
Abstract
Background
Diabetes is a leading health disorder and is responsible for high mortality rates across the globe. Multiple treatment protocols are being applied to overcome this morbidity and mortality including plant-based traditional medicines. This study was designed to investigate the ethnomedicinal status of plant species used to treat diabetes in District Karak, Pakistan.
Materials and methods
A semi-structured survey was created to collect data about traditionally used medicinal plants for diabetes and other ailments. The convenience sampling method was applied for the selection of informants. The collected data was evaluated through quantitative tools like frequency of citation (FC), relative frequency of citation (RFC), informant consensus factor (FIC), fidelity level (FL), and use value (UV).
Results
A total of 346 local informants were selected for this research. Out of them, 135 participants were men and 211 participants were women. Overall 38 plant species belonging to 29 plant families were used to treat diabetes. The most dominant plant family was Oleaceae having 11 species. Powder form (19%) was the most recommended mode of preparation for plant-based ethnomedicines. Leaves (68%) were the most frequently used parts followed by fruit (47%). The highest RFC was recorded for Apteranthes tuberculata (0.147). The maximum FL was reported for Apteranthes tuberculata (94.4) and Zygophyllum indicum (94.11) for diabetes, skin, and wounds. Similarly, the highest UV of (1) each was found for Brassica rapa, Melia azedarach, and Calotropis procera. Based on documented data, the reported ailments were grouped into 7 categories. The ICF values range between 0.89 (diabetes) to 0.33 (Cardiovascular disorders).
Conclusion
The study includes a variety of antidiabetic medicinal plants, which are used by the locals in various herbal preparations. The species Apteranthes tuberculata has been reported to be the most frequently used medicinal plant against diabetes. Therefore, it is recommended that such plants be further investigated in-vitro and in-vivo to determine their anti-diabetic effects.
Similar content being viewed by others


Background
Plants are the essential components of the planet Earth and are considered an excellent source of medicine. They are utilized in the treatment or prevention of a wide variety of diseases like diabetes, cancer, and cardiovascular problems [1]. Globally, diabetes mellitus is considered one of the leading causes of death as well as a top health condition [2]. A common metabolic disorder, diabetes mellitus occurs when there is insufficient supply of insulin (Type I) or when the body is resistant to insulin (Type II) [3]. Type II diabetes is also characterized by two significant conditions resulting from defective insulin secretion or reduced insulin sensitivity (insulin resistance) [4]. A report presented by the World Health Organization indicates that the diabetic population is possible to increase up to 300 million or more in 2025 [5]. Approximately 536.6 million people worldwide suffer from diabetes (diagnosed or undiagnosed) in 2021 according to the International Diabetes Federation and by 2045, this number will grow by 46% to 783.2 million [6]. There are several methods of treating diabetes including insulin, allopathic homeopathic, and traditional herbal medicines [7, 8].
According to International Diabetes Federation an estimated 26.7% of Pakistani adults affected by diabetes in 2022, and the number may reach 33 million approximately [9]. If awareness programs and proper treatment are not adopted, Pakistan may have double the number of diabetic patients by 2040 [10] and it is expected to reach 37.1 million by 2045 [11]. Additionally, diabetes was found to be more prevalent in urban areas (15.1%) than in rural areas (1.6%) [12]. A study reported that in rural areas, women's tolerance for glucose is 10.9% and men's is 6.9%, but in urban areas, it is 14.2% and women's is 6.3% [13].
The rural population of Pakistan relies significantly on their conventional herbal system for diabetic problems because the cost of allopathic prescription treatment for diabetes is too high [14]. According to research by the WHO, 855 traditional medicines use crude plant extracts, and more than 86% of people in underdeveloped countries depend on traditional remedies like herbs for their everyday requirements [15]. Plants with antidiabetic properties are commonly used in folk medicines. In ethnobotanical studies, around 800 plants are thought to have anti-diabetic effects [16]. In addition to these 800 plants, Momordica charantia, Pterocarpus marsupium, and Trigonella foenum-graecum have been reported to benefit type 2 diabetes patients [17]. Laboratory experiments have shown that around 343 plants have been tested for blood glucose [18]. The control of glucose metabolism is greatly influenced by natural plant products with a variety of distinct chemical components, such as phenolic compounds, flavonoids, terpenoids, alkaloids, glycosides, and coumarins [19]. Multiple herbs have exposed antidiabetic activity when reviewed using streptozotocin-induced diabetic rats [20]. Natural substances known as antioxidants help diabetes patients by scavenging different types of free radicals and decreasing the harm carried on by oxidative stress [21].
District Karak has diverse environmental conditions with unique flora. The people who live in this region are well-versed in the uses of plants. It not only reflects the unique identity of a community but also provides accessible and affordable healthcare solutions, particularly in areas where modern medical resources are scarce. As traditional healers often maintain close ties with their communities, they provide a holistic approach to health, focusing on not only physical but also mental and spiritual well-being. Their expertise, grounded in local knowledge of plants, herbs, and environmental factors, contributes to the diagnosis and treatment of ailments specific to the region. Local inhabitants use different plants for the treatment of different diseases like diabetes, cardiovascular, gastrointestinal, skin, and rheumatoid traditionally [22].
Studies on ethnobotany focus on the complex interactions between native people and plants, including traditions and cultural beliefs related to different applications. This research supports the collection of essential ethnobotanical data from indigenous people, such as herbalists, to conserve traditional knowledge of disease diagnosis and plant species utilized in folk medicine. In addition, their methods of planning and management, as well as the indigenous people's sociocultural heritage for future generations. The present research work is designed to summarize data about ethnobotanical data of plant species used against diabetes. This study aimed to have a long-term date of plants used traditionally by local inhabitants of southern regions of KPK, Pakistan. The area was selected based on rich sources of medicinal wild local plants, traditional uses of medicines by local people, and easily accessible areas.
Materials and methods
Study area
The current survey was carried out in District Karak, Pakistan (Fig. 1). The district Karak is situated in the south of KPK between latitudes 70-40° and 71-30°N and longitudes 32-48° and 33-23°E It includes both rural and urban areas with a total size of 600 Km2[23]. Small mountains make up the geography of the Karak district, and these mountains generally move from east to west. The climate during summer is hot with temperatures ranging from 40-45 0C. Sand storms are common in Tehsil Takht-e-Nasrati. Most areas in the district are arid. The area is rich in flora. Mostly it comprises xerophytes. Common species of the area are Acacia nilotica, Acacia arabica, Calotropis procera, Peganum harmala, and Citrullus colocynthis. Cultivated includes Wheat, Sorghum, Peanut, and Gram. The district is home to a variety of fauna like quail, crane, black and brown. It's a popular place to hunt quails and fowl (Batair). In Karak, many natural resources have been found. The salt mines were an important source of salt for the Indo-Pak subcontinent throughout the British period and were well-known in antiquity. Uranium, gas, and oil were found more recently. Makori, Noshpa Banda, and Gurguri are the three towns where oil and gas deposits have been discovered. Being rich in wild herbs, people have sufficient knowledge about medicinal plants and their use against different ailments.

