
Abstract
Background
The integration of patient portals into health systems has the potential to increase access for women. For example, within a mental health context, women are at a higher risk of developing anxiety and depression but may experience barriers in accessing care. Therefore, the aim of this rapid review was to understand what is currently known about patient portal use among women. The objectives were (1) To discover pertinent facilitators for women when using patient portals; (2) To discern if women face individual barriers to accessing patient portals; and (3) To explore the potential role of patient portals for women’s mental health care.
Methods
A rapid review methodology was implemented using the Cochrane Rapid Reviews Methods Group, as well as a grey literature scan. Inclusion criteria included articles that focused on women’s use of patient portals within healthcare settings. Four databases were searched, including Embase, MEDLINE (Ovid), CINAHL and PsycINFO in September 2023. Two independent reviewers performed screening, data extraction, and analysis.
Results
This search resulted in screening 1385 titles and abstracts, and 82 articles for full-text eligibility. 15 articles were included in the review. Data were extracted and analyzed, guided by the research objectives. Facilitators to patient portal use included processes that enhanced user engagement, the provision of portal tools, and management of health care features. Barriers included health equity factors and use of medical jargon. Applications to mental health care included how use of portals eased women’s anxiety and increased their sense of internal control.
Conclusions
The results of this review indicate that interrelated factors influence women’s experiences with using patient portals. By understanding facilitators and barriers to portal use, and applications for mental health care, we can understand how to improve women’s use of portals in the future.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Patient portals
Patient portals are online systems where patients can access various components of their personal health information, such as prescriptions, treatment protocols, and appointment schedules, and at times interact with their health care providers [1]. Patient portals may also include electronic personal health records (ePHRs) [2]. Since their inception, patient portals have enhanced health care access for patients through features such as direct messaging with providers [3] and having access to notes from their care plans [4]. Health care access through use of a patient portal has been studied among patient groups from other marginalized populations [5, 6] and with specific diagnoses such as cancer [7] and multiple sclerosis [8]. In mental health care, research continues to evolve on the potential benefits of patient portals for care outcomes, and how to tailor the user experience to this health context [9]. For example, Turvey et al. (2022) examined the collaborative relationship between patients and clinicians through use of a patient portal and secure messaging system, and described how patients experienced higher levels of trust, comfort, and medication adherence [10]. Additionally, Strudwick et al. (2020) examined meaningful indicators of patient portal use by conducting focus groups among mental health patients, care partners, and family members [11]. As we learn more about patient portal use within various health settings, it is imperative to discern how to foster positive experiences for subpopulations who may have different health needs, including women’s health care.
Women and patient portal use
Despite evolving research on patient portals, information about women’s use is limited, including people who identify as cisgender, transgender, non-binary, or gender diverse who were assigned the sex of female at birth. As this review is part of a larger project that focuses on developing actionable recommendations for patient portal use by women with mental health challenges, it is important to find existing data on women’s use of patient portals. Specifically, some previous work has been conducted in obstetric and gynecological settings among varying populations [12]. For example, Kim et al. (2018) examined patient portal use among low-income pregnant women, with a goal of improving clinical outcomes through its use. The authors discovered that use of the portal was enhanced through information sharing by health care providers, but that further discussion-based support was needed to improve access [12].
Women and mental health care
Patient portal use may have positive applications for women, specifically with accessing mental health care. Women are at higher risk of developing common mental health disorders [13], such as anxiety and depression, when compared to men [14]. However, they are significantly more likely to experience barriers in accessing specialized mental health services and care [14], especially when health issues are sex-specific, such as perinatal mental illness [15]. Some of these noted barriers include fear of stigmatization, difficulties attending appointments, and an unwillingness to seek help [16]. Additionally, women may have unique mental health needs when compared to men in some professions, roles, or other contexts. For example, Runnals et al. (2014) found that women veterans experienced higher rates of depression and medical/functional impairments versus male veterans [17]. Additionally, women have historically taken on caregiving roles for family members, and experience worse mental health outcomes when trying to balance these roles with employment [18]. Therefore, as patient portals are more regularly implemented into healthcare settings to increase patient engagement [19, 20] and collaboration [21], it is crucial to examine barriers and facilitators for women’s access. Additionally, it is valuable to discern if these barriers and facilitators have applications to mental health care.
