
Abstract
Background
Data harmonisation (DH) has emerged amongst health managers, information technology specialists and researchers as an important intervention for routine health information systems (RHISs). It is important to understand what DH is, how it is defined and conceptualised, and how it can lead to better health management decision-making. This scoping review identifies a range of definitions for DH, its characteristics (in terms of key components and processes), and common explanations of the relationship between DH and health management decision-making.
Methods
This scoping review identified relevant studies from 2000 onwards (date filter), written in English and published in PubMed, Web of Science and CINAHL. Two reviewers independently screened records for potential inclusion for the abstract and full-text screening stages. One reviewer did the data extraction, analysis and synthesis, with built-in reliability checks from the rest of the team. We developed a narrative synthesis of definitions and explanations of the relationship between DH and health management decision-making.
Results
We sampled 61 of 181 included to synthesis definitions and concepts of DH in detail. We identified six common terms for data harmonisation: record linkage, data linkage, data warehousing, data sharing, data interoperability and health information exchange. We also identified nine key components of data harmonisation: DH involves (a) a process of multiple steps; (b) integrating, harmonising and bringing together different databases (c) two or more databases; (d) electronic data; (e) pooling data using unique patient identifiers; and (f) different types of data; (g) data found within and across different departments and institutions at facility, district, regional and national levels; (h) different types of technical activities; (i) has a specific scope. The relationship between DH and health management decision-making is not well-described in the literature. Several studies mentioned health providers’ concerns about data completeness, data quality, terminology and coding of data elements as barriers to data utilisation for clinical decision-making.
Conclusion
To our knowledge, this scoping review was the first to synthesise definitions and concepts of DH and address the causal relationship between DH and health management decision-making. Future research is required to assess the effectiveness of data harmonisation on health management decision-making.
Similar content being viewed by others


Background
Data harmonisation (DH) in healthcare is a digital, technology-based innovation that can potentially help routine health information systems (RHISs) function at their best. It can help organise and integrate large databases containing routine health information [1]. Designing, developing and implementing DH interventions has the potential to strengthen aspects of the health system, by enhancing RHISs to high-quality and relevant information that can support decisions, actions and changes across all components and levels of the health system [2, 3]. When RHISs are functioning properly, they can help health practitioners and managers identify and close gaps in health service delivery as well as inform their planning, implementation and monitoring of interventions [4, 5]. They can also help deal address problems related to using different variables and indicators for collecting, analysing and reporting health information across programmes [6], which is common in low-and-middle-income (LMIC) settings. Other challenges to effective RHIS functioning include the production of poor-quality data that cannot easily be exchanged and programmatic fragmentation across levels of the health system, which can result in the duplication and excessive production of data [7].
Lack of standardised data production processes, fragmentation of databases, and errors and duplication in data production are only some of the challenges of RHISs, which may, at first glance be categorised as technical challenges [3, 8]. Solutions to such apparently technical challenges include introducing new data forms, setting up warning systems to detect potential errors, and developing algorithms for integrating different databases.
However, DH interventions for RHISs may not be used effectively if data production and utilisation processes are viewed as merely technical. Given that RHISs are embedded in complex health systems, DH interventions to improve RHIS functions are also influenced by the broader setting, in which dynamic and complex social and technical factors interact [9,10,11]. There is a need to consider the influence of social factors as well. These may include people’s competencies in dealing with new data production processes, institutional values about data utilisation, and existing relationships between data producers and decision-makers [8, 12, 13].
There is growing recognition that the development and implementation of DH interventions occurs in multiple technical and social contexts, and that DH interventions may differ in definition, purpose and intended outcomes [14]. So, various terms are used for interventions with similar aims and activities to data harmonisation. For example, terms such as record linkage, data warehousing, data sharing and health information exchange are all used to describe data harmonisation-type activities [15,16,17]; and it is not always clear to which extent these efforts are similar in practice, scope and relevance. The use of multiple terms may not be a problem in itself, but a common understanding of the components and processes will bring more clarity about what constitutes ‘data harmonisation’, and will make it easier to compare and appraise the relevance and usefulness of DH interventions across settings.
Although DH has the potential to enhance RHISs, it is still unclear whether or how it affects health management decision-making. In some cases, DH interventions may not directly impact on improved management decision-making, especially when interventions are more focused on the technical aspects of data production and less on the organisational and behavioural aspects of data use for decision-making [18]. The scope of this review is to therefore understand the different ways in which DH is defined, to identify its components and processes, and to describe whether or how DH can affect health management decision-making. Greater clarity about the range of definitions, components and processes of DH interventions, and its intended outcomes can help to better evaluate its relevance, usefulness, and impact [12].
