
Abstract
Background
Breast cancer is one of the most common diseases globally that may have side effects on liver and renal function. Pharmacological treatments to reduce adverse liver and renal effects are still limited. It has been proposed that silymarin may possess hepatoprotective and anti-inflammatory properties. The present trial aims to assess the hepatorenal protective efficacy of silymarin supplementation in cancer patients receiving chemotherapy in an outpatient setting.
Method
This is a randomized, placebo-controlled clinical trial that recruited female breast cancer patients. Participants were randomly assigned to one placebo group and two intervention groups. The control group received 140 mg of placebo daily, while the two intervention groups received 140 mg silymarin daily. Follow-up assessments were conducted at baseline, 3 weeks, and 6 weeks. At the beginning of the study, the patients were subjected to a computed tomography (CT) scan, and the liver and renal parameters such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), bilirubin, Blood urea nitrogen (BUN) and Creatinine (Cr) were examined through laboratory tests.
Results
Despite two deaths and three dropouts, 100 patients completed the study. Silymarin showed significant effects on liver enzymes in the levels of ALP and bilirubin (P < 0.05), with no significant impact on renal function in the levels of Blood urea nitrogen (BUN) and Creatinine (Cr) (P > 0.05). The medication was well-tolerated, with minimal reported side effects (P > 0.05).
Discussion
The study suggests that silymarin may have hepato-renal protective potential in breast cancer patients and improve patient tolerance to chemotherapy. The data presented on the efficacy and safety of silymarin may provide stronger foundation for further trials and for a possible use in clinical practice.
Trial registration information
Registration Number: IRCT20201123049474N2, First Trial Registration: 16/08/2021, Access: https://www.irct.behdasht.gov.ir/trial/57641
Similar content being viewed by others

Introduction
Cancer is one of the common chronic and non-communicable diseases that account for 9% of deaths worldwide [1]. In advanced countries, it is the second leading cause of death after cardiovascular diseases and it ranks as the fourth leading cause of death in developing countries [2]. In total, 50 million deaths occur annually worldwide, with over 5 million attributed to cancer [3]. According to published statistics, the death rate from cancer in Iran was 66.92 per 100,000 people each year [4]. The prevalence of cancer is increasing, with factors such as global population aging, increased risk behaviors, especially smoking, exposure to stimulants like chemicals and radiotherapy [5], inappropriate dietary habits, and sedentary lifestyles contributing to this rise [6, 7].
Various techniques are used to predict and treat cancers, including chemotherapy, radiotherapy, surgery, hormone therapy, immunotherapy, biological therapies, cryotherapy and artificial intelligence [8,9,10,11,12]. These treatments can last for weeks or months, significantly impacting a patient’s quality of life [13]. On the other hand, chemotherapy drugs are generally associated with various side effects. The most common of these side effects include nausea, vomiting, diarrhea, hair loss, darkening of the skin and nails, bone marrow suppression, mucositis, ovarian dysfunction, hyperuricemia, neuropathy, cardiomyopathy, hemorrhagic cystitis, renal and hepatic issues, and electrolyte imbalances [14,15,16]. A study in the United States has shown that 22 FDA-approved cancer drugs between 2000 and 2002 were associated with 25 serious adverse effects [17]. Paclitaxel and docetaxel are new class spindle inhibitor drugs that prevent mitosis. The mechanism of action is through microtubules. These two drugs have been associated with an increase in aminotransferase levels in 7 to 26% of cases and mild elevation in bilirubin levels, as well as causing hepatotoxicity in 5 to 20% of cases, which is usually asymptomatic and self-limiting due to the direct effect of the drug [18, 19].
Extensive studies have been conducted to evaluate the protective effects of various chemical compounds in reducing the toxic effects of chemotherapeutic drugs on the liver [20, 21]. However, some compounds used as chemoprotectors to reduce the adverse effects and toxicity in therapeutic methods may decrease their anticancer effects, while others do not completely eliminate the toxic effects of these drugs [22]. On the other hand, biologically derived plant-based substances, which constitute a branch of modern pharmacotherapy for diseases, have very minimal side effects in patients [23,24,25]. Therefore, the search for natural products in this field is of particular clinical importance. In recent years, the development of new plant-derived antioxidants to overcome damage caused by toxic chemical factors has been a serious focus for researchers [26]. Antioxidants are substances that, even in small amounts, can protect the body against various oxidative damages caused by reactive oxygen species [27].
In recent decades, a variety of dietary and herbal supplements have been traditionally used alongside some industrial drugs and non-steroidal anti-inflammatory drugs to control and modify undesirable symptoms and indicators of many diseases [28, 29]. Therefore, the results of some studies suggest that the herbal medicine Silybum marianum (Milk Thistle), also known as Mary Thistle or Holy Thistle, as a member of the daisy or aster family native to the Mediterranean region, has clinically significant effects in treating many metabolic diseases in modern medicine [30,31,32]. Researchers highlight the importance of the main methanolic extract of Milk Thistle seeds, namely Silymarin with the chemical formula C25H22O10, as the main effective flavonoid for pharmacological and physiological purposes [31, 32]. Silymarin is a complex mixture of polyphenolic molecules, including seven related flavonolignans such as Silybin A, Silybin B, Isosilybin A, Isosilybin B, Silychristin, Isosilychristin, and Silidianin, and a flavonoid called Taxifolin [33]. Clinical studies have shown that Silymarin, particularly Silybum as a Major Bioactive Component of Milk Thistle [34, 35], due to its antioxidant, anti-inflammatory, antifibrotic, hepatocyte-regenerating, and immune system-regulating properties, is widely used for the treatment of various liver diseases (such as cirrhosis, carcinoma, hepatitis, and fatty liver), diabetes, atherosclerosis, cancer, osteoporosis, and for the regulation of lipids and blood sugar [36,37,38].