Research question
The research question for this review was: What is currently known about patient portal use among women?
Objectives
-
1.
To discover pertinent facilitators for women when using patient portals.
-
2.
To discern if women face individual barriers to accessing patient portals.
-
3.
To explore the potential role of patient portals for women’s mental health care.
Methods
A rapid review methodology was implemented due to the limited timeframe needed for the results [22], as this data will be used for the implementation of patient portal guidelines within a large mental health organization. To perform this rapid review, we searched academic literature using the criteria from the Cochrane Rapid Reviews Methods Group [22] and conducted a grey literature scan. A preliminary search occurred to ensure that no current or in-progress reviews were being performed on the same topic, which included the following databases: the Cochrane Database of Systematic Reviews, Joanna Briggs Institute (JBI) Evidence Synthesis, and MEDLINE. Recent reviews that have examined individual experiences of patient portals have included older adult populations [23] and caregivers [24]. Additionally, Antonio et al. (2019) explored health equity factors, and how these are addressed within patient portal research [25].
Search strategy
The search strategy was developed in consultation with a research librarian for how to perform thorough searches using index terms/subject headings and to identify relevant databases. Four databases were searched in September 2023, including: Embase, MEDLINE (Ovid), CINAHL and PsycINFO. As this is a novel topic, we included databases for different health disciplines to ensure the results were comprehensive. Applicable search words and phrases were used for the corresponding databases. Search terms included patient portal(s) and gender-specific terms including women, woman, human female, transgender, transgender person(s), and non-binary. Searched databases and associated terms or subject headings are listed in Table 1. A grey literature scan included searching the first ten pages of the Google and Million Short search engines for relevant documents related to women’s health and patient portals. Predefined terms were used to search for relevant results.
Inclusion criteria
For this review, the inclusion criteria are listed below. A more comprehensive description of inclusion and exclusion criteria with full-text exclusion rationale can be found in Table 2.
-
1.
Population: Women, including cisgender, transgender, and non-binary/gender diverse people assigned the sex of female at birth.
-
2.
Intervention: Population must have accessed/used a patient portal.
-
3.
Setting: Patient portal use occurred within a healthcare setting, such as a hospital, clinic, or the community. Data from all countries is included in this review.
-
4.
Language: Articles are available in English.
-
5.
Date: Articles should be published during or after 2006, when patient portal use was widely adapted within healthcare settings [19].
Screening
Articles yielded from the searches were uploaded into the online Covidence [26] software system to assist with screening procedures. KD was the primary reviewer and performed data extraction. HDS was the second reviewer. Throughout the screening procedures, ad-hoc meetings occurred to discuss discrepancies and resolve conflicts. The steps for the screening procedures were as follows:
-
a)
A pilot exercise for calibration, where 30 titles and abstracts were screened by both reviewers. An agreement rate of at least 80% was met before moving to the next step.
-
b)
KD completed the full screening and HDS screened 20% of the remaining articles. The excluded articles were then reviewed by HDS.
-
c)
A pilot screening exercise of five full-text articles was performed by both reviewers for calibration.
-
d)
KD screened the remainder of the full-text articles and HDS reviewed the excluded articles to check for any missed data.
-
e)
KD performed data extraction. All extracted data was reviewed by HDS prior to analysis procedures.
Data analysis and presentation
Data analysis was performed by KD and was reviewed by HDS for completion and accuracy. Data are summarized and presented in table format (see Additional File 1). To meet the research objectives, narrative descriptions of barriers, facilitators, and mental health considerations were organized into categories that were inductively generated from the extracted data.
