
Abstract
Background
Complementary medicine (CM) is frequently used by patients, but little is known about the usage of CM in surgical patients. The study aimed to elucidate the relevance of CM in surgery.
Methods
This cross-sectional, multi-center survey utilized a paper-based questionnaire consisting of 21 questions to capture CM usage and interest as well as CM communication in visceral and thoracic surgical patients being hospitalized at the corresponding departments of surgery at the University Medical Centers in Freiburg, Heidelberg und Ulm, Germany.
Results
Overall, 151 patients consented to the survey. On average, current CM usage was stated by 44% of patients. Most frequently used CM approaches were physical exercise (63%), nutritional supplements (59%) and herbal medicine (56%). Strong interest in CM counselling was stated by 51% of patients. Almost 80% of patients wanted to be treated in a holistic manner and desired for reliable information about CM as well as CM informed physicians. Only 12% of patients communicated CM usage and interest with their attending physician. Review of literature revealed similar results showing an overall CM usage of 43%, preferring nutritional supplements and herbal medicine.
Conclusion
The results of our cross-sectional study indicate a high percentage of CM users and a strong interest in CM among surgical patients. Indeed, the current communication about CM between patients and surgeons is poor. With respect to safety and quality reasons, but also to pay attention to patients’ demands, physicians should be aware of patients’ CM usage in surgery.
Trial registration
German Clinical Trial register (DRKS00015445).
Similar content being viewed by others


Introduction
Cross-sectional surveys indicate experience with complementary medicine (CM) of approximately two thirds of the population in Western countries [1,2,3]. CM consists of different holistic medical approaches such as Traditional Chinese Medicine (TCM), anthroposophic medicine, homeopathy as well as naturopathy. Common therapies of CM are acupuncture, different types of physical exercise, changing of diet and fasting as well as herbal medication. CM is often used independently and without medical consultation [1]. Since the 1970ies frequency of CM usage is increasing, but it depends on patients’ disease as well as on sex and socioeconomic state [4,5,6]. CM is not only used at home as a previous research work by our group suggested also a high CM usage frequency of almost 50% in hospitalized patients [7]. Interestingly, the results of this study indicated that CM might also play a role in surgery [7]. Studies about CM usage in surgery are widely lacking. Two publications from Canada and Hungary indicate a CM usage frequency of 30% in inpatient general surgical patients [8, 9]. A survey examining German orthopedic and trauma surgical patients showed usage rates of 30%, whereas two thirds of patients stated to be interested in CM [10]. Uncontrolled CM treatment in surgery might be a safety issue due to potential interactions and side effects [8, 11, 12]. Recent research suggests an affection of blood coagulation of some herbal medicine potentially leading to higher risk of bleeding intraoperatively [13, 14]. Communication about CM between patients and treating physicians appears to be poor as only a few patients communicate about CM usage, tightening the safety issue [8,9,10, 15,16,17,18]. Moreover, as patient-physician-contacts in surgery appear to be short and ward rounds just last a few minutes in average [19], it is possible that there is a large gap between patients’ CM needs and communication about it in surgery. Beside risks and safety hazards, CM in surgery might also be a chance to improve for example perioperative management of pain and postoperative paralytic ileus [20,21,22]. Due to the challenge of a patient-centered therapy respecting the patient’s individual demands, the relevance of CM in surgery has to be addressed by research. To estimate the relevance of CM in surgery, two central hypotheses were posed – (I) a considerable part of hospitalized surgical patients uses CM during their hospital stay and (II) surgical patients are interested in CM, which should be addressed by a subgroup analysis of a multicenter, multidisciplinary cross-sectional study [7].
Methods
We report about a cross-sectional study. To address the aim of the study, we performed a subgroup analysis of a multicenter, paper-based, multidisciplinary and pseudo-anonymous survey performed at the German University Medical Centers in Freiburg, Heidelberg, Tübingen and Ulm, which was previously reported [7].
Primary aim of the study
The primary aim of the study was to estimate the relevance of CM in surgery. Two central hypotheses were posed – (I) a considerable part of hospitalized surgical patients uses CM during their hospital stay and (II) surgical patients are interested in CM. Secondary aims of the study were the types of used CM, the communication about CM usage as well as patients’ demands and attitudes towards CM.
