
Abstract
Background
Short peripheral catheters (SPC) insertion technique has a high failure rate, one of the reasons why the ultrasound (US)-guided method has been proposed as a valid alternative to traditional technique in SPC insertion. This umbrella review aims to synthesize the available evidence comparing the US-guided method with the traditional method on SPC insertion in terms of effectiveness, safety and patient satisfaction.
Methods
An umbrella review addressing the comparison between US-guided versus traditional method for SPC insertion in which only systematic reviews of all comparative study designs were eligible was carried out. Previous systematic reviews and meta-analyses were systematically searched in MEDLINE, EMBASE, Web of Science and Cochrane Library. Methodological quality was assessed with AMSTAR-2 tool. The quality of evidence per association was assessed using the GRADE criteria and was stablished as high, moderate, low and very low.
Results
Twelve systematic reviews with a range of 75–1860 patients were included. Moderate certainty evidence supports the positive effect of US-guided method on first-attempt success rate and number of attempts. There is moderate certainty evidence that US-guided method does not reduce the time spent in SPC insertion. Low certainty evidence supports that US-guided method improves both overall success rates and patient satisfaction. Emergency department was the main hospital department where these findings were reported.
Conclusions
The best current evidence indicates that US-guided method for SPC insertion is postulated as a valid alternative for both adult and pediatric population, especially in patients with difficult venous access and in hospital departments where optimal vascular access in the shortest time possible is critical.
Trial registration
PROSPERO: CRD42021290824.
Similar content being viewed by others


Background
Peripheral venous access devices (PVADs) are required in more than a billion hospitalized patients each year, which corresponds to 59–80% of hospitalized patients depending on the region, becoming the most used clinical invasive device [1, 2]. In the emergency department (ED), PVADs are placed in 70% patients [3]. However, PVADs insertion failure rate is between 43 to 59%, [4] a disappointing data considering the pain, care delays and infection probability to which patients are exposed [5]. Several patient-related circumstances such as chronic illness, edema, obesity or the use of injecting drugs could hinder the PVADs insertion [6]. Among the PVADs, according to international consensus standards, both the short peripheral catheters (SPC), the long peripheral catheters (LPC) and the midline catheters (MC) could be described [7, 8].
Regarding the SPC, the traditional method used for SPC insertion requires vein visualization and/or palpation from the provider [9]. Recently, the potential advantages of ultrasonography (US) guided over the traditional method in SPC insertion have been assessed [10]. In this sense, several reviews have been published to elucidate the outcomes which significantly improve when using the US-guided method in comparison with traditional method, especially in patients with difficult venous access (DVA) [11]. However, there are some methodological differences which could be responsible for the fact that, to date, not conclusive evidence is available supporting US-guided method over the traditional one [11, 12]. Likewise, there is a lack of information as to the differences between both methods in SPC-related complications [12, 13].
Umbrella reviews are a useful strategy to overcome these concerns because they assess the consistency of the evidence that the existing systematic reviews and meta-analyses provide. In our case, this methodology was used to synthesize and critically assess the evidence provided by previous systematic reviews and meta-analyses that have compared the effectiveness of US method to that of the traditional method in SPC insertion.
Methods
This umbrella review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (Registration Number: CRD42021290824) and was adhered to both the Cochrane Collaboration Handbook [14] and the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (PRISMA Checklist, Table S1, Supplementary data) [15]. Because we are conscious that the Preferred Reporting Items for Overviews of Reviews (PRIOR) guidelines will be soon released, we have also considered most of the key aspects of methods and results reported in the majority of the overviews of reviews published so far [16].
Search strategy
A comprehensive literature search was conducted in MEDLINE (via PubMed), EMBASE (via Scopus), Web of Science, and Cochrane Library from their inception until February 23, 2022. The following relevant terms were combined through Boolean operators: ‘Ultrasound’, ‘Echoguided’, ‘Ultrasound-guided’, ‘Sonography’, ‘Ultrasonography’, ‘Echo’, ‘Peripheral vein’, ‘Peripheral venous’, ‘Peripheral intravenous’, ‘Vein’, ‘Venous’, ‘Intravenous’, ‘Vascular’, ‘Cannulation’, ‘Access’, ‘Catheterization’, ‘Arterial’, ‘Radial’, ‘Femoral’, ‘PICC’, ‘Central’, ‘Midline’, ‘Systematic review’ and ‘Meta-analysis’. The references of the selected studies and grey literature were reviewed in order to identify additional studies. Articles retrieved were imported and managed by Mendeley reference manager. The search strategy is specified in supplementary material (Table S2).
