
Abstract
Background
This study aimed to identify the healthcare providers’ experience and perspectives toward end-of-life care decisions focusing on end-of-life discussion and physician’s order of life-sustaining treatment documentation in Korea which are major parts of the Life-Sustaining Treatment Act.
Methods
A cross-sectional survey was conducted using a questionnaire developed by the authors. A total of 474 subjects—94 attending physicians, 87 resident physicians, and 293 nurses—participated in the survey, and the data analysis was performed in terms of frequency, percentage, mean and standard deviation using the SPSS 24.0 program.
Results
Study results showed that respondents were aware of terminal illness and physician’s order of life-sustaining treatment in Korea well enough except for some details. Physicians reported uncertainty in terminal state diagnosis and disease trajectory as the most challenging. Study participants regarded factors (related to relationships and communications) on the healthcare providers’ side as the major impediment to end-of-life discussion. Study respondents suggested that simplification of the process and more staff are required to facilitate end-of-life discussion and documentation.
Conclusion
Based on the study results, adequate education and training for better end-of-life discussion are required for future practice. Also, a simple and clear procedure for completing a physician’s order of life-sustaining treatment in Korea should be prepared and legal and ethical advice would be required. Since the enactment of the Life-Sustaining Treatment Act, several revisions already have been made including disease categories, thus continuous education to update and support clinicians is also called for.
Similar content being viewed by others


Background
With the recent development of novel and innovative medical treatments, life expectancy has been extended and withholding and/or withdrawal of any medical treatment is sometimes considered as failure in Korea [1]. This has caused an increase in aggressive treatment of terminally ill patients [2, 3]. In addition, as in the Boramae Hospital case (a representative case in which discussions on dying with dignity were raised in Korean society in 1997), the Supreme Court applied the physicians with aiding and abetting in a murder if a patient died after being discharged from hospital against medical advice [4]. The aforementioned have led to the some degree the excessive use of life-sustaining treatment (LST) by healthcare providers in Korea for the terminally ill or end-of-life (EOL) patients.
For medical care of terminally ill patients, various decisions are required and discussions about death and dying are inevitable, which used to be regarded as a social and medical taboo in Korea. However, people are aware that death is unavoidable, and they wish to have a meaningful life untill the end and to maintain quality of life even in the EOL period [5]. For EOL care decisions, autonomy manifested by self-determination reflecting people’s values and wishes is critical and people need to talk about death and dying in advance. In the process of EOL discussion, terminally ill patients and relevant stakeholders, usually healthcare providers and family members, share information and thoughts that could lead to an appropriate decision. Nevertheless, until recently, only a small number of patients have been directly involved in EOL discussions [6], despite some studies showing that most patients want to be involved in EOL discussions [7].
As of February 2018, the Act on Hospice and Palliative Care and Decisions on Life-sustaining Treatment for Patients at EOL (the “LST Act”), which advocates for patient autonomy and self-determination, has been enforced [8]. According to this law, a discussion on the end of life, which is usually recommended to be done in advance of end stage of life, is required. This discussion process is called advance care planning (ACP) and legal documentation including advance directives (AD) and physician’s orders for life-sustaining treatment (POLST) is completed as a result of this discussion. However, EOL discussion itself and relevant policies such as AD and POLST are new to healthcare providers in Korea. For that reason, the Ministry of Health and Welfare initiated a pilot project prior to full-scale implementation of LST Act. This paper reported the outcome of that pilot project. This pilot study was conducted focusing on two areas which would support more efficient law enforcement, based on the data drawn from the pilot project: EOL discussion and ACP documentation, especially completion procedures of POLST of Korea (POLST-K).
Methods
Aims
This study was performed to identify healthcare providers’ experiences and perspectives including awareness and opinions related to EOL discussion and POLST-K.
Study design and settings
This cross-sectional study was conducted from October 2017 to January 2018 in seven hospitals, including teaching hospitals and general hospitals that participated in the pilot project promoted by the government across the nation.