Results
Characteristics of included articles
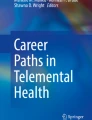
After searching the four databases, we sourced 1548 studies that were uploaded into Covidence [26]. A total of 81 duplicate articles were identified and removed, leaving 1467 articles to be screened at the title and abstract stage. A total of 1385 studies were deemed irrelevant at this stage, leaving 82 articles to be screened for full-text eligibility. Articles excluded at this stage were classified into the following categories: wrong source (n=29), wrong outcomes (n=20), wrong concept (n=13), wrong patient population (n=3), and article not available (n=2). This process left 15 articles to be included in the review for data extraction and analysis. Please refer to Fig. 1 for a flow diagram of the review screening procedures.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)
The publication dates of the 15 included articles ranged over nine years, from 2014-2023. Most of the research was conducted in the United States [27,28,29,30,31,32,33,34,35,36,37,38], and one article was yielded each from Australia [39], Belgium [40], and Canada [41]. There were a variety of study designs employed by the researchers, including cross-sectional [30, 31, 37, 39], quality improvement projects [28, 29, 35], retrospective or prospective studies [27, 32, 33, 36, 39], quasi experimental designs [40], and qualitative designs [34, 41]. Examples of the data collection methods included questionnaires [38], surveys [31, 33, 39], and interviews [34]. Some of the studies included patient populations that were specifically focused on women’s health, such as women with cancer [41], veterans [29], pregnant or postpartum patients [27, 33,34,35,36, 38, 39], and women with human immunodeficiency viruses (HIV) [28]. Other studies included both sexes, however, the outcomes were stratified to discuss women’s health and patient portal use. In 13 of the studies, the researchers provided details of the implemented patient portal within the study setting. Some of the study settings included primary and secondary care clinics [28, 30, 32,33,34, 37, 40], general or tertiary hospitals [27, 29, 31, 35, 36, 38], and specialty hospitals [39, 41]. A summary of all extracted data can be found in Table 3 (see Additional File 1). From the grey literature scan, no documents were yielded related to women’s use of patient portals.
Facilitators of patient portal use
We discovered a variety of facilitators for patient portal use for women within the included studies’ outcomes. Firstly, active engagement was a facilitator in two studies, where researchers discovered that women exhibited higher levels of engagement with the patient portal compared to men [31, 37]. Being actively engaged with the patient portal was critical for women to utilize the portal functions [31, 37]. A second facilitator to accessing and using patient portals was having all information readily available, such as tools to assist with portal navigation [33], supplementary information for discharge planning [35], and contact information for providers [41]. Another facilitator for women included using the patient portals for health care management, such as remembering appointments [34], communicating with providers [34], medication regimens [27, 34], and secure messaging [38]. Lastly, ensuring the patient portal was easy to navigate was discussed as a high priority within two of the included studies [30, 33].
Access barriers to patient portal use
Within the included studies, some notable health equity barriers were discussed that are relevant to patient portal use for women, including health status [27], income [27], and literacy [34]. Ukoha et al. (2019) discovered that women with high-risk pregnancies were less likely to enroll in the patient portal versus women with no complications [27]. These researchers also discovered how having public health insurance was a barrier to accessing the patient portal versus having private coverage. Another significant barrier to portal use for women was not understanding medical jargon or lab results that were uploaded by providers [34].
Some authors also discussed methods to prevent patient portal access barriers. For example, Lewi et al. (2018) found that a patient’s age must be considered to prevent barriers to portal use, as women in different age categories had different preferences when using the patient portal [40]. For example, women in older age categories were found to request information about diagnoses and treatment, while younger women requested prevention material. Conversely, Wieland et al. (2017) explored the concept of barriers for postpartum women and accessing the patient portal [38], although some participants did not perceive any barriers in adopting the patient portal and found the functions to be useful for their health care.
Role of patient portals for women’s mental health care
Due to the limited research performed in this space, there were no patient populations within this review that were specific to mental health care. However, some of the findings from other care settings can be applied within women’s mental health contexts to identify clinical applications that are relevant to accessing and utilizing patient portals. For example, in a study by Mohsen et al. (2021), women remarked how the patient portal provided them with a sense of control over their care planning and that this provided reassurance when receiving cancer treatment [41]. Furthermore, in a study by MacEwan et al. (2023), the participants remarked how using a patient portal can ease anxiety about pregnancy/postpartum care outcomes, and that use of a portal promotes involvement in care [34].
Discussion
This rapid review was conducted to explore the scope of literature on women’s use of patient portals, including facilitators and barriers to use, and applications for mental health care. The results of the review demonstrate that patient portals are being implemented in a variety of settings that focus on women’s health, and that researchers are beginning to explore how patient portals relate to women’s health care. Through reviewing this data, we can understand how to improve the user experience for women across different clinical settings.
