
Abstract
Background
The addition of coronary artery calcium score (CACS) to prediction models has been verified to improve performance. Machine learning (ML) algorithms become important medical tools in an era of precision medicine, However, combined utility by CACS and ML algorithms in hypertensive patients to forecast obstructive coronary artery disease (CAD) on coronary computed tomography angiography (CCTA) is rare.
Methods
This retrospective study was composed of 1,273 individuals with hypertension and without a history of CAD, who underwent dual-source computed tomography evaluation. We applied five ML algorithms, coupled with clinical factors, imaging parameters, and CACS to construct predictive models. Moreover, 80% individuals were randomly taken as a training set on which 5-fold cross-validation was done and the remaining 20% were regarded as a validation set.
Results
16.7% (212 out of 1,273) of hypertensive patients had obstructive CAD. Extreme Gradient Boosting (XGBoost) posted the biggest area under the receiver operator characteristic curve (AUC) of 0.83 in five ML algorithms. Continuous net reclassification improvement (NRI) was 0.55 (95% CI (0.39–0.71), p < 0.001), and integrated discrimination improvement (IDI) was 0.04 (95% CI (0.01–0. 07), p = 0.0048) when the XGBoost model was compared with traditional Models. In the subgroup analysis stratified by hypertension levels, XGBoost still had excellent performance.
Conclusion
The ML model incorporating clinical features and CACS may accurately forecast the presence of obstructive CAD on CCTA among hypertensive patients. XGBoost is superior to other ML algorithms.
Similar content being viewed by others

Introduction
Hypertension affects approximately one-third of the world’s adult population and is a major risk for the presence of coronary artery disease (CAD) [1]. Arguably the biggest challenge for cardiologists is to more accurately identify patients with obstructive CAD among all individuals with hypertension. Coincidentally, coronary computed tomography angiography (CCTA) has emerged as a non-invasive and popular method for the evaluation of CAD for many years [2, 3]. With the extensive application of CCTA in clinical practice, it is imperative to optimize patient selection to improve diagnostic yield and cost-effectiveness of CCTA [4].
The coronary artery calcium (CAC) scan, different from the CCTA, can be accomplished with 10 to 15 min of total room time at about 1 mSy of radiation, without the need for contrast agents [5]. CAC, as a biomarker of subclinical atherosclerosis, is the most significant independent predictor for cardiovascular events as well as all-cause mortality [6, 7]. Furthermore, accumulated evidence has demonstrated that the absence of coronary artery calcium (CAC) in CCTA represents a low risk for the incidence of cardiovascular events while there is increased cardiovascular risk with CACS increasing [8, 9]. In addition, the addition of CACS to clinical prediction models has been revealed to improve predictive performance for CAD [10, 11]. Interestingly, previous reports have unveiled that CAC is not only accelerated by hypertension but also contributes to hypertension [12]. However, the predictive importance of CACS for obstructive CAD in hypertensive patients has rarely been defined.
Machine learning (ML) is an emerging sort of artificial intelligence (AI) and is skilled at uniting diverse population characteristics to fit superior prediction models. Thus, ML has been widely applied to healthcare data analysis in recent years [13, 14]. By taking full advantage of the powerful prediction ability of ML algorithms, it may be feasible to develop prediction tools that surpass traditional statistical models in some cases, thus optimizing the prediction of CAD and decreasing the extensive use of CCTA in hypertensive patients. In this study, we seek to develop ML-based models integrating clinical factors and CACS, to forecast the presence of obstructive CAD on CCTA among patients with hypertension.