Participants
Study participants were physicians and nurses recruited from seven hospitals that agreed to participate in this study. Among the 200 physicians and 300 nurses who agreed to participate, 181 physicians’ and 293 nurses’ surveys were collected (response rate: 90.5% in physicians; 97.7% in nurses). A questionnaire on the experience and perspectives related to EOL care and discussion and POLST-K were administered to potential study respondents who were practicing or witnessing the EOL decision-making process during the pilot project period.
Questionnaires and data collection
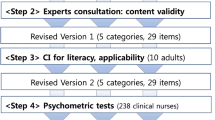
The questionnaire to solicit healthcare providers’ experience and perspectives was developed by the authors through rigorous literature and law analysis and validated by expert consultation. The consultation panel consisted of oncologists, hospice/palliative medicine specialists, internal medicine specialists and clinical nurses. In addition, a pilot study was also carried out with five physicians and five nurses to further refine items of the questionnaire. The final version of the questionnaire consisted of three categories, i.e., (1) participant characteristics, (2) experience and (3) perspectives. For experience, items relating to giving bad news and POLST-K completion were included (3 items). Under the perspective category, five subcategories were included as follows; (1) awareness of terminal illness care and POLST-K (11 items), (2) opinions about the factors that hinder terminal state diagnosis and giving bad news (13 items), (3) opinions about impediments to EOL discussion per stakeholder (13 items), (4) impediments to completion of POLST-K (6 items), and (5) suggestions and/or recommendations for future EOL care decision-making (10 items) respondents (Additional file 1). Due to the differences in the role of physicians and nurses, items on disease diagnosis and POLST were omitted from the survey of nurse respondents (Additional file 2).
The study was approved by the institutional review board (IRB) of Ulsan University Medical Center where the authors were based. The researchers explained the study purpose to the participants, and all data were collected after respondent’s permission was confirmed utilizing a written informed consent form. All participating healthcare providers completed the questionnaire anonymously and voluntarily. The study was carried out in accordance with the 1995 Helsinki Declaration and the ethical standards of National Research Committee. Data collected were handled confidentially in an approved manner.
Statistical analysis
Data were analyzed using SPSS version 25.0 for Windows (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to explore healthcare providers’ experiences and perspectives of the EOL decision-making process according to the study aim.
Results
Participant characteristics
A total of 474 respondents (181 physicians and 293 nurses) participated in this study (Table 1). Of the physicians, 94 were attending physicians, and 87 were first to fourth-year resident physicians. The characteristics of the participants are shown in Table 1. A total of 26.7% of the physicians and 11.7% of the nurses had at least ten years clinical. A total of 58.6% of the physicians were in internal medicine, and 41.4% were from other departments including surgery, radiology, urology, ophthalmology, otolaryngology, etc. The primary disease reported by study participants in relation to patients for whom they had been caring was cancer (64.6% of the physicians and 83.6% of the nurses).
Experience of terminal illness and EOL care
Experience of terminal and EOL care are presented in Table 2 and Fig. 1. About half of the physicians had made a terminal diagnosis in more than two cases per month and 80% of physicians and 70% of nurses reported that they had some experience with POLST-K. Overall satisfaction level about EOL decisions appeared evenly (about 50%) across the subgroups.

Experience in regarding terminal illness and EOL care. A Frequency of patient notification of terminal illness. B Subjects to be first notified of terminal illness. C Subjects in the discussion to complete the POLST form
Fifty-six percent of the physician respondents reported that they either always or mostly talked to patients about terminal state diagnosis (Fig. 1A). Seventy-four percent of the physicians notified the family members first about the patients’ terminal state, and 22.1% notified both the patient and family members at the same time (Fig. 1B). Physicians completed the POLST-K form along with a discussion with patients and family members (64.6%), family members only (27.6%), and patient only (5.5%), respectively. The study found that 29.9% of patients were excluded from the EOL decision-making process according to the physicians’ report (Fig. 1C).