Selection criteria
Systematic reviews or meta-analyses comparing and addressing the effectiveness, efficiency and patient satisfaction of US-guided peripheral intravenous access versus traditional landmark method in both pediatric and adult patients were included. According to the PICO strategy tool, inclusion criteria were as follows: (a) participants: children (included small children) and adults; (b) intervention: ultrasound-guided peripheral intravenous access; (c) comparison: traditional and ultrasound-guided peripheral intravenous access method; and (d) outcome: efficiency and effectiveness, which were measured through both success and time to cannulation, type and/or number of associated complications and patients’ satisfaction (or parents satisfaction in the case of pediatrics).
Studies were excluded when: (a) involved patients with long-term central venous lines; (b) ultrasound was used to insert an arterial or central venous access, or to insert a LPC or MC; (c) the ultrasound group was compared to another different from the traditional method (such as innovative vascular access technologies, infrared devices or doppler); and (d) its design was not systematic review or meta-analysis of all comparative study designs (randomized control trials, cohort, quasi-experimental, or combinations thereof). No language restriction was applied.
Data extraction
After screening retrieved original systematic reviews, the following data were collected: (a) author and publication year; (b) design and number of included studies in each systematic review; (c) whether or not the meta-analysis was performed; (d) total sample and participants age; (e) no exposed group: defined as traditional landmark method for peripheral intravenous access; (f) exposed group: defined as ultrasound-guided method for peripheral intravenous access; (g) DVA definition; (h) main outcomes measured (overall success, first-attempt success rate, number of attempts, time to success, patient satisfaction and associated complications); (i) professional provider and (j) hospital department.
Methodological quality assessment
The AMSTAR-2 tool was used for the assessment of the methodological quality of systematic reviews that included randomized or non-randomized studies of healthcare interventions, or both. After assessment, the overall confidence in the results of the analyzed review may be high, moderate, low or critically low (if there are more than one critical flaw) [17].
Evidence quality assessment
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) criteria were applied for the assessment of the certainty of evidence of the effect of both techniques on main outcomes measured. GRADE was only applied to meta-analyses of randomized controlled trials, as recommended by Pollock and colleagues, [18] and the domains evaluated were as follows: (i) number of participants; (ii) risk of bias of trials; (iii) heterogeneity; and (iv) methodological quality of the review. Level of evidence was ranked according to established GRADE criteria as high, moderate, low and very low [18].
Two reviewers (C.B-M and JA.M-H) carried out independently the search strategy, studies selection, data extraction, and risk of bias and quality of evidence assessment. Any disagreement was solved by consensus, and, if it could not be reached, a third reviewer was consulted (V.M-V).
Quantitative synthesis
It was not possible to carry out a meta-analysis due to the high heterogeneity of quantitative data from the previous systematic reviews, as originally planned and stated in the PROSPERO record.
Summary findings
As a meta-analysis was not carried out, the results related to the main outcomes provided by each systematic review were graphically represented. Forest plots were used to represent estimates of the main outcomes from original studies, comparing both methods, where stated, including confidence intervals, sample sizes of each group and heterogeneity observed (I2). Using information provided in the included studies, the estimates were represented as relative risk or odds ratio [19], and mean difference or standardized mean difference, depending on the nature of the effect measures. Graphs were performed using STATA SE software, version 15 (StataCorp, College Station, TX, USA).
Results
Study characteristics
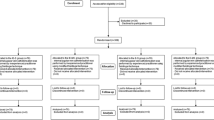
The comprehensive literature search retrieved a total of 2946 articles. From all of them, 12 systematic reviews were included in this systematic review. (Fig. 1) The detailed reasons for exclusion of full-text articles are available in supplementary material (Table S3).