Nowadays, Silymarin is utilized in in managing a broad spectrum of diseases including liver dysfunctions (fatty liver, hepatitis, jaundice, alcohol-induced liver damage, ischemia, drug and environmental toxicities, and even liver fibrosis) [39], cancers, neurological diseases, parasitic and infectious diseases, and metabolic disorders [40, 41]. Silymarin can reduce the levels of free radicals such as hydroxyl, superoxide, and hydrogen peroxide, increase the stimulation of glutathione production and enhance the activity of superoxide dismutase enzymes, leading to the prevention of lipid peroxidation, maintenance of cell membrane integrity, prevention of leakage of intracellular enzymes, and consequently reducing liver tissue damage. Additionally, by inhibiting the NF-κB gene and subsequently reducing the production of pro-inflammatory cytokines from the liver, Silymarin protects against damage [42, 43]. Furthermore, Silymarin is involved in preventing liver-related damage by inhibiting phosphatidylcholine synthesis and protein and RNA simulation [44].
The preventive and anticancer effects of silymarin have been confirmed and well-documented in many studies. However, its hepatorenal protective effects have been limitedly investigated in cancer patients, particularly those with breast cancer [45]. Kakar et al. have demonstrated that a one-month treatment with silymarin (140 milligrams three times a day) among 30 breast cancer patients without any metastasis can significantly reduce severity of hepatotoxicity in patients undergoing treatment with doxorubicin/cyclophosphamide-paclitaxel (AC-T) regimen [46]. A study conducted by Mohaghegh et al. to investigate the effect of silymarin on reducing hepatic side effects of taxanes in breast cancer patients undergoing chemotherapy with taxane-containing regimens divided patients into two treatment groups and a placebo group, showed that although there was a significant difference between the two groups after the study, the changes in the intervention group before and after treatment were not significant [21]. Another study by Hangag et al. in children with acute lymphoblastic leukemia undergoing chemotherapy with methotrexate, silymarin therapy improved some liver function indicators such as ALT, AST, and ALP, while albumin and bilirubin levels did not differ between the treatment and control groups [47]. Studies also highlight the hepatorenal protective effects of silymarin through its anti-inflammatory, anti-apoptotic, and antioxidant properties, as well as its capacity to prevent oxidative stress and pathological tissue changes caused by chemotherapy-induced damage [48, 49].
The importance of using silymarin as a complementary or non-toxic drug in improving the function of various cancer, kidney and liver groups has been highlighted. However, limited studies have focused on the hepatorenal protective effects of silymarin on breast cancer patients undergoing chemotherapy. Therefore, proactive evaluation of silymarin on the health performance of cancer patients undergoing chemotherapy with the aim of improving quality of life and increasing tolerance to chemotherapy is essential, given the importance of preventing liver damage in the treatment process of cancer patients. This randomized controlled clinical trial, with a parallel drug-controlled group, can help improve treatment performance methods, increase the effectiveness of chemotherapy in breast cancer patients and play a significant role in improving patient health by identifying and determining the protective potential of silymarin. Therefore, the main objective of this study was to evaluate the hepatorenal protective efficacy of silymarin supplementation in cancer patients receiving chemotherapy, with the hypothesis that silymarin supplementation leads to improved liver and renal function test results compared to placebo.
Method: participants, interventions, and outcomes
Study design
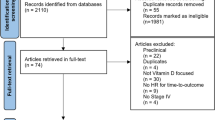
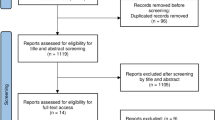
This study is a randomized, parallel-group, placebo-controlled clinical trial conducted to investigate the preventive effect of silymarin (livergel) on hepatorenal damage caused by chemotherapy in cancer patients referred to affiliated outpatient clinics of an academic institution with chemotherapy indications in 2021. To perform interventions and collect data, after the study protocol was approved by the Medical Ethics Committee (First Trial Registration: 16/08/2021, Registration Number: IRCT20201123049474N2), patients meeting the inclusion criteria completed informed consent forms to participate in the study. The informed consent form included elements such as the introduction of the research, the procedures involved, the manner of participation, benefits and potential side effects, costs, alternative methods, confidentiality of information, the researcher’s accountability to answer queries, the right to decline or withdraw from the study, and the affirmation of the consent form. After determining the required sample size for each group and identifying breast cancer patients without hepatic metastasis, a randomization method (using computer-generated random numbers) was employed to allocate patients to each group, and 35 individuals were recruited per group. Initially, encompassing detailed of patient demographics, medical history, and clinical outcomes were collected, and after the intervention, data were reassessed following a 60-day period. The study flowchart is shown in Fig. 1. Data collection was conducted by a trained researcher following approved protocol. A clinical trials expert verified and confirmed the collected data to ensure its accuracy and validity. A secure and centralized data repository was established with restricted access to maintain confidentiality and data integrity.