Geographical location of the study area. Indicating three Tehsils (Takht-e-Nasrati, Karak, and Banda Daud Shah) where the study was conducted in District Karak, Khyber Pakhtunkhwa province, Pakistan
Data collection and field survey
Data on ethnomedicines was collected from September 2021 to February 2022. The data was collected in the Pashtu (native language) and then translated into English through a semi-structured questionnaire. The first section of the questionnaire includes the demographics of the informants, age, gender, and educational status. While remaining part of the questionnaire consists of knowledge of medicinal plants to treat diabetes and other ailments. Mainly concentrating on the native name of the medicinal plant, other additional ingredients, remedy preparation, which part of the plant is used, and the mode of administration and dosage information for children and adults. A convenience sampling method was used to collect information regarding medicinal plants used against diabetes traditionally. Participants in the study were acknowledged as well informed about local medicinal plants and had long-standing interactions with the local flora and ecosystem. Our survey's primary respondents, rather than conventional healers or professionals, were common people with local plant knowledge who learned it orally from their elders [24].
Code of Ethics of the International Society of Ethnobiology (ISE) was strictly followed while conducting the survey [25]. Before each interview, each participant verbally agreed. A description of the study's purpose and the subject matter was given to each participant. The convenience sampling method was applied to select the interviewers using the Cochran formula (1977) for sample size. n0=z2⋅p⋅ (1−p) e2. After calculation from the Cochran formula, a total of 790 primary participants were visited to know about their knowledge about the traditional usage of medicinal plants. Out of these, 346 respondents were considered for their knowledge related to the plants against diabetes.
In the first instance, local people medically diagnosed with diabetes were identified and designated as participants for this study. They were questioned about the plants, which are traditionally used against diabetes along with other ailments. This study primarily focused on medicinal plants used to cure diabetes.
Collection, identification, and preservation of medicinal plants
Plant species collected from the study area were identified by Dr.Ghazala Nawaz, Assistant Professor, Department of Botany, Kohat University of Science and Technology, Kohat, voucher numbers and deposition numbers were given e.g. BOT-KHS-90/2023-001 (BOT-KHS-90 represents voucher number(s) while 2023-001 is the deposition number). The specimens were then submitted to the Herbarium at the Department of Botany, Kohat University of Science and Technology, Pakistan. For specimen validation, the www.floraonline.org/taxon/wfo-0001020013 was accessed.
Data quality assurance
Each primary participant was contacted at least three times to confirm the information they had provided for data confirmation. Only validated and related information was subject to further analytical processes. Moreover, the authors were skilled in collecting medicinal plants from the area as well as gathering remedy formulation-related information, their uses, pointing out missing information, and replication material to maintain data quality.
Ethnobotanical indices
Frequency of citation (FC), relative frequency of citation (RFC), Species Use Value (UV), Fidelity level (FL), and Informant consensus factor (ICF), were among the quantitative indices used to analyze the ethnobotanical data.
Frequency of citation (FC)
FC is the number of primary participants who described using each monoherbal recipe for ethnomedicinal purposes [26].
Relative frequency of citation (RFC)
Relative frequency of citation (RFC) indicates the importance of each species locally within a study region [27]. N is the total number of informants in the survey, and FC is the number of primary participants who cited a helpful species. Using the previously discussed formula, RFC is determined. When the RFC value is 0, it indicates that fewer primary participants have found that monoherbal formulation to be helpful, and when the RFC value is 1, it indicates that more survey primary participants have found that monoherbal formulation to be helpful (Table 2) [28].
Use Value (UV)
Plant utilization standards are possessed and followed [29].
The N represents the total number of primary participants while U represents the amount of utilization average collected from each source for known species of plant and the Use value conveys the quantifiable sum of qualified purpose of species of plant.
Fidelity level (FL%)
Fidelity level is the ratio between the number of primary participants who independently mention one use of a plant species and the total number of primary participants who initially mention all uses of that plant species proposed by [30]. It is calculated as follows: Np is the number of primary participants who reported the usage of a species; N is the total number of primary participants who mentioned all the uses of that species; and N is multiplied by 100. When a plant species has a high FL for particular uses, the local population prefers that species for that use. The species with high FL authenticates its uniqueness to treat a disease [31].
Np =number of primary participants citing the use of the plant species for the treatment of a disease
N = total number of primary participants citing the species for disease.
Informant consensus factor (ICF)
To estimate the usage variability of medicinal plants by local informants, ICF was used [32]. It is a consensus between local primary participants for the treatment of a disease or disease category. ICF was calculated by following the formula;
Nur = total number of use citations for each disease category
Nt = total number of species listed in that category
The value of ICF ranges from 0 to 1. A higher value means there are well-defined criteria for medicine in the areas for a specific disease. A low value indicates that plants are not preferred and there is no exchange of information about their use [33].
Literature review
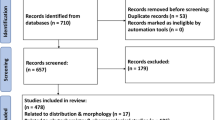
To find published data on the pharmacology and phytochemistry of anti-diabetic plants, online sources such as Google, Pub Med, Google Scholar, Web of Science, and Flora of Pakistan were utilized. Our Study examined 245 English-language research articles and 138 were then, selected and reviewed based on their pharmacological and phytochemical content. Out of these 138, a total of 66 were included in the review table (Fig. 2). Articles containing irrelevant data not related to our study were dropped. Various keywords, such as the in-vivo and in-vitro actions of anti-diabetic plants and the activity of secondary metabolites against diabetes were used to search the published literature. Using Tropicos, Plant List, www.flora.org, and the Flora of Pakistan, the accepted family names, recognized plant names, and synonyms were corrected (Table 3).

Flow chart showing the main stages of the review process
Results
Demographic characteristics of informants
A total of 346 respondents (211 male and 135 female) participated in collecting traditional information about the use of monoherbal medicines. They were divided into different modules based on their age, education, and occupation. Most of the primary participants (78%) were aged ≥50 years. Due to having more information about traditional medicinal plants, and recipes used against different diseases as well, males were more involved in commercial activities as compared to females. In males, most of the primary participants were shopkeepers while among females mostly they were housewives. The majority of them completed secondary school education, while the second largest number was illiterate (Fig. 3).

Demographic data of the respondents
Quantitative data analysis
Use value
The UV of the recorded medicinal plants varied from 1 to 0.03. Species having the highest use value were recorded for Brassica rapa, Melia azedarach and Calotropis procera [1], Trigonella foenum-graecum (0.66), Carica papaya (0.33), Abelmoschus esculentus and Aloe vera (0.23). The high used value indicates that these species are highly suggested and well-known by the interviewers, indicating the significance of the species. The plants with less UV are Apteranthes tuberculata and Zygophyllum indicum (0.03). This least UV specifies that the species have low or few medicinal uses known to the local informants (Table 2).
Relative frequency of citation
Apteranthes tuberculata was found to have the highest RFC (0.147), followed by Momordica charantia (0.11), Zygophyllum indicum (0.092), and Withania coagulans (0.078) (Table 1). The least RFC was observed for Brassica rapa, Capsicum baccatum, Tamarix aphylla, and Calotropis procera, respectively (Table 2).