Preferred reporting items for systematic reviews and meta-analyses flow diagram of identification, screening, eligibility and inclusion of studies. WOS, Web of science
The main characteristics of the included systematic reviews are summarized in Table 1. All systematic reviews were published between 2012 to 2022, and only four did not provide quantitative synthesis [13, 20,21,22]. The number of included studies in each review ranged from two [22] to ten [11], most of them provided data from randomized controlled trials (RCT), but four studies also incorporated data from observational studies [11, 12, 20, 23]. Likewise, the sample size of the included systematic reviews ranged from 75 to 1860 [11, 22]. Five studies included only adults as reference population; [11, 12, 20, 22, 24] both adults and pediatric population were included in four studies; [10, 13, 23, 25] and, finally, three studies included only pediatric population [21, 26, 27].
The exposure variable in control group of all reviews was traditional method-guided SPC insertion, defined as both standard/traditional method/technique [10, 21,22,23, 25] and landmark/palpation and direct visualization technique [11,12,13, 20, 24, 26, 27]. Only three out of ten studies did not describe if reference population had history of DVA [11, 12, 27].
Overall, the outcome variables related to the efficiency and effectiveness of US-guided method were as follows: (a) overall success, (b) first-attempt success rate; (c) number of attempts; (d) time spent for SPC insertion; (e) satisfaction of patients; and (f) associated complications to technique (pain, phlebitis, hematoma, accidental catheter removal, obstruction, arterial or nerve puncture and infiltration) [8,9,10,11, 18,19,20,21,22,23,24,25].
Finally, the professional providers participating in the included reviews were anesthetists, physicians, pediatricians, nurses, investigators, fellows and residents or students which carried out the technique in ED, intensive unit care (ICU), operating room (OR), trauma center or surgical hospitalization unit. Only one systematic review did not report the setting in which SPC was inserted [11].
Methodological quality assessment
According to AMSTAR-2, no included studies met all the criteria included in the scale, and the compliance level ranged from 44 to 75% [10, 12, 23, 25, 26]. It should be noted that the overall confidence in the results of all systematic reviews was stablished as ‘Critically low’. On the other hand, all the included reviews met the items related to ‘PICO components’ and ‘Managements of conflict interest’. The ‘Partial yes’ option was assigned to ‘Detailed study description’ item in all the studies. (Table S4, Supplementary data).
GRADE evidence quality
Evidence quality of the 27 associations assessed according to GRADE ranged from ‘Moderate’ (11%) [11] to ‘Very low’ certainty evidence (7.4%) [24, 25]. Twenty-two associations assessed showed ‘Low’ certainty evidence (Table S5) [10,11,12, 23,24,25,26,27]. The evidence map (Table S6) shows that the US-guided method is a protective factor related to both ‘first-attempt success rate’ and ‘number of attempts’ outcomes, with a ‘Moderate’ certainty evidence [11]. Likewise, there is no effect on the use of US-guided method for ‘time’ outcome (‘Moderate’ certainty evidence) [11].
Summary findings
The main results of included systematic reviews were graphically pooled by main outcome variables (Figs. 23 and 4).

Graphical representation of data regarding (A) overall success, (B) first-attempt success rate and (C) number of attempts of US-guided method compared to the traditional method. CI, Confidence interval; MD, Mean difference; NA, Not available; OR, Odds ratio; RR, Relative risk; SMD, Standardized mean difference; US, Ultrasound

Graphical representation of data regarding time spent using US-guided method compared to the traditional method. CI, Confidence interval; MD, Mean difference; NA, Not available; SMD, Standardized mean difference; US, Ultrasound; WMD, Weighted mean difference

Graphical representation of data regarding patient’ satisfaction using US-guided method compared to the traditional method. CI, Confidence interval; MD, Mean difference; SMD, Standardized mean difference; US, Ultrasound
Figure 2 shows the main results related to (A) overall success, (B) first-attempt success rate and (C) number of attempts. Regarding overall success (Fig. 2A), five reviews provided data for the stated relationship, [12, 23, 25,26,27] and four of them found higher success in US method with respect to traditional method, ranging the RR/OR estimates from 1.13 to 3.96 [12, 23, 25, 27]. The heterogeneity (I2) ranged from 41 to 84%.
The findings about first-attempt success rate, for which five studies provided data, are shown in Fig. 2B [11, 12, 24, 26, 27]. Four studies [11, 24, 26, 27] found a significant positive association between US method and first-attempt success rate, ranging the RR/OR estimates from 1.53 to 2.10. The I2 ranged from 0 to 91%.