Methods
Study population and definition
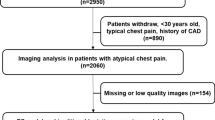
We retrospectively screened 1,346 hypertensive patients without a history of CAD who were admitted to the Department of Hypertension and underwent CCTA examination in the First Affiliated Hospital of Dalian Medical University from January 2014 to December 2017. Hypertension is defined as a prior diagnosis of hypertension or the use of antihypertensive medications. Definition of hypertension is based on the 2017 ACC/AHA guideline (systolic blood pressure (SBP) ≥ 140 mm Hg and/or diastolic blood pressure (DBP) ≥ 90 mm Hg). Meanwhile, patients previously diagnosed with CAD according to CCTA, coronary angiography, treadmill exercise testing, and (or) typical chest pain symptoms were excluded. Additional exclusion criteria were missing data of scan identifiers, uncertain date of birth, and unavailable CACS. Patients with severe hepatic/renal insufficiency, malignant disease, and poor CCTA image quality were excluded. Moreover, laboratory parameters were from fasting venous blood which was collected on the second morning of admission and detected in the biochemistry lab of the First Affiliated Hospital of Dalian Medical University.
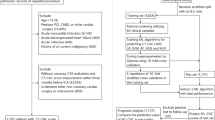
The data included baseline patient characteristics, the results of blood tests, and imaging data in the preliminary experiment. For data preprocessing, we removed variables that have no clinical significance, and deleted some variables that have no obvious causal relationship with the outcomes. The dataset was imputed using multiple imputation. Then, the recursive feature elimination (RFE) algorithm was used to select key variables and develop machine learning model. Finally, A total of 68 variables from 1,273 people were eventually applied in the study (Detailed study flow was shown in Fig. 1, and the list of included variables is shown in Supplementary Table 1). Furthermore, all the individuals were randomly distributed into two sets, namely the training set (80%) for ML model development and the validation set (20%) for performance evaluation. Furthermore, random splitting was repeated until the patients were equally distributed in both sets. The comparable differences in baseline characteristics between the training set and the validation set were shown in Supplementary Table 2.

Flow chart of the study
CAD, coronary artery disease; CCTA, coronary computed tomography angiography; CACS, coronary artery calcium score
Coronary computed tomography angiography and coronary artery calcium scanning
According to the guidelines outlined by the Society of Cardiovascular Computed Tomography, CCTA image acquisition, and processing, as well as coronary artery calcium scanning, were performed on the scanner (dual-source, Somatom Definition CT, Siemens, Erlangen, Germany). Two professional imaging physicians blind to the patients’ clinical data independently evaluated all images to determine the extent of CAD and provide a CACS using the Agatston method which semi-automatically calculates a weighted sum of the area of coronary calcification in line with the available study [15]. The presence of diameter stenosis ≥ 50% in any of the four major epicardial coronary arteries detected on CCTA was defined as obstructive CAD.
The optimal machine learning model
Five types of ML algorithms were performed to model our data: Extreme Gradient Boosting (XGBoost), Random Forest (RF), Support Vector Machine (SVM), Neural Network (NNET), and traditional Logistic Regression (LR). The traditional LR model used in this study was composed of traditional clinical factors (including age, gender, stage of hypertension, history of diabetes mellitus, current smoker, as well as the levels of total cholesterol and triglyceride) and CACS. Moreover, the remaining 4 models included all available variables. Meanwhile, tuning was considered to avoid overfitting for ML-based models and the optimal hyper-parameter in the training process for ML models was 5-fold cross-validation. Followingly, the R software was applied to further train the ML algorithms to forecast the presence of obstructive CAD. Furthermore, the best-performing algorithm (with the highest area under the receiver operator characteristic curve (AUC)) was used to construct the classifier from the whole training set, with the same hyper-parameter, and applied it to the validation set to independently assess the predictive performance [16]. Additionally, shapely additive explanations (SHAP) was calculated to assess the feature ranking, as previously described [17].