Study design and flowchart
Sample size
The sample size was calculated based on the equation for comparing means in at least two groups using SPSS 26.0 software (IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp). Considering the assumption of equal variances, a minimum of 10% dropout rate, study power of 80% with a statistical significance level (α) of 95% (P = 0.05), a sample size of 35 individuals per group was determined, resulting in a total sample size of 105 individuals in the current study (Eq. 1).
Where \(\:Z(1-\frac{\alpha\:}{2})=1.96\), α = 0.05, β = 0.2, d = 0.7 SD
After calculating the sample size, patients who met the study inclusion criteria were selected using simple random sampling method and allocated into three groups (placebo, treatment 1, and treatment 2) in a 1:1 ratio based on random allocation generated by a biostatistician using a computer-generated random number table inside the clinic.
Eligibility criteria
Inclusion and exclusion criteria
Inclusion criteria for the study included female patients aged 30 to 60 years, ability to take oral medication, definitive diagnosis of breast cancer with indication for chemotherapy but not yet received chemotherapy, normal liver function tests before intervention, indication for treatment with chemotherapy regimen, non-pregnant and not lactating, absence of liver metastasis (except stage 4) and liver disease. Exclusion criteria also included patient death, pregnancy during the study, patients who were unwilling to continue and cooperate in the study.
Interventions
Following determining the sample size in each group, researchers identified patients by attending the clinic. Initially, patients with breast cancer who had been visited by an oncology specialist and met the indication for chemotherapy and study entry criteria were informed consented, and the study objective was explained. To this end, patients underwent an initial computed tomography (CT) scan at the beginning of the study to confirm the absence of hepatic metastasis based on the initial assessment results. Subsequently, using a two-part checklist including demographic information such as age, and basic clinical information such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), bilirubin, Blood urea nitrogen (BUN) and Creatinine (Cr), all patients were collected. After assigning individuals to the relevant intervention and control groups, each group received two tablets daily (total of 120 tablets) for 60 days during the study period. The control group (G1) received a placebo, while treatment groups 1 (G2) and 2 (G3) received silymarin. The control group received two placebo tablets daily, treatment group 1 received two tablets of 140 mg silymarin daily cycle simultaneously with the start of the first chemotherapy cycle, and treatment group 2 received two tablets of 140 mg silymarin daily one week before the start of the first chemotherapy for two months.
The control group also received placebo tablets daily for two months starting with the first chemotherapy cycle. Liver and renal enzymes were re-evaluated at three time points (0, 3, and 6 weeks) during the study by a reliable laboratory that was unaware of the study and groups. Furthermore, participants were provided with information about the study drug, such as a drug information brochure, in accordance with local procedures, and a drug diary card for recording their weekly consumption. In case of missing a dose, participants were instructed not to take the medication unless 3 ± days had passed from the scheduled date. face-to-face consultations every two weeks and monthly Telephone contact were carried out for all participants. Finally, after completing the intervention period, a brief telephone counseling session was conducted to discuss the side effects of the drug taken and improvements in the participants’ health conditions.
Statistical analysis
After collecting the relevant data, the information was entered into the software. Continuous and categorical variables were reported as mean ± standard deviation (SD) and frequency (percentage). Normality of continuous data was evaluated using Kolmogorov-Smirnov test and Q-Q plot. categorical data were compared between three groups using chi-squared test. Repeated measures analysis of variance was used for evaluating within and between groups compassions in terms of liver enzymes and nephrological indices. Sphericity assumption was evaluated by using Muchly test and when it was violated, the multivariate analysis of variance adopted for data analysis. We also compared three groups in each study time point by using one-way analysis of variance (ANOVA) along with Bonferroni correction for multiple testing [50]. All statistical analyses were conducted using SPSS version 26 (IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp). A statistical significance level of P-Value < 0.05 was considered for all analyses.
Results
During the period of this clinical trial study, totally 105 female patients with breast cancer were screened and recruited for the trial, of whom 35 patients in placebo group 1 (G1), 35 patients in the silymarin group 2 (G2), and 35 patients in the silymarin group 3 (G3). During the study, two individuals died due to a heart attack (Group G2) and a pulmonary embolism (Group G3). Three individuals also dropped out due to the recommendation of their relatives not to use herbal medication (Group G1), experience severe nausea and vomiting (Group G2), and reading the drug information leaflet and being aware of the side effects of the drug (Group G2). they discontinued medicine use and were not willing to continued cooperation. Ultimately, 100 patients completed the study (Fig. 1).
The minimum age in G1 and G3 groups was 28 years, and the maximum age was 60 years, while the minimum and maximum age in the G2 group was 33 and 60 years, respectively. The mean age of patients in G1 group was 48.74 ± 8.06 years, in G2 group was 52.09 ± 7.35 years, and in G3 group was 48.51 ± 8.85 years. There was no statistically significant difference among the three groups in terms of age and P = 0.125 indicated that the three groups were approximately equal in age.