Methods
This scoping review was conducted according to the methods outlined by Arksey and O’Malley [19]. They recommend a process that is “not linear but, requiring researchers to engage with each stage in a reflexive way” to achieve both ‘in-depth and broad’ results. This review followed the standard steps for systematic reviews: identifying the research question, identifying relevant studies, selecting studies for inclusion, data extraction and data synthesis. These are detailed in our published study protocol [20].
Study objectives
This scoping review appraised the definitions, components and processes of data harmonisation activities, and provided a broad explanation of the relationship between data harmonisation interventions and health management decision-making. The specific objectives are:
-
1.
To identify and synthesise the various definitions, components and processes of data harmonisation in healthcare; and
-
2.
To describe the relationship between data harmonisation interventions and health management decision-making.
We took a stepped approach in addressing these objectives. All included studies were used to address Objective 1. To address Objective 2, we sampled studies that were using alternative terms for DH interventions and used those to identify, synthesise and compare similarities and differences in definitions. While executing Objective 1 and 2, we identified a smaller number of studies that contributed to Objective 3.
Identifying relevant studies
Eligibility criteria
Peer-reviewed studies and grey literature were considered eligible for inclusion into the scoping review if they provided a definition or description of DH, and or, a more detailed conceptual explanation (in the form of a model, framework or process) of a DH intervention. Additionally, studies were eligible if they provided an explanation of the causal relationship between DH and health management decision-making (such as through improved quality and accessibility of harmonised information for management and/or the utilisation of harmonised health information for management decision-making). We considered any studies concerned with different technical activities of DH (such as linking, merging, cleaning and transferring). After screening, only studies for which we could access full-text articles were eligible for inclusion in the review.
Search strategy
A systematic literature search was conducted in PubMed, CINAHL and Web of Science for eligible studies from 1 January 2000 to 30 September 2018. We limited our search to the year 2000 as digital technology-based innovations began during this period (such as health information exchange) began in high-income countries (predominantly in the United States of America) and when researchers and health system managers in LMICs became interested in the integration of large digital databases [21]. We present the search strategy in the study protocol [20]. Based on preliminary searches we anticipated that these databases would yield the highest results. The search strategies include a combination of keywords and Medical Subject Headings (MeSH) terms related to data harmonisation (concept A) and health information system (concept B). There were no geographic restrictions, but for logistical reasons of time and resources, we only searched for English studies.
Selecting studies for inclusion
Screening records
The first reviewer (BS) conducted all the searches with the help of a librarian and collated the records in the EndNote reference management programme where duplicates were removed. Two reviewers (BS) and second reviewer (AH) then independently screened the records (titles and abstracts) to assess eligibility for full-text review. BS and AH resolved conflicts that emerged at this stage by talking through the inclusion criteria and arriving at a joint decision.
The full-texts of potentially eligible studies were retrieved and assessed by the two reviewers (BS and AH). Final inclusion into the review was based on whether at a minimum the study had a definition or description of a DH intervention or referred to its relationship with health management decision-making. The first reviewer read all full-texts and the second reviewer only read a sample (roughly a third) of the full-texts to verify the first reviewer’s decision about inclusion. BS and AH disagreed on four studies, and after discussion, agreed to exclude the studies.
After finalising screening, the two reviewers then mapped out the characteristics of included studies in an Excel spreadsheet. They recorded the name of the first author, the date, the type of study (primary, review, conceptual, commentary), the term used for the intervention they described (DH or alternative), the country in which the study was taking place, level at which the intervention was implemented (frontline, management, research), and ticked whether there was a conceptual model, framework, diagram or process description of DH and health management decision-making. This detailed mapping of study characteristics was useful for informing sampling options for Objectives 2 and 3.
Sampling of studies
A scoping review aims to map the literature on a particular topic rather than to provide an exhaustive explanation of a particular phenomenon of interest [19, 22]. Thus, the number of included studies was expected to be high in the scoping reviews. To manage the high numbers for a scoping review such as this one (where the aim was to provide definitions and concepts) it was necessary to make use of a qualitative sampling approach. A qualitative sampling approach for this review aimed for variation and depth rather than an exhaustive sample; reviewing too large a number of studies can impair the quality of the analysis and synthesis [23]. We used two types of purposive sampling techniques called maximum variation sampling and theoretical sampling [24]. These techniques were used to identify both the range, variation and similarities or differences in definitions and concepts and intervention descriptions (as per Objective 2) and to provide a rich synthesis of explanations of causal relationships between DH and health management decision-making (as per Objective 3). For Objective 1, we did not apply a sampling strategy. Thus, we included all the studies that at a minimum provided a definition or description of a DH intervention.
Data extraction
BS extracted data for Objective 1 from all the included studies (n = 181). AH independently extracted data from 81 (45%) of included studies to verify data extraction done by the first reviewer. We used an MS Excel spreadsheet for data extraction as presented in Fig. 1. AH and BS extracted a few studies before clarifying the items in the spreadsheet. Once data extraction was complete, the reviewers were able to filter according to the individual items extracted to synthesise and compare studies. Given the objectives of the scoping review, we did not extract any information relevant for conducting risk of bias or quality assessment. Not conducting risk of bias or quality assessment is consistent with scoping reviews of similar aims and methodological approaches [19, 22, 25].