Statistical analysis
Kolmogorov–Smirnov test was applied to assess the distribution of continuous variables. Normally distributed continuous variables were expressed as mean (standard deviation (SD)) and compared with the t-test; non-normally distributed continuous variables were expressed as median (interquartile range) and compared with the non-parametric test. Fisher’s exact test was used to assess the differences between categorical variables, which are reported as a number (percentage). A multivariable logistic regression analysis with backward stepwise selection was applied to verify the independent risk factors of obstructive CAD and related results were reported as odds ratios (ORs) (95% confidence intervals (CIs)).
Five ML algorithms were compared to find the best algorithm. Further, the optimal algorithm was compared with the traditional LR regression using the calibration curve and Hosmer-Lemeshow test. In the subgroup analysis of hypertension, the corresponding sensitivity, specificity, positive predictive value, negative predictive value, as well as overall accuracy of ML algorithms were calculated. In addition, net reclassification improvement (NRI) and integrated discrimination improvement (IDI) were applied to compare predictive performance between the best ML algorithm and the traditional LR model. Additionally, SHAP was calculated to assess the importance of variables included in the XGBoost model. R software (https://www.r-project.org/) was used in statistical analyses. A two-tailed p < 0.05 was considered statistically significant.
Results
Demographic features
A total of 1,273 patients were finally included in the study and divided into two groups according to the presence of obstructive CAD (shown in Table 1). The prevalence of obstructive CAD was 16.3% (212 out of 1,273). Moreover, the proportion of CACS > 0 in the general population was 54.6% (695 out of 1,273), and 92% (195 out of 212) in obstructive CAD. The prevalence of males, previous diabetes mellitus, and current smokers was significantly higher in the obstructive CAD group (p < 0.05). The differences in CACS between the two groups were obvious (p < 0.05).
Univariate and multivariate logistic regression analysis of obstructive CAD
In univariate analysis, age, gender, history of diabetes mellitus, current smoker, and CACS were all significantly linked to obstructive CAD (p < 0.05), whereas there was no significant difference in total cholesterol levels. In multivariable logistic regression analysis, the results revealed that age (OR 1.035, 95% CI (1.021–1.050), p < 0.001), current smoker (OR 1.699, 95% CI (1.108–2.626), p = 0.016), and CACS (OR1.002, 95% CI (1.001–1.002), p < 0.001) were independently related to obstructive CAD. In addition, hypertension [stage 2 vs. stage 1 (OR 3.433, 95% CI (1.099–12.82), p = 0.046); stage 3 vs. stage 1(OR 3.373, 95% CI (1.254–10.932), p = 0.030)] was a positive predictor for obstructive CAD (shown in Table 2).
Performance of machine learning algorithm for obstructive CAD
Within the training cohort and validation cohort, comparisons of the performance of the five ML algorithms models were detailed in Fig. 2, and their performance was evaluated based on the area under the receiver operating characteristics curve (AUC) through 5-fold cross-validation (AUC of the RF model (SD) = 0.8090(0.04); AUC of the SVM model (SD) = 0.7524 (0.05); AUC of the LR model (SD) = 0.7558 (0.03); AUC of the XGBoost model (SD) = 0.8266 (0.03); AUC of the NNET (SD) = 0.7127(0.07)). The predictive value and optimal cutoff in the different machine learning algorithms for obstructive CAD were presented in Table 3. Moreover, XGBoost, as the best-performing algorithm, achieved a high AUC of 0.794 in the independent validation set (shown in Fig. 3).

The area under the curve as a measure of individual model performance for the prediction of obstructive coronary artery disease on coronary computed tomography angiography in training cohort (A) and validation cohort (B)
AUC, area under the curve; LR, Logistic Regression; XGBoost, Extreme Gradient Boosting; RF, Random Forest; SVM, Support Vector Machine; NNET, Neural Network

The receiver operating characteristic curve from applying the best-performing classifier (XGBoost) built in validation cohort
AUC, the area under the curve; XGBoost, Extreme Gradient Boosting
To evaluate the deterministic of a given new observation belonging to one of the already established sorts (prediction value for the presence or absence of CAD on CCTA), Model calibration was applied (shown in Fig. 4). Interestingly, the minimum difference between the predicted and observed likelihood of obstructive CAD appeared in the XGBoost model. That is, the XGBoost model achieved a good model fit. Further, the Hosmer-Lemeshow test indicates that the XGBoost model had a high calibration (p = 0.301), while the traditional LR model was disappointing (p < 0.05). Additionally, continuous NRI was 0.55 (95% CI (0.39–0.71), p < 0.001), IDI was 0.04 (95% CI (0.01–0. 07), p = 0.0048) when the XGBoost model was compared with LR Models.