Survey
Only patients being hospitalized at the normal ward at the department of general and visceral surgery (Freiburg und Ulm) and at the department of thoracic surgery (Heidelberg) between April and December 2018 were eligible for participation. In Tübingen, no surgical patients were surveyed. Patients of all ages, regardless of sex, diagnosis and treatment, being able to speak and understand German (at least B2 level according to the European Framework of Reference for Languages [23]) and to complete a questionnaire on their own, were eligible for participation. Recruiting was carried out consecutively. All patients had to give written informed consent before participation. The study was registered at the German Clinical Trial register (DRKS00015445) and approved by the ethical committee of the University Medical Center of Freiburg, Germany (EK FR 25/17) before onset.
Questionnaire
In absence of a validated questionnaire for surveying CM usage of surgical patients, an existing questionnaire, which previously has been used by the authors, was adjusted [24, 25]. The questionnaire consisted of 21 neutral questions, 15 CM-related and 6 on socio-demographic aspects. Current and previous usage of 21 CM approaches (herbal medicine, balneotherapy, acupuncture/acupressure, mental healing/mindfulness, anthroposophic medicine, homeopathy, physical exercise, aroma therapy, hyperthermia, detoxification, mistletoe, Ayurveda, osteopathy/chiropractic, traditional Chinese medicine (TCM), compresses, colonic cleansing & probiotics, nutritional supplements, diet & nutrition, relaxing/mediation, yoga/qigong, fasting) were evaluated. Furthermore, reasons for and against usage as well as knowledge about CM, interest towards CM and communication about CM usage were inquired. Further information about the questionnaire was previously published [7]. Patients had around 30 min for completing the questionnaires. To avoid manipulation by others, patients had to be able to complete the questionnaire independently and on their own, but they were allowed to ask study staff for help in case of ambiguity. Study staff checked completeness of the questionnaire. In case of incompleteness, the study staff asked the patient to complete the questionnaire independently. The study staff was encouraged to appear friendly but uncommitted.
Statistics
This was an exploratory subgroup analysis. Based on recent publications, a sample-size of at least 100 patients was calculated to predict reliability of multiple logistic regression including 5 predictive variables (age, male vs. female patients, survey location, nationality and diagnosis of cancer), which are well-known variables affecting CM usage with except of survey location [15, 16]. Beside survey location, all other variables are well-known to affect CM usage [26, 27]. Only patients for whom a complete data set was available were evaluated by multiple logistic regression. The Goodness-of-fit was assessed using the Hosmer-Lemeshow-Test (p < 0.05 was considered significant). Data was entered by three authors in a preformed table and database was closed before onset of analysis (IBM SPSS (Version 27.0)). To analyze distribution and for comparison of categorical variables, chi-squared test was used. P < 0.05 was considered significant. Unless otherwise stated, the results are given as a percentage of patients, who have answered a question, or as absolute values. In case of denial to complete the questionnaire, missing data was not complemented.
Results
Overall, 151 out of 224 eligible patients (67%) were willing to participate. Not all of the participating patients responded to all questions. An overview of all responses including also the number of responding patients is shown in Fig. 1.

Overview of all included patients, number of responses and results. (CM = Complementary medicine)
Seventy-eight patients (52%) were male and 136 patients (91%) were German citizens. The second most common nationalities were Turkish (2%) and Italian (2%). The average age of participants was 59 ± 15 years (range 18–86 years). One third of the patients (36%) was hospitalized due to cancer.
CM usage of surgical patients (hypothesis I)
Fifty-seven patients (44%) stated current usage of CM (Fig. 1, A).
Most frequently current or previously used CM approaches were physical exercise (63%), nutritional supplements (59%), herbal medicine (56%), balneotherapy (46%) and homeopathy (45%) (Fig. 2).

Previously and currently used CM approaches in Freiburg (black bar), Heidelberg (light grey bar) and Ulm (dark grey bar)
(Percentage of patients, who replied to the question; TCM = Traditional Chinese Medicine)
CM interest of surgical patients (hypothesis II)
Strong interest in CM counselling was stated by 75 patients (51%). Further 37 patients (25%) were indecisive (Fig. 1, B).
Communication about CM in surgical patients
Only 17 patients (12%) stated to communicate CM usage and interest with their attending physicians (Fig. 1, C). Reasons for non-communication were no time (56%), being afraid of physician’s negative attitude towards CM (20%) and missing competence of the physician (16%).
Further results of survey: demands of patients
Eighty-nine patients (60%) stated to feel little or not at all informed about CM (Fig. 1, D). Reliable information about CM was desired by 114 patients (79%), and 114 patients (78%) stated that physicians should be informed about CM (Fig. 1, E and F). One hundred thirty-three patients (89%) wanted to take over responsibility for treatment decisions, and 129 patients (88%) wanted to be treated in a holistic manner (Fig. 1, G and H).
