi Arabia. The characteristics of the respondents were analyzed using descriptive statistics. Percentages and frequencies were used to report categorical variables.
Results
Overall, 1,002 nurses responded to the online survey, of whom 592 (59.1%) were female. Only 248 (24.7%) nurses had ever used APRV mode, whereas only 229 (22.8%) received training on APRV mode. Moreover, 602 (60.0%) nurses did not know whether APRV was utilized in their hospital. Additionally, 658 (65.6%) nurses did not know whether APRV mode was managed using a standard protocol. Prone positioning was the highest recommended intervention by 444 (43.8%) when a conventional MV failed to improve oxygenation in patients with ARDS. 323 (32.2%) respondents stated that the P-high should be set equal to the plateau pressure on a conventional ventilator, while 400 (39.9%) said that the P-low should match PEEP from a conventional ventilator. Almost half of the respondents (446, 44.5%) stated that the T-high should be set between 4 and 6 s, while 415 (41.4%) said that the T-low should be set at 0.4 to 0.8 s. Over half of the nurses (540, 53.9%) thought that the maximum allowed tidal volume during the release phase should be 4–6 ml/kg. Moreover, 475 (47.4%) believed that the maximum allowed P-high setting should be 35 cm H2O. One-third of the responders (329, 32.8%) stated that when weaning patients with ARDS while in APRV mode, the P-high should be reduced gradually to reach a target of 10 cm H2O. However, 444 (44.3%) thought that the T-high should be gradually increased to reach a target of 10 s. Half of the responders (556, 55.5%) felt that the criteria to switch the patient to continuous positive airway pressure (CPAP) were for the patient to have an FiO2 ≤ 0.4, P-high ≤ 10 cm H2O, and T-high ≥ 10 s. Lack of training was the most common barrier to not using APRV by 615 (61.4%).
Conclusion
The majority of nurses who work in critical care units have not received sufficient training in APRV mode. A significant discrepancy was observed regarding the clinical application and management of APRV parameters. Inadequate training was the most frequently reported barrier to the use of APRV in patients with ARDS.
Similar content being viewed by others

Introduction
Airway pressure release ventilation (APRV) is a mechanical breathing mode that alternates between two degrees of continuous positive airway pressure (CPAP) support [1, 2]. It also allows for spontaneous respiratory effort at any CPAP intensity. It is seen as a potentially life-saving method for patients suffering from acute respiratory distress syndrome (ARDS) who are struggling to maintain oxygenation [3]. APRV is a safe and effective technique for breathing that is pressure-limited, time-triggered, and time-cycled [1, 2]. The APRV mode employs CPAP with an inverse ratio of inspiration to expiration time (I = E) and can facilitate unrestricted spontaneous breathing in all ventilator cycles to make patients comfortable [4]. APRV has been found to give lower peak pressure, better oxygenation, less circulatory loss, and better gas exchange than conventional ventilation, without worsening the ARDS patient’s hemodynamic status [5]. This method is thought to aid in the goal of recruiting consolidated lung regions and preventing recurrent opening and closing of the alveoli (decruitment) [3]. Research has demonstrated that, when compared to other ventilation modes in ARDS patients, the APRV mode increased gas exchange and arterial oxygenation (PaO2/FiO2) ratios [6, 7]. Previous literature has elucidated that the timely implementation of APRV in adult patients with ARDS is associated with improvements in oxygenation status, respiratory compliance, and a reduction in the duration of both mechanical ventilation and intensive care unit (ICU) stays [8, 9].
Despite its widespread utilization as an ARDS rescue therapy in many ICUs worldwide, the terminology and settings for the APRV mode may differ slightly, but the concepts remain similar to those of other traditional modes [2, 10]. APRV settings encompass four fundamental parameters: P-high, T-high, P-low, and T-low. The term P-high denotes the heightened continuous positive airway pressure (CPAP) level sustained for an extended duration (T-high), aiming to facilitate optimal lung volume and alveolar recruitment. Conversely, P-low signifies a brief application of low CPAP pressure during a short period (T-low), wherein the majority of ventilation processes occur [2, 11]. Established protocols for APRV recommend setting P-high equivalent to the plateau pressure (Pplat) observed during conventional mechanical ventilation (CMV), while maintaining P-low at 0 cm H2O to prevent alveolar erosion during the release phase. Furthermore, initiating T-high within the range of 4 to 6 s is advised to sustain optimal minute ventilation, with T-low adjusted to achieve the end of expiratory airflow at 75% of the peak expiratory flow rate (PEFR) [12, 13].