Calibration curve for different models for prediction of the likelihood of obstructive CAD
LR, Logistic Regression; XGBoost, Extreme Gradient Boosting; RF, Random Forest; SVM, Support Vector Machine; NNET, Neural Network; CAD, coronary artery disease
Feature importance in the XGBoost model
As shown in Fig. 5, the probability of the prevalence of obstructive CAD increased, with CACS increasing. That is, CACS had the highest predictive value for the presence of obstructive CAD. Age was the second important variable and was followed by plasma triglycerides levels, estimated glomerular filtration rate (eGFR), and plasma creatinine levels. Interestingly, carotid intima-media thickness was also related to obstructive CAD among imaging parameters.

Feature importance plot in the XGBoost model
The top 15 clinical variables are shown. The yellow and purple points in each row represent participants having low to high values of the specific variable, while the x-axis gives the SHAP value which affects the model [i.e. does it tend to drive the predictions towards the event (positive value of SHAP) or non-event (negative value of SHAP)]
CACS, coronary artery calcium score; XGBoost, extreme gradient boosting; SHAP, Shapley additive explanation values; E/e’, early diastolic transmitral velocity to early mitral annulus diastolic velocity ratio; Carotid artery IMT, Carotid artery intima-media thickness
Subgroup analysis stratified by Hypertension levels
Because the proportion of patients in stage 1 and stage 2 hypertension was low, we grouped patients according to whether they were in stage 3 hypertension or not. The proportion of CAC > 0 in stage 3 hypertension was significantly higher than that in patients without stage 3 hypertension, and a similar result was found with CACS as a continuous variable(p < 0.05) (shown in Table 4). The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of the XGBoost model for obstructive CAD in patients with stage 3 hypertension were 82.0%, 87.6%, 57.9%, 93.1%, and 84.8%, respectively; results were and 86.9%, 90.5%, 53.3%, 92.3%, and 88.7% in non-stage 3 hypertensive patients (shown in Table 5).
Discussion
In this study, we developed and validated multiple popular ML algorithms to forecast the presence of obstructive CAD in hypertensive patients. A comparison among five ML algorithms demonstrated that the XGBoost model was the most excellent in terms of predictive power and appropriate for patients with different levels of blood pressure (BP). The ML algorithm-based model was potentially able to guide clinical decision-making and improve risk stratification in hypertensive patients. In addition, this study further emphasized the importance of CACS as a risk stratification tool in hypertensive patients.