Perspectives on EOL discussion
Awareness of terminal illness and POLST-K
Regarding terminal illness, 50.3% of the physicians and 83.8% of the nurses answered that stage 4 cancer meant terminal illness which is not all ways true. Approximately 30% of the physicians and nurses considered that terminal illnesses can be cured after adequate medical treatment. However, 85.6% of the physicians and 79.5% of the nurses answered that “the survival rate of patients with advanced cancer after cardiopulmonary resuscitation is usually less than 10%.” Almost 95.0% of respondents reported that patients should be notified of a terminal illness. While 18.2% of the physicians and 16.7% of the nurses said that hospice palliative care would mean hopelessness to patients with a terminal illness, 86.7% of the physicians and 97.3% of the nurses considered that hospice palliative care could be more helpful than aggressive treatment (Table 3).
In relation to the contents of POLST-K, the level of awareness about the decision-maker was very low across all respondents, while physicians and nurses all revealed high awareness relating to document updating and/or abolition. Also, the majority of physicians and nurses considered that do not resuscitate (DNR) could replace POLST-K in the future.
Physicians’ opinions on impediments to terminal state diagnosis and giving bad news
Difficulties regarding terminal illness diagnosis and giving bad news to patients are shown in Table 4. Physicians reported that the uncertainty of the disease trajectory (34.1%) and ambiguity of the diagnosis criteria (30.1%) hindered timely diagnosis of a terminal illness. Worries about the patients’ frustration or disappointment (27.9%) and family members’ objection to telling the truth to patients (25.3%) were the main factors that prohibited telling patients about their terminal illness.
From a total of 362 responses relating to impediments to EOL discussions with patients or family members, factors on the physicians’ side were considered the main impediments (75.7%) (Table 5). The top most factor was uncertainty about the appropriate timing of the EOL discussion (26.0%). Family members’ negative attitudes and disagreement among family members about EOL discussion were recognised as major barriers among 13% of physician respondents, while 11.3% of physicians considered patients’ factors as the key barriers to EOL discussion. The main impediment to completing the POLST-K document was the complicated procedures (20.6%) (Table 6).
Suggestion for future EOL discussion and POLST-K
From a list of 10 potential actions to increase EOL discussion and POLST-K completion, over 40% of physicians, considered that simplifying the POLST-K completion process was the highest priority to facilitate EOL discussion and POLST-K documentation, while nurses reported that sufficient staffing would be the biggest barrier. (Table 7). Keywords expressed by physicians related to POLST-K completion and its utility in future are outlined in Fig. 2.

Key words expressed by physicians related by POLST-K documentation
Discussion
It has been years since the LST Act was enacted in 2018, and it is reported that the POLST-K completion rate is continuously increasing and data related to this Act are being presented [9, 10]. However, research conducted on EOL discussion and POLST-K in direct connection with this law is still lacking. Thus we have attempted to present relevant data and opinions for better practice in the future from healthcare providers’ point of view.
In this study, 74.0% of physicians informed the patient’s family about a terminal diagnosis before telling the patient. In EOL discussions, including giving bad news and providing LST options, the social and emotional environments are key factors [11]. Korea is well known to be a family-oriented society, and family members are the main and preferential stakeholders in a conversation about EOL care planning [12] which often leads to patients’ autonomy in the decision-making process on EOL care being overlooked. Nevertheless, the LST Act clearly states that the patient is the one who should participate in the discussion about EOL care decisions, knowing his/her disease state and making their own decisions. Therefore, according to the LST Act, physicians should tell the patient about EOL care options as well as a disease state. However, because of a long-standing cultural tradition of telling families first, some physicians would not find that easy to do; this might explain why 74.0% of physicians told bad news to patients’ families first. Therefore, various communication strategies including education and guidelines are being proposed. Likewise, strategies that reflect Korean culture, law, and clinical environment will be needed to facilitate EOL discussions.
The majority of physicians and nurses appeared to be aware of what is classified as terminal illness, albeit with relatively low levels of awareness in some aspects. To be more specific, most nurses reported that they considered stage 4 cancer as a terminal stage but this is not always the case. This is a surprising finding in that healthcare providers' attitudes toward disease can influence patient care and needs to be corrected.