It is not widely known how the APRV mode is utilized in the management of ARDS patients by nurses who work in critical care units, and what barriers there are to using the APRV mode. As a result, we hypothesize that nurses lack proficient knowledge regarding the effective application of APRV to patients diagnosed with ARDS. Thus, the study aimed to assess APRV utilization by nurses who work at critical care units in the management of ARDS patients and identify the most common barriers to not using APRV mode.
Method
Study design and instrument
A cross-sectional design was used in this study. The survey was developed, formulated by experts who had experience using APRV mode (ICU physician, respiratory therapist and ICU nurse) and consisted of three parts, 24 questions. The first part was about demographic data, the second part involved knowledge and clinical practice of the APRV mode, the selection of this part from and the strategies were used in APRV mode were from previous literature [12,13,14,15]. The last part was about barriers of not using the APRV mode. The questionnaire was tested and evaluated by ten ICU nurses to ensure clarity and comprehensibility (Supplementary 3).
Data collection and sampling
Data collection was conducted and assembled through the SurveyMonkey platform from December 2022 to April 2023. Invitations to nurses were sent via professional organizations established on social media platforms, as well as the Saudi Nurses Association and the Saudi Nursing Society. Nurses employed in critical units in the Kingdom of Saudi Arabia (KSA) were the main target population of this study. Before starting the questionnaire, information about the study as well as chief investigator contact information were available. Additionally, a written informed consent was obtained from each participant, and voluntary participation was ensured. Participants can only answer the survey link once and the expected time to complete the survey was 10 min.
Data analysis
The data were analyzed using descriptive analysis. Frequency and percentages were used to summarize the results. Mean and standard deviation were used to calculate the number of ARDS patients cared for per shift. The Statistical Package for the Social Sciences (SPSS) version 29 was used to perform the statistical analysis.
Ethical approval
Ethical approval for this study was sought from the bioethical committee at Jazan University with reference number (44/04/364). The study has been conducted in accordance with the Declaration of Helsinki.
Results
Demographic data of the study participants
Overall, 1,002 nurses who worked in critical units completed the online survey. More than half of the participants were female (592, 59.1%). The majority of participants were from the central region of Saudi Arabia (410, 40.9%), followed by the western region (303, 30.2%). Most of the participants had a bachelor’s degree (746, 74.5%). The largest group of participants worked at the Ministry of Health hospitals (372, 37.1%), and had one to five years of clinical experience. The mean (SD) ARDS patients cared for per shift was between 2 and 3 (Table 1). Only one quarter (248, 24.7%) of the nurses had ever used APRV mode, whereas only 229 (22.8%) had received training on APRV mode. Moreover, well over half (602, 60.0%) of the nurses did not know whether APRV was utilized in their hospital. Additionally, two-thirds (658, 65.6%) of the nurses did not know whether APRV mode was managed using the standard protocol with ARDS patients. The full demographic data of the study participants are shown in Table 1.
Indications and initial settings of APRV mode with ARDS patients
The majority of participants 672 (67.1%) recommended using APRV mode with ARDS patients, followed by COVID-19 patients 468 (46.7%), patients with pneumonia 362 (36.1%), asthma patients 176 (17.6%), patients with pulmonary edema 174 (17.4%), patients with obesity-induced hypoventilation syndrome 148 (14.8) and the lowest percentage was with sleep apnea patients 57 (5,7%). Additionally, 444 (43.8%) of the participants chose prone positioning as the next strategy to improve oxygenation in ARDS patients when conventional M.V fails to improve oxygenation (please see Table 2).