The importance of machine learning
The current study demonstrated that ML algorithms are necessary and applicable in the context of clinical requirements. Furthermore, the XGBoost model is the most appropriate model among the five ML algorithms in terms of predictive power for the presence of obstructive CAD in hypertensive patients and is superior to traditional regression models. CAD is a common and frequently-occurring disease linked to high morbidity, mortality, and healthcare expenditure. To invasively forecast the occurrence of CAD, many models have been developed. Nevertheless, the performance of most of the existing models is limited to the presence of CAD [18,19,20]. Additionally, the discriminative ability of several models becomes lower, when they have been validated in more than one external population [21]. This downward trend may be partly attributed to the utilization of diverse imaging modalities as well as the different definition of obstructive CAD, and model complexity. Importantly, with the development of social and extensive popularization of health knowledge, dietary habits, environmental exposures, and preventative practices are ever-changing. Therefore, previous models may not be comprehensive. That is, there is an urgent need for optimal predictive models for obstructive CAD in hypertensive patients. ML algorithms became an available and suitable option, as a result of two inherent characteristics. On the one hand, ML algorithms are superior to the one-dimensional traditional statistical methods in terms of finding correlations between variables; on the other hand, ML algorithms are optimal to make use of increasingly complex data that is pivotal to improving prediction performance. And not coincidentally, ML algorithms have been verified to be a powerful predictive tool in the context of cardiovascular applications [22,23,24]. Similarly, the predictive power of ML for obstructive CAD was superior to traditional models in this study. Meanwhile, the XGBoost model may be the optimal model given calibration and predictive performance for the presence of obstructive CAD in patients with hypertension. This study upholds that intermediate to high-risk hypertensive patients evaluated by the XGBoost model to directly receive further testing such as CCTA and coronary angiography, as well as preventive therapies, may be reasonable and cost-efficient.
The importance of coronary artery calcium score
The current study uncovered that CACS is the most important factor among the diverse clinical parameters that can stratify hypertensive patients with the risk of obstructive CAD. Previous researchers have unveiled that the performance of predictive models was markedly improved by the addition of CACS [10, 11, 25]. For example, the C-statistic increased from 0.79 to 0.88 with the addition of the CACS to extend CAD clinical score to forecast the presence of obstructive CAD on invasive coronary angiography [26]. Furthermore, the Heinz Nixdorf Recall (HNR) study demonstrated the absence of coronary calcium represents a relatively low CVD risk regardless of BP stage in hypertensive patients. Namely, CAC was a more robust predictor for cardiovascular events than BP levels in the HNR study. Whatever in any BP category, the adjusted hazard ratios of cardiovascular events grew with the increase of CACS. Meanwhile, an increasing BP level played no (or only a modest) role in CAD risk within each CACS category [27]. Taken together, the accumulated studies support that CACS is very valuable to optimize risk stratification in hypertensive patients. Most previous researches prospectively focused on the relations between CACS and MACEs, however, cross-sectional studies evaluating the predictive performance of CACS for obstructive CAD in patients with hypertension were rare. Our study from cross-sectional data unveiled that CACS is a superior predictor for the occurrence of obstructive CAD in patients with different blood pressure levels. Given its high predictive value, CACS may be an applicable tool to guide clinical decision-making and optimize treatment strategies even in patients with prehypertension and mild hypertension, while without the symptoms of CAD. Our investigation greatly enhances the evidence of CACS as a significant risk stratification tool in hypertensive adults and supports a stronger recommendation of the CACS in future clinical guidelines.
The relationship between Hypertension and coronary artery calcification
To a certain extent, this study further verified that hypertension and coronary artery calcification mutually reinforce. With the aging population and epidemic of obesity in recent years, the prevalence of hypertension is scheduled to gradually increase in the future. Moreover, hypertension is an independent risk for the development of atherosclerosis [28]. Therefore, rational methods about how to early and non-invasively forecast the prevalence of CAD attract more and more attention in patients with hypertension. As far as we know, vascular calcifications are not only accelerated by hypertension but also contribute to hypertension. Current consensus holds that vascular calcification, either intimal or medial, may directly increase arterial stiffness. Alternatively, arterial stiffness is closely linked to raised blood pressure [29]. Parallelly, the proportion of patients with CACS > 0 and CACS was significantly higher in the stage 3 hypertension group than in other groups in this study. Similar results were seen in the proportion of patients with diabetes, possibly because there is a large overlap in etiology between hypertension and diabetes, the level of hypertension is closely related to the proportion of patients with diabetes [30]. Additionally, consistent with previous reports [10, 17], CACS had a higher negative value for obstructive CAD. The reasonable explanation is that the presence of calcification may affect the accuracy of CCTA in assessing the degree of coronary artery stenosis.