Extract of the Excel data extraction form
Data synthesis: collating, summarising and reporting findings
The first reviewer (BS) conducted data analysis using manual coding and the filter option in MS Excel. Another reviewer (NL) reviewed the data analysis work on an ongoing basis as an additional quality check. For Objective 1, we conducted a numerical analysis to provide an overview of the characteristics of all the included studies. For Objective 2, we conducted a qualitative analysis to provide a narrative synthesis of the different DH definitions and concepts, and to identify different components or activities that are considered part of the DH processes. For Objective 3, we reviewed data related to intentions, suggestions and or explanations of how DH may lead to improved health management decision-making. We extracted and analysed data relevant to Objective 2 and 3 at the same time. We first created a list of all the different terms used to describe DH interventions and then compared definitions across alternative terms by looking for similarities or differences in the definitions or descriptions of DH interventions. We then coded key components, processes and outcomes of DH interventions and the factors reported as important in the relationship between DH and health management decision-making.
The findings are structured according to three themes matching the three study objectives: an overview of the key characteristics of included studies, alternative terms and definitions of DH, and a narrative synthesis of the relationship between DH and health management decision-making.
Reflexivity
Throughout the review, the authors were aware of their own positions and reflected on how these could influence the study design, search strategy, inclusion decisions, data extraction, analysis, and synthesis, and interpretation of the findings [23]. The review authors are trained in anthropology, epidemiology, health systems, and evidence synthesis research. The first author was involved in participant observation of an innovative DH project in the Western Cape Department of Health in South Africa as part of her doctoral research where she grappled with questions that informed the objectives of this review. Three of the authors (BS, AH and NL) were involved in a Cochrane systematic review on RHIS interventions when this scoping review was conceptualised, so they were familiar with some of the health information literature (HIS) literature and had some appreciation for the conceptual and methodological complexities of studying the field of health information management. This experience informed the way the first author developed the search strategy. She used an iterative approach to narrow down the search as much as possible because of her prior knowledge that it was difficult to balance sensitivity and specificity when developing a search strategy for HIS literature that is often multi-disciplinary in nature.
Results
Results of the search
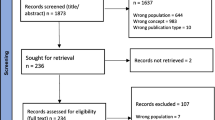
Figure 2 shows a PRISMA diagram of the search results. We screened a total of 1331 records;1232 titles and abstracts identified from searching three electronic databases, and 99 from screening for a Cochrane systematic review assessing the effectiveness of RHIS interventions on health systems management [26] and grey literature. Almost a quarter (289 of 1331) were deemed potentially eligible for full-text screening. We accessed full-texts for 275 studies and of those, 181 were included in the scoping review for Objective 1. We excluded 94 full-text articles because they did not meet the minimum criteria; that is, provide a definition or description of a DH intervention or activity. We sampled 61 studies from the 181 for Objective 2 and 3. We arrived at 61 studies by including all reviews (systematic or literature reviews) and all studies (irrespective of the type of study), that also had a process description, conceptual framework or theory of a DH intervention (that is, in addition to the minimum criteria for Objective 1).

PRISMA diagram of eligible studies
An overview of key characteristics of data harmonisation studies
A total of 181 studies were included into this scoping review for Objective 1 (see Table 1). Given the high number of included studies, we decided to only map the following key characteristics of those studies: first author, date, type of study, intervention term (DH or alternative), country and level of the health care system. Most included studies (126 of 181) were primary studies assessing various aspects of developing and implementing DH interventions (quantitative studies n = 86) or patient, providers or stakeholders’ perspectives (qualitative studies n = 34) or a combination of both (mixed methods studies n = 6).
Of the 181 included studies, 9 were not country specific (these were global reviews), 151 were from the USA and the rest were from other countries (specifically Australia, Brazil, Canada, China, Finland, Germany, Israel, Japan, Jordan, Korea, Malaysia, Netherlands, South Africa and South Korea). In terms of the level of the health care system, 128 studies were on a DH intervention or activity that was concerned with the frontline level (health service providers), 48 studies were concerned with health system factors or policy-related activities at the managerial level, and 5 studies focused on DH interventions specifically for research purposes. Most studies (92%) used the term health information exchange (HIE), while the remaining studies (8%) used a variety of terms to describe various DH interventions and activities, specifically, record linkage, data mining, data linkage, data warehousing, data sharing and data harmonisation.