The level of liver enzymes in three different periods in the intervention and control groups has been presented in Table 1. Mean change of AST over study period was significant in group G3 (P = 0.01), and marginally significant in group G2 (P = 0.059). Also, it was not significant in group G1 (P = 0.143). However, there was no significant difference between three groups both generally (PGroup=0.216) and each time point (P > 0.01 for all three time points). The trend of changes in three groups for AST was similar (PTime*Group=0.414). Mean change of ALT over study period was significant in group G2 (P = 0.007), and group G3 (P = 0.039). However, there was not significant different in group G1 (P = 0.277). Also, there was no significant difference between three groups both generally (PGroup=0.599) and each time point (P > 0.01 for all three time points). The trend of changes in three groups for ALT was similar (PTime*Group=0.063).
Mean ALP period showed significant change over study in group G2 (PTime =0.001), and group G3 (PTime = < 0.001). However, it was not significant difference in group G1 (PTime =0.324). Three groups showed significant difference overly in terms of changes in this variable (PGroup=0.001) and the difference between three groups was significant at 6 weeks in which the mean ALP in this time point in groups G2 and G3 was significantly higher than G1 (P < 0.001). The trend of changes show similar patterns over time in three groups for ALP (PTime*Group<0.001). Furthermore, Mean bilirubin period indicated significant change over study in group G3 (PTime =0.042). However, there was not significant difference in group G1 (PTime =0.57), and group G2 (PTime=0.55). Also, there was no significant difference between three groups both generally (PGroup = 0.314). However, the trend of bilirubin changes among three groups after a period of 6 weeks was significant (PTime*Group = 0.046). These findings demonstrate that silymarin’s hepatoprotective effects on breast cancer patients are notable in certain parameters, such as ALP and Bilirubin, potentially leading to improved liver function.
Furthermore, the laboratory test results of two parameters, BUN and Cr, were compared among the three groups after administration of silymarin and placebo (Table 2). The Mean change of BUN and Cr over study period was not significant among any of the groups (P > 0.05). Also, there was no significant difference between the three groups both in general (PGroup>0.05) and each time point (P > 0.05 for all three time periods). However, the trend of changes in three groups for BUN and Cr were similar (PTime*Group=0.414). These findings indicate that the renal protective effect of silymarin on breast cancer patients was not considerable and did not result in any significant changes.
The results of the assessment of medication and chemotherapy side effects among three groups are showed in Table 3. Only one individual in Group G2 reported medication side effects (3.1%). The chemotherapy side effects reported in Group G2 (12%) were higher compared to the other groups. However, the reported side effects among the groups did not show a significant difference (P > 0.05). Therefore, silymarin has not shown significant toxicity or drug interactions among patients and is considered safe for medicinal use.
Discussion
Breast cancer is one of the most common malignancies, especially among women worldwide. According to statistics in 2020, more than 2.3 million cases of breast cancer were reported globally [51]. Various studies have shown a high incidence of functional disorders and hepatotoxicity in cancer patients undergoing chemotherapy [52, 53]. Medications and agents used in cancer chemotherapy are often associated with drug-induced liver injury (DILI). Therefore, cancer patients, as a sensitive group receiving chemotherapy, require precise evaluation of liver and renal functions to select the most appropriate chemotherapy agent and necessary medication [54]. These findings highlight the importance of finding a medicine to control hepatotoxicity and improve liver function in cancer patients. Therefore, this study was conducted to investigate the effectiveness of silymarin on liver and renal function tests and related markers in cancer patients undergoing chemotherapy in an outpatient setting. To the best of our knowledge, this clinical trial is the first human study to examine the effects of silymarin on serum levels of antioxidant markers and liver enzymes in breast cancer patients with liver damage.
The preliminary findings of this study indicated that receiving 140 mg of silymarin supplement twice daily over a 60-day period can lead to significant changes on liver enzymes such as bilirubin and ALP compared to the placebo. However, these changes were not significant for liver enzymes including ALT, AST, and BUN compared to the placebo. The multiple beneficial effects and properties of silymarin, such as its antioxidant, anti-inflammatory, liver-protective, anti-fibrotic properties, and its role in insulin resistance modulation, have been identified in many studies [54, 55]. Therefore, the findings of this study are comparable and open to further examination with the results of other studies.
Based on the findings of Kim et al., the oral consumption of silymarin may have a significant impact on liver damage caused by stress in mice, particularly antioxidant and anti-inflammatory damages [56]. Additionally, Yemişen et al. reported that silymarin had positive effects on reversing liver damage caused by burns in burned rats with both topical and systemic silymarin treatment [57]. Numerous clinical trials have been conducted on the hepatoprotective effects of silymarin in various pathological conditions in different groups. Mirzaei et al. reported that the consumption of livergol tablets containing 140 mg of silymarin three times daily for 14 days by 90 trauma patients hospitalized in the intensive care unit significantly reduced liver enzymes compared to the placebo group [58]. Furthermore, in the study by Eqbali et al., comparing the changes of silymarin consumption in a patient with acute lymphoblastic leukemia (ALL) over 5 years showed that oral silymarin intake led to a partial significant decrease in ALT, AST, GGT, and bilirubin levels, but had no effect on ALP, albumin, and cholesterol [59]. In other studies, the effects of silymarin on improving liver parameters in patients with Non-alcoholic fatty liver disease (NAFLD) [60] and inhibiting the proliferation of human breast cancer cells have been proven [56].