Further results of survey: factors affecting CM usage and CM communication
Current usage of CM differed between the locations as patients in Freiburg (71%) had a significantly higher CM usage rate compared to patients in Ulm (22%) and Heidelberg (32%, Table 1). In Freiburg, the most frequently used CM approaches were nutritional supplements (68%), homeopathy (65%) and physical exercise (61%). In Heidelberg, the most frequently used CM approaches were nutritional supplements (52%), physical exercise (50%) and herbal medicine (47%) and in Ulm, physical exercise (76%), herbal medicine (62%) and compresses (57%). Usage frequency of all surveyed CM approaches subdivided by survey location is shown in Fig. 1. The survey location had a significantly influence on CM usage rate (p = 0.001, Table 2) and CM communication (p = 0.048, Table 3).
Significantly more patients in Heidelberg felt little or not at all informed about CM compared to Freiburg und Ulm (80% vs. 60% and 59%, p = 0.020, Table 1). Patients in Heidelberg suffered significantly more frequently from cancer (32% vs. 27% and 20%, p < 0.001), but multiple logistic regression did not reveal an influence of cancer diagnosis on frequency of current CM usage (Table 2).
CM communication was more likely in patients with diagnosis of cancer (p = 0.018, Table 3).
All results of multiple logistic regression considering factors, which might be able to affect CM usage and CM communication are shown in Tables 2 and 3.
Discussion
This is the first survey assessing CM usage and interest amongst patients hospitalized at surgical departments of University Medical Centers in Germany. We found almost half of the patients stating a current CM usage during their hospital stay; physical exercise, herbal medicine and dietary supplements were most frequently used.
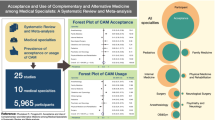
Similar to the results of our survey, literature review revealed an average CM usage frequency of approximately 43% in surgical patients of all disciplines (Table 4). CM usage of surgical patients varies internationally between 16 and 75%, depending among others on country and definition of CM. A variety of surveys indicate a higher CM affinity of women [8, 10, 28,29,30], but we found no influence of sex on CM usage frequency. As shown in Table 4, recent research suggests that the focus of patient-selected CM is on herbal medicine and dietary supplements, which is also confirmed by the results of our survey. Patients often consider CM, especially herbal medicine and dietary supplements, as safe and harmless [10, 31, 32]. The risk of CM interventions, especially of herbal medicine and dietary supplements, is still a matter of scientific discussion. Herbal medicine and dietary supplements may cause side-effects or interactions, but evidence is mostly lacking and serious CM-related risks appear to be at least unlikely [33,34,35,36]. Potential interactions being relevant in surgery are effects on blood coagulation as wells as anesthesia-related risks such as arrhythmogenic potential and interactions with membrane receptors. Recent literature recommends to stop intake of herbal medication and dietary supplements with a related risk profile before surgery [11, 21, 37]. On the other hand, CM might improve self-management and patient-centered care and offers promising approaches for the treatment of typical postoperative complaints such as nausea and vomiting, pain and sleep disturbances which might be integrated into daily surgical practice [21]. Recent surveys indicate that approximately two thirds of surgical patients in Western countries are interested in CM (Table 4). Almost 90% of patients in our study and also almost 90% of patients in a prior cross-sectional study evaluating orthopedic patients in Germany showed that patients attached importance to make their own treatment decisions [10]. The integration of a patient’s view for decision making and the usage of shared decision making model is known to improve treatment adherence, knowledge of patients and patients satisfaction [38,39,40]. The high rate of patients desiring to take over responsibility for treatment decisions also supports the important role of self-management. Self-management is a central element of CM and an effective approach to improve treatment of chronic diseases [41, 42]. Unfortunately, the communication about CM between patients and attending surgeons is poor (Table 4), and similarly low communication rates are reported for other physicians such as oncologists and radiologists [18, 29, 43]. In our study, the most stated reason for non-communication of CM usage or interest was “no time”. In general, this is not surprising as research about communication in surgery indicates that patients report the feeling of lack of information and too less time for deeper communication with their attending surgeons [44, 45]. Nevertheless, the statement of “no time for communication” emphasizes that CM was not considered as relevant enough for communication. Similarly, parents of children suffering from cancer responded that the reason for non-communication was that no one raised the question about CM [46]. As mentioned above, patients consider CM as harmless, which is why, patients might be not able to see the clinical relevance of CM usage in surgery. It is, therefore, a physician’s task to ask for CM. Furthermore, a fifth of patients in our study stated that they were afraid of the physician’s attitude towards CM. In a cross-sectional study by Stub et al., who evaluated the attitudes and knowledge of health care providers regarding CM in cancer care, it was shown that most.