Figure 2C states the results related to the number of attempts. Seven studies provided data about the stated outcome, [10,11,12, 23,24,25, 27] and only three of them found that US method required lower number of attempts than traditional method, ranging the SMD/MD estimates from -0.27 to -1.93 [10, 11, 27]. The data provided by Egan and colleagues [25] could not be included in the forest plot due to a discrepancy between the effect size and confidence interval. The I2 observed was between 0 to 98.3%.
About the findings about time spent in SPC insertion using both methods, neither of the seven studies which analyzed the association between the method used for SPC insertion and the time spent during the technique found significant results (Fig. 3) [10,11,12, 23,24,25, 27]. The I2 observed was between 0 to 95.1%.
Figure 4 highlights that patient satisfaction was higher when US method was used, ranging the SMD estimates from 0.54 to 1.47 [11, 12, 24]. The I2 observed was between 0 to 77%.
Finally, secondary outcomes such as pain, phlebitis, hematoma, accidental catheter removal, obstruction, arterial and nerve puncture and infiltration -associated complications- were not graphically represented due to the unavailability of quantitative data. Seven studies took into account these complications, [10,11,12, 20, 24, 26, 27] where infiltration, pain and arterial puncture were the most frequently mentioned, and only one study reported pooled quantitative data about infiltration in pediatric patients, and a significant protective effect of US-guided method was not found [RR = 1.59 (0.99,2.54) I2 = 0%] [27]. Together with the infiltration, the pain reported by patients was the most frequently secondary outcome discussed [12, 20, 26]. Among all the original RCTs included in the previous meta-analyses, one RCT which included adult patients reported lower pain rates when US-guided method was used, [28] while other RCT which studied pediatric patients showed lower arterial puncture rates when US-guided method was used [29] (Table S7).
Discussion
The synthesis of the systematic reviews and meta-analyses included in this umbrella review support that the use of US-guided method, compared to the traditional method, increases the success rates and reduces the number of attempts needed in SPC insertion in both adults and pediatric patients. Likewise, the satisfaction was higher in those groups of patients in whom the US-guided method was used, albeit with a low certainty level. Conversely, it is not clear whether the US-guided method is more efficient than the traditional one because there was not a significant reduction in the time spent in SPC insertion.
The previously available evidence regarding the effectiveness of US guided cannulation seems to be controversial. The majority of meta-analyses published to date support that the overall success, the first-attempt success, and the number of attempts rates support the use of the US guided procedure, and it could decrease problems associated to SPC insertion, such as pain, dissatisfaction or anxiety [30].
Considering that pediatrics have particular conditions and a higher failure rate, as it happens in adults, [4, 31] US is presented as a valid alternative in both populations. However, Kleidon and colleagues [26] did not find a positive effect of US-guided method in the overall success in children, as reported in four previous meta-analyses in both adult and children [12, 23, 25, 27] and in a recent study that showed an overall success rate above 90% [32]. On the other hand, the findings of Van loon and colleagues [12] are not in line with the association between US-guided method and the first-attempt success rate, which was reported with a moderate certainty level [11, 24, 26, 27] and which is supported by a recent study in patients with DVA [32]. In regard to the number of attempts, Tran and colleagues [11] found a positive significant association in favor of US-guided method in adults, although with several discrepancies.
The variability in the estimates could be a consequence of the differences in both the way to measure the experience and training of operators and the device used [10, 25]. In the same line, providers have extensive experience in the traditional technique, which could underestimate the potential benefit of the US-guided technique [33]. On the other hand, there is neither agreement on the groups studied nor on the distribution by age group (< 3, < 7, < 10 and/or < 18 years).
Regarding efficiency, no studies found a significant positive effect of US versus traditional method in the time spent in SPC insertion, as stated by a recent RCT which has not been included in any systematic review [34]. The lack of significant findings may result from the large variability among studies. Several methodology-related reasons could be behind this variability, such as differences in the definitions of procedure length [35,36,37]. Likewise, history of DVA has not been well-defined in all studies. Since a validated scale for reporting DVA is not available, each study could define it in a different way [12]. Thus, the use of a predicting scale to recognize patients with DVA may improve the methodological quality of further studies [38, 39]. The use of validated methods is important because the inexperience of the operator could be mistaken for a difficult access, which involves a risk of bias [25].