Limitation
Several limitations of the present study should be paid more attention to. Firstly, the present investigation was lack of external validation in an independent cohort, which was planned for subsequent analysis. Secondly, the presence of severe calcification may lead to overestimates stenosis on CCTA. Hence, more than 50% stenosis on CCTA may not represent the accuracy > 50% stenosis evaluated by coronary angiography. Finally, the number of patients with stage 1 and stage 2 hypertension in our cohort was too small to be stratified separately, we will expand the sample size for further research.
Conclusions
The ML model, especially The XGBoost model, incorporating clinical features and CACS may accurately forecast the presence of obstructive CAD on CCTA among patients with hypertension. It may be reasonable for intermediate to high-risk hypertensive patients evaluated by the XGBoost model to directly receive further testing such as CCTA and coronary angiography, as well as preventive therapies.
Data availability
The data are available from the corresponding authors upon reasonable request.
References
Wu CY, Hu HY, Chou YJ, Huang N, Chou YC, Li CP. High Blood Pressure and all-cause and Cardiovascular Disease mortalities in Community-Dwelling older adults. Medicine. 2015;94:e2160. https://doi.org/10.1097/md.0000000000002160.
Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery Disease: results from the prospective multicenter ACCURACY (Assessment by Coronary computed Tomographic Angiography of individuals undergoing invasive coronary angiography) trial. J Am Coll Cardiol. 2008;52:1724–32. https://doi.org/10.1016/j.jacc.2008.07.031.
Miller JM, Rochitte CE, Dewey M, Arbab-Zadeh A, Niinuma H, Gottlieb I, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008;359:2324–36. https://doi.org/10.1056/NEJMoa0806576.
Chinnaiyan KM, Peyser P, Goraya T, Ananthasubramaniam K, Gallagher M, Depetris A, et al. Impact of a continuous quality improvement initiative on appropriate use of coronary computed tomography angiography. Results from a multicenter, statewide registry, the Advanced Cardiovascular Imaging Consortium. J Am Coll Cardiol. 2012;60:1185–91. https://doi.org/10.1016/j.jacc.2012.06.008.
Greenland P, Blaha MJ, Budoff MJ, Erbel R, Watson KE. Coronary calcium score and Cardiovascular Risk. J Am Coll Cardiol. 2018;72:434–47. https://doi.org/10.1016/j.jacc.2018.05.027.
Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358:1336–45. https://doi.org/10.1056/NEJMoa072100.
Okwuosa TM, Mallikethi-Reddy S, Jones DM. Strategies for treating lipids for prevention: risk stratification models with and without imaging. Best practice. Res Clin Endocrinol Metabolism. 2014;28:295–307. https://doi.org/10.1016/j.beem.2014.01.004.
Cho I, Chang HJ, ÓH B, Shin S, Sung JM, Lin FY, et al. Incremental prognostic utility of coronary CT angiography for asymptomatic patients based upon extent and severity of coronary artery calcium: results from the COronary CT angiography EvaluatioN for clinical outcomes InteRnational Multicenter (CONFIRM) study. Eur Heart J. 2015;36:501–8. https://doi.org/10.1093/eurheartj/ehu358.
Lin FY, Shaw LJ, Dunning AM, Labounty TM, Choi JH, Weinsaft JW, et al. Mortality risk in symptomatic patients with nonobstructive coronary artery Disease: a prospective 2-center study of 2,583 patients undergoing 64-detector row coronary computed tomographic angiography. J Am Coll Cardiol. 2011;58:510–9. https://doi.org/10.1016/j.jacc.2010.11.078.
Budoff MJ, Diamond GA, Raggi P, Arad Y, Guerci AD, Callister TQ et al. Continuous probabilistic prediction of angiographically significant coronary artery Disease using electron beam tomography. Circulation.(2002) 105:1791–6. https://doi.org/10.1161/01.cir.0000014483.43921.8c.