The majority of study respondents reported that they were familiar with the important contents of POLST-K. However, the level of awareness of the POLST-K completion process and decision-makers was not satisfactory. Since this study is an analysis of data from the pilot project in 2017, we expected that the level of awareness would have increased since the time of data collection. On the contrary, it is reported that the overall awareness of resident physicians has not changed over time even though a majority of resident physicians responded that they were educated about the LST Act [13]. Therefore, more practical strategies are required in terms of education technology and content. For example, education in the clinical setting makes a significant difference to overall awareness about the LST Act [13], and on-site education might be one important option to consider. Education programs are especially helpful when awareness or knowledge issues are more concerned in EOL discussion [14]. In addition to awareness issues, communication about EOL decisions is well known to be challenging to clinicians and simple solutions are unlikely to be effective [15]. Therefore, education or training programs including adequate content and ‘how to’ issues would be necessary.
Physician respondents reported that most of their difficulties in diagnosing terminal illnesses were due to uncertainty of the disease trajectory and the ambiguity of the terminal state’s diagnostic criteria. This result is supported by a systematic review [16] which reported that prognostic uncertainty was a key factor to hinder EOL discussion. For this reason, opinions on terminal state diagnosis vary among physicians [17] and the Korean Academy of Medical Sciences has published consensus guidelines [18]. However, application of the guidelines in actual practice seems still challenging, judging from the results of this study. In fact, disease trajectory itself implies uncertainty, which also needs to be acknowledged. Thus, various aspects such as a patient’s functional status, signs and symptoms, and available laboratory data also should be considered along with disease state [19]. In addition, there are various tools for diagnosing terminal diseases that were constructed using the aforementioned factors. Examples of these tools include the Palliative Prognostic Score [20], Palliative Prognostic Index [21], or Surprise question [22]. These tools were developed more than a decade ago and have been widely promoted; implementation of these tools in clinical practice would help to overcome the ambiguity of diagnosing terminal illnesses.
When the discussion is actually initiated, ACP document completion rate is found to increas [23]. In addition to awareness or knowledge-related factors, each patient's attitude toward EOL care that is influenced by their beliefs and cultural background is important [11] and each patient’s wishes and needs also should be taken into account in the discussion. In addition, the conversation guide for serious illness recommends exploring the patient’s values and discussing goals of care and preferences for life-sustaining interventions before completing the POLST documents [24].
Even after a terminal state is confirmed, informing patients of their condition and initiating discussions on EOL care is a still difficult issue for healthcare providers. Nonetheless, guidelines suggest that a conversation about EOL care decisions should be maintained even after the diagnosis of life-threatening disease in clinical practice [25]. Impediments to informing patients about their terminal state could hinder timely initiation of the EOL discussion and specific barriers were revealed in this study. The top two factors for physicians to be reluctant to give bad news to patients were fear of the patient’s disappointment/frustration and family members’ opposition. However, the LST Act clearly specifys having EOL discussions with patients and ACP documentation rate is found to be increased when the discussion is actually initiated [23]. ACP documents, especially POLST are made through a structured discussion and allow integration of the patient’s values and the physician’s expertise [26] which can promote the patient’s best interest. In addition, when it comes to communication issues, barriers to hinder effective conversation could be overcome with increasing confidence with EOL care conversations by communication skills [27], which also can be improved with appropriate strategies [15].
We identified factors hindering EOL discussions by stakeholder groups of physicians, patients, and families, and most of the factors reported as impediments to EOL discussions turned out to be physician-side factors. Among those, the uncertainty of appropriate EOL discussion timing, concerns about the patient’s disappointment/frustration, and the thought of giving up on the patient’s life were the main barriers reported by the physicians. These impediments are mainly procedure-related and could be solved by education and training including communication skills. Physicians’ education on EOL care was reported to be insufficient, which led to a lack of confidence during EOL discussions with patients and caregivers [28]. When appropriate EOL communication skill training is provided, it can improve EOL discussion and increase the ACP document completion rate as well [29]. Therefore, EOL discussions need to be part of routine medical care for patients with a terminal disease. The Royal College of Physicians in the United Kingdom released the “Talking About Dying” report in 2018, which contains practical advice to physicians on EOL conversations [30]. This type of training and learning materials with clearly defined objectives, a structured curriculum, evaluation methods, and feedback mechanisms would be helpful.