Regarding patients’ satisfaction, although our findings only referred to adult population, the higher rates were obtained when US-guided method was used, except in one study [11, 12, 24]. One reason which could respond to the variability in findings about satisfaction, and which is applicable to the rest of outcomes, is the context where studies were developed. It is logical to think that both the pressure on healthcare personnel and the target response time vary among hospital departments, [40] so the SPC insertion technique is not carried out on equal terms. For example, in the treatment of cardiac arrests in pediatric population the European Resuscitation Council Guidelines 2021 recommend getting a vascular access in 5 min at most and suggest the use of US to guide cannulation in competent providers [41]. Considering that ED is a hospital area where cardiac arrests are common, [42] it seems reasonable to assume that there might be differences between different hospital areas in the US-guided method for SPC cannulation.
In spite of the possible controversial findings and the wide heterogeneity in the studies included, US-guided method seems to be a useful technique that could improve the quality indexes regarding the care and safety of the patient. Likewise, these findings might help to reduce the central venous catheterization (CVC) in patients with DVA, as stated by Au and colleagues, [43] which could avoid the CVC-associated complications [44]. However, this technique requires an in-depth knowledge by operators, [26, 45] and the traditional technique training is more established compared to the US-guided method, [33] although the US training could be further enhanced by the use of long peripheral catheters in DVA patients [46, 47]. The development of training programs could enhance the use of this alternative and its benefits [48]. Furthermore, the inexistence of significant benefit in the time spent in US-guided method, together with pressure on healthcare personnel in certain hospital departments and the availability of the required US equipment, could limit the use of this alternative. However, according to ERPIUP Consensus, those US-guided SPC used to canalize deep vein could have a duration of about 24 h or less [7], so it is necessary further research in order to elucidate the differences between short and long peripheral catheters in terms of feasibility and duration. Likewise, operators should consider this statement in the different clinical situations because the US-guided SPC insertion could be a great tool in the immediate treatment of DVA patients, but it could also be a handicap in long-term intravenous treatments, particularly if the canalized vein is deep.
Limitations of the study
Firstly, there are methodological differences between the studies included, especially in the quantitative synthesis and the operationalization of variables. Secondly, there is a large overlap between previous systematic reviews included in our umbrella review. (Table S8). On the other hand, the ‘peripheral intravenous catheters (PIVCs)’ terminology is ambiguous, and its use in some of the included previous studies could be associated with the existence of selection bias specially if some of them have included LPC or MC within the PIVCs. Finally, considering that several systematic reviews included compared data from both RCT and observational studies, the findings must be cautiously interpreted because the analysis of effectiveness of clinical techniques through observational studies could lead to several limitations. These limitations could be counterbalanced with further RCTs that include patients with similar age categorized by hospital areas, using a standardized definition of both the PVADs and the procedure length and a validated scale for DVA definition. Likewise, the comparison between both techniques should be carried out through operators who report similar levels of expertise.
Conclusions
US-guided method for SPC insertions has shown itself to be more effective in terms of success rates and patient satisfaction when compared to traditional landmark method in adult and pediatric population. Our results have clinical importance because it could benefit patients with special conditions which difficult the venous access or whose venous resources have particular characteristics. Likewise, this method, by reducing the common technique-associated complications, could increase the quality of healthcare and stablish an optimal level of compliance between patients and providers. With a moderate certainty level, the US-guided method is postulated as a valid alternative in comparison with the traditional method in the SPC insertion. A higher success rate, a lower number of unsuccessful attempts and a lower presence of associated complications make the US-guided method the main option in patients with DVA.
Availability of data and materials
All data analyzed during this study are included in this article [and its supplementary information files].