However, contrary to the findings of the present study, the results of the Atarodi et al.‘s study, which was conducted on 56 morbidly obese patients, showed that consuming 140 mg of silymarin three times a day for 4 weeks did not show any significant difference in changes in aspartate transaminase, alkaline phosphatase, liver size, cholesterol, and triglycerides between the silymarin and placebo groups [61]. Additionally, in another randomized controlled trial on patients with acute clinical hepatitis, no discernible effect on biomarkers of the inflammatory process of liver cells, including ALT and AST, was reported [62]. These contradictory results may stem from variations in study design, dosages, patient populations, and specific conditions under treatment. Furthermore, understanding molecular mechanisms and identifying optimal dosage regimens for the effective integration of silymarin in the clinical management of cancer patients is of great importance [63]. Therefore, while silymarin has protective potential, its use should be approached with caution.
Potential mechanisms and clinical implications
silymarin, the main compound found in milk thistle, prevents various toxins from entering liver cells by promoting cell regeneration and altering the outer layer of liver cells, and possesses a unique property of protecting the liver [40, 64]. Silymarin is also considered a promising candidate for addressing liver disorders associated with inflammation and oxidative stress, as it suppresses the activation of NF-kB, which regulates the expression of pro-inflammatory genes [65]. Studies also indicate that silymarin stimulates the liver to produce more bile, aiding in liver detoxification and improving digestive system function. Despite advances in pharmacology, the use of silymarin is still considered the best therapeutic option without any specific aggressive side effects [39, 66].
Other findings of this study also demonstrated that patients undergoing silymarin therapy tolerated it well, and no side effects were observed among the participants. Only one individual reported nausea and vomiting as a result. According to the results of studies, the most common side effects of silymarin are gastrointestinal symptoms including diarrhea, dyspepsia, irregular bowel movements, and nausea [67]. Our results are in line with previous studies that have confirmed the safety of silymarin [68]. Therefore, silymarin as a complementary medicine can be beneficial in managing pathological conditions such as a wide range of cancers, alcoholic liver diseases, liver cirrhosis, Amanita mushroom poisoning, viral hepatitis, drug-induced liver diseases, and drug-induced kidney damage.
Study limitations and suggestions
Our study had limitations that need to be addressed. Firstly, patients may be influenced by incorrect conversations and recommendations from their surroundings and may refrain from taking their medication, which can be addressed through further education and continuous efforts to raise awareness. Secondly, due to limitations, the mechanism of drug action on changes in renal parameters was not investigated, which could be explored in future studies. Additionally, there was no follow-up period after the completion of the drug regimen, which could be a focus in future studies. Specific liver tumor markers associated with breast cancer, such as CA 15 − 3 and CEA, can provide further insights. Therefore, liver and kidney tissue biopsy samples can be utilized for hepatorenal histological studies. However, it should be noted that liver biopsies are invasive procedures that can carry significant risks, especially in patients undergoing chemotherapy. Therefore, despite the existing limitations, the present study provides preliminary evidence that silymarin may be a safe and effective supportive care agent in improving liver function in patients undergoing chemotherapy.
Conclusion
The results of this clinical trial study showed that supplementation with 140 mg of silymarin two times daily could significantly lower the serum levels of Bili and ALP in breast cancer patients with increased levels of liver enzymes. The results of this study may provide a valuable opinion on whether silymarin can be used as adjuvant therapy for the management or treatment of liver disease of cancer patients. The data presented on the efficacy and safety of silymarin may provide more foundation for further trials and for a possible use in clinical practice. Therefore, further studies with larger sample sizes and longer follow-up durations are required to better determine the efficacy of this treatment modality.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Razzaghi H, Martin DN, Quesnel-Crooks S, Hong Y, Gregg E, Andall-Brereton G, et al. 10-year trends in noncommunicable disease mortality in the Caribbean region. Rev Panam Salud Publica. 2019;43:e37.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians. 2021;71(3):209–49.
Frick C, Rumgay H, Vignat J, Ginsburg O, Nolte E, Bray F, et al. Quantitative estimates of preventable and treatable deaths from 36 cancers worldwide: a population-based study. Lancet Glob Health. 2023;11(11):e1700–12.
Neda I, Etemad K, Mohseni P, Khosravi A, Akbari M. Mortality rates and years of life lost due to cancer in Iran: analysis of data from the National Death Registration System, 2016. Int J Cancer Manage. 2022;15.
Liu M, An R, Wu Z, Dai L, Zeng Q, Chen W. The trajectory of oral mucositis in head and neck cancer patients undergoing radiotherapy and its influencing factors. Ear Nose Throat J. 2024;0(0):01455613241228211.
Alshammari FD, Ahmed HG, Alshammari D, Alharbi AM, Alsaedi AS, Elasbaly A. Population insight of the relationship between lifestyle and cancer: a population-based survey. AIMS Public Health. 2019;6(1):34–48.
Fentie H, Ntenda PAM, Tiruneh FN. Dietary pattern and other factors of breast cancer among women: a case control study in Northwest Ethiopia. BMC Cancer. 2023;23(1):1050.