of the non-CM-skilled responders stated that CM can cause adverse events in cancer treatment, and that they would neither encourage nor discourage the usage of CM in cancer patients [47]. Indeed, this is interesting as CM is rated as risky by the physicians in the study, but no recommendation regarding CM usage is given for the patient. Keeping this in mind, it is also assumable that patients did not communicate their CM usage or interest to their attending physicians as they are not expecting constructive feedback. Recent research indicates an increase of internet searching for health specific topics, although the quality of information is often low [48]. On this way, the low communication rate between physicians and patients might be able to promote uncontrolled CM usage as patients are misled by online-communicated misinformation about CM. Once more, the consequence is an increased risk of side effects and interactions by CM. The non-communication about CM is, therefore, a vicious circle. Attending physicians should be aware of patients’ non-communication, focusing on consider CM usage during anamnesis and treatment. The results of our study emphasize the role of CM in surgery indicating that surgeons should be also informed about CM. Almost 80% of patients in our study stated that attending physicians should have knowledge about CM, which is also confirmed by other studies showing similar results [10]. The demand of patients for reliable information about CM is also a call for science as evidence-based CM is still needed.
Limitations and strengths
Results of surveys are always limited due to the possibility of selection bias. It is assumable that patients, who are interested in CM, are more interested in participating in a CM-related survey. As previously mentioned, the results of this manuscript are a subgroup analysis of an interdisciplinary survey evaluating CM usage of hospitalized patients in University Medical Centers in Southern Germany, which showed a response rate of 67% [7]. A response rate of approximately 60% is recommended to avoid bias [63]. Furthermore, CM usage was more likely in Freiburg indicating the previously reported limited transferability of surveys due to regional factors such as local culture and institutions [2]. In 2020, Li et al. stated that nature connectedness is a factor for favoring herbal medicine [64]. Freiburg can be characterized as “green city” emphasizing a close affinity to nature and high relevance of nature medicine of the population. The center for complementary medicine in Freiburg (UZN) is one of the first (founded 1998) and largest (> 4000 out-patient and in-patient consultations per year) of its kind in Germany. Even though patients participating in the survey have not been counselled by UZN-physicians during their hospital stay, CM might have a good reputation in Freiburg due to the existence of this center. The size of the three cities (Freiburg, Ulm and Heidelberg) and their socio-economic situation is similar and probably not a relevant factor.
Conclusion
Our study shows a high percentage of CM users and a strong interest in CM among surgical patients admitted to surgical wards of university hospitals in the South-West of Germany. The complementing review of literatures supports a worldwide CM usage of surgical patients. Current communication about CM between patients and surgeons is poor. The results emphasize the necessity for physicians to be aware of complementary medicine usage, also in surgery. With respect to a patient-centered treatment, but also for safety and quality reasons, the topic is of relevance for all physicians as well as for researchers to promote an evidence-based complementary medicine, which is demanded by patients.
Data availability
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Change history
19 November 2022
A Correction to this paper has been published: https://doi.org/10.1186/s12906-022-03772-1
Abbreviations
- AZKIM:
-
Akademisches Zentrum für Komplementäre und Integrative Medizin.
- CM:
-
Complementary medicine.
- TCM:
-
Traditional Chinese Medicine.
- UZN:
-
Center for complementary medicine Freiburg.
References
Institut für Demoskopie Allensbach. Naturheilmittel 2010 - Ergebnisse einer bevölkerungsrepräsentativen Befragung. 2010;:23. http://www.ifd-allensbach.de/uploads/tx_studies/7528_Naturheilmittel_2010.pdf. Accessed 9 May 2017.
World Health Organization. WHO Global report on traditional and complementary medicine 2019. 2019. https://apps.who.int/iris/bitstream/handle/10665/312342/9789241515436-eng.pdf?ua=1.
Steel A, McIntyre E, Harnett J, Foley H, Adams J, Sibbritt D, et al. Complementary medicine use in the Australian population: Results of a nationally-representative cross-sectional survey. Sci Rep. 2018;8:17325. doi:https://doi.org/10.1038/s41598-018-35508-y.