Shemesh J, Morag-Koren N, Goldbourt U, Grossman E, Tenenbaum A, Fisman EZ, et al. Coronary calcium by spiral computed tomography predicts cardiovascular events in high-risk hypertensive patients. J Hypertens. 2004;22:605–10. https://doi.org/10.1097/00004872-200403000-00024.
Kalra SS, Shanahan CM. Vascular calcification and hypertension: cause and effect. Annals of medicine.(2012) 44 Suppl 1:S85-92. https://doi.org/10.3109/07853890.2012.660498.
Singal AG, Mukherjee A, Elmunzer BJ, Higgins PD, Lok AS, Zhu J, et al. Machine learning algorithms outperform conventional regression models in predicting development of hepatocellular carcinoma. Am J Gastroenterol. 2013;108:1723–30. https://doi.org/10.1038/ajg.2013.332.
Wu Y, Rao K, Liu J, Han C, Gong L, Chong Y, et al. Machine learning algorithms for the prediction of Central Lymph Node Metastasis in patients with papillary thyroid Cancer. Front Endocrinol. 2020;11:577537. https://doi.org/10.3389/fendo.2020.577537.
Lai R, Ju J, Lin Q, Xu H. Coronary artery calcification under statin therapy and its Effect on Cardiovascular outcomes: a systematic review and Meta-analysis. Front Cardiovasc Med. 2020;7:600497. https://doi.org/10.3389/fcvm.2020.600497.
Han L, Yuan Y, Zheng S, Yang Y, Li J, Edgerton ME, et al. The Pan-cancer analysis of pseudogene expression reveals biologically and clinically relevant tumour subtypes. Nat Commun. 2014;5:3963. https://doi.org/10.1038/ncomms4963.
Al’Aref SJ, Maliakal G, Singh G, van Rosendael AR, Ma X, Xu Z et al. Machine learning of clinical variables and coronary artery calcium scoring for the prediction of obstructive coronary artery disease on coronary computed tomography angiography: analysis from the CONFIRM registry. European heart journal.(2020) 41:359 – 67. https://doi.org/10.1093/eurheartj/ehz565.
Isma’eel HA, Serhan M, Sakr GE, Lamaa N, Garabedian T, Elhajj I, et al. Diamond-Forrester and Morise risk models perform poorly in predicting obstructive coronary Disease in Middle Eastern Cohort. Int J Cardiol. 2016;203:803–5. https://doi.org/10.1016/j.ijcard.2015.11.011.
Baskaran L, Danad I, Gransar H, Schulman-Marcus BÓH, Lin J et al. FY, A Comparison of the Updated Diamond-Forrester, CAD Consortium, and CONFIRM History-Based Risk Scores for Predicting Obstructive Coronary Artery Disease in Patients With Stable Chest Pain: The SCOT-HEART Coronary CTA Cohort. JACC Cardiovascular imaging.(2019) 12:1392 – 400. https://doi.org/10.1016/j.jcmg.2018.02.020.
Zhou J, Liu Y, Huang L, Tan Y, Li X, Zhang H et al. Validation and comparison of four models to calculate pretest probability of obstructive coronary artery disease in a Chinese population: A coronary computed tomographic angiography study. Journal of cardiovascular computed tomography.(2017) 11:317 – 23. https://doi.org/10.1016/j.jcct.2017.05.004.
He T, Liu X, Xu N, Li Y, Wu Q, Liu M et al. Diagnostic models of the pre-test probability of stable coronary artery disease: A systematic review. Clinics (Sao Paulo, Brazil).(2017) 72:188 – 96. https://doi.org/10.6061/clinics/2017(03)10.
Motwani M, Dey D, Berman DS, Germano G, Achenbach S, Al-Mallah MH et al. Machine learning for prediction of all-cause mortality in patients with suspected coronary artery Disease: a 5-year multicentre prospective registry analysis. European heart journal.(2017) 38:500–7. https://doi.org/10.1093/eurheartj/ehw188.