When APRV mode was initiated, 323 (32.2%) of the nurses recommended that the initial P-high settings should be equal to the plateau pressure on a conventional ventilator, while 400 (39.9%) recommended the initial P-low settings should match PEEP from a conventional ventilator. Furthermore, 446 (44.5%) recommended that the initial T-high settings should be between 4 and 6 s, while 415 (41.4%) recommended the initial T-low settings should be a set time (between 0.4 and 0.8 s). Of the 1,002 participants, 588 (58.7%) used pressure support during spontaneous breathing (please see Table 2).
APRV mode management with ARDS patients
The maximum allowed tidal volume during the release phase recommended by 540 (53.9%) of the participants was between 4 and 6 ml/kg, whereas 475 (47.4%) recommended the maximum allowed P-high during the release phase to be 35 cm H2O (please see Table 2).
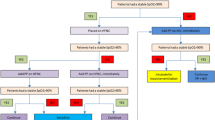
When using APRV in managing patients with ARDS, 553 (55.2%) of the nurses stated that increasing P-high (assuming P-high is less than 25 cm H2O), followed by 394 (39.3%) who stated that decreasing P-low, and 515 (51.4%) who stated that increasing T-low would be their first, second, and third prefatory choices to manage unacceptably low levels of pH with elevated partial pressure of arterial carbon dioxide (PaCO2) in patients with ARDS (please see Fig. 1 and Supplementary Table 1).

The order of interventions when levels of pH are unacceptably low and the PaCO2 is elevated in patients with ARDS (n = 1,002)
When using APRV in managing patients with ARDS, just over half of the nurses 515 (51.4%) chose increasing P-high (assuming P-high is less than 25 cm H2O), followed by 424 (42.3%) who preferred increasing T-high, and 513 (51.2%) who stated that decreasing T-low would be their first, second, and third prefatory choices to manage unacceptably low levels of oxygen in patients with ARDS (please see Fig. 2 and Supplementary Table 2).

The order of interventions when levels of oxygen are unacceptably low in patients with ARDS (n = 1,002)
APRV Weaning and discontinuation in ARDS patients
One-third 329 (32.8%) of participants believed that when weaning ARDS patients, while in APRV mode, the P-high should be reduced gradually in an attempt to reach a target of 10 cm H2O, followed by 309 (30.8%) participants who thought that the P-high should be reduced gradually in an attempt to reach a target of 15 cm H2O. Moreover, 444 (44.3%) felt that the T-high should be gradually increased in an attempt to reach a target of 10 s, followed by 252 (25.1%) who thought that the T-high should be gradually increased in an attempt to reach a target of 7 s. When oxygenation goals are achieved and the ARDS patient is clinically stable, over half of the participants 556 (55.5%) thought that the criteria to switch the patient to CPAP would be to have an FiO2 ≤ 0.4, P-high ≤ 10 cm H2O, and T-high ≥ 10 s (please see Table 2).
Common barriers to not using APRV mode with ARDS patients
The most common barriers to not using APRV mode with ARDS patients from the perspective of nurses were inadequate training 615 (61.4%) followed by high work overload 416 (41.5%) and absence of protocols 411 (41.0%) (Fig. 3).

The most common barriers to using APRV mode (n = 1,002)
Discussion
To the best of our knowledge, there is an extreme paucity of studies examining the clinical practice of APRV among nursing staff who work at critical units in Saudi Arabia. In light of this knowledge gap, this is the first national study to evaluate current awareness, practices, and barriers to the use of APRV mode in ARDS patients among nurses who work at critical units in the Kingdom of Saudi Arabia. Overall, our study’s results indicated that majority of nursing staff did not receive any training in utilizing APRV mode, and neither were they aware of APRV usage in their hospital nor the availability of APRV application guidelines in their facility. In addition, a significant discrepancy was found in nursing responses regarding indication, initial setting, weaning criteria, and discontinuation of APRV placement. However, nurses working in critical units revealed modest consistency in managing APRV settings to mitigate hypoxemia and hypercapnia.