Teo TY, Yap J, Shen T, Yeo KK. Complementary and alternative medicine use amongst patients with cardiovascular disease in Singapore. BMC Complement Altern Med. 2016;16:446.
Kim S, Chang L, Weinstock-Guttman B, Gandhi S, Jakimovski D, Carl E, et al. Complementary and Alternative Medicine Usage by Multiple Sclerosis Patients: Results from a Prospective Clinical Study. J Altern Complement Med. 2018;24:596–602.
Nilsson J, Källman M, Östlund U, Holgersson G, Bergqvist M, Bergström S. The Use of Complementary and Alternative Medicine in Scandinavia. Anticancer Res. 2016;36:3243–51.
Lederer A-K, Baginski A, Raab L, Joos S, Valentini J, Klocke C, et al. Complementary medicine in Germany: a multi-centre cross-sectional survey on the usage by and the needs of patients hospitalized in university medical centers. BMC Complement Med Ther. 2021;21:285. doi:https://doi.org/10.1186/s12906-021-03460-6.
Soós S, Jeszenői N, Darvas K, Harsányi L. Nem konvencionális gyógymódok használata sebészeti betegek között. Orv Hetil. 2016;157:1483–8. doi:https://doi.org/10.1556/650.2016.30543.
Schieman C, Rudmik LR, Dixon E, Sutherland F, Bathe OF. Complementary and alternative medicine use among general surgery, hepatobiliary surgery and surgical oncology patients. Can J Surg. 2009;52:422–6. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2769094&tool=pmcentrez&rendertype=abstract
Kilper A, Müller A, Huber R, Reimers N, Schütz L, Lederer A-K. Complementary medicine in orthopaedic and trauma surgery: a cross-sectional survey on usage and needs. BMJ Open. 2020;10:e037192. doi:https://doi.org/10.1136/bmjopen-2020-037192.
Wang C-Z, Moss J, Yuan C-S. Commonly Used Dietary Supplements on Coagulation Function during Surgery. Medicines. 2015;2:157–85. doi:https://doi.org/10.3390/medicines2030157.
Moss J, Yuan C-S. Herbal medicines and perioperative care. Anesthesiology. 2006;105:441–2. https://doi.org/10.1001/jama.286.2.208.
Mohammed Abdul MI, Jiang X, Williams KM, Day RO, Roufogalis BD, Liauw WS, et al. Pharmacodynamic interaction of warfarin with cranberry but not with garlic in healthy subjects. Br J Pharmacol. 2009;154:1691–700. doi:https://doi.org/10.1038/bjp.2008.210.
Abebe W. Review of herbal medications with the potential to cause bleeding: dental implications, and risk prediction and prevention avenues. EPMA J. 2019;10:51–64. doi:https://doi.org/10.1007/s13167-018-0158-2.
Bauer BA, Townsend KM, Cutshall SM, Hazelton JF, Mahapatra S, Meek AM, et al. Advanced Practice Providers’ Knowledge, Attitudes, and Utilization of Complementary and Integrative Medicine at an Academic Medical Center. Altern Ther Health Med. 2020;26:8–16. http://www.ncbi.nlm.nih.gov/pubmed/32663179.
Welz AN, Emberger-Klein A, Menrad K. Why people use herbal medicine: insights from a focus-group study in Germany. BMC Complement Altern Med. 2018;18:92. doi:https://doi.org/10.1186/s12906-018-2160-6.
Bello N, Winit-Watjana W, Baquir W, McGarry K. Disclosure and adverse effects of complementary and alternative medicine used by hospitalized patients in the North East of England. Pharm Pract. 2012;10:125–35. doi:https://doi.org/10.4321/S1886-36552012000300002.
Azaz-Livshits T, Muszkat M, Levy M. Use of complementary alternative medicine in patients admitted to internal medicine wards. Int J Clin Pharmacol Ther. 2002;40:539–47. doi:https://doi.org/10.5414/CPP40539.
Creamer GL, Dahl A, Perumal D, Tan G, Koea JB. Anatomy of the ward round: the time spent in different activities. ANZ J Surg. 2010;80:930–2. doi:https://doi.org/10.1111/j.1445-2197.2010.05522.x.
Gkegkes ID, Minis EE, Iavazzo C. Effect of Caffeine Intake on Postoperative Ileus: A Systematic Review and Meta-Analysis. Dig Surg. 2020;37:22–31. doi:https://doi.org/10.1159/000496431.