Definitions, components and processes of data harmonisation
We first discuss the alternative terms and definitions of DH and then we summarise key components and processes of DH using studies sampled from the 61 studies identified for Objective 2 and 3. Table 2 presents identifying details of the 61 studies; that is, the type of study design, the intervention terms, the country, the level of the health care system and the purpose of the study (see Table 2). These studies were concerned with the challenges and opportunities of DH, the barriers and facilitators of DH, the various factors affecting DH (such as technical and financial factors), the outcomes of DH (such as patient safety and quality of care), and privacy and security issues of patient information.
Alternative terms and definitions of data harmonisation
For Objective 2 (a), we describe alternative terms and definitions of DH. We sampled 21 studies from the 61 studies identified for Objective 2 and 3. The alternative terms and definitions are summarised in Table 3. During data analysis we realised that most studies (53 of 61) used term ‘health information exchange’, with similar definitions. We sample 13 of the 53 studies to contribute to the composite HIE definition in the table. These 13 studies were chosen to represent the term HIE because they were review studies and we assumed that reviews provided synthesised definitions of interventions. Using maximum variation sampling, we included 8 more studies (21 studies in total), because they provided a range of different terms for DH activities, besides the term HIE.
There is overlap between the terms and definitions. Definitions for data harmonisation, record linkage and data warehousing explicitly state that these interventions involve a process of having to integrate different or ‘homogeneous’ databases or information systems. Data linkage and record linkage both focus on ‘linkage’ as a core activity in combining different databases using a unique patient identifier. HIE is described as a key outcome of data interoperability, that is, where the focus is on technical linkage of different electronic data bases. Data sharing, where the focus is on data accessibility and use, is described as a key outcome of HIE.
Based on the literature, we identified elements found in the various definitions of data harmonisation. DH is considered a multi-step process with a range of activities (such as identifying, reviewing, matching, redefining and standardising information). Data harmonisation interventions rely on interoperability between databases and systems which means copying standardised patient-level data into a separate repository. Data linkage and record linkage are activities of a broader intervention (data harmonisation), using mechanisms (such as unique patient identifiers) for integrating large datasets. Data warehousing is concerned with extracting, transforming and loading large datasets using information technology (IT) platforms, application systems and data displays (data marts or data dashboards). Data sharing (through the accessing and exchanging electronic health information), can be considered an outcome of HIE interventions. The aim of these interventions is to integrate and make data accessible across different platforms (such as clinical and financial systems), and to allow for the sharing of this data across the patient care trajectory. The ultimate aim of DH, it would seem, is to improve patient outcomes, coordination of health services, quality of care and efficiency and facilitate public health interventions.
In reviewing the definitions, we identified nine characteristics of DH. No single study included all these characteristics, and there are no specific factors such as study design, country or level of the health care system associated with the definitions. DH is characterised by the following characteristics:
-
Any type of DH intervention or activity is a process of multiple steps involving both technical and social processes.
-
The goal of a DH intervention or activity is to integrate, harmonise and bring together different electronic databases into useable formats.
-
There are at least two or more databases involved in any DH intervention or activity.
-
A data harmonisation intervention or activity involves electronic data (no reference is made to data found in paper-based sources).
-
Data harmonisation occurs when there is an increasing availability of electronic data that can be pooled together using unique patient identifiers.
-
Different types of data can be linked and shared such as individual patient clinical, pharmacy and laboratory data, health care utilisation and cost data, and personnel-related data.
-
Electronic data required for DH processes can be found within and across different departments and institutions at facility, district, regional and national levels.
-
A data harmonisation process consists of different types of technical activities such as identifying, reviewing, matching, defining, redefining, standardising, merging, linking, merging and formatting data.
-
DH interventions or activities are defined according to a specific scope and purpose such as disease surveillance, monitoring of long-term outcomes, screening for adverse events, geographic area, secondary data use and data display mechanisms (data marts or dashboards).
Components and processes of data harmonisation
To synthesise key components and processes of DH interventions (Objective 2(b)) we sampled 5 from the 61 studies identified for Objective 2 and 3. We selected 5 studies [16, 17, 29,30,31] based on the conceptual descriptions and visual illustrations of their DH interventions (See Table 4).
The conceptual description by [30], comes closest to a comprehensive conceptual model of a DH intervention, illustrating different types of data, different levels of the health care system (e.g. clinics and hospitals), the multiple processes of exchanging data, the multiple directions in exchange of data, and the key role of the unique patient identifier in enabling the DH process [30]. In the next model, Boyd et al. [16] and Santos et al. [31] both lay out the technical processes involved in the linkage process of different databases, but Santos et al. specifically focuses on linking data required for individual patient clinical management into a central repository. Lastly, Elysee et al. [29] and Hu et al. [17] describe DH interventions with different purposes, that is, medication reconciliation and disease outbreak surveillance respectively.