Debela DT, Muzazu SG, Heraro KD, Ndalama MT, Mesele BW, Haile DC, et al. New approaches and procedures for cancer treatment: current perspectives. SAGE Open Med. 2021;9:20503121211034366.
Pucci C, Martinelli C, Ciofani G. Innovative approaches for cancer treatment: current perspectives and new challenges. Ecancermedicalscience. 2019;13:961.
He B, Sun H, Bao M, Li H, He J, Tian G, et al. A cross-cohort computational framework to trace tumor tissue-of-origin based on RNA sequencing. Sci Rep. 2023;13(1):15356.
He B, Zhang Y, Zhou Z, Wang B, Liang Y, Lang J, et al. A neural network framework for predicting the tissue-of-origin of 15 common cancer types based on RNA-Seq data. Front Bioeng Biotechnol. 2020;8:737.
Li M, Wei J, Xue C, Zhou X, Chen S, Zheng L, et al. Dissecting the roles and clinical potential of YY1 in the tumor microenvironment. Front Oncol. 2023;13:1122110.
Antony A, Joel J, Shetty J, Umar NF. Identification and analysis of adverse drug reactions associated with cancer chemotherapy in hospitalized patients. 2016;8:448–51.
van den Boogaard WM, Komninos DS, Vermeij WP. Chemotherapy side-effects: not all DNA damage is equal. Cancers. 2022;14(3):627.
Oun R, Moussa YE, Wheate NJ. The side effects of platinum-based chemotherapy drugs: a review for chemists. Dalton Trans. 2018;47(19):6645–53.
Fan Z, He Y, Sun W, Li Z, Ye C, Wang C. Clinical characteristics, diagnosis and management of sweet syndrome induced by azathioprine. Clin Experimental Med. 2023;23(7):3581–7.
Hanigan MH, Devarajan P. Cisplatin nephrotoxicity: molecular mechanisms. Cancer Ther. 2003;1:47–61.
Huizing MT, Misser VH, Pieters RC, ten Bokkel Huinink WW, Veenhof CH, Vermorken JB, et al. Taxanes: a new class of antitumor agents. Cancer Invest. 1995;13(4):381–404.
Hooker AC, Ten Tije AJ, Carducci MA, Weber J, Garrett-Mayer E, Gelderblom H, et al. Population pharmacokinetic model for docetaxel in patients with varying degrees of liver function: incorporating cytochrome P4503A activity measurements. Clin Pharmacol Ther. 2008;84(1):111–8.
Shirani K, Yousefsani BS, Shirani M, Karimi G. Protective effects of naringin against drugs and chemical toxins induced hepatotoxicity: a review. Phytother Res. 2020;34(8):1734–44.
Mohaghegh F, Solhi H, Kazemifar AM. Silymarin (milk thistle) can revoke liver enzyme changes during chemotherapy of breast cancer with Taxanes. Eur J Integr Med. 2015;7(6):650–2.
Datta S, Aggarwal D, Sehrawat N, Yadav M, Sharma V, Sharma A, et al. Hepatoprotective effects of natural drugs: current trends, scope, relevance and future perspectives. Phytomedicine. 2023;121:155100.
Chaachouay N, Zidane L. Plant-derived natural products: a source for drug discovery and development. Drugs Drug Candidates. 2024;3(1):184–207.
Desai AG, Qazi GN, Ganju RK, El-Tamer M, Singh J, Saxena AK, et al. Medicinal plants and cancer chemoprevention. Curr Drug Metab. 2008;9(7):581–91.
Gao T-H, Liao W, Lin L-T, Zhu Z-P, Lu M-G, Fu C-M, et al. Curcumae rhizoma and its major constituents against hepatobiliary disease: pharmacotherapeutic properties and potential clinical applications. Phytomedicine. 2022;102:154090.
Akbari B, Baghaei-Yazdi N, Bahmaie M, Mahdavi Abhari F. The role of plant‐derived natural antioxidants in reduction of oxidative stress. BioFactors. 2022;48(3):611–33.
Agrawal AD. Pharmacological activities of flavonoids: a review. Int J Pharm Sci Nanotechnology(IJPSN). 2011;4(2):1394–8.
Pandey G, Sahni YP. A review on hepatoprotective activity of silymarin. Int J Res Ayurveda Pharm. 2011;2:75–9.
Newman DJ, Cragg GM. Natural products as sources of new drugs over the nearly four decades from 01/1981 to 09/2019. J Nat Prod. 2020;83(3):770–803.
Jia R, Cao L, Du J, Xu P, Jeney G, Yin G. The protective effect of silymarin on the carbon tetrachloride (CCl4)-induced liver injury in common carp (Cyprinus carpio). Vitro Cell Dev Biol Anim. 2013;49(3):155–61.
Shaker E, Mahmoud H, Mnaa S. Silymarin, the antioxidant component and Silybum marianum extracts prevent liver damage. Food Chem Toxicol. 2010;48(3):803–6.
Guo Y, Wang S, Wang Y, Zhu T. Silymarin improved diet-induced liver damage and insulin resistance by decreasing inflammation in mice. Pharm Biol. 2016;54(12):2995–3000.