Coenen A, Kim YH, Kruk M, Tesche C, De Geer J, Kurata A et al. Diagnostic Accuracy of a Machine-Learning Approach to Coronary Computed Tomographic Angiography-Based Fractional Flow Reserve: Result From the MACHINE Consortium. Circulation Cardiovascular imaging.(2018) 11:e007217. https://doi.org/10.1161/circimaging.117.007217.
Kalscheur MM, Kipp RT, Tattersall MC, Mei C, Buhr KA, DeMets DL et al. Machine Learning Algorithm Predicts Cardiac Resynchronization Therapy Outcomes: Lessons From the COMPANION Trial. Circulation Arrhythmia and electrophysiology.(2018) 11:e005499. https://doi.org/10.1161/circep.117.005499.
Nakanishi R, Slomka PJ, Rios R, Betancur J, Blaha MJ, Nasir K et al. Machine Learning Adds to Clinical and CAC Assessments in Predicting 10-Year CHD and CVD Deaths. JACC Cardiovascular imaging.(2021) 14:615 – 25. https://doi.org/10.1016/j.jcmg.2020.08.024.
Genders TS, Steyerberg EW, Hunink MG, Nieman K, Galema TW, Mollet NR et al. Prediction model to estimate presence of coronary artery disease: retrospective pooled analysis of existing cohorts. BMJ (Clinical research ed).(2012) 344:e3485. https://doi.org/10.1136/bmj.e3485.
Erbel R, Lehmann N, Möhlenkamp S, Churzidse S, Bauer M, Kälsch H et al. Subclinical coronary atherosclerosis predicts cardiovascular risk in different stages of hypertension: result of the Heinz Nixdorf Recall Study. Hypertension (Dallas, Tex: 1979).(2012) 59:44–53. https://doi.org/10.1161/hypertensionaha.111.180489.
Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation.(2018) 137:e67-e492. https://doi.org/10.1161/cir.0000000000000558.
Mackey RH, Venkitachalam L, Sutton-Tyrrell K. Calcifications, arterial stiffness and atherosclerosis. Advances in cardiology.(2007) 44:234 – 44. https://doi.org/10.1159/000096744.
Lee SW, Kim HC, Lee JM, Yun YM, Lee JY, Suh I. Association between changes in systolic blood pressure and incident Diabetes in a community-based cohort study in Korea. Hypertens Research: Official J Japanese Soc Hypertens. 2017;40:710–6. https://doi.org/10.1038/hr.2017.21.
Acknowledgements
All authors would like to thank the assistance from Yidu Cloud Technology Co., Ltd in data searching, extraction, and processing.
Funding
None.
Author information
Authors and Affiliations
Contributions
Mingxian Wang: Conceptualization, Methodology, Software, Supervision. Mengting Sun: Writing- Conceptualization, Methodology, Formal analysis, Writing-Original draft preparation, Writing- Reviewing and Editing; Yao Yu: Conceptualization, Methodology, and Writing-Original draft preparation; Xinsheng Li: Formal analysis and Visualization; Yongkui Ren: Conceptualization, Methodology, Software, Data curation, and Funding acquisition; Da Yin: Conceptualization, Formal analysis and Writing - Review & Editing;
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2000. This study was approved by the Ethics Committee Board of the First Affiliated Hospital of Dalian Medical University. All participants gave their written informed consent.
Consent for publication
Not applicable.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Table 1
Pre-implant clinical features included in the analysis. Supplementary Table 2 Baseline characteristics for training and validation sets
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, M., Sun, M., Yu, Y. et al. Predictive value of machine learning algorithm of coronary artery calcium score and clinical factors for obstructive coronary artery disease in hypertensive patients. BMC Med Inform Decis Mak 23, 244 (2023). https://doi.org/10.1186/s12911-023-02352-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12911-023-02352-8