Due to minimal published literature on this topic, few facilitators and barriers to patient portal use exist that are limited to women’s health. However, the studies within this review included data that support how women’s care outcomes can be improved through use of a patient portal. Specifically, some evidence showed how patient portals were related to increased breastfeeding rates for postpartum women [36] and improved viral load counts for women with HIV [28]. Previous work on patient portal use and health care outcomes has shown similar results. For example, patient portal use has been linked with a decreased risk of cervical cancer [42] and improved diabetes management [43]. Our findings also revealed that some facilitators for patient portal use for women included having access to all health care information, managing health outcomes, and ensuring that patient portal systems are user-friendly. Similar facilitators were explored in a literature review that focused on older adults’ use of patient portals, specifically, ensuring that the performance of the portal was suitable [44]. Additionally, in a scoping review that explored patient portal use for patients with asthma, ease of use was described as a primary facilitator to patient portal uptake [45].
Within our results, health equity factors, such as income [18], lack of access to private insurance [27], and health literacy [33], were mentioned as potential barriers to accessing and using patient portals for women. Similar health equity barriers have been found within other groups, including Hispanic populations, people that did not graduate from high school, and people with lower incomes [46]. Gender equity can be enhanced through digital health interventions but must be designed using principles of feminist intersectionality [43, 47]. These principles include all social identities that relate to marginalization, in addition to women’s health, such as race, socioeconomic status, and sexual orientation [43]. Therefore, designing patient portals using a feminist intersectionality lens can reduce the chance of widening different groups’ access to health services through technology, also known as the digital divide [31]. Suggested strategies from other literature to reduce the digital divide have included implementing user-centered designs and considering preferences of different groups [29]. Providers can also offer enrollment assistance for patients [48] with supplementary materials for guidance. Lastly, providers must ensure to use patient-friendly language by reducing the use of medical jargon, complex terminology and abbreviations [20].
Despite retrieving no literature specific to patient portal use and women receiving mental health care, implementation of patient portals within mental health settings is becoming a more prominent area of research. Therefore, it is important to consider how use of patient portals can specifically impact women with mental health challenges, such as depression and anxiety [12]. In a scoping review by Rabbani et al. (2023), characteristics for portal use were evaluated specifically for individuals with depression, including providing tailored services and having a messaging feature between the patient and provider [49]. Additionally, specific characteristics of providers, such as providing compassionate care and fostering interprofessional collaboration, may enhance treatment experiences [4, 21].
Limitations
To our knowledge, this is the first review to explore patient portal use among women, barriers and facilitators to their use of patient portals, and considerations for women’s mental health care. Although a rigorous process was integrated using criteria from the Cochrane Rapid Reviews Methods Group [22], some limitations still exist. Firstly, as most of the articles within the review were from the United States, these results may not have vast applications on a global scale. Future research within this space should focus on patient portal implementation within different global contexts, and how cultural implications and varying healthcare funding structures may impact patient portal adoption and use. Secondly, due to the novel topic area, high-quality studies, such as randomized control trials, have not yet been performed to evaluate patient portal use for women. Therefore, future reviews may have to be conducted to discern if there are further barriers and facilitators to portal use for this group. Lastly, although this review broadly looks at women’s experiences, women with different health outcomes may have additional needs for using patient portals. Therefore, future research can explore small subgroups of women to discover further interventions.
Conclusions
The results of this rapid review have presented the body of literature that has focused on the use of patient portals by women. By understanding facilitators and barriers for portal use, and additional applications for mental health care, we can understand how to improve the user experience for women in the future. Understanding how to engage patients, improve interface usability, and to design patient portals to help women with the management of their health care, were identified as important facilitators. Also, being aware of barriers of patient portal use, such as health complications and health equity factors, are important considerations for the use and uptake of patient portals. Future research should focus on how these experiences may differ globally, and how variations may exist among women with unique health needs. As patient portals continue to be integrated into health systems in the future, continued research can help women successfully use patient portals to manage their health care.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Abbreviations
- ePHRs:
-
Electronic Personal Health Records
- HIV:
-
Human Immunodeficiency Viruses
- JBI:
-
Joanna Briggs Institute
References
MedlinePlus. Patient portals - an online tool for your health. 2023. Available from: https://medlineplus.gov/ency/patientinstructions/000880.htm. Accessed 1 Oct 2023.