These conceptual models of DH interventions and activities highlight that there are various steps involved in the integration of databases and in the transformation of data into useable formats. Integrating databases means bringing together data of the same individual from within and between different electronic databases, through various activities involving identifying, reviewing, matching, redefining and standardising data [1, 16]. Once data is harmonised, it can be categorised by various criteria of interest, such as geographic area or disease or patient population, and transformed into different formats such as graphs, tables or dashboards to make it easier for users to access and use the information [28]. There may be different ways that the data is harmonised; in some studies, DH is described as a linear and one-directional process, while other studies described it as an iterative and multi-directional process.
The relationship between data harmonisation and health management decision-making
We sampled 9 studies from the 61 studies (identified for Objective 2 and 3) that provide an explanation of the relationship between DH and health management decision-making. These 9 studies were selected because they referred to the intended benefit, or directly referred to the relationship between DH and health management decision-making. We present extracts of explanations of the relationship in Table 5. According to Eylsee et al. [29] (the study providing the most detail), there is a positive relationship between increased availability of electronic data sets and the ability of clinicians to deal with high volumes of data. This necessitates interoperability between electronic databases at different hospitals, to improve timeliness, accuracy, and completeness of information sharing. According to Ji, Boyd, Santos and Hu the main benefit of DH is health management decision-making, including clinical decision-making [16, 17, 30, 31]. Across the studies, there is agreement that DH interventions make it possible for health providers to use data over time and across organisations to support clinical management decision-making. There is acknowledgement that DH interventions were sometimes unable to deal effectively with inconsistencies, incompleteness, and poor quality of data.
From the 9 studies, we identified three types of health management decision-making that DH contributed to. These are:
-
Clinical decision-making for individual patient clinical management or clinical support and quality improvement tools
-
Operational and strategic decision-making for health system managers and policy-makers
-
Population-level decision-making for disease surveillance and outbreak management
The first level involves frontline clinicians being able to access their patients’ medical information and treatment data and timelines (datasets of longitudinal, clinically relevant individual-level data) through DH interventions. In these situations, DH can make it easier for frontline clinicians to develop tools for reminding them about patients’ performance in treatment and care services as well as help them improve the quality of health care services. At the operational and strategic decision-making level, DH interventions have the potential to support high-level health managers in decision-making involving a wide network of stakeholders (consumers, patients and professionals). Lastly, disease surveillance and outbreak management decision-making rely on harmonised data to plan, monitor and evaluate population-level interventions.
Discussion
Synthesis of findings
This scoping review aimed to provide an overview of the key characteristics of DH studies, identify definitions, alternative terms, components, and processes of DH interventions, and provide explanations of the relationship between DH and health management decision-making. Of the 181 studies that at a minimum provided a definition or description of a DH intervention or activity, 86 were primary quantitative studies, 151 were studies conducted in the USA, and 128 were aimed at improving frontline level health services.
A key finding is that ‘Health information exchange’ or HIE, was the term most frequently used in the literature, especially for studies for the USA. Other terms used were data harmonisation, record linkage, data linkage, data warehousing, data sharing, and data interoperability. Terms like data harmonisation and data warehousing seem to describe a more comprehensive approach to DH interventions (involving both data production and data utilisation aspects), whereas terms like record and data linkage described specific activities within health information exchange. The term data interoperability focuses on the technical aspects that allows for different electronic databases to be linked and for data to be integrated, which allows for synthesis and analysis of health information. Even though different studies used different terms, there was consensus that DH is a useful tool for health management decision making and can support improvements in patient and health system outcomes.
We identified nine characteristics of DH interventions and activities. Using these nine characteristics, DH can be summarised as a process that aims to integrate two or more electronic databases, it involves different types of data captured within and across various institutions at different health care system levels, and varying activities are required to pool together data using unique patient identifiers for the purpose of providing information support for health management decision-making. The review identified three types of health management decision-making that DH contributed to: (a) clinical decision-making for individual patient management, clinical support and quality improvement tools; (b) operational and strategic decision-making for health system managers and policy-makers; and (c) population-level decision-making for disease surveillance and outbreak management.
Drawing on the definitions and the conceptual models of DH identified in this review, we developed a concept map (see Fig. 3) to explain how different aspects of DH interventions and activities work together to support health management decision-making. The concept map consists of different types of databases (1 to 5) containing different types of data such as demographic, clinical, pharmacy, laboratory, administrative and financial, and terminology data. A technical process involving different types of activities (such as matching, merging and linking) takes place to integrate the different types of data using a unique patient identifier. The central repository, where the data is harmonised, is defined according to specific criteria such as a geographic area or disease outcomes. The data kept in the repository should be accessible to data users, who can then use this harmonised data as an information and analytic tool to support health management decision-making for clinical, operational, strategic, and or population-level decision-making.