Vrba J, Papoušková B, Kosina P, Lněničková K, Valentová K, Ulrichová J. Identification of human sulfotransferases active towards Silymarin flavonolignans and Taxifolin. Metabolites. 2020;10(8).
Loguercio C, Festi D. Silybin and the liver: from basic research to clinical practice. World J Gastroenterol. 2011;17(18):2288–301.
Bijak M. Silybin, a major bioactive component of milk thistle (Silybum marianum L. Gaernt.)—Chemistry, Bioavailability, and metabolism. Molecules. 2017;22(11):1942.
Anthony KP, Saleh MA. Free radical scavenging and antioxidant activities of Silymarin components. Antioxid (Basel). 2013;2(4):398–407.
El-Lakkany NM, Hammam OA, El-Maadawy WH, Badawy AA, Ain-Shoka AA, Ebeid FA. Anti-inflammatory/anti-fibrotic effects of the hepatoprotective silymarin and the schistosomicide praziquantel against Schistosoma mansoni-induced liver fibrosis. Parasites Vectors. 2012;5(1):9.
Induction of Microsomal Liver. Enzymes by silymarin in experimental animals. J Fac Med Baghdad. 2011;53(2):233–5.
Jaffar HM, Al-Asmari F, Khan FA, Rahim MA, Zongo E. Silymarin: unveiling its pharmacological spectrum and therapeutic potential in liver diseases—A comprehensive narrative review. Food Science & Nutrition. 2024;n/a(n/a).
Al-Rasheed N, Faddah L, Al-Rasheed N, Bassiouni YA, Hasan IH, Mahmoud AM, et al. Protective effects of Silymarin, alone or in combination with chlorogenic acid and/or melatonin, against carbon tetrachloride-induced hepatotoxicity. Pharmacogn Mag. 2016;12(Suppl 3):S337–45.
Wang Y, Yuan A-J, Wu Y-J, Wu L-M, Zhang L. Silymarin in cancer therapy: mechanisms of action, protective roles in chemotherapy-induced toxicity, and nanoformulations. J Funct Foods. 2023;100:105384.
Hackett ES, Twedt DC, Gustafson DL. Milk thistle and its derivative compounds: a review of opportunities for treatment of liver disease. J Vet Intern Med. 2013;27(1):10–6.
Matias ML, Gomes VJ, Romao-Veiga M, Ribeiro VR, Nunes PR, Romagnoli GG et al. Silibinin downregulates the NF-κB pathway and NLRP1/NLRP3 inflammasomes in monocytes from pregnant women with preeclampsia. Molecules. 2019;24(8).
Banaee M, Sureda A, Mirvaghefi AR, Rafei GR. Effects of long-term silymarin oral supplementation on the blood biochemical profile of rainbow trout (Oncorhynchus mykiss). Fish Physiol Biochem. 2011;37(4):885–96.
Koltai T, Fliegel L. Role of silymarin in cancer treatment: facts, hypotheses, and questions. J Evid Based Integr Med. 2022;27:2515690x211068826.
Kacar S, Bektur Aykanat NE, Sahinturk V. Silymarin inhibited DU145 cells by activating SLIT2 protein and suppressing expression of CXCR4. Med Oncol. 2020;37(3):18.
Hagag AA, Elgamsy MA, El-Asy HM, Mabrouk MM. Protective role of silymarin on hepatic and renal toxicity induced by MTX based chemotherapy in children with acute lymphoblastic leukemia. Mediterr J Hematol Infect Dis. 2016;8(1):e2016043.
Gür FM, Aktaş İ. Silymarin protects kidneys from paclitaxel-induced nephrotoxicity. Turkish J Agric - Food Sci Technol. 2022;10(3):452–8.
Koltai T, Fliegel L. Role of silymarin in cancer treatment: facts, hypotheses, and questions. J Evidence-Based Integr Med. 2022;27:2515690X211068826.
Al-Laith M, Jasenecova M, Abraham S, Bosworth A, Bruce IN, Buckley CD, et al. Arthritis prevention in the pre-clinical phase of RA with abatacept (the APIPPRA study): a multi-centre, randomised, double-blind, parallel-group, placebo-controlled clinical trial protocol. Trials. 2019;20(1):429.
Sedeta ET, Jobre B, Avezbakiyev B. Breast cancer: global patterns of incidence, mortality, and trends. J Clin Oncol. 2023;41(16suppl):10528.
Christ TN, Stock W, Knoebel RW. Incidence of asparaginase-related hepatotoxicity, pancreatitis, and thrombotic events in adults with acute lymphoblastic leukemia treated with a pediatric-inspired regimen. J Oncol Pharm Pract. 2018;24(4):299–308.
Denton CC, Rawlins YA, Oberley MJ, Bhojwani D, Orgel E. Predictors of hepatotoxicity and pancreatitis in children and adolescents with acute lymphoblastic leukemia treated according to contemporary regimens. Pediatr Blood Cancer. 2018;65(3).
Gillessen A, Schmidt HH. Silymarin as supportive treatment in liver diseases: a narrative review. Adv Ther. 2020;37(4):1279–301.
Calderon Martinez E, Herrera D, Mogan S, Hameed Z, Jangda AA, Khan TJ, et al. Impact of silymarin supplements on liver enzyme levels: a systematic review. Cureus. 2023;15(10):e47608.