Lederer A-K, Schmucker C, Kousoulas L, Fichtner-Feigl S, Huber R. Naturopathic treatment and complementary medicine in surgical practice. Dtsch Aerzteblatt Online. 2018. doi:https://doi.org/10.3238/arztebl.2018.0815.
Wu M-S, Chen K-H, Chen I-F, Huang SK, Tzeng P-C, Yeh M-L, et al. The Efficacy of Acupuncture in Post-Operative Pain Management: A Systematic Review and Meta-Analysis. PLoS One. 2016;11:e0150367. doi:https://doi.org/10.1371/journal.pone.0150367.
Council of Europe. Gemeinsamer europäischer Referenzrahmen für Sprachen: Lernen, lehren, beurteilen. 2001. http://www.goethe.de/z/50/commeuro/deindex.htm. Accessed 15 Aug 2020.
Huber R, Lüdtke R, Beiser I, Koch D. Coping Strategies and the Request for a Consultation on Complementary and Alternative Medicine – a Cross-Sectional Survey of Patients in a Psychosomatic and Three Medical Departments of a German University Hospital. Forschende Komplementärmedizin /. Res Complement Med. 2004;11:207–11. doi:https://doi.org/10.1159/000080556.
KOKON. KOKON - Kompetenznetz Komplementärmedizin in der Onkologie. https://www.kompetenznetz-kokon.de/. Accessed 28 Aug 2019.
Ciarlo G, Ahmadi E, Welter S, Hübner J. Factors influencing the usage of complementary and alternative medicine by patients with cancer. Complement Ther Clin Pract. 2021;44:101389. doi:https://doi.org/10.1016/j.ctcp.2021.101389.
Tangkiatkumjai M, Boardman H, Walker D-M. Potential factors that influence usage of complementary and alternative medicine worldwide: a systematic review. BMC Complement Med Ther. 2020;20:363. doi:https://doi.org/10.1186/s12906-020-03157-2.
Schuerger N, Klein E, Hapfelmeier A, Kiechle M, Brambs C, Paepke D. Evaluating the Demand for Integrative Medicine Practices in Breast and Gynecological Cancer Patients. Breast Care. 2019;14:35–40. doi:https://doi.org/10.1159/000492235.
Bauer F, Schmidt T, Eisfeld H, Dubois C, Kastrati K, Hochhaus A, et al. Information needs and usage of complementary and alternative medicine in members of a German self-help group for gastrointestinal stroma tumours, sarcoma, and renal cancer. Complement Ther Med. 2018;41:105–10. doi:https://doi.org/10.1016/j.ctim.2018.09.008.
Wortmann JK, Bremer A, Eich H, Wortmann HK, Schuster A, Fühner J, et al. Use of complementary and alternative medicine by patients with cancer: a cross-sectional study at different points of cancer care. Med Oncol. 2016;33:78. doi:https://doi.org/10.1007/s12032-016-0790-4.
Jermini M, Dubois J, Rodondi P-Y, Zaman K, Buclin T, Csajka C, et al. Complementary medicine use during cancer treatment and potential herb-drug interactions from a cross-sectional study in an academic centre. Sci Rep. 2019;9:5078. doi:https://doi.org/10.1038/s41598-019-41532-3.
Giveon SM, Liberman N, Klang S, Kahan E. Are people who use “natural drugs” aware of their potentially harmful side effects and reporting to family physician? Patient Educ Couns. 2004;53:5–11. doi:https://doi.org/10.1016/S0738-3991(03)00241-6.
Shakeel M, Bruce J, Jehan S, McAdam TK, Bruce DM. Use of Complementary and Alternative Medicine by Patients Admitted to a Surgical Unit in Scotland. Ann R Coll Surg Engl. 2008;90:571–6. doi:https://doi.org/10.1308/003588408X301046.
Woodward KN. The potential impact of the use of homeopathic and herbal remedies on monitoring the safety of prescription products. Hum Exp Toxicol. 2005;24:219–33. doi:https://doi.org/10.1191/0960327105ht529oa.
White A, Boon H, Alraek T, Lewith G, Liu J-P, Norheim A-J, et al. Reducing the risk of complementary and alternative medicine (CAM): Challenges and priorities. Eur J Integr Med. 2014;6:404–8. doi:https://doi.org/10.1016/j.eujim.2013.09.006.