A concept map of data harmonisation and its relationship to health management decision-making
Study limitations
There are two main differences between the published protocol and this scoping review. We did not search the Global Health database as planned; we realised late that none of the reviewers had permissions to access the database and gaining access was not affordable. We did however manage to search at least three electronic databases, as is the convention in reviews [23]. Due to the large volume of studies included for full-text screening, it was not feasible to conduct the full text screening in duplicate as planned. The first reviewer (BS) assessed all full-texts and then the second reviewer (AH) verified the decisions of the first reviewer in a third of the included studies, which allowed for additional quality checks.
There are two main limitations of the review. Firstly, we restricted our literature search to English. We did not have the resources required for reviewing non-English studies. Most studies identified were from the USA, but it is possible that studies from other non-English speaking, high-income countries with extensive electronic health systems (such as France) may have been missed. Secondly, although sampling aimed to identify variety, comprehensiveness and meaningfulness of the definitions and explanations, there is a possibility that due to sampling, we may have missed relevant studies for Objectives 2 and 3.
Implications for research and practice
There is a need to understand what DH interventions and activities are comprised of in diverse settings and contexts, especially in LMICs. There were fewer studies from LMICs, which may be due to a lower prevalence of electronic health information systems in those settings. Nevertheless, DH interventions hold promise for improving the informational support in LMICs; studies in these contexts could usefully expand the evidence base.
The review highlights the importance of providing detailed descriptions of DH interventions, to allow for better comparisons and to improve the transferability of study results. Additionally, many resources are spent on the technical development of DH projects, with the implicit assumption that this will provide the informational and analytic support for health management decision-making, but this assumption is seldom tested in the research. There is a need for qualitative research on the health system factors of implementing DH and for formative work to inform design of DH interventions. Finally, primary research and evidence synthesis of the experiences of key stakeholders involved (implementers and users of harmonised data) would improve our understanding of the causal mechanisms between data harmonisation and health systems strengthening.
Conclusion
The review aimed to widen our understanding about the range of definitions, components and processes of DH interventions, and how it can contribute to health management decision-making. Most studies of DH interventions and activities were conducted in high-income settings and used the term ‘health information exchange’. The review described the processes, technical activities, types of data, mechanisms for integrating data, and purpose of the DH interventions. DH interventions contributed to three types of health management decision-making, that is, clinical decision-making, operational and strategic decision-making, and population-level surveillance decision-making. We provided a concept map of the components of DH and make recommendations for future research.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- DH:
-
Data harmonisation
- RHISs:
-
Routine health information systems
- LMICs:
-
Low- and middle-income countries
- MeSH:
-
Medical Subject Headings
- HIS:
-
Health information system
- IT:
-
Information technology
- HIE:
-
Health information exchange
References
Liu D, et al. Harmonization of health data at national level: a pilot study in China. Int J Med Inform. 2010;79(6):450 https://doi.org/10.1016/j.ijmedinf.2010.03.002.
Nutley T, Reynolds H. Improving the use of health data for health system strengthening. Glob Health Action. 2013;6(1):20001 https://doi.org/10.3402/gha.v6i0.20001.
Lippeveld T. Routine health information systems: the glue of a unified health system. In: Keynote address at the Workshop on Issues and Innovation in Routine Health Information in Developing Countries. Potomac; 2001.
World Health Organization. Everybody's business-strengthening health systems to improve health outcomes: WHO's framework for action; 2007. Retrieved from https://www.who.int/healthsystems/strategy/everybodys_business.pdf?ua=1.
World Health Organization. Country health information systems assessments: overview and lessons learnt. 2012.
Heywood A, Boone D. Guidelines for data management standards in routine health information systems. Measure Evaluation. 2015; Retrieved from https://www.measureevaluation.org/resources/publications/ms-15-99.
Karuri J, et al. DHIS2: the tool to improve health data demand and use in Kenya. J Health Informatics Dev Countries. 2014;8(1):38 Retrieved from https://jhidc.org/index.php/jhidc/article/view/113.
Harrison MI, et al. Unintended consequences of information technologies in health care—an interactive sociotechnical analysis. J Am Med Inform Assoc. 2007;14(5):542 https://doi.org/10.1197/jamia.M2384.
Olmen JV, et al. The Health System Dynamics Framework: The introduction of an analytical model for health system analysis and its application to two case-studies. Health Culture Soc. 2012;2(1):1 Retrieved from https://hcs.pitt.edu/ojs/index.php/hcs/article/view/71/0.
Sittig DF, Singh H. A new sociotechnical model for studying health information technology in complex adaptive healthcare systems. BMJ Qual Saf. 2010;19(Suppl 3):i68 https://doi.org/10.1136/qshc.2010.042085.
Plsek, P. Complexity and the adoption of innovation in health care. Accelerating Quality Improvement in Health Care: Strategies to Accelerate the Diffusion of Evidence-Based Innovations. National Institute for Healthcare Management Foundation and National Committee for Quality in Health Care. 2003. Retrieved from https://www.nihcm.org/pdf/Plsek.pdf.