Kim SH, Choo GS, Yoo ES, Woo JS, Lee JH, Han SH, et al. Silymarin inhibits proliferation of human breast cancer cells via regulation of the MAPK signaling pathway and induction of apoptosis. Oncol Lett. 2021;21(6):492.
Yemişen E, Yarat A, Tunalı Akbay T, Toklu H, Şener G. The effect of silymarin on the liver in thermal burn injury. Marmara Pharm J. 2014;18(2):56–61.
Mirzaei E, Sabetian G, Masjedi M, Heidari R, Mirjalili M, Dehghanian A, et al. The effect of silymarin on liver enzymes and antioxidant status in trauma patients in the intensive care unit: a randomized double blinded placebo-controlled clinical trial. Clin Exp Hepatol. 2021;7(2):149–55.
Eghbali A, Sadeghian M, Ghasemi A, Afzal RR, Eghbali A, Ghaffari K. Effect of oral silymarin on liver function in pediatric acute lymphoblastic leukemia in the maintenance phase: a double-blind randomized clinical trial. Front Pharmacol. 2024;15:1295816.
de Avelar CR, Nunes BVC, da Silva Sassaki B, dos Santos Vasconcelos M, de Oliveira LPM, Lyra AC, et al. Efficacy of silymarin in patients with non-alcoholic fatty liver disease — the Siliver trial: a study protocol for a randomized controlled clinical trial. Trials. 2023;24(1):177.
Atarodi H, Pazouki A, Gholizadeh B, Karami R, Kabir A, Sadri G, et al. Effect of silymarin on liver size and nonalcoholic fatty liver disease in morbidly obese patients: a randomized double-blind clinical trial. J Res Med Sci. 2022;27:76.
El-Kamary SS, Shardell MD, Abdel-Hamid M, Ismail S, El-Ateek M, Metwally M, et al. A randomized controlled trial to assess the safety and efficacy of silymarin on symptoms, signs and biomarkers of acute hepatitis. Phytomedicine. 2009;16(5):391–400.
Kohutek F, Bystricky B. Optimal dose of silymarin for the management of drug–induced liver injury in oncology. Mol Clin Oncol. 2023;18(5):35.
Moradveisi B, Yazdanifard P, Fathollahpour A. Prevalence of clinical and paraclinical features of leukemia among children with acute lymphoblastic leukemia in Sanandaj Besat Hospital, 2008–2013. Sci J Iran Blood Transfus Organ. 2017;14:281–8.
Jaffar HM, Al-Asmari F, Khan FA, Rahim MA, Zongo E. Silymarin: unveiling its pharmacological spectrum and therapeutic potential in liver diseases—a comprehensive narrative review. Food Sci Nutr. 2024;12(5):3097–111.
Matutes E, Brito-Babapulle V, Swansbury J, Ellis J, Morilla R, Dearden C, et al. Clinical and laboratory features of 78 cases of T-prolymphocytic leukemia. Blood. 1991;78(12):3269–74.
Saller R, Brignoli R, Melzer J, Meier R. An updated systematic review with meta-analysis for the clinical evidence of silymarin. Forsch Komplementmed. 2008;15(1):9–20.
Mahi-birjand M, Karimzadeh I, Zarban A, Abdollahpour-Alitappeh M, Saadatjoo SA, Ziaee M. Protective effects of silymarin on gentamicin-induced nephrotoxicity in infectious patients: a randomized double blinded placebo-controlled clinical trial. Pharm Sci. 2020;26(3):287–95.
Acknowledgements
All authors would like to thank the Vice-Chancellor of Research and Technology of Isfahan University of Medical Sciences, as well as all the staff of the Hematology and Oncology, Department of Alzahra Hospital, Isfahan, Iran who participated in this study.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The present study was supported by Isfahan University of Medical Sciences, which has provided funding for this research (Grant No: 57641).
Author information
Authors and Affiliations
Contributions
SSE: Methodology, Project administration, Data curation, Software, Validation, Writing–original draft. AH: Investigation, Methodology, Writing–original draft. ShHJ: Writing–review and editing. ZA: Writing–review and editing. HA: Conceptualization, Methodology, Funding acquisition, Formal Analysis, Supervision, Visualization, Writing–original draft, Writing–review and editing.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was performed in line with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Isfahan University of Medical Sciences (IR.MUI.MED.REC.1399.763). Also, this study was conducted based on the approval of the clinical trial protocol (Registration Number: IRCT20201123049474N2, First Trial Registration: 16/08/2021, Access: https://www.irct.behdasht.gov.ir/trial/57641) and according to the CONSORT reporting guidelines. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants or their legal guardians/next of kin. The informed consent form included elements such as the introduction of the research, the procedures involved, the manner of participation, benefits and potential side effects, costs, alternative methods, confidentiality of information, the researcher’s accountability to answer queries, the right to decline or withdraw from the study, and the affirmation of the consent form.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Erfanian, S.S., Ansari, H., Javanmard, S.H. et al. The hepatorenal protective effects of silymarin in cancer patients receiving chemotherapy: a randomized, placebo-controlled trial. BMC Complement Med Ther 24, 329 (2024). https://doi.org/10.1186/s12906-024-04627-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-024-04627-7