Abd-Alrazaq A, Alalwan AA, McMillan B, et al. Patients’ Adoption of Electronic Personal Health Records in England: Secondary Data Analysis. J Med Internet Res. 2020;22(10): e17499. https://doi.org/10.2196/17499.
Ammenwerth E, Schnell-Inderst P, Hoerbst A. The Impact of Electronic Patient Portals on Patient Care: A Systematic Review of Controlled Trials. J Med Internet Res. 2012;14(6): e162. https://doi.org/10.2196/jmir.2238.
Shin HD, Durocher K, Lo B, et al. Impact of a mental health patient portal on patients’ views of compassion: a mixed-methods study. BMC Digit Health. 2023;1(1). https://doi.org/10.1186/s44247-022-00002-z.
Ordaz OH, Croff RL, Robinson LD, et al. Optimization of Primary Care Among Black Americans Using Patient Portals: Qualitative Study. J Med Internet Res. 2021;23(6):e27820. https://doi.org/10.2196/27820.
Arcury TA, Quandt SA, Sandberg JC, et al. Patient Portal Utilization Among Ethnically Diverse Low Income Older Adults: Observational Study. JMIR Med Inform. 2017;5(4): e47. https://doi.org/10.2196/medinform.8026.
Santos AD, Caine V, Robson PJ, et al. Oncology Patients’ Experiences With Novel Electronic Patient Portals to Support Care and Treatment: Qualitative Study With Early Users and Nonusers of Portals in Alberta, Canada. JMIR Cancer. 2021;7(4): e32609. https://doi.org/10.2196/32609.
Voigt I, Benedict M, Susky M, et al. A Digital Patient Portal for Patients With Multiple Sclerosis. Front Neurol. 2020;11. https://doi.org/10.3389/fneur.2020.00400.
Zhang T, Shen N, Booth R, et al. Supporting the use of patient portals in mental health settings: a scoping review. Inform Health Soc Care. 2022;47(1):62–79. https://doi.org/10.1080/17538157.2021.1929998.
Turvey CL, Fuhrmeister LA, Klein DM, et al. Patient and Provider Experience of Electronic Patient Portals and Secure Messaging in Mental Health Treatment. Telemed E-Health. 2022;28(2):189–98. https://doi.org/10.1089/tmj.2020.0395.
Strudwick G, Booth RG, McLean D, et al. Identifying indicators of meaningful patient portal use by psychiatric populations. Inform Health Soc Care. 2020;45(4):396–409. https://doi.org/10.1080/17538157.2020.1776291.
Kim J, Mathews H, Cortright LM, et al. Factors Affecting Patient Portal Use Among Low-Income Pregnant Women: Mixed-Methods Pilot Study. JMIR Form Res. 2018;2(1): e6. https://doi.org/10.2196/formative.5322.
Adult Psychiatric Morbidity Survey. Adult Psychiatric Morbidity Survey: Survey of Mental Health and Wellbeing, England, 2014. NHS Digital; 2016. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/adult-psychiatric-morbidity-survey/adult-psychiatric-morbidity-survey-survey-of-mental-health-and-wellbeing-england-2014. Accessed 22 Jan 2024.
World Health Organization. Gender and women’s mental health. 2022. Available from: https://www.who.int/teams/mental-health-and-substance-use/promotion-prevention/gender-and-women-s-mental-health. Accessed 16 Jan 2024.
Sambrook Smith M, Lawrence V, Sadler E, et al. Barriers to accessing mental health services for women with perinatal mental illness: systematic review and meta-synthesis of qualitative studies in the UK. BMJ Open. 2019;9(1): e024803. https://doi.org/10.1136/bmjopen-2018-024803.
Ford E, Roomi H, Hugh H, et al. Understanding barriers to women seeking and receiving help for perinatal mental health problems in UK general practice: development of a questionnaire. Prim Health Care Res Dev. 2019;20:e156. https://doi.org/10.1017/S1463423619000902.
Runnals JJ, Garovoy N, McCutcheon SJ, et al. Systematic Review of Women Veterans’ Mental Health. Women’s Health Issues. 2014;24(5):485–502. https://doi.org/10.1016/j.whi.2014.06.012.