Fidelity level (FL %)
FL indicates the primary participants' choice of a potential plant species to treat a given disease. Fidelity levels ranged from 3.70 % to 94.44 % in the present study. Maximum value of FL (94.44%) was recorded for Apteranthes tuberculata, Zygophyllum indicum (94.11), Citrullus colocynthis (88.88), and Abelmoschus esculentus (83.3) for treating diabetes, skin and wounds. However, Ligustrum vulgare (3.70), Momordica charantia (4.76), and Olea europaea (5.55) had the lowest FL values (Table 2).
Informant consensus factor (FIC)
For calculating informant consensus factor (FIC) to various ailment categories 346 use reports were observed for diabetes followed by Skin disorders (195 use reports), wounds (78 use reports), teeth (48 use reports), sexual disorders (40 use reports) and cardiovascular disorders [22] (Table 1). During the present study, it has been noted that diabetes has high Fic value (0.89) followed by dermatological disorders (0.86 each). The lowest value was observed for cardiovascular disorders (0.33).
Diversity of medicinal plant species recorded and their taxonomy
A total of 38 plant species from 29 families were identified, and local people frequently utilized these to cure diabetes. Most plant species that have been identified are members of the Oleaceae family. The remaining plant species have been divided into the following families: Cucurbitaceae, Solanaceae, and Asteraceae (Fig. 4). Medicinal plant species that have been most frequently cited were Apteranthes tuberculata, Momordica charantia, Zygophyllum indicum and Withania coagulans (Table 2).

Dominant antidiabetic medicinal plant families of the study area
Plant parts used
The primary participants in the area mainly utilized leaves, stems, bark, and roots of plants for the manufacture of herbal treatments. The most common medicinal part among the plant parts that have been reported is the leaf, which is followed by the stem, bark, whole plant, seeds, and fruits, in that order (Fig. 5).

Medicinal plant parts in the herbal formulation against Diabetes
Habit forms
The majority of the medicinal plant species in the study area have been from woody plant species, specifically trees (17 species). They made up as much as 44% of all plant forms. Herbs with (13 species) comprise the second highest followed by shrubs (6 species), climbers, and runners each with 1 species respectively (Fig. 6).

Habits of antidiabetic medicinal plants species
Mode of preparation
The primary participants most frequently used the following methods to prepare herbal medicines: powder [19], fresh [16], juice [15], and decoction [11] (Fig. 7).

Mode of utilization of medicinal plants
Dosage and toxicity
In most cases, the recipes were administered trice and twice a day, at breakfast, lunch, and dinner. Some of these were taken before breakfast, and some after. Most of the primary participants mentioned using traditional remedies after lunch and dinner. In a few instances, toxicity reports have also indicated that long-term usage of Azadirachta indica causes a rise in uric acid levels in the bloodstream. Momordica charantia and Eriobotrya japonica have been linked to difficulties such as elevated heart rate and stomach issues.
Review results
Many plant species such as A. vera, B. rapa, C. colocynthis, A. tuberculata, and C. papaya, etc were analyzed for in-vivo antidiabetic activities. For in-vitro and in-vivo activity, a total of 36 plant species from 28 distinct families were recorded. Thirty-five (35) plant species were evaluated for in-vivo animal studies and 28 for in-vitro anti-enzymatic activities. Among these families, Oleaceae and Solanaceae were dominant with 4 and 3 plant species followed by Meliaceae and Solanaceae with 2 species each. The rest of the families were reported with one plant species. Different plant parts were found to be utilized for antidiabetic potentials. Leaf as plant part reported mostly followed by fruit and seed. Leaf was used 14 times and fruit 9. Ethanolic, aqueous, and methanolic were among the leading solvents used for the formulation of extracts. The result from the literature also reveals that phenolic, flavonoids, alkaloids, and terpenoids were reported mostly from phytochemical analysis (Table 3).
In-vitro antidiabetic activity reveals that C. colocynthis and O. europaea showed the highest zone of inhibition against a-amylase (210%) and a-glucosidase (355% and 204%) respectively. C. baccatum against a-amylase showed a 143% zone of inhibition while F. carica with 104% (Table 3). However, two plant species reported in the survey that is Buxus wallichiana Baill and Launaea nudicaulis (L.) found to have rare data regarding in-vivo and in-vitro anti-diabetic activities.
Discussion
The present study revealed that people who are local inhabitants have great traditional knowledge regarding plants having medicinal potential. The study was based on traditional uses of plants used against diabetes by local people. Data revealed that people preferred plants over modern drugs to treat diabetes. The plants are safe and productive.
The study was conducted randomly from different areas of District Karak to explore that not only local healers used these plants but also common people who did not practice medicine have great knowledge of plants having anti-diabetic properties. In the present study total of 346 respondents (211 male and 135 female) participated in collecting usual information about the use of herbal medicines. The data was divided into different modules based on their age, education, and occupation. According to [96, 97], a total of 67 informants out of 103 individuals (response rate: 69%) from nine ethnic groups were interviewed; 70% of the informants were men and 30% were women. A study was conducted by [98] and reported a total of 150 respondents (100 females and 50 males). They participated while collecting information regarding multiple diseases including diabetes, gastrointestinal, and urinary tract infections. Our results agreed with [99] where males were the major respondents.
The results of the present study show that the maximum use values (UV) were noted for Brassica rapa, Melia azedarach, and Calotropis procera [1] while Apteranthes tuberculata (0.147) followed by Momordica charantia (0.11), Zygophyllum indicum (0.092) and Withania coagulans (0.078). In 2019 [100] applied UV and RFC on the collected data and reported the highest RFC for Adiantum venustum (0.27) used in the form of paste for wound healing properties, Artemisia fragrans (0.25) used in the treatment of boils, similarly Aconitum chasmanthum (0.24) used as a decoction for treatment of mumps and measles. The UV recorded highest for Pisum sativum (0.143), Cynodon dactylon (0.125) and Adiantum venustum had a very low use value (0.021).
Among all modes of preparation, powder was most preferable. The results of the study conducted in Northern Pakistan by [100] reported that in various preparation methods, the powder was most frequently used.
According to the current study, the percentages of plant parts that are used are as follows: 68% for leaves, 47% for fruits, 21% for seeds, 7% for flowers and whole plants, and 4% for rhizomes and areal stems with branches. According to a study by [101] leaves (90%) fruits and roots (16%), seeds, and entire plants (8%), each. This is beneficial in terms that plants may not be damaged as leaves were removed from plants rather than stem and root. In another study, the most common ingredient utilized to prepare traditional medicines was leaves. Rich in several phytochemicals, including tannins, glycosides, alkaloids, and saponins, leaves are readily available [102].
Trees and Herbs were major life forms of plant species used as antidiabetic medicine. These findings were in accordance with many other surveys documented for monoherbal recipes where trees and herbs were the dominant plant status [103, 104]. It may be because traditional healers have access to a large number of trees or herbs that are natural.