Abbreviations
- AMSTAR:
-
Assessment of multiple systematic reviews
- CI:
-
Confidence interval
- CVC:
-
Central venous catheterization
- DVA:
-
Difficult venous access
- ED:
-
Emergency department
- EMBASE:
-
Excerpta Medica Data Base
- ES:
-
Effect size
- GRADE:
-
Grading of Recommendations, Assessment, Development, and Evaluation
- I2 :
-
Heterogeneity
- ICU:
-
Intensive unit care
- LPC:
-
Long peripheral catheters
- MC:
-
Midline catheters
- MEDLINE:
-
Medical Literature Analysis and Retrieval System Online
- MD:
-
Mean difference
- NA:
-
Not available
- No:
-
Number
- OR:
-
Odds ratio
- OR*:
-
operating room
- PICC:
-
Peripherally Inserted Central Catheter
- PICO:
-
Patient Intervention Comparison And Outcome
- PIVCs:
-
Peripheral intravenous catheters
- PRIOR:
-
Preferred Reporting Items for Overviews of Reviews
- PRISMA:
-
Preferred Reporting Items for Systematic Review and Meta-Analyses
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- PVADs:
-
Peripheral venous access devices
- RCT:
-
Randomized controlled trial
- RR:
-
Relative Risk
- SMD:
-
Standardized mean difference
- SPC:
-
Short peripheral catheter
- STATA:
-
Statistics and data
- US:
-
Ultrasonography
- WMD:
-
Weighted mean difference
- WOS:
-
Web of science
References
Alexandrou E, Ray-Barruel G, Carr PJ, Frost S, Inwood S, Higgins N, et al. International prevalence of the use of peripheral intravenous catheters. J Hosp Med. 2015;10:530–3.
Zingg W, Pittet D. Peripheral venous catheters: an under-evaluated problem. Int J Antimicrob Agents. 2009;34:S38-42.
Thomas C, Cabilan CJ, Johnston ANB. Peripheral intravenous cannula insertion and use in a tertiary hospital emergency department: A cross-sectional study. Australas Emerg Care. 2020;23:166–72.
Helm RE, Klausner JD, Klemperer JD, Flint LM, Huang E. Accepted but Unacceptable: Peripheral IV Catheter Failure. J Infus Nurs. 2015;38:189–203.
Miles G, Salcedo A, Spear D. Implementation of a Successful Registered Nurse Peripheral Ultrasound-Guided Intravenous Catheter Program in an Emergency Department. J Emerg Nurs. 2012;38:353–6.
Brannam L, Blaivas M, Lyon M, Flake M. Emergency nurses’ utilization of ultrasound guidance for placement of peripheral intravenous lines in difficult-access patients. Acad Emerg Med. 2004;11:1361–3.
Pittiruti M, Van Boxtel T, Scoppettuolo G, Konstantinou E, Ortiz Miluy G, Lamperti M, et al. European recommendations on the proper indication and use of peripheral venous access devices (the ERPIUP consensus): A WoCoVA project. J Vasc Access. 2021;0:1-18.
Gorski LA, Hadaway L, Hagle ME, Broadhurst D, Clare S, Kleidon T, et al. Infusion Therapy Standars of Practice, 8th Edition. J Infus Nurs. 2021;44(1S Suppl 1):S1–224.
Ortega R, Sekhar P, Song M, Hansen CJ, Peterson L. Peripheral Intravenous Cannulation. N Engl J Med. 2008;359:e26.
Heinrichs J, Fritze Z, Vandermeer B, Klassen T, Curtis S. Ultrasonographically guided peripheral intravenous cannulation of children and adults: A systematic review and meta-analysis. Ann Emerg Med. 2013;61:444-454.e1.
Tran QK, Fairchild M, Yardi I, Mirda D, Markin K, Pourmand A. Efficacy of Ultrasound-Guided Peripheral Intravenous Cannulation versus Standard of Care: A Systematic Review and Meta-analysis. Ultrasound Med Biol. 2021;47:3068–78.
van Loon FHJ, Buise MP, Claassen JJF, Dierick-van Daele ATM, Bouwman ARA. Comparison of ultrasound guidance with palpation and direct visualisation for peripheral vein cannulation in adult patients: a systematic review and meta-analysis. Br J Anaesth. 2018;121:358–66.
Liu YT, Alsaawi A, Bjornsson HM. Ultrasound-guided peripheral venous access: A systematic review of randomized-controlled trials. Eur J Emerg Med. 2014;21:18–23.
Pollock M, Fernandes RM, Becker LA, Pieper D, Hartling L. Chapter V: Overviews of Reviews. In: Higgins JPT, Thomas J, Chandler J, et al (eds). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71.
Pollock M, Fernandes RM, Pieper D, Tricco AC, Gates M, Gates A, et al. Preferred Reporting Items for Overviews of Reviews (PRIOR): A protocol for development of a reporting guideline for overviews of reviews of healthcare interventions. Syst Rev. 2019;8:1–9.
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008.
Pollock A, Farmer SE, Brady MC, Langhorne P, Mead GE, Mehrholz J, et al. An algorithm was developed to assign GRADE levels of evidence to comparisons within systematic reviews. J Clin Epidemiol. 2016;70:106–10.