Patient- or family-related factors were much less an issue in end-of-life communication than physician-related factors. Nevertheless, effort to resolve a small portion of these problems can make big difference and ACP, along with shared decision-making (SDM) through family meetings or embedding EOL discussion into everyday practice, would be helpful for patients facing death.
Factors perceived as impediments and suggestions to overcome them in completing POLST-K were consistent as shown in Fig. 2 and Table 6, and they were mainly procedure-related. A domestic study evaluating the feasibility of the POLST-K discussion for patients with terminal cancer reported that only about one-third of the patients had a POLST form completed [31]. Fortunately, recent statistics [9] show that feasibility is improving over time as experience accumulates; however more effort still is needed to facilitate POLST-K preparation through simple and clear procedures.
Based on the results of this study, it is important to elicit the opinions of patients and their families as well to obtain their agreement. In a clinical setting, disagreement among stakeholders including patients, family members and healthcare providers is not unusual. Especially in relation to disagreements between patients and family members, a qualitative study on LST decision-making in Korea proposed ‘a context-oriented model for EOL communication’ [32]. This study suggested that healthcare providers need to identify the decision-making dynamics between the patient and family first, and then determine the patient’s willingness to make decisions independently or jointly with family members (or at least those family members who are willing to participate in decision-making). When the patient or family members accept the terminal state and are ready to participate in the decision-making process, effective EOL discussion and adequate decision-making are more likely [32].
Conclusion
This study explored practical details and suggestions in applying the LST Act focusing on healthcare providers’ experience and perspectives toward EOL discussion. The study results are derived from clinicians directly involved in practice related to the LST Act, thus having important implications for present and future EOL decisions especially related to the LST Act. In conclusion, this study revealed factors that impede the diagnosis of terminal illnesses and EOL discussion. Physician-related factors were the main impediment to the EOL discussion and to overcome these barriers, approaches including on-site education are required. In addition, patient and family knowledge and awareness of related issues must also be improved through appropriate strategies such as social marketing.
This study also had several limitations. First, this study involved only healthcare providers, not patients and their family members. To accurately determine impediments, studies involving patients and family members need to be conducted. Second, this study was conducted just before the implementation of the LST Act, therefore further studies exploring the influence of this Act on EOL discussion are called for.
Availability of data and materials
All data generated and analyzed during this study are included in this published article. Data are available from the corresponding author on reasonable request.
Abbreviations
- ACP:
-
Advance care planning
- AD:
-
Advance directives
- DNR:
-
Do not resuscitate
- EOL:
-
End-of-life
- IRB:
-
Institutional review board
- LST:
-
Life-sustaining treatment
- POLST:
-
Physician’s orders for life-sustaining treatment
- POLST-K:
-
Physician’s orders for life-sustaining treatment of Korea
- SDM:
-
Shared decision-making
References
Kim PM, Oh SM, Park M, Kim YH. The attitude of doctors towards end-of-life care decision makings in Korea: focused on palliative sedation. Korean J Med Ethics. 2016;19(1):60–73. https://doi.org/10.35301/ksme.2016.19.1.60.
Earle CC, Neville BA, Landrum MB, Ayanian JZ, Block SD, Weeks JC. Trends in the aggressiveness of cancer care near the end of life. J Clin Oncol. 2004;22(2):315–21.
Keam B, Oh DY, Lee SH, Kim DW, Kim MR, Im SA, et al. Aggressiveness of cancer-care near the end-of-life in Korea. Jpn J Clin Oncol. 2008;38(5):381–6.