Norred CL. Complementary and alternative medicine use by surgical patients. AORN J. 2002;76:1013–21. http://www.ncbi.nlm.nih.gov/pubmed/12528489.
Wong A, Townley SA. Herbal medicines and anaesthesia. Contin Educ Anaesth Crit Care Pain. 2011;11:14–7. doi:https://doi.org/10.1093/bjaceaccp/mkq046.
Wei Y, Ming J, Shi L, Ke X, Sun H, Chen Y. Physician–patient shared decision making, patient satisfaction, and adoption of new health technology in China. Int J Technol Assess Health Care. 2020;36:518–24. doi:https://doi.org/10.1017/S0266462320000719.
Elwyn G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P, et al. Shared Decision Making: A Model for Clinical Practice. J Gen Intern Med. 2012;27:1361–7. doi:https://doi.org/10.1007/s11606-012-2077-6.
Barry MJ, Edgman-Levitan S. Shared Decision Making — The Pinnacle of Patient-Centered Care. N Engl J Med. 2012;366:780–1. doi:https://doi.org/10.1056/NEJMp1109283.
Shahaj O, Denneny D, Schwappach A, Pearce G, Epiphaniou E, Parke HL, et al. Supporting self-management for people with hypertension. J Hypertens. 2019;37:264–79. doi:https://doi.org/10.1097/HJH.0000000000001867.
Armour M, Sinclair J, Chalmers KJ, Smith CA. Self-management strategies amongst Australian women with endometriosis: a national online survey. BMC Complement Altern Med. 2019;19:17. doi:https://doi.org/10.1186/s12906-019-2431-x.
Ge J, Fishman J, Vapiwala N, Li SQ, Desai K, Xie SX, et al. Patient-Physician Communication About Complementary and Alternative Medicine in a Radiation Oncology Setting. Int J Radiat Oncol. 2013;85:e1–6. doi:https://doi.org/10.1016/j.ijrobp.2012.08.018.
Richards J, McDonald P. Doctor-Patient Communication in Surgery. J R Soc Med. 1985;78:922–4. doi:https://doi.org/10.1177/014107688507801109.
Langewitz W. Kommunikation in der Chirurgie. Allg und Visz up2date. 2013;7:451–63. doi:https://doi.org/10.1055/s-0033-1346885.
Stub T, Quandt SA, Kristoffersen AE, Jong MC, Arcury TA. Communication and information needs about complementary and alternative medicine: a qualitative study of parents of children with cancer. BMC Complement Med Ther. 2021;21:85. doi:https://doi.org/10.1186/s12906-021-03253-x.
Stub T, Quandt SA, Arcury TA, Sandberg JC, Kristoffersen AE. Attitudes and knowledge about direct and indirect risks among conventional and complementary health care providers in cancer care. BMC Complement Altern Med. 2018;18:44. doi:https://doi.org/10.1186/s12906-018-2106-z.
Sansevere ME, White JD. Quality Assessment of Online Complementary and Alternative Medicine Information Resources Relevant to Cancer. Integr Cancer Ther. 2021;20:153473542110660. doi:https://doi.org/10.1177/15347354211066081.
Adusumilli PS, Ben-Porat L, Pereira M, Roesler D, Leitman IM. The prevalence and predictors of herbal medicine use in surgical patients1 1No competing interests declared. J Am Coll Surg. 2004;198:583–90. doi:https://doi.org/10.1016/j.jamcollsurg.2003.11.019.
Andersen MR, Sweet E, Zhou M, Standish LJ. Complementary and Alternative Medicine Use by Breast Cancer Patients at Time of Surgery Which Increases the Potential for Excessive Bleeding. Integr Cancer Ther. 2015;14:119–24. doi:https://doi.org/10.1177/1534735414555808.
Braun LA, Cohen M. Use of Complementary Medicines by Cardiac Surgery Patients; Undisclosed and Undetected. Hear Lung Circ. 2011;20:305–11. doi:https://doi.org/10.1016/j.hlc.2011.01.013.
Dalmayrac E, Quignon A, Baufreton C. Complementary and Alternative Medicine in Cardiac Surgery: Prevalence and Modality of use. Hear Lung Circ. 2016;25:712–8. doi:https://doi.org/10.1016/j.hlc.2016.01.017.
Dhanoa A, Yong TL, Yeap SJL, Lee ISZ, Singh VA. Complementary and alternative medicine use amongst Malaysian orthopaedic oncology patients. BMC Complement Altern Med. 2014;14:404. doi:https://doi.org/10.1186/1472-6882-14-404.