Stare J, Maucort-Boulch D. Odds ratio, hazard ratio and relative risk. Metod Zv. 2016;13:59–67.
Varndell W, Topacio M, Hagness C, Lemon H, Tracy D. Nurse-performed focused ultrasound in the emergency department: A systematic review. Australas Emerg Care. 2018;21:121–30.
Parker SIA, Benzies KM, Hayden KA. A systematic review: effectiveness of pediatric peripheral intravenous catheterization strategies. J Adv Nurs. 2017;73:1570–82.
Parker SIA, Benzies KM, Hayden KA, Lang ES. Effectiveness of interventions for adult peripheral intravenous catheterization: A systematic review and meta-analysis of randomized controlled trials. Int Emerg Nurs. 2017;31:15–21.
Stolz LA, Stolz U, Howe C, Farrell IJ, Adhikari S. Ultrasound-guided peripheral venous access: A meta-analysis and systematic review. J Vasc Access. 2015;16:321–6.
Egan G, Healy D, O’neill H, Clarke-Moloney M, Grace PA, Walsh SR. Ultrasound guidance for difficult peripheral venous access: Systematic review and meta-analysis. Emerg Med J. 2013;30:521–6.
Tran QK, Flanagan K, Fairchild M, Yardi I, Pourmand A. Nurses and Efficacy of Ultrasound-guided Versus Traditional Venous Access: A Systemic Review and Meta-analysis. J Emerg Nurs. 2022;48:145-158.e1.
Kleidon TM, Schults J, Rickard CM. Techniques and Technologies to Improve Peripheral Intravenous Catheter Outcomes in Pediatric Patients: Systematic Review and Meta-Analysis. J Hosp Med. 2021;16:742–50.
Ye X, Li M. Comparison of ultrasound guided and conventional techniques for peripheral venous catheter insertion in pediatric patients: a systematic review and meta-analysis of randomized controlled trials. Front Pediatr. 2022;9:797705.
Darvish AH, Shroff SD, Mostofi MB, Weiner S, Sarff AR. Single-Operator Ultrasound-Guided IV Placement by Emergency Nurses. J Emerg Med. 2011;41:211–2.
Doniger SJ, Ishimine P, Fox JC, Kanegaye JT. Randomized controlled trial of ultrasound-guided peripheral intravenous catheter placement versus traditional techniques in difficult-access pediatric patients. Pediatr Emerg Care. 2009;25:154–9.
Page DE, Taylor DMD. Vapocoolant spray vs subcutaneous lidocaine injection for reducing the pain of intravenous cannulation: A randomized, controlled, clinical trial. Br J Anaesth. 2010;105:519–25.
Indarwati F, Mathew S, Munday J, Keogh S. Incidence of peripheral intravenous catheter failure and complications in paediatric patients: Systematic review and meta analysis. Int J Nurs Stud. 2020;102:103488.
Privitera D, Mazzone A, Pierotti F, Airoldi C, Galazzi A, Geraneo A, et al. Ultrasound-guided peripheral intravenous catheters insertion in patient with difficult vascular access: Short axis/out-of-plane versus long axis/in-plane, a randomized controlled trial. J Vasc Access. 2021;23:589–97.
Weiner MM, Geldard P, Mittnacht AJC. Ultrasound-guided vascular access: a comprehensive review. J Cardiothorac Vasc Anesth. 2013;27:345–60.
Yalçınlı S, Akarca FK, Can Ö, Uz İ, Konakçı G. Comparison of standard technique, ultrasonography, and near-infrared light in difficult peripheral vascular access: a randomized controlled trial. Prehosp Disaster Med. 2022;37:65–70.
Aponte H, Acosta S, Rigamonti D, Sylvia B, Austin P, Samolitis T. The use of ultrasound for placement of intravenous catheters. AANA J. 2007;75:212–6.
Bauman M, Braude D, Crandall C. Ultrasound-guidance vs. standard technique in difficult vascular access patients by ED technicians. Am J Emerg Med. 2009;27:135–40.
Kerforne T, Petitpas F, Frasca D, Goudet V, Robert R, Mimoz O. Ultrasound-guided peripheral venous access in severely ill patients with suspected difficult vascular puncture. Chest. 2012;141:279–80.