Li L, Lee Y, Lai DWL. Mental Health of Employed Family Caregivers in Canada: A Gender-Based Analysis on the Role of Workplace Support. Int J Aging Hum Dev. 2022;95(4):470–92. https://doi.org/10.1177/00914150221077948.
Dendere R, Slade C, Burton-Jones A, et al. Patient Portals Facilitating Engagement with Inpatient Electronic Medical Records: A Systematic Review. J Med Internet Res. 2019;21(4): e12779. https://doi.org/10.2196/12779.
Irizarry T, DeVito Dabbs A, Curran CR. Patient Portals and Patient Engagement: A State of the Science Review. J Med Internet Res. 2015;17(6):e148. https://doi.org/10.2196/jmir.4255.
Durocher K, Shin HD, Lo B, et al. Understanding the Role of Patient Portals in Fostering Interprofessional Collaboration Within Mental Health Care Settings: Mixed Methods Study. JMIR Hum Factors. 2023;10: e44747. https://doi.org/10.2196/44747.
Garritty C, Gartlehner G, Nussbaumer-Streit B, et al. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J Clin Epidemiol. 2020;15(130):13–22. https://doi.org/10.1016/j.jclinepi.2020.10.007.
Sakaguchi-Tang DK, Bosold AL, Choi YK, Turner AM. Patient Portal Use and Experience Among Older Adults: Systematic Review. JMIR Med Inform. 2017;5(4):3e8. https://doi.org/10.2196/medinform.8092.
Reynolds TL, Ali N, Zheng K. What Do Patients and Caregivers Want? A Systematic Review of User Suggestions to Improve Patient Portals. AMIA Annu Symp Proc Arch. 2021;2020:1070–9.
Antonio MG, Petrovskaya O, Lau F. Is research on patient portals attuned to health equity? A scoping review. J Am Med Inform Assoc. 2019;26(8–9):871–83. https://doi.org/10.1093/jamia/ocz054.
Covidence. Better systematic review management. 2021. Available from: https://www.covidence.org/. Accessed 9 Feb 2024.
Ukoha EP, Feinglass J, Yee LM. Disparities in Electronic Patient Portal Use in Prenatal Care: Retrospective Cohort Study. J Med Internet Res. 2019;21(9): e14445. https://doi.org/10.2196/14445.
Plimpton E. A Quality Improvement Project to Increase Patient Portal Enrollment and Utilization in Women Living With HIV at Risk for Disengagement in Care. J Assoc Nurses AIDS Care. 2020;31(1):60–5. https://doi.org/10.1097/jnc.0000000000000153.
Dang S, Thavalathil B, Ruiz D, et al. A Patient Portal Intervention for Menopause Knowledge and Shared Decision-Making. J Women’s Health. 2019;28(12):1614–22. https://doi.org/10.1089/jwh.2018.7461.
Eden KB, Ivlev I, Bensching KL, et al. Use of an Online Breast Cancer Risk Assessment and Patient Decision Aid in Primary Care Practices. J Women’s Health. 2020;29(6):763–9. https://doi.org/10.1089/jwh.2019.8143.
Graetz I, Gordon N, Fung V, et al. The Digital Divide and Patient Portals. Med Care. 2016;54(8):772–9. Available from: https://www.jstor.org/stable/26418215. Accessed 13 Feb 2024.
Jung C, Padman R. Virtualized healthcare delivery: Understanding users and their usage patterns of online medical consultations. Int J Med Inf. 2014;83(12):901–14. https://doi.org/10.1016/j.ijmedinf.2014.08.004.
Kalejta CD, Higgins S, Kershberg H, et al. Evaluation of an automated process for disclosure of negative noninvasive prenatal test results. J Genet Couns. 2019;28(4):847–55. https://doi.org/10.1002/jgc4.1127.
MacEwan SR, Fareed N, Jonnalagadda P, et al. Patient and provider perspectives on the use of patient portals during pregnancy and the postpartum period. J Telemed Telecare. 2023;1–9. https://doi.org/10.1177/1357633x231177742.
McArthur L. A Quality Improvement Project for Breastfeeding Promotion via the Patient Portal. J Inform Nurs. 2020;5(4):13–21.