Guilmetdinov EF, Al-Khalaf M, Bhatt J, Parsons R, Sim TF. Complementary medicines use amongst elective surgery patients at a public tertiary hospital: A prospective observational cohort study in Australia. Complement Ther Clin Pract. 2019;35:284–9. doi:https://doi.org/10.1016/j.ctcp.2019.03.012.
Lim CM, Ng A, Loh KS. Use of complementary and alternative medicine in head and neck cancer patients. J Laryngol Otol. 2010;124:529–32. doi:https://doi.org/10.1017/S0022215109992817.
Lin Y-C, Bioteau AB, Ferrari LR, Berde CB. The use of herbs and complementary and alternative medicine in pediatric preoperative patients. J Clin Anesth. 2004;16:4–6. doi:https://doi.org/10.1016/j.jclinane.2003.03.005.
Liu EH, Turner LM, Lin SX, Klaus L, Choi LY, Whitworth J, et al. Use of alternative medicine by patients undergoing cardiac surgery. J Thorac Cardiovasc Surg. 2000;120:335–41. doi:https://doi.org/10.1067/mtc.2000.107339.
Norred CL. Complementary and Alternative Medicine Use by Surgical Patients. AORN J. 2002;76:1013–21. doi:https://doi.org/10.1016/S0001-2092(06)61003-X.
Shakeel M, Newton JR, Ah-See KW. Complementary and alternative medicine use among patients undergoing otolaryngologic surgery. J Otolaryngol Head Neck Surg. 2009;38:355–61. http://www.ncbi.nlm.nih.gov/pubmed/19476768.
Wang S-M, Caldwell-Andrews AA, Kain ZN. The Use of Complementary and Alternative Medicines by Surgical Patients: A Follow-Up Survey Study. Anesth Analg. 2003;:1010–5. doi:https://doi.org/10.1213/01.ANE.0000078578.75597.F3.
Yazici G, Erdogan Z, Bulut H, Ay A, Kalkan N, Atasayar S, et al. The Use of Complementary and Alternative Medicines Among Surgical Patients: A Survey Study. J PeriAnesthesia Nurs. 2019;34:322–9. doi:https://doi.org/10.1016/j.jopan.2018.04.007.
Yoshimura K, Ichioka K, Terada N, Terai A, Arai Y. Use of complementary and alternative medicine by patients with localized prostate carcinoma: study at a single institute in Japan. Int J Clin Oncol. 2003;8:26–30. doi:https://doi.org/10.1007/s101470300003.
Draugalis JR, Coons SJ, Plaza CM. Best Practices for Survey Research Reports: A Synopsis for Authors and Reviewers. Am J Pharm Educ. 2008;72:11. doi:https://doi.org/10.5688/aj720111.
Li H, Cao Y. For the love of nature: People who prefer natural versus synthetic drugs are higher in nature connectedness. J Environ Psychol. 2020;71:101496. doi:https://doi.org/10.1016/j.jenvp.2020.101496.
Acknowledgements
Thank you to Lena Raab, Alexandra Baginski, Ivana Andreeva, Susanne Hafner und Anna Freisinger for helping with data acquisition and curation.
Funding
The Ministry of Science, Research and Arts of the state Baden-Württemberg, Germany, financed the Academic Centre for Complementary and Integrative Medicine (AZKIM), otherwise the study was financed by institutional resources.
Authors’ contributions.
Study conceptualization and design: YS, TSi, TSy, RH.
Development of questionnaire: YS, RH.
Data collection: AKL.
Data entering: AKL.
Interpretation and analysis of results: AKL, YS, TSi, TSy, RH.
Drafting of manuscript: AKL.
Review and editing of manuscript: RH.
Supervision of study: YS, TSi, TSy, RH.
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Study was approved by ethical committee of the University Medical Centre of Freiburg, Germany (EK FR 25/17). For participation, patients had to give written informed consent before inclusion.
All methods were performed in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
None. The authors have no conflicts of interest or financial ties to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: the authors reported an error in Tables 2 and 3 presentation, and insertion of reference details of “Liu et al. 2000” in the list. Due to the insertion, references were renumbered in the proof.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lederer, AK., Samstag, Y., Simmet, T. et al. Complementary medicine usage in surgery: a cross-sectional survey in Germany. BMC Complement Med Ther 22, 263 (2022). https://doi.org/10.1186/s12906-022-03746-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-022-03746-3