Despite the enormous burden of the implementation of APRV in ARDS patients, APRV placement in the clinical setting remains controversial due to the lack of a standardized protocol [16, 17]. The clinical effectiveness of APRV mode has not been empirically proven in experimental studies due to the significant heterogeneity in APRV placement settings [18, 19]. Previous studies have indicated that RTs in Saudi Arabia were not well conversant in the application of APRV, where considerable disparities in setting and managing APRV parameters were observed as a result of a dearth of protocol and training seminars on the effective use of APRV [20, 21]. In line with this, our study outcomes found that nurses who work in critical units were not well-versed in APRV placement, as the vast majority (75%) had never used APRV mode, and a similar number (77%) had not received training in utilizing APRV mode. Furthermore, over half of the nurses (60%) were unaware of APRV usage in their hospital and two-thirds (66%) were not cognizant of the availability of APRV application guidelines at their facility. Thus, strict adherence to published guidelines, and receiving training in setting and adjusting the fundamental parameters of APRV, are indispensable prerequisites for obtaining the clinical benefit of the APRV application and avoiding life-threatening risks [12, 13].
Since the emergence of the APRV mode, it has contributed significantly as a rescue strategy for a wide spectrum of diseases, particularly ARDS [22]. Accordingly, the majority of the nurses in our study (67%) stated that ARDS was a primary indication for APRV application. Previous literature has attested to the clinical benefit of early APRV placement in adult patients with ARDS, as it substantially encourages spontaneous breathing, increases functional residual capacity (FRC), and thus optimizes ventilation/perfusion matching [2, 23]. A meta-analysis of randomized controlled trials (RCTs) has proven the significant advantages of APRV utilization, as it contributes to lower mortality, shortens the length of stay on a ventilator, and improves lung compliance and oxygenation status [24]. Notwithstanding, recent evidence has shown that the indication and effectiveness of APRV remain ambiguous due to a lack of robust evidence supporting the purported benefits of APRV [22, 25].
Understanding the complexity of APRV settings is vitally important for optimal clinical management [17]. Only one-third of the nurses (32%) reported that the P-high should match up with the plateau pressure (Pplat) on a conventional mechanical ventilator (CMV). These results are consistent with established APRV protocols that suggest setting P-high equal to the measured Pplat in volume control mode or similar to the set inspiratory pressure when switching from pressure control mode [12, 13]. A survey of 60 healthcare providers revealed that nearly half (48%) were strictly adherent to ARPV protocols for setting P-high [14]. Moreover, our study observed that approximately 40% of nurses indicated that P-low should be set to the same level as PEEP in a conventional ventilator. This result contradicts the APRV guidelines, which recommend initiating P-low at 0 cm H2O [12, 13]. These protocols were closely followed by healthcare professionals in the Miller et al. study, in which three-quarters (78%) set the initial P-value at 0 cm H2O [14]. It has previously been observed that setting P-low at 0 cm H2O generates an intrinsic PEEP that intentionally prevents alveolar erosion during the release phase because it will never permit expiratory flow to terminate below 25% of the peak expiratory flow rate (PEFR) [11, 26].
Furthermore, the results of our study indicated that almost half (45%) of the nurses thought that T-high should be started between 4 and 6 s, which matches the APRV protocols [12, 13]. Likewise, 65% of the participants in Miller et al.’s study showed identical findings in the T-high setting [14]. It is widely recommended that T-high not be set lower than 4 s to provide 8 to 12 releases per minute and consequently maintain optimal minute ventilation [2]. However, our study findings revealed that around 41% of nurses believed that the T-low should be set between 0.4 and 0.8 s. Similar disparities across healthcare practitioners were seen in Miller et al.’s study, with a significant number (39%) using an arbitrary T-low [14]. In contrast, several studies have shown the importance of adjusting the T-low to reach the end of expiratory airflow at 75% of the peak expiratory flow rate (PEFR) [27, 28]. In particular, appropriate adjustment of the T-low plays a pivotal role in stabilizing the alveoli by maintaining sufficient lung volume at the end of expiration to prevent periodic closure and reopening of the pulmonary units at low lung volumes [29, 30].