In the current survey, 38 plant species belonging to 29 families were recognized which were frequently used by inhabitants to treat diabetes. Among these 29 families, four families Oleaceae, Cucurbitaceae, Solanaceae, and Asteraceae were dominant. According to [105] families that were frequently cited are Solanaceae and Moraceae followed by Apiaceae, Cucurbitaceae, Euphorbiaceae, and Fabaceae. The remaining families contributed a minor role in the ailment of diseases traditionally.
The species that the inhabitants preferred to treat specific diseases based on their level of fidelity. There were significant variations in the documented species' fidelity levels for a specific disease. Among the species that have been reported, a maximum value of FL (94.44%) was recorded for A. tuberculata, Z. indicum (94.11), C. colocynthis (88.88), and A. esculentus (83.3) for treating diabetes, skin and wounds. On the other hand, the least FL was recorded for L. vulgare (3.70), M. charantia (4.76) and O. europaea 5.55 respectively.
According to a study conducted in 2023, Berberis lycium had the highest FL value (89.9%) when used to treat ulcers and stomach pain. Decaspermum blancoi came in second with an FL value of 62.2 percent when treating diarrhea and abdominal pain, and Sageretia thea and Solanum nigrum each had an FL value of 53.3% when treating hepatitis and blood purification, respectively. However, the Xanthium strumarium, Cephalanthera longifolia, and Astragalus grahamianus showed the lowest fidelity level [106].
FL ranged from 28 to 100%. The plant species mostly used in the study area with 100% fidelity level were Aesculus indica, Amaranthus viridis, Artemisia scoparia, Cedrus deodara, Chenopodium botrys, Jasminum humile, Malva sylvestris, Layia chrysanthemoides, Thalictrum foliolosum, and Urtica dioica [107].
In the present study, the ICF values for different ailment categories treated by the local informants in this survey ranged from 0.33 to 0.89. Diabetes, skin, wounds, and respiratory 0.89, 0.86, and 0.81 ICF, respectively, were ranked as the most popular ailment categories for medicinal plants in this region. Diabetes disorder scored the highest ICF (0.89). This unexpected result is due to the high use report of few medicinal plants for treating diabetes mellitus such as Apteranthes tuberculata, Zygophyllum indicum, Citrullus colocynthis, and Abelmoschus esculentus with 346, 195, 78, and 61 use reports, respectively.
The condition with the greatest ICF was diabetes (0.92). This surprising outcome can be attributed to the high number of reported uses of a select few medicinal herbs, such as Tecomella undulata, Berberis integerrima, and Citrullus colocynthis, which had 91, 61, and 41 usage reports, respectively, for treating diabetes mellitus. In this instance, the antidiabetic qualities of C. colocynthis, a well-known medicinal plant in the province of Kerman, are well documented [108].
These findings are due to high-use reports for plant species such as Calotropis procera, Pergularia tomentosa, Rhazya srticta, and Tecomella undulata in the treatment of eczema, wound healing, and other skin disorders]. A different study found that endocrine problems had a high FIC value (0.90), followed by fever (0.88), gastrointestinal disorders, and dangerous bites. The dental care category has the lowest value (0.60) [109].
Compounds reported in A. tuberculata such as pregnane glycosides, and flavone glycosides have anti-diabetic properties [110]. Bioactive polysaccharides such as rhamnose and galacturonic acid belong to the class carbohydrates found in A. esculantus (okra) and reportedly have biological functions in the body [111]. Another study [112] reported compounds like pectin, guar gum, and carboxymethylcellulose (CMC) add good results in various conditions like hyperlipidemia and diabetes. Saponin a natural product found in C. colocynthis has the anti-hyperglycemic effect and may interact with many metabolic pathways or insulin metabolism. It also affects glucose homeostasis directly or indirectly [113]. A compound isolated from M. charantia L. named charantin is documented to have insulin-like activity by promoting the release of insulin and decelerating glucogenesis [114].
Numerous plant species, including A. vera, B. rapa, C. colocynthis, A. tuberculata, and C. papaya, among others, were tested for their in-vivo antidiabetic properties, according to the review results. For in-vivo and in-vitro activity, a total of 36 plant species from 29 distinct families were described. For in-vivo animal research, 35 plant species were assessed, and 28 were investigated for their in vitro anti-enzymatic properties. With four and three plant species, respectively, Oleaceae and Solanaceae were the most numerous of these families, followed by Meliaceae and Solanaceae with two species apiece. A study by [115] found that 255 plant species from 70 families were recorded. It was claimed that the two most represented families are Compositae and Lamiaceae. Most Moroccans use Artemisia herba-alba, Nigella sativa, Olea europaea, Marrubium vulgare, Trigonella foenum-graecum, and Allium cepa as common plant species.
Conclusions and recommendations
Having assessed, the ethnopharmacological properties of antidiabetic medicinal plants has provided valuable insights into the traditional diabetes management practices in the study area. The present study highlights the importance of indigenous wisdom in preventing diabetes and identifies several plants that may have anti-diabetic properties. The findings of our study bridge the gap between traditional and modern medicine, encouraging further investigation and validation of these plants' therapeutic effects through in-vivo, in-vitro, and phytochemical activities.
Validating the anti-diabetic properties of identified medicinal plants requires rigorous scientific research. For instance, phytochemical analysis and bioassays may be conducted to understand the active compounds causing the observed effects. Furthermore, the findings of this study support the initiation of clinical trials to examine the safety, efficacy, and optimal dosage of the most promising antidiabetic herbs. The study proposes standard protocols for preparing and administering herbal remedies to ensure consistency and quality control. Moreover, it is also important to promote the cultivation of medicinal plants to reduce pressure on wild populations and ensure a sustainable supply.
To summarize, ethnopharmacological assessment of antidiabetic medicinal plants offers significant potential for diabetes management. By respecting traditional knowledge, conducting rigorous research, and implementing appropriate regulatory measures, we can harness the potential of investigated medicinal plants and improve diabetes care.
Availability of data and materials
The article contains all the data generated or analyzed during this study. Upon request, we will make the materials and data of our study available to other researchers from the principal author (Ms. Amina Nazar amnanazarktk@gmail.com).
References
Khosravi-Boroujeni H, Sarrafzadegan N, Mohammadifard N, Sajjadi F, Maghroun M, Asgari S, Rafieian-Kopaei M, Azadbakht L. White rice consumption and CVD risk factors among Iranian population. J Health Popul Nutr. 2013;31(2):252.
Joseph B, Jini D. Antidiabetic effects of Momordica charantia (bitter melon) and its medicinal potency. Asian Pac J Trop Dis. 2013;3(2):93–102.
Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, Shaw JE. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract. 2014;103(2):137–49.
Boden G, Shulman GI. Free fatty acids in obesity and type 2 diabetes: defining their role in the development of insulin resistance and β-cell dysfunction. Eur J Clin Pharmacol. 2002;32:14–23.
Sy GY, Cissé A, Nongonierma RB, Sarr M, Mbodj NA, Faye B. Hypoglycaemic and antidiabetic activity of acetonic extract of Vernonia colorata leaves in normoglycaemic and alloxan-induced diabetic rats. J Ethnopharmacol. 2005;98(1–2):171–5.