Han SH. Case studies: Withdrawal of life sustaining treatment and distinction between action and inaction in Korean criminal law. Yonsei Law Review. 2005;15(1):249–74.
Mack JW, Cronin A, Keating NL, Taback N, Huskamp HA, Malin JL, et al. Associations between end-of-life discussion characteristics and care received near death: a prospective cohort study. J Clin Oncol. 2012;30(35):4387–95.
Macmillan Cancer Support. Missed opportunities: Advance care planning report. England and Wales, Scotland: Macmillan Cancer Support. 2018 [cited 2019 May 24]. Available from: https://www.macmillan.org.uk/images/missed-opportunities-end-of-life-advance-care-planning_tcm9-326204.pdf.
The Kaiser Family Foundation. View and experiences with end-of-life medical care in Japan, Italy, the United States, and Brazil: a cross-country survey [Internet]. Washington DC: The Kaiser Family Foundation. 2017 [cited 2019 May 19]. Available from: https://www.kff.org/other/report/views-and-experiences-with-end-of-life-medical-care-in-japan-italy-the-united-states-and-brazil-a-cross-country-survey.
Ministry of Health and Welfare. Act on decisions on life-sustaining treatment for patients in hospice and palliative care or at the end of life [Internet]. Sejong; Ministry of Health and Welfare. 2016 [cited 2019 May 07]. Available from: https://law.go.kr/LSW/lsInfoP.do?lsiSeq=180823&viewCls=engLsInfoR&urlMode=engLsInfoR#0000.
National Agency for Management of Life-sustaining Treatment. Monthly report of POLST-K [Internet]. Seoul; National Agency for Management of Life-sustaining Treatment. 2021 [cited 2021 Oct 19]. Available from: https://www.lst.go.kr/comm/monthlyStatistics.do
Ministry of Health and Welfare and National Agency for Management of Life-sustaining Treatment. 2020 Annual Report Book. [Internet]. Seoul; National Agency for Management of Life-sustaining Treatment. 2021 [cited 2021 Oct 19]. Available from: https://www.lst.go.kr/comm/referenceDetail.do?pgNo=&cate=&searchOption=0&searchText=&bno=2115
Johnson S, Butow P, Kerridge I, Tattersall M. Advance care planning for cancer patients: a systematic review of perceptions and experiences of patients, families, and healthcare providers. Psychooncology. 2016;25(4):362–86. https://doi.org/10.1002/pon.3926.
Oh DY, Kim JE, Lee CH, Lim JS, Jung KH, Heo DS, et al. Discrepancies among patients, family members, and physicians in Korea in terms of values regarding the withholding of treatment from patients with terminal malignancies. Cancer. 2004;100(9):1961–6. https://doi.org/10.1002/cncr.20184.
Kim YJ, Lim CM, Shim TS, Hong SB, Huh JW, Oh DK, Koh Y. The influence of new legislation on the withdrawal of life-sustaining treatment on the perceptions and experiences of residents in a tertiary hospital in Korea. Korean J Med Ethics. 2020;23(4):279–99. https://doi.org/10.35301/ksme.2020.23.4.279.
Head BA, Schapmire T, Earnshaw L, Faul A, Hermann C, Jones C, et al. Evaluation of an interdisciplinary curriculum teaching team-based palliative care integration in oncology. J Canc Educ. 2016;31(2):358–65. https://doi.org/10.1007/s13187-015-0799-y.
Brighton LJ, Bristowe K. Communication in palliative care: talking about the end of life, before the end of life. Postgrad Med J. 2016;92(1090):466–70. https://doi.org/10.1136/postgradmedj-2015-133368.
Hancock K, Clayton JM, Parker SM, et al. Truth-telling in discussing prognosis in advanced life-limiting illnesses: a systematic review. Palliat Med. 2007;21:507–17. https://doi.org/10.1177/0269216307080823.