Ossai CR, McDonnell J, Behairy M, et al. Association of Parental Use of Patient Portals with Breastfeeding Rates in Infants. J Consum Health Internet. 2021;25(3):261–74. https://doi.org/10.1080/15398285.2021.1943635.
Sun EY, Alvarez C, Callahan LF, et al. The Disparities in Patient Portal Use Among Patients With Rheumatic and Musculoskeletal Diseases: Retrospective Cross-sectional Study. J Med Internet Res. 2022;24(8): e38802. https://doi.org/10.2196/38802.
Wieland D, Gibeau A, Dewey C, et al. Patient portal readiness among postpartum patients in a safety net setting. Appl Clin Inform. 2017;8(3):698–709. https://doi.org/10.4338/ACI-2016-12-RA-0204.
Forster M, Dennison K, Callen J, et al. Maternity patients’ access to their electronic medical records: use and perspectives of a patient portal. Health Inf Manag J. 2015;44(1):4–11. https://doi.org/10.1177/183335831504400101.
Lewi M, De Pelsmacker P, Cauberghec V. Women’s information preferences, information needs and online interactive information portal engagement in a breast cancer early diagnosis context. J Commun Healthc. 2018;11(2):114–27. https://doi.org/10.1080/17538068.2018.1449581.
Mohsen K, Kildea J, Lambert SD, et al. Exploring Cancer Patients’ Perceptions of Accessing and Experience with Using the Educational Material in the Opal Patient Portal. Support Care Cancer. 2021;29(8):4365–74. https://doi.org/10.1007/s00520-020-05900-4.
Malone C, Buist DSM, Tiro J, et al. Out of reach? Correlates of cervical cancer underscreening in women with varying levels of healthcare interactions in a United States integrated delivery system. Prev Med. 2021;145: 106410. https://doi.org/10.1016/j.ypmed.2020.106410.
Lau M, Campbell H, Tang T, et al. Impact of patient use of an online patient portal on diabetes outcomes. Can J Diabetes. 2014;38(1):17–21. https://doi.org/10.1016/j.jcjd.2013.10.005.
Wildenbos GA, Peute L, Jaspers M. Facilitators and Barriers of Electronic Health Record Patient Portal Adoption by Older Adults: A Literature Study. Stud Health Technol Inform. 2017;235:308–12.
Radparvar I, Ross MK. Barriers and facilitators of electronic patient portal uptake for asthma management. J Asthma. 2022;60(4):635–46. https://doi.org/10.1080/02770903.2022.2087190.
Turner K, Clary A, Hong YR, et al. Patient Portal Barriers and Group Differences: Cross-Sectional National Survey Study. J Med Internet Res. 2020;22(9):e18870. https://doi.org/10.2196/18870.
Figueroa CA, Luo T, Aguilera A, Lyles CR. The need for feminist intersectionality in digital health. Lancet Digit Health. 2021;3(8):526–33. https://doi.org/10.1016/s2589-7500(21)00118-7.
Matthews AK, Jung MY, Akufo J, et al. Barriers to Using a Patient Portal Among Low-income Patient Populations: A Qualitative Descriptive Study. J Health Care Poor Underserved. 2023;34(3):863–83.
Rabbani M, Nasiri M, Mowla A, et al. Mental Health Patient Portals Aimed at Depression: A Picture Close to Reality. Stud Health Technol Inform. 2023;311:45–53. https://doi.org/10.3233/shti200608.
Acknowledgements
Not applicable
Funding
This work was supported by the Health System Impact Fellowship from the Canadian Institutes of Health Research.
Author information
Authors and Affiliations
Contributions
The content of this manuscript was conceptualized by KD in collaboration with all authors. KD was responsible for drafting the original manuscript and overseeing revisions by the other authors. KD and HDS performed all screening and data extraction procedures, as detailed in the manuscript. KD, GS, HDS, and KTJ were thoroughly involved in revising the manuscript prior to submitting it for publication consideration. All authors agree regarding the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Durocher, K., Shin, H.D., Jackson, K.T. et al. Women’s experiences of using patient portals in healthcare settings: a rapid review. BMC Women's Health 24, 449 (2024). https://doi.org/10.1186/s12905-024-03292-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-024-03292-9