Ogurtsova K, Guariguata L, Barengo NC, Ruiz PL, Sacre JW, Karuranga S, Sun H, Boyko EJ, Magliano DJ. IDF diabetes Atlas: Global estimates of undiagnosed diabetes in adults for 2021. Diabetes Res Clin Pract. 2022;183:109118.
Wagman AS, Nuss JM. Current therapies and emerging targets for the treatment of diabetes. Curr Pharm Des. 2001;7(6):417–50.
Al-Rowais NA. Herbal medicine in the treatment of diabetes mellitus. Saudi Med J. 2002;23(11):1327–31.
Azeem S, Khan U, Liaquat A. The increasing rate of diabetes in Pakistan: a silent killer. Ann Med Surg (Lond). 2022;79:103901. https://doi.org/10.1016/j.amsu.2022.103901.
Roglic G, editor. Global report on diabetes. World Health Organization; 2016;1(1):3-8.
International Diabetes Federation. IDF Diabetes Atlas. 9th ed. 2019. Brussels, Belgium; 2021. Available online at: https://www.diabetesatlas.org. Accessed 06 June 2023.
Adnan M, Aasim M. Prevalence of type 2 diabetes mellitus in adult population of Pakistan: a meta-analysis of prospective cross-sectional surveys. Ann Glob Health. 2020;86(1):1–8.
Shera AS, Jawad F, Maqsood A. Prevalence of diabetes in Pakistan. Diabetes Res Clin Pract. 2007;76(2):219–22.
Jayawardena R, Ranasinghe P, Byrne NM, Soares MJ, Katulanda P, Hills AP. Prevalence and trends of the diabetes epidemic in South Asia: a systematic review and meta-analysis. BMC Public Health. 2012;12(1):1–1.
Nimenibo-Uadia R. Effect of aqueous extract of Canavalia ensiformis seeds on hyperlipidaemia and hyperketonaemia in alloxan-induced diabetic rats. Biokemistri. 2003;15(1):7–15.
Mannan A, Rupa BA, Azam NK, Ahmed N, Hasan N. A quick review on anti-diabetic plants and action of phytochemicals. Int J Adv Res. 2014;2:227.
Ponnusamy S, Ravindran R, Zinjarde S, Bhargava S, Ravi Kumar A. Evaluation of traditional Indian antidiabetic medicinal plants for human pancreatic amylase inhibitory effect of in-vitro. J Evid-Based Complement Altern Med. 2010; 2011(10). https://doi.org/10.1155/2011/515647.
Zaman K. Medicinal plants with hypoglycemic activity. J Ethnopharmacol. 1989;26(1):1–55.
Hussain AI, Rathore HA, Sattar MZ, Chatha SA, Sarker SD, Gilani AH. Citrullus colocynthis (L.) Schrad (bitter apple fruit): a review of its phytochemistry, pharmacology, traditional uses and nutritional potential. J Ethnopharmacol. 2014;155(1):54–66.
Khan HB, Vinayagam KS, Palanivelu S, Panchanatham S. Anti-diabetic effect of Semecarpus anacardium Linn nut milk extract in a high fat diet STZ-induced type 2 diabetic rat model. Comp Clin Path. 2012;21:1395–400.
Patel V, Sharma V. Antioxidant and antidiabetic effect of capparis spinosa linn in streptozotocin induced diabetic rats. Eur J Biomed Pharm Sci. 2015;2:308–18.
Murad W, Azizullah A, Adnan M, Tariq A, Khan KU, Waheed S, Ahmad A. Ethnobotanical assessment of plant resources of Banda Daud Shah, district Karak Pakistan. J Ethnobiol Ethnomed. 2013;9:1.
Khan M, Hussain F, Musharaf S. Ethnobotanical profile of Tehsil Takht-e-Nasratti, District Karak Pakistan. J Med Plant Res. 2013;7(22):1636–51.
Espinosa MM, Bieski IGC, Martins DTO. Sampling in Ethnobotanical Studies of Medicinal Plants. In: Albuquerque U, Cruz da Cunha L, de Lucena R, Alves R, (eds). Methods and Techniques in Ethnobiology and Ethnoecology. Springer Protocols Handbooks. New York, NY: Humana Press. https://doi.org/10.1007/978-1-4614-8636-7_13.
International Society of Ethnobiology. ISE Code of Ethics. Department of Anthropology. University of Florida, USA. 2006. Available online at: https://www.ethnobiology.net/what-we-do/core-programs/ise-ethics-program/code-ofethics/. Accessed on 12 Jul 2023.
Hoffman B, Gallaher T. Importance indices in ethnobotany. Ethnobot Res Appl. 2007;5:201–18.
Ugulu I, Baslar S, Yorek N, Dogan Y. The investigation and quantitative ethnobotanical evaluation of medicinal plants used around Izmir province Turkey. J Med Plant Res. 2009;3(5):345–67.
Tardío J, Pardo-de-Santayana M. Cultural importance indices: a comparative analysis based on the useful wild plants of Southern Cantabria (Northern Spain). Econ Bot. 2008;62:24–39.
Bibi Y, Tabassum S, Zahara K, Bashir T, Haider S. Ethnomedicinal and pharmacological properties of Caralluma tuberculata NE Brown-A review. Pure Appl Biol. 2015;4(4):503.
Friedman J, Yaniv Z, Dafni A, Palewitch D. A preliminary classification of the healing potential of medicinal plants, based on a rational analysis of an ethnopharmacological field survey among Bedouins in the Negev Desert Israel. J Ethnopharmacol. 1986;16(2–3):275–87.
Shil S, Choudhury MD, Das S. Indigenous knowledge of medicinal plants used by the Reang tribe of Tripura state of India. J Ethnopharmacol. 2014;152(1):135–41.
Heinrich M, Edwards S, Moerman DE, Leonti M. Ethnopharmacological field studies: a critical assessment of their conceptual basis and methods. J Ethnopharmacol. 2009;124(1):1–7.
Rashid S, Ahmad M, Zafar M, Sultana S, Ayub M, Khan MA, Yaseen G. Ethnobotanical survey of medicinally important shrubs and trees of Himalayan region of Azad Jammu and Kashmir Pakistan. J Ethnopharmacol. 2015;166:340–51.
Hbika A, Daoudi NE, Bouyanzer A, Bouhrim M, Mohti H, Loukili EH, Mechchate H, Al-Salahi R, Nasr FA, Bnouham M, Zaid A. Artemisia absinthium L. Aqueous and ethyl acetate extracts: Antioxidant effect and potential activity in vitro and in vivo against pancreatic α-amylase and intestinal α-glucosidase. Pharmaceutics. 2022;14(3):481.
Abo-Youssef AM, Messiha BA. Beneficial effects of Aloe vera in treatment of diabetes: comparative in vivo and in vitro studies. Bull Faculty Pharm Cairo Univ. 2013;51(1):7–11.
Muñiz-Ramirez A, Perez RM, Garcia E, Garcia FE. Antidiabetic activity of Aloe vera leaves. J Evid Based Complementary Altern Med. 2020;2020(9):1–9.