Koh SJ, Kim S, Kim J, Keam B, Heo DS, Lee KH, et al. Experiences and opinions related to end-of-life discussion: from oncologists’ and resident physicians’ perspectives. Cancer Res Treat. 2018;50(2):614–23. https://doi.org/10.4143/crt.2016.446.
Lee SM, Kim SJ, Choi YS, Heo DS, Baik S, Choi BM, et al. Consensus guidelines for the definition of the end stage of disease and last days of life and criteria for medical judgment. J Korean Med Assoc. 2018;61(8):509–21. https://doi.org/10.5124/jkma.2018.61.8.509.
Hauser CA, Stockler MR, Tattersall MH. Prognostic factors in patients with recently diagnosed incurable cancer: a systematic review. Support Care Cancer. 2006;14(10):999–1011. https://doi.org/10.1007/s00520-006-0079-9.
Maltoni M, Caraceni A, Brunelli C, Broeckaert B, Christakis N, Eychmueller S, et al. Prognostic factors in advanced cancer patients: evidence-based clinical recommendations-a study by the Steering Committee of the European Association for Palliative Care. J Clin Oncol. 2005;23(25):6240–8. https://doi.org/10.1200/jco.2005.06.866.
Morita T, Tsunoda J, Inoue S, Chihara S. The palliative prognostic index: a scoring system for survival prediction of terminally ill cancer patients. Support Care Cancer. 1999;7(3):128–33. https://doi.org/10.1007/s005200050242.
Moroni M, Zocchi D, Bolognesi D, Abernethy A, Rondelli R, Savorani G, et al. The “surprise” question in advanced cancer patients: a prospective study among general practitioners. Palliat Med. 2014;28(7):959–64. https://doi.org/10.1177/0269216314526273.
Van Scoy LJ, Reading JM, Hopkins M, Smith B, Dillon J, Green MJ, et al. Community game day: using an end-of-life conversation game to encourage advance care planning. J Pain Symptom Manag. 2017;54(5):680–91. https://doi.org/10.1016/j.jpainsymman.2017.07.034.
Céspedes P, Sánchez-Martínez V, Lera-Calatayud G, Vila-Candel R, Cauli O, Buigues C. Delay in the diagnosis of breast and colorectal cancer in people with severe mental disorders. Cancer Nurs. 2020;43(6):E356–62. https://doi.org/10.1097/NCC.0000000000000727.
Schrijvers D, Cherny NI. ESMO clinical practice guidelines on palliative care: advanced care planning. Ann Oncol. 2014;25(Supp 3):138–42. https://doi.org/10.1093/annonc/mdu241.
Kapp MB. Overcoming legal impediments to physician orders for life-sustaining treatment. A J Ethics. 2016;18(9):861–8. https://doi.org/10.1001/journalofethics.2016.18.09.peer1-1609.
Griffiths J, Wilson C, Ewing G, et al. Improving communication with palliative care cancer patients at home: a pilot study of SAGE & THYME communication skills model. Eur J Oncol Nurs. 2015;19:465–72. https://doi.org/10.1016/j.ejon.2015.02.005.
Schroder C, Heyland D, Jiang X, Rocker G, Dodek P. Educating medical residents in end-of-life care: insights from a multicenter survey. J Palliat Med. 2009;12(5):459–70. https://doi.org/10.1089/jpm.2008.0280.
Brighton LJ, Koffman J, Hawkins A, McDonald C, O’Brien S, Robinson V, et al. A systematic review of end-of-life care communication skills training for generalist palliative care providers: research quality and reporting guidance. J Pain Symptom Manag. 2017;54(3):417–25. https://doi.org/10.1016/j.jpainsymman.2017.04.008.
Royal College of Physicians UK. Talking about dying: How to begin honest conversations about what lies ahead [Internet]. London; Royal College of Physicians. 2018 [cited 2019 May 23]. Available from: https://www.rcplondon.ac.uk/projects/outputs/talking-about-dying-how-begin-honest-conversations-about-what-lies-ahead.