Regarding the management of the APRV settings, it was found that more than half of the nursing staff (54%) assumed that the maximum allowed tidal volume (Vt) ranged between 4 and 6 ml/kg. In contrast, healthcare providers in the study by Miller et al. presented erratic results, with most of them (38%) stating that Vt should be set between 6 and 8 ml/kg [14]. Previous research has pointed out that tidal volume in APRV mode is controlled indirectly by adjusting T-low to maintain Vt between 4 and 6 ml/kg, thus optimizing alveolar ventilation [2]. Meanwhile, the expiratory time (T-low) should be effectively adjusted to be brief enough to prevent lung recruitment and long enough to attain an adequate tidal volume [11]. However, it was observed that nearly half (47%) of nurses believed that P-high should be limited to 35 cm H2O. In accordance with this, healthcare practitioners revealed similar findings in Miller et al.’s study, where 45% of them indicated the same limit [14]. It is strongly suggested to maintain a P-high less than 35 cm H2O and below the upper inflection point to reduce trans-alveolar pressure and hence decrease the risk of lung injury [2, 4, 31].
The results of our survey showed that increasing the P-high was the most dominant technique for enhancing ventilation and oxygenation status. It is well established that prolonged P-high is the first-line intervention in the management of respiratory acidosis and severe hypoxemia. Extended P-high can significantly promote alveolar recruitment by increasing mean airway pressure and lengthening gas exchange, resulting in better oxygenation levels and carbon dioxide clearance [11, 12]. Additionally, lowering the T-high and raising the T-low can be beneficial in improving alveolar ventilation because they provide greater time for exhalation and removal of PaCO2 [13]. Likewise, it has been shown that brief release periods at P-low can significantly improve pulmonary ventilation and lessen life-threatening hypercapnia [11, 26].
In terms of weaning APRV parameters, our study outcomes revealed that one-third (33%) of nurses believed that weaning of APRV mode should begin with a steady reduction in P-high to achieve 10 cm H2O, and 44% stated that a gradual increase in T-high should be applied to reach 10 s. These findings are in line with prior APRV protocols that advocated the “drop and stretch” approach to weaning APRV settings, which intended to decrease the P-high by 1 to 2 cm H2O and increase the T-high by 0.5 s for every 1 cm H2O drop in P-high [12, 13]. Furthermore, over half of nursing staff pointed out that an ARDS patient must meet certain criteria before converting to CPAP mode, including FiO2 ≤ 0.4, a P-high ≤ 10 cm H2O, and a T-high ≥ 10 s. Accordingly, subsequent studies have revealed the same criteria for switching an ARDS patient to CPAP mode with a PEEP value similar to P-high [11,12,13].
Although utilizing the APRV mode in patients with APRV has been associated with positive therapeutic outcomes, there are a variety of obstacles that may impede APRV implementation in the clinical setting. Our study analysis found that the most frequently mentioned barriers to adopting APRV mode are an absence of protocols, a heavy workload, and inadequate training. In agreement with this, it has been conclusively shown that the absence of randomized controlled trials is the primary impediment to the use of APRV in patients with ARDS [17, 18, 32]. A lack of consensus among practitioners in the initiation and management of APRV settings has been noted, which can be attributed to the absence of solid proof supporting the application of APRV placement [22, 33]. In light of the aforementioned findings, it is highly recommended to establish a training program and implement an institutional policy to improve nursing staff’s knowledge of the effective way to use APRV.
Strengths and limitations
Our study is noteworthy because it is the first of its kind to evaluate Saudi Arabian nurses’ awareness, practice, and barriers related to using the APRV mode with ARDS patients. Additionally, it includes a sizable sample of nursing staff from different geographic areas, which facilitates the generalization of the results throughout the country. Nevertheless, certain limitations may hinder the scope of the research. This is a survey-based study that is unable to pinpoint the root cause of poor awareness of the APRV mode. In light of these limitations, further studies are warranted to examine the mechanism of action and to create evidence-based protocols for APRV mode in an attempt to raise the awareness of nursing staff regarding the optimal application of APRV.