Satyanarayana K, Sravanthi K, Shaker IA, Ponnulakshmi R. Molecular approach to identify antidiabetic potential of Azadirachta indica. J Ayurveda Integr Med. 2015;6(3):165.
Shaheen G. Phytochemical Screening, Anti-Oxidant and Enzymatic Activity of Azadirachta Indica. J Xi’an Shiyou Univ Nat Sci Ed. 2022;18(12):421–34.
Yaradua I, Ibrahim M, Matazu KI, Nasir A, Matazu NU, Zainab AS, Abdul Rahman MB, Bilbis L, Abbas AY. Antidiabetic activity of Abelmoschus esculentus (Ex-Maradi Okra) fruit in alloxan-induced diabetic rats Niger. J Biochem Mol Biol. 2017;32:44–52.
Chowdhury NS, Jamaly S, Farjana F, Begum N, Zenat EA. A review on ethnomedicinal, pharmacological, phytochemical and pharmaceutical profile of lady’s finger (Abelmoschus esculentus L.) plant. Pharmacol Pharm. 2019;10(02):94–108.
Daryoush M, Bahram AT, Yousef D, Mehrdad N. Brassica rapa L. extract alleviate early hepatic injury in alloxan-induced diabetic rats. J Med Plant Res. 2011;5(31):6813–21.
Ardalani H, Hejazi Amiri F, Hadipanah A, Kongstad KT. Potential antidiabetic phytochemicals in plant roots: a review of in vivo studies. J Diabetes Metab Disord. 2021;12:1–8.
Cao W, Wang C, Mayhesumu X, Pan L, Dang Y, Yili A, Abuduwaili A, Mansur S. Isolation, Structural Elucidation, Antioxidant and Hypoglycemic Activity of Polysaccharides of Brassica rapa L. Molecules. 2022;27(9):3002.
Aldughaylibi FS, Raza MA, Naeem S, Rafi H, Alam MW, Souayeh B, Farhan M, Aamir M, Zaidi N, Mir TA. Extraction of bioactive compounds for antioxidant, antimicrobial, and antidiabetic applications. Molecules. 2022;27(18):5935.
Roy S, Sehgal R, Padhy BM, Kumar VL. Antioxidant and protective effect of latex of Calotropis procera against alloxan-induced diabetes in rats. J Ethnopharmacol. 2005;102(3):470–3.
Benariba N, Djaziri R, Bellakhdar W, Belkacem N, Kadiata M, Malaisse WJ, Sener A. Phytochemical screening and free radical scavenging activity of Citrullus colocynthis seeds extracts. Asian Pac J Trop Biomed. 2013;3(1):35–40.
Ghauri AO, Ahmad S, Rehman T. In vitro and in vivo anti-diabetic activity of Citrullus colocynthis pulpy flesh with seeds hydro-ethanolic extract. J Complement Integr Med. 2020;17(2):20180228.
Jayaraman R, Shivakumar A, Anitha T, Joshi VD, Palei NN. Antidiabetic effect of petroleum ether extract of Citrullus colocynthis fruits against streptozotocin-induced hyperglycemic rats. Rom J Biol-Plant Biol. 2009;4:127–34.
Kaskoos RA. GC/MS Profile and in-vitro Antidiabetic Activity of Cinnamomum z eylanicum Blume., Bark and Trachyspermum ammi (L.) Sprague Seeds. J Essent Oil-Bear Plants. 2019;22(2):535–44.
Sultan K, Zakir M, Khan H, Khan IU, Rehman A, Akber NU, Muhammad N, Khan MA. The effect of extract/fractions of Caralluma tuberculata on blood glucose levels and body weight in alloxan-induced diabetic rabbits. J Evid Based Complement Altern Med. 2014;19(3):195–9.
Rathee S, Mogla OP, Sardana S, Vats M, Rathee P. Antidiabetic activity of Capparis decidua Forsk Edgew. J Pharm Res. 2010;3:231–4.
Mohammed A, Koorbanally N, Md SI. Anti-diabetic effect of Capsicum annuum L. fruit acetone fraction in a type 2 diabetes model of rats. Acta poloniae pharmaceutica. 2017;74(6):1767–79.
Sricharoen P, Lamaiphan N, Patthawaro P, Limchoowong N, Techawongstien S, Chanthai S. Phytochemicals in Capsicum oleoresin from different varieties of hot chilli peppers with their antidiabetic and antioxidant activities due to some phenolic compounds. Ultrasonics Sonochem. 2017;38:629–39.
Solikhah TI, Setiawan B, Ismukada DR. Antidiabetic activity of papaya leaf extract (Carica Papaya L.) isolated with maceration method in alloxan-induces diabetic mice. Syst Rev Pharm. 2020;11(9):774–8.
Liu Y, Zhang W, Xu C, Li X. Biological activities of extracts from loquat (Eriobotrya japonica Lindl.): a review. Int J Mol Sci. 2016;17(12):1983.
Kamran SH, Shoaib RM, Ahmad M, Ishtiaq S, Anwar R. Antidiabetic and renoprotective effect of Fagonia cretica L. methanolic extract and Citrus paradise Macfad. juice in alloxan induced diabetic rabbits. J Pharm Pharmacogn Res. 2017;5(6):365–80.
Anil P, Nikhil B, Manoj G, Prakash N. Phytochemicals and biological activities of Fagonia indica. Int Res J Pharm. 2012;3(6):56–9.
Mopuri R, Ganjayi M, Meriga B, Koorbanally NA, Islam MS. The effects of Ficus carica on the activity of enzymes related to metabolic syndrome. J Food Drug Anal. 2018;26(1):201–10.
Lin L, Zhang Y. Chemical Constituents and Antidiabetic Activity of Dichloromethane Extract from Ficus carica Leaves. Diabetes Metab Syndr Obes. 2023;979–91:16.
Minaiyan M, Ghannadi A, Movahedian A, Hakim-Elahi I. Effect of Hordeum vulgare L.(Barley) on blood glucose levels of normal and STZ-induced diabetic rats. Res Pharm Sci. 2014;9(3):173.
Hamli S, Kadi K, Addad D, Bouzerzour H. Phytochemical screening and radical scavenging activity of whole seed of durum wheat (Triticum durum Desf.) and barley (Hordeum vulgare L.) varieties. Jordan J Biol Sci. 2017;10(4):323–7.
Venkatachalam T, Kumar VK, Selvi PK, Maske AO, Anbarasan V, Kumar PS. Antidiabetic activity of Lantana camara Linn fruits in normal and streptozotocin-induced diabetic rats. J Pharm Res. 2011;4(5):1550–2.
Czerwińska ME, Gąsińska E, Leśniak A, Krawczyk P, Kiss AK, Naruszewicz M, Bujalska-Zadrożny M. Inhibitory effect of Ligustrum vulgare leaf extract on the development of neuropathic pain in a streptozotocin-induced rat model of diabetes. Phytomedicine. 2018;49:75–82.