Cresswell KM, Sheikh A. Undertaking sociotechnical evaluations of health information technologies. J Innovation Health Informatics. 2014;21(2):78 https://doi.org/10.14236/jhi.v21i2.54.
Cresswell KM, et al. Ten key considerations for the successful optimization of large-scale health information technology. J Am Med Inform Assoc. 2016;24(1):182 https://doi.org/10.1093/jamia/ocw037.
Fichtinger A, et al. Data harmonisation put into practice by the HUMBOLDT project. Int J Spatial Data Infrastructures Res. 2011;6:234 https://doi.org/10.2902/ijsdir.v6i0.191.
Akhlaq A, et al. Barriers and facilitators to health information exchange in low- and middle-income country settings: a systematic review. Health Policy Plan. 2016;31(9):1310 https://doi.org/10.1093/heapol/czw056.
Boyd JH, et al. Technical challenges of providing record linkage services for research. BMC Med Informatics Decision Making. 2014;14(1):23 https://doi.org/10.1186/1472-6947-14-23.
Hu PJ, et al. System for infectious disease information sharing and analysis: design and evaluation. IEEE Trans Inf Technol Biomed. 2007a;11(4):483 https://doi.org/10.1109/titb.2007.893286.
Aqil A, et al. PRISM framework: a paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy Plan. 2009;24(3):217 https://doi.org/10.1093/heapol/czp010.
Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19 https://doi.org/10.1080/1364557032000119616.
Schmidt B-M, et al. Defining and conceptualising data harmonisation: a scoping review protocol. Syst Rev. 2018;7(1):226 https://doi.org/10.1186/s13643-018-0890-7.
Cimino JJ, et al. Consumer-mediated health information exchanges: the 2012 ACMI debate. J Biomed Inform. 2014;48(2014):5 https://doi.org/10.1016/j.jbi.2014.02.009.
Tricco AC, et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med Res Methodol. 2016;16(1):15 https://doi.org/10.1016/j.jbi.2014.02.009.
Cochrane Effective Practice and Organisation of Care (EPOC) Group. EPOC Qualitative Evidence Syntheses: protocol template. 2018. Retrieved from https://epoc.cochrane.org/news/qualitative-evidence-synthesis-template.
Suri H. Purposeful sampling in qualitative research synthesis. Qual Res J. 2011;11(2):63 https://doi.org/10.3316/QRJ1102063.
Popay J, et al. Guidance on the conduct of narrative synthesis in systematic reviews. In: A product from the ESRC methods programme; 2006. https://doi.org/10.13140/2.1.1018.4643.
Leon N, et al. Routine Health Information System (RHIS) interventions to improve health systems management. Cochrane Database Syst Rev. 2015;12(CD012012):1 https://doi.org/10.1002/14651858.CD012012.
Mastebroek M, Naaldenberg J, Lagro-Janssen AL, van Schrojenstein Lantman de Valk H. Health information exchange in general practice care for people with intellectual disabilities: a qualitative review of the literature. Res Dev Disabil. 2014;35(9):1978–87 https://doi.org/10.1016/j.ridd.2014.04.029.
Haarbrandt BE, et al. Automated population of an i2b2 clinical data warehouse from an openEHR-based data repository. J Biomed Inform. 2016;63(2016):277 https://doi.org/10.1016/j.jbi.2016.08.007.
Elysee GJ, et al. An observational study of the relationship between meaningful use-based electronic health information exchange, interoperability, and medication reconciliation capabilities. Medicine (Baltimore). 2017;96(41):e8274 https://doi.org/10.1097/MD.0000000000008274.
Ji H, et al. Technology and policy challenges in the adoption and operation of health information exchange systems. Adv Health Care Manag. 2017;23(4):314 https://doi.org/10.4258/hir.2017.23.4.314.
Santos MR, et al. Health information exchange for continuity of maternal and neonatal care supporting: a proof-of-concept based on ISO standard. Applied Clin Informatics. 2017;8(4):1082 https://doi.org/10.4338/ACI-2017-06-RA-0106.
Downs SM, van Dyck PC, Rinaldo P, McDonald C, Howell RR, Zuckerman A, Downing G. Improving newborn screening laboratory test ordering and result reporting using health information exchange. J Am Med Inform Assoc. 2010;17(1):13–8 https://doi.org/10.1197/jamia.M3295.
Dixon BE, Zafar A, Overhage JM. A Framework for evaluating the costs, effort, and value of nationwide health information exchange. J Am Med Inform Assoc. 2010;17(3):295–301 https://doi.org/10.1136/jamia.2009.000570.
Esmaeilzadeh P, Sambasivan M. Health Information Exchange (HIE): A literature review, assimilation pattern and a proposed classification for a new policy approach. J Biomed Inform. 2016;64:74–86. https://doi.org/10.1016/j.jbi.2016.09.011.