Conclusion
Overall, the majority of nurses who work in critical care units in Saudi Arabia did not receive sufficient training in APRV mode. A significant discrepancy was observed regarding the clinical application and management of APRV parameters. Inadequate training, a high workload, and a lack of guidelines were the frequently reported barriers to the use of APRV in patients with ARDS. A well-established evidence-based protocols and training programs for APRV mode are warranted to improve the clinical awareness of nursing staff regarding the optimal utilization of APRV.
Availability of data and materials
The data used for the current study are available from the corresponding author on reasonable request.
References
Roth A. Mechanical Ventilation: Airway Pressure Release Ventilation (Respiratory Therapy). Elsevier Clinical Skills; 2020: p. 1-6. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/http://repository.phb.ac.id/658/1/Mechanical-Ventilation-Airway-Pressure-Release-Ventilation-Skill-Respiratory-Therapy-_070420.pdf.
Daoud EG, Farag HL, Chatburn RL. Airway pressure release ventilation: what do we know? Respir Care. 2012;57(2):282–92.
Küçük MP, et al. The effect of preemptive airway pressure release ventilation on patients with high risk for acute respiratory distress syndrome: a randomized controlled trial. Braz J Anesthesiol (English Edition). 2022;72(1):29–36.
Daoud EG. Airway pressure release ventilation. Ann Thorac Med. 2007;2(4):176.
Demirkol D, Karabocuoglu M, Citak A. Airway pressure release ventilation: an alternative ventilation mode for pediatric acute hypoxemic respiratory failure. Indian J Pediatr. 2010;77:1322–5.
Putensen C, et al. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med. 2001;164(1):43–9.
Sydow M, et al. Long-term effects of two different ventilatory modes on oxygenation in acute lung injury. Comparison of airway pressure release ventilation and volume-controlled inverse ratio ventilation. Am J Respir Crit Care Med. 1994;149(6):1550–6.
Zhou Y, et al. Early application of airway pressure release ventilation may reduce the duration of mechanical ventilation in acute respiratory distress syndrome. Intensive Care Med. 2017;43:1648–59.
Küçük MP, et al. The effect of preemptive airway pressure release ventilation on patients with high risk for acute respiratory distress syndrome: a randomized controlled trial. Braz J Anesthesiol. 2022;72:29–36.
González M, et al. Airway pressure release ventilation versus assist-control ventilation: a comparative propensity score and international cohort study. Intensive Care Med. 2010;36:817–27.
Swindin J, Sampson C, Howatson A. Airway pressure release ventilation. BJA Educ. 2020;20(3):80.
Habashi NM. Other approaches to open-lung ventilation: airway pressure release ventilation. Crit Care Med. 2005;33(3):S228–40.
Modrykamien A, Chatburn RL, Ashton RW. Airway pressure release ventilation: an alternative mode of mechanical ventilation in acute respiratory distress syndrome. Cleve Clin J Med. 2011;78(2):101–10.
Knowledge and practice of using airway pressure release ventilation mode in ARDS patients: A survey of physicians Heliyon. 2023;9(12):e22725. https://doi.org/10.1016/j.heliyon.2023.e22725.
Miller AG, et al. Clinical management strategies for airway pressure release ventilation: a survey of clinical practice. Respir Care. 2017;62(10):1264–8.
Piraino T, Fan E. Airway pressure release ventilation in patients with acute respiratory distress syndrome: not yet, we still need more data. J Thorac Dis. 2018;10(2):670.
Mireles-Cabodevila E, Dugar S, Chatburn RL. APRV for ARDS: the complexities of a mode and how it affects even the best trials. J Thorac Dis. 2018;10(Suppl 9):S1058.
Jain SV, et al. The 30-year evolution of airway pressure release ventilation (APRV). Intensive Care Med Exp. 2016;4(1):1–18.
Andrews P, et al. Myths and misconceptions of airway pressure release ventilation: getting past the noise and on to the signal. Front Physiol. 2022;1403. https://doi.org/10.3389/fphys.2022.928562.