Madhuri AS, Mohanvelu R. Evaluation of antidiabetic activity of aqueous extract of Mangifera indica leaves in alloxan induced diabetic rats. Biomed Pharmacol J. 2017;10(2):1029–35.
Ngo DH, Ngo DN, Vo TT, Vo TS. Mechanism of action of Mangifera indica leaves for anti-diabetic activity. Scientia Pharmaceutica. 2019;87(2):13.
Mohammady I, Elattar S, Mohammed S, Ewais M. An evaluation of anti-diabetic and anti-lipidemic properties of Momordica charantia (Bitter Melon) fruit extract in experimentally induced diabetes. Life Sci J. 2012;9(2):363–74.
Daniel P, Supe U, Roymon MG. A review on phytochemical analysis of Momordica charantia. Int J Adv Pharm Biol Chem. 2014;3(1):214–20.
Tende JA, Ezekiel I, Dikko AA, Goji AD. Effect of ethanolic leaves extract of Moringa oleifera on blood glucose levels of streptozocin-induced diabetics and normoglycemic Wistar rats. Br J Pharmacol Toxicol. 2011;2(1):1–4.
Khan MF, Rawat AK, Khatoon S, Hussain MK, Mishra A, Negi DS. In vitro and in vivo antidiabetic effect of extracts of Melia azedarach, Zanthoxylum alatum, and Tanacetum nubigenum. Integr Med Res. 2018;7(2):176–83.
Safithri M, Sari YP. Inhibition of α-glucosidase activity by ethanolic extract of Melia azedarach L. leaves. InIOP Conference Series. 2016;31(1):12–25.
Abbasnezhad A, Niazmand S, Mahmoudabady M, Rezaee SA, Soukhtanloo M, Mosallanejad R, Hayatdavoudi P. Nigella sativa L. seed regulated eNOS, VCAM-1 and LOX-1 genes expression and improved vasoreactivity in aorta of diabetic rat. J Ethnopharmacol. 2019;228:142–7.
Tiji S, Bouhrim M, Addi M, Drouet S, Lorenzo JM, Hano C, Bnouham M, Mimouni M. Linking the phytochemicals and the α-glucosidase and α-amylase enzyme inhibitory effects of Nigella sativa seed extracts. Foods. 2021;10(8):2–19.
Liaqat S, Islam M, Saeed H, Iqtedar M, Mehmood A. Investigation of Olea ferruginea Roylebark extracts for potential in vitroantidiabetic and anticancer effects. Turk J Chem. 2021;45(1):92–103.
Turk J Chem. 2021;45(1):92-103.
Mansour HM, Zeitoun AA, Abd-Rabou HS, El Enshasy HA, Dailin DJ, Zeitoun MA, El-Sohaimy SA. Antioxidant and Anti-Diabetic Properties of Olive (Olea europaea) Leaf Extracts: In Vitro and In Vivo Evaluation. Antioxidants. 2023;12(6):1275.
Hwang SH, Kang IJ, Lim SS. Antidiabetic effect of fresh nopal (Opuntia ficus-indica) in low-dose streptozotocin-induced diabetic rats fed a high-fat diet. J Evid Based Complementary Altern Med. 2017;2017:1–8.
Chintu RK, Patel UD, Chauhan VB, Patel HB, Chirag M, Modi PR, Pandya KB, Shah TM. In-vitro antioxidant and antidiabetic activity of hydro alcoholic extract of Opuntia elatior fruit as well as quercetin. Int J Environ Sci Technol. 2017;6(2):1028–35.
Eidi A, Eidi M, Darzi R. Antidiabetic effect of Olea europaea L. in normal and diabetic rats. Phytother Res. 2009;23(3):347–50.
Khan Y, Panchal S, Vyas N, Butani A, Kumar V. Olea europaea: a phyto-pharmacological review. Pharmacognosy Rev. 2007;1(1):114–8.
Ahamad J, Uthirapathy S, Ameen MS, Anwer ET, Hussain FH, Mir SR. Chemical composition and in vitro antidiabetic effects of Olea europaea Linn.(Olive). Curr Bioactive Compounds. 2020;16(8):1157–63.
Vlavcheski F, Young M, Tsiani E. Antidiabetic effects of hydroxytyrosol: In vitro and in vivo evidence. Antioxidants. 2019;8(6):4–20.
Patel VS, Chitra V, Prasanna PL, Krishnaraju V. Hypoglycemic effect of aqueous extract of Parthenium hysterophorus L. in normal and alloxan induced diabetic rats. Indian J Pharmacol. 2008;40(4):183–5.
Oh WK, Lee CH, Lee MS, Bae EY, Sohn CB, Oh H, Kim BY, Ahn JS. Antidiabetic effects of extracts from Psidium guajava. J Ethnopharmacol. 2005;96(3):411–5.
Manikandan R, Balamuralikrishnan B, Boro A, Karthika P, Arun M, Velayuthaprabhu S, Malaisamy A, Rengarajan RL, Anand AV. Impact on cardioprotective effect of Psidium guajava leaves extract in streptozotocin-induced Wistar mice with molecular in silico analysis. Qual Assurance Saf Crops Foods. 2023;15(2):209–21.
Khalil EA. Antidiabetic effect of an aqueous extract of Pomegranate (Punica granatum L.) peels in normal and alloxan diabetic rats. Egypt J Hosp Med. 2004;16(1):92–9.
Mayasankaravalli C, Deepika K, Lydia DE, Agada R, Thagriki D, Govindasamy C, Chinnadurai V, Gatar OM, Khusro A, Kim YO, Kim HJ. Profiling the phyto-constituents of Punica granatum fruits peel extract and accessing its in-vitro antioxidant, anti-diabetic, anti-obesity, and angiotensin-converting enzyme inhibitory properties. Saudi J Biol Sci. 2020;27(12):3228–34.
Ahmed A, Asad MJ, Ahmad MS, Qureshi R, Shah SI, Gul H, Gulfraz M. Antidiabetic and hypolipidemic potential of Rhazya stricta Decne extract and its fractions. Int Curr Pharm J. 2015;4(2):353–61.
Umamageswari MS, Karthikeyan TM, Maniyar YA. Antidiabetic activity of aqueous extract of Solanum nigrum linn berries in alloxan induced diabetic wistar albino rats. J Clin Diagnostic Res. 2017;11(7):16–9.
Ullah R, Tariq SA, Khan N, Sharif N, Din ZU, Mansoor K. Antihyperglycemic effect of methanol extract of Tamarix aphylla L. Karst (Saltcedar) in streptozocin–nicotinamide induced diabetic rats. Asian Pac J Trop Biomed. 2017;7(7):619–23.
Nguyen TK, Im KH, Choi J, Shin PG, Lee TS. Evaluation of antioxidant, anti-cholinesterase, and anti-inflammatory effects of culinary mushroom Pleurotus pulmonarius. Mycobiology. 2016;44(4):291–301.
Kumar GP, Arulselvan P, Kumar DS, Subramanian SP. Anti-diabetic activity of fruits of Terminalia chebula on streptozotocin induced diabetic rats. J Health Sci. 2006;52(3):283–91.