Esmaeilzadeh P, Sambasivan M. Patients’ support for health information exchange: a literature review and classification of key factors. BMC Med Inform Decis Mak. 2017;17:33 https://doi.org/10.1186/s12911-017-0436-2.
Fontaine P, Ross SE, Zink T, Schilling LM. Systematic review of health information exchange in primary care practices. J Am Board Fam Med. 2010;23(5):655–70. https://doi.org/10.3122/jabfm.2010.05.090192.
Grossman JM, Kushner KL, November EA. Creating sustainable local health information exchanges: can barriers to stakeholder participation be overcome? Res Brief. 2008;2:1–12.
Hopf YM, Bond C, Francis J, Haughney J, Helms PJ. Views of healthcare professionals to linkage of routinely collected healthcare data: a systematic literature review. J Am Med Inform Assoc. https://doi.org/10.1136/amiajnl-2012-001575.
Kash BA, Baek J, Davis E, Champagne-Langabeer T, Langabeer JR 2nd. Review of successful hospital readmission reduction strategies and the role of health information exchange. Int J Med Inform. 2017;104:97–104 https://doi.org/10.1016/j.ijmedinf.2017.05.012.
Kuperman GJ, McGowan JJ. Potential unintended consequences of health information exchange. J Gen Intern Med. 2013;28(12):1663–6 https://doi.org/10.1007/s11606-012-2313-0.
Politi L, Codish S, Sagy I, Fink L. Use patterns of health information exchange through a multidimensional lens: conceptual framework and empirical validation. J Biomed Inform. 2014;52:212–21 https://doi.org/10.1016/j.jbi.2014.07.003.
Parker C, Weiner M, Reeves M. Health information exchanges--Unfulfilled promise as a data source for clinical research. Int J Med Inform. 2016;87:1–9 https://doi.org/10.1016/j.ijmedinf.2015.12.005.
Vest JR, Gamm LD. Health information exchange: persistent challenges and new strategies. J Am Med Inform Assoc. 2010;17(3):288–94 https://doi.org/10.1136/jamia.2010.003673.
Rahurkar S, Vest JR, Menachemi N. Despite the spread of health information exchange, there is little evidence of its impact on cost,use, and quality of care. Health Aff. 2015;34(3):477–83 https://doi.org/10.1377/hlthaff.2014.0729.
Rudin RS, Motala A, Goldzweig CL, Shekelle PG. Usage and effect of health information exchange: a systematic review. Ann Intern Med. 2014;161(11):803–11 https://doi.org/10.7326/M14-0877.
Sadoughi F, Nasiri S, Ahmadi H. The impact of health information exchange on healthcare quality and cost-effectiveness: A systematic literature review. Comput Methods Prog Biomed. 2018;161:209–32 https://doi.org/10.1016/j.cmpb.2018.04.023.
Shapiro JS, Kannry J, Lipton M, Goldberg E, Conocenti P, Stuard S, Wyatt BM, Kuperman G. Approaches to Patient Health Information Exchange and Their Impact on Emergency Medicine. Ann Emerg Health. 2006; https://doi.org/10.1016/j.annemergmed.2006.03.032.
Vest JR, Jasperson S. How are health professionals using health information exchange systems? Measuring usage for evaluation and system improvement. J Med Syst. 2012;36(5):3195–204 https://doi.org/10.1007/s10916-011-9810-2.
Vest JR, Abramson E. Organizational Uses of Health Information Exchange to Change Cost and Utilization Outcomes: A Typology from a Multi-Site Qualitative Analysis. AMIA Annu Symp Proc. 2015:1260–8.
Zaidan BB, Haiqi A, Zaidan AA, Abdulnabi M, Mat Kiah ML, Muzamel H. A Security Framework for Nationwide Health Information Exchange based on Telehealth Strategy. J Med Syst. 2015;39(5):235. https://doi.org/10.1007/s10916-015-0235-1.
Acknowledgements
We would like to thank Ms. Gill Morgan, University of Cape Town, who assisted with developing the search strategy.
Funding
Time to write this paper was supported by the US National Institute of Mental Health [grant number 1R01 MH106600] and the South African Medical Research Council (SAMRC). The content of this paper is solely the responsibility of the authors and does not necessarily represent the official views of the US National Institutes of Health or the SAMRC.
Author information
Authors and Affiliations
Contributions
BS was involved in all the tasks of conducting the scoping review. She drafted the manuscript with help from CC and NL. AH contributed to searching, screening and data extraction processes. All authors reviewed and approved the final manuscript before final submission for peer review.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schmidt, BM., Colvin, C.J., Hohlfeld, A. et al. Definitions, components and processes of data harmonisation in healthcare: a scoping review. BMC Med Inform Decis Mak 20, 222 (2020). https://doi.org/10.1186/s12911-020-01218-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12911-020-01218-7