An HJ, Jeon HJ, Chun SH, Jung HA, Ahn HK, Lee KH, et al. Feasibility study of physician orders for life-sustaining treatment for patients with terminal cancer. Cancer Res Treat. 2019;51(4):1632–8. https://doi.org/10.4143/crt.2019.009.
Koh SJ, Kim S, Kim J. Communication for end-of-life care planning among Korean patients with terminal cancer: a context-oriented model. Palliat Support Care. 2016;14(1):69–76. https://doi.org/10.1017/S1478951515000590.
Acknowledgements
We would like to appreciate the research coordinators who supported data collection at the study centers: Chungnam National University Hospital; Jeju National University Hospital; Kangwon National University Hospital; National Health Insurance Service Ilsan Hospital; The Catholic University of Korea, Seoul St. Mary’s Hospital; Ulsan University Hospital; Yeungnam University Hospital. Also, the authors would like to thank the Korea National Institute for Bioethics Policy’s Foundation Promotion Agency for National Agency for Management of Life-Sustaining Treatment in 2017.
Funding
This research was supported by the Korea National Institute for Bioethics Policy’s Foundation Promotion Agency for National Agency for Management of Life-Sustaining Treatment in 2017.
Author information
Authors and Affiliations
Contributions
All authors agree to be accountable for all aspects of this work. HSI, SJK, SK, and IL was involved in the conception and design of the study, the analysis and interpretation of the data, the drafting of the manuscript, critical revision of the intellectual content, and approval of the final manuscript. SJK was involved in the conception and design of the study, was responsible for the acquisition of funding, analysed and interpreted the survey data, drafted the manuscript, revised the manuscript critically with respect to its intellectual content, and approved the final manuscript. SK and IL contributed to survey preparation and data collection, analysed and interpreted the data, cowrote the original draft of the manuscript, critically revised the manuscript, and approved the final manuscript. JHK, JSL, JYM, BKP, KHL, MAL, SH, YH, HK, and JC were performend the investigation and drafted the manuscript. All authors read and approved the final manuscript.
Author’s information
HIS, JSL, JHK, HK, and SJK work at Department of Internal Medicine, Ulsan University Hospital, Ulsan University College of Medicine, Ulsan, Korea. IL and SK work at Department of Nursing, Changwon National University, Changwon, Korea. JYM work at Department of Internal Medicine, Chungnam National University Sejong Hospital, Chungnam National University College of Medicine, Daejeon, Korea. BKP work at Department of Internal Medicine, National Health Insurance Service Ilsan Hospital, Goyang, Korea. KHL work at Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea. MAL work at Department of Internal Medicine, Seoul St. Mary's hospital, The Catholic University of Korea, Seoul. SH work at Department of Hematology and Oncology, Jeju National University Hospital, Jeju National University College of Medicine, Jeju. YH work at Department of Internal Medicine, Kangwon National University Hospital, Kangwon National University College of Medicine, Chuncheon. JC work at Department of Medical Oncology, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The institutional review board (IRB) of Ulsan University Medical Center approved this study (approved No.: 2017-11-013). We obtained appropriate permissions utilizing a written informed consent document prior to study participation and questionnaire was completed anonymously and voluntarily. All data collected were handled confidentially in an approved manner. In addition to this, we declare that we performed in accordance with the ethical standards of the National Research Committee and the provisions of the Declaration of Helsinki in 1995 of research and publication ethics strictly including authorship and regulations by including a statement in the ethics approval and consent to participate section.
Consent for publication
Not Applicable.
Competing interests
Competing interests relevant to this article was not reported. All authors declare that they have no all financial and non-financial competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Life-sustaining treatment pilot project questionnaire for doctors.
Additional file 2.
Life-sustaining treatment pilot project questionnaire for nurses.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Im, HS., Lee, I., Kim, S. et al. Experience and perspectives of end-of-life care discussion and physician orders for life-sustaining treatment of Korea (POLST-K): a cross-sectional study. BMC Med Ethics 24, 18 (2023). https://doi.org/10.1186/s12910-023-00897-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12910-023-00897-x