Chang CL, Lin CS. Phytochemical composition, antioxidant activity, and neuroprotective effect of Terminalia chebula Retzius extracts. J Evid Based Complement Altern Med. 2012;2012:1–7.
Shukla K, Dikshit P, Shukla R, Gambhir JK. The aqueous extract of Withania coagulans fruit partially reverses nicotinamide/streptozotocin-induced diabetes mellitus in rats. J Med Food. 2012;15(8):718–25.
Meeran SB, Subburaya U, Narasimhan G. In silico and in vitro screening of ethanolic extract of fruits of Withania coagulans against diabetes. Res J Pharm Technol. 2020;13(2):631–5.
Aggarwal B, Sharma P, Lamba H. Ethanobotanical, phytochemical and pharmacological properties of Zizyphus nummularia (Burm. F.): A Review. Int J Phytomedicine. 2018;10:137–47.
Dubey K, Dubey R, Gupta R, Gupta A. Anti-Diabetic Potential of Aqueous, Methanolic and Saponin Extract of Leaves of Ziziphus nummlaria Linn. J Drug Deliv Ther. 2017;7(7):173–84.
Ahmad L, Riaz M, Jan HA, Semotiuk AJ, Ahmad I, Khan I, Ali F, Rashid W, Bussmann RW. An ethnobotanical survey of wild food plants used by the local communities of Kumrat Valley in District Upper Dir Pakistan. Ethnobot Res Appl. 2021;22:1–3.
Saha S, Bhattacharjee A, Singh BK, Biswas A, Sen S. An ethnobotanical study of the indigenous medicinal knowledge by the rural people in different villages of Agaya Narah Gram Panchayat, West Bengal, India. Plant Biosyst-An Int J Deal Aspects Plant Biol. 2023;157(5):935–8.
Mussarat S, Adnan M, Begum S, Alqarawi AA, Rehman SU, Abd_Allah EF. Diversity of traditionally used polyherbal medicines. Pak J Bot. 2021;53(4):10-30.
Amjad MS, Zahoor U, Bussmann RW, Altaf M, Gardazi SM, Abbasi AM. Ethnobotanical survey of the medicinal flora of Harighal, Azad Jammu & Kashmir Pakistan. J Ethnobiol Ethnomed. 2020;16:1–28.
Malik K, Ahmad M, Zafar M, Ullah R, Mahmood HM, Parveen B, Rashid N, Sultana S, Shah SN. Lubna. An ethnobotanical study of medicinal plants used to treat skin diseases in northern Pakistan. BMC Complement Altern Med. 2019;19:1–38.
Naceiri Mrabti H, Bouyahya A, Naceiri Mrabti N, Jaradat N, Doudach L, Faouzi ME. Ethnobotanical survey of medicinal plants used by traditional healers to treat diabetes in the Taza region of Morocco. J Evid-Based Complement Altern. 2021;26:20211–6.
Passalacqua NG, Guarrera PM, De Fine G. Contribution to the knowledge of the folk plant medicine in Calabria region (Southern Italy). Fitoterapia. 2007;78(1):52–68.
Kadir MF, Sayeed MS, Shams T, Mia MM. Ethnobotanical survey of medicinal plants used by Bangladeshi traditional health practitioners in the management of diabetes mellitus. J Ethnopharmacol. 2012;144(3):605–11.
Tag H, Kalita P, Dwivedi P, Das AK, Namsa ND. Herbal medicines used in the treatment of diabetes mellitus in Arunachal Himalaya, Northeast. India J Ethnopharmacol. 2012;141:786–95.
Ullah I, Ullah I, Ali M, Durrani F, Khan SU, Hussain D, Mehmood S, Khan SU, Ullah M, Hussain K, Bahadur S. Quantitative study of medicinal plants and biological activities of two common species used by inhabitants of district Bannu Pakistan. Acta Ecologica Sinica. 2023;43(2):271–87.
Haq A, Badshah L, Hussain W, Ullah I. Quantitative ethnobotanical exploration of wild medicinal plants of Arang Valley, District Bajaur, Khyber Pakhtunkhwa, Pakistan: a mountainous region of the Hindu Kush Range. Ethnobot Res Appl. 2023;25:1–29.
Hussain S, Hussain W, Nawaz A, Badshah L, Ali A, Ullah S, Ali M, Hussain H, Bussmann RW. Quantitative ethnomedicinal study of indigenous knowledge on medicinal plants used by the tribal communities of Central Kurram, Khyber Pakhtunkhwa Pakistan. Ethnobot Res Appl. 2022;23:1–31.
Ostovan F, Olomi H, Gol A. The Citrullus Colocynthis pulp antioxidant activity on oxidative stress factors of liver in streptozotocin-induced diabetic rats. Physiol Pharmacol. 2014;17(4):388–98.
Remesh M, Al Faify EA, Alfaifi MM, Al Abboud MA, Ismail KS, Al-Namazi AA, Masrahi YS. Ethnobotanical survey of medicinal plants native to the mountains of Jazan, southwestern Saudi Arabia. International Int J Adv Appl Sci. 2023;10(9):218–27.
Alqahtani SN, Alkholy SO, Ferreira MP. Antidiabetic and anticancer potential of native medicinal plants from Saudi Arabia, in Polyphenols in human health and disease. Elsevier; 2014:119-132.
Deters AM, Lengsfeld C, Hensel A. Oligo-and polysaccharides exhibit a structure-dependent bioactivity on human keratinocytes in vitro. J Ethnopharmacol. 2005;102(3):391–9.
Alam MS, Khan GA. Chemical analysis of okra bast fiber (Abelmoschus esculentus) and its physico-chemical properties. J Text Appar Technol Manag. 2007;5(4):1–9.
Prabhakar PK, Doble M. A target based therapeutic approach towards diabetes mellitus using medicinal plants. Curr Diabetes Rev. 2008;4(4):291–308.
Ng TB, Wong CM, Li WW. Yeung HW Insulin-like molecules in Momordica Charantia seeds. J Ethnopharmacol. 1986;15:107–17.
Acknowledgments
This paper is part of Amina Nazar’s PhD thesis. The authors are thankful to Kohat University of Science and Technology for their support. The authors wish to thank the Researchers Supporting Project Number (RSP2024R346) at King Saud University Riyadh Saudi Arabia for financial support.
Author information
Authors and Affiliations
Contributions
A.N. conducted the field survey and wrote the initial draft of the manuscript. M.A., S.M.S, and N. A designed the project and helped in the revision of the manuscript. M.A. also supervised all the stages of the research. A.T., A.B. and R.U. helped in data analysis and review.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethical Committee of Kohat University of Science and Technology Kohat, Pakistan granted ethical approval (Ref. No./KUST/Ethical Committee/729) for this study. Moreover, informed consent have been obtained from the respondents.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nazar, A., Adnan, M., Shah, S.M. et al. Ethnobotanical assessment of antidiabetic medicinal plants in District Karak, Pakistan. BMC Complement Med Ther 24, 173 (2024). https://doi.org/10.1186/s12906-024-04462-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-024-04462-w