Sebbane M, Claret PG, Lefebvre S, Mercier G, Rubenovitch J, Jreige R, et al. Predicting peripheral venous access difficulty in the emergency department using body mass index and a clinical evaluation of venous accessibility. J Emerg Med. 2013;44:299–305.
Angles E, Robin F, Moal B, Roy M, Sesay M, Outtara A, et al. Pre-operative peripheral intravenous cannula insertion failure at the first attempt in adults: Development of the VENSCORE predictive scale and identification of risk factors. J Clin Anesth. 2021;75:110435.
Hooper C, Craig J, Janvrin DR, Wetsel MA, Reimels E. Compassion satisfaction, burnout, and compassion fatigue among emergency nurses compared with nurses in other selected inpatient specialties. J Emerg Nurs. 2010;36:420–7.
Van De Voorde P, Turner NM, Djakow J, de Lucas N, Martínez-Mejías A, Biarent D, et al. European resuscitation council guidelines 2021: paediatric life support. Resuscitation. 2021;161:327–87.
Donoghue AJ, Abella BS, Merchant R, Praestgaard A, Topjian A, Berg R, et al. Cardiopulmonary resuscitation for in-hospital events in the emergency department: a comparison of adult and pediatric outcomes and care processes. Resuscitation. 2015;92:94–100.
Au AK, Rotte MJ, Grzybowski RJ, Ku BS, Fields JM. Decrease in central venous catheter placement due to use of ultrasound guidance for peripheral intravenous catheters. Am J Emerg Med. 2012;30:1950–4.
Parienti J-J, Mongardon N, Mégarbane B, Mira J-P, Kalfon P, Gros A, et al. Intravascular Complications of Central Venous Catheterization by Insertion Site. N Engl J Med. 2015;373:1220–9.
McCarthy ML, Shokoohi H, Boniface KS, Eggelton R, Lowey A, Lim K, et al. Ultrasonography versus landmark for peripheral intravenous cannulation: a randomized controlled trial. Ann Emerg Med. 2016;68:10–8.
Qin KR, Pittiruti M, Nataraja RM, Pacilli M. Long peripheral catheters and midline catheters: Insights from a survey of vascular access specialists. J Vasc Access. 2021;22(6):905–10.
Qin KR, Ensor N, Barnes R, Englin A, Nataraja RM, Pacilli M. Long peripheral catheters for intravenous access in adults and children: A systematic review of the literature. J Vasc Access. 2021;22(5):767–77.
Edwards C, Jones J. Development and implementation of an ultrasound-guided peripheral intravenous catheter program for emergency nurses. J Emerg Nurs. 2018;44:33–6.
Acknowledgements
We would like to thank the researchers from the Health and Social Research Center for their support during the preparation of this systematic review and meta‑analysis.
Funding
This study was funded by European Regional Development Fund (ERDF). ISD is supported by a grant from the Spanish Ministry of Educational and Vocational Training (FPU19/00109). ASL is supported by a grant from the University of Castilla-La Mancha (2019-PREDUCLM-10708).
Author information
Authors and Affiliations
Contributions
CBM and JAMH designed the study. CBM and JAMH were the principal investigators and guarantors. ADF and VMV established the methods. JAMH, ADF and VMV were the main coordinators of the study. CBM, ADF and VMV conducted the study. ADF, ISD and JAMH gave statistical and epidemiological support. CBM wrote the article with the support of ADF, JAMH, ISD, ASL, DPC and VMV. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Table S1
. PRISMA 2020 Checklist. Table S2. Search strategy from database inception to 23rd February 2022. Table S3. Excluded studies from the umbrella review with reasons. Table S4. Methodological quality assessment by AMSTAR-2 (a critical appraisal tool for systematic reviews of healthcare interventions). Table S5. Certainty of evidence according to Grading of Recommendation Assessment, Development, and Evaluation (GRADE). Table S6. Evidence map. Table S7. Characteristics of the randomized controlled trials which compare traditional versus US-guided method for SPC insertion and have been included in the previous meta-analyses. Table S8. Study overlaps in included systematic reviews and meta-analyses.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Berlanga-Macías, C., Díez-Fernández, A., Martínez-Hortelano, J.A. et al. Ultrasound-guided versus traditional method for peripheral venous access: an umbrella review. BMC Nurs 21, 307 (2022). https://doi.org/10.1186/s12912-022-01077-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-022-01077-9