Mohammad Abdulhameed Al O, Lynda G, Rachel C. Assessment of the Knowledge, Perception, and Prevalence of Using APRV Among Respiratory Therapists. Respiratory Care. 2021;66(Suppl 10):3600836.
Alamri F. Prevalence, and Attitudes among Respiratory Therapists in Saudi Arabia toward Using Airway Pressure Release Ventilation Mode with Pediatric Acute Respiratory Distress Syndrome Patients. 2023. https://doi.org/10.57709/34704392.
Mallory P, Cheifetz I. A comprehensive review of the use and understanding of airway pressure release ventilation. Expert Rev Respir Med. 2020;14(3):307–15.
Maung AA, Kaplan LJ. Airway pressure release ventilation in acute respiratory distress syndrome. Crit Care Clin. 2011;27(3):501–9.
Zhong X, et al. Airway pressure release ventilation versus low tidal volume ventilation for patients with acute respiratory distress syndrome/acute lung injury: a meta-analysis of randomized clinical trials. Ann Transl Med. 2020;8(24):1641. https://doi.org/10.21037/atm-20-6917.
Li R, et al. Effects of airway pressure release ventilation on lung physiology assessed by electrical impedance tomography in patients with early moderate-to-severe ARDS. Crit Care. 2023;27(1):178.
Fredericks AS, et al. Airway pressure release ventilation: A review of the evidence, theoretical benefits, and alternative titration strategies. Clin Med Insights. 2020;14:1179548420903297.
Kollisch-Singule M, et al. Airway pressure release ventilation reduces conducting airway micro-strain in lung injury. J Am Coll Surg. 2014;219(5):968–76.
Kollisch-Singule M, et al. Effect of airway pressure release ventilation on dynamic alveolar heterogeneity. JAMA Surg. 2016;151(1):64–72.
Michaela K-S, et al. The time-controlled adaptive ventilation protocol: mechanistic approach to reducing ventilator-induced lung injury. European Respiratory Review. 2019;28(152):180126. https://doi.org/10.1183/16000617.0126-2018.
Kollisch-Singule M, et al. Mechanical breath profile of airway pressure release ventilation: the effect on alveolar recruitment and microstrain in acute lung injury. JAMA Surg. 2014;149(11):1138–45.
Porhomayon J, El-Solh A, Nader ND. Applications of airway pressure release ventilation. Lung. 2010;188:87–96.
Rose L, Hawkins M. Airway pressure release ventilation and biphasic positive airway pressure: a systematic review of definitional criteria. Intens Care Med. 2008;34:1766–73.
Light A. Why All the shots at airway pressure release ventilation when conventional ventilation doesn’t have consensus? Respir Care. 2018;63(1):127–8.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
Conceptualization, AMA, AAA, & MMA; Data curation, MAM, HHM, AAB; Formal analysis, HHM & SMA; Investigation, MAS, AHA; Methodology, ASA, JSA; Project administration; AMA; Supervision, AH & OAA; Validation, JSA, ASA; Writing original draft, AMA, MAM, HHM, AAB, AHA; Writing – review & editing, All authors. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for this study was sought from the bioethical committee at Jazan University with reference number (44/04/364). The study has been conducted in accordance with the Declaration of Helsinki. A written informed consent was obtained from each participant, and voluntary participation was ensured.
Consent for publication
Not-applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 2: Supplementary Table 1.
The complete order for each intervention as reported by participants to manage unacceptably low levels of pH with elevated PaCO2 in patients with ARDS. Supplementary Table 2. The complete order for each intervention as reported by participants to manage unacceptably low levels of oxygen in patients with ARDS.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Aldhahir, A.M., Alqarni, A.A., Madkhali, M.A. et al. Awareness and practice of airway pressure release ventilation mode in acute respiratory distress syndrome patients among nurses in Saudi Arabia. BMC Nurs 23, 79 (2024). https://doi.org/10.1186/s12912-024-01763-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-024-01763-w