
Abstract
Background
Childhood victimization has been associated with long-term psychological effects and an increased risk of being victimized in later life. Previous research has primarily focused on sexual abuse during childhood, and a wide range of consequences have been identified. However, a significant gap remains in our understanding of the complex interaction between different forms of childhood abuse and violence in later life, particularly in the context of broader social stressors such as armed conflict and displacement.
Methods
This study examines the association between exposure to different types of childhood maltreatment in the context of family and intimate partner violence (IPV) among displaced women living in refugee camps in northern Iraq. Structured interviews were conducted by trained female psychologists with 332 women aged between 20 and 62 years.
Results
Results indicated that over one-third of the participating women reported experiencing at least one occurrence of IPV by their husbands within the past year. In addition, participants reported experiences of different types of maltreatment (physical, emotional, and sexual violence and physical and emotional neglect) perpetrated by family members in their childhood. While all forms of childhood maltreatment showed an association with IPV within the past year, only emotional childhood maltreatment was found to be a significant predictor of IPV in a multivariate analysis.
Conclusion
The study highlights the ongoing impact of child maltreatment and its contribution to increased vulnerability to IPV victimization in later life. In addition, this study describes the specific cultural and contextual elements that contribute to IPV in refugee camps.
Similar content being viewed by others

Background
Violence against children is an escalating global problem with profound societal implications. It is estimated that nearly one billion children between the ages of 2 and 17 have experienced physical, sexual, or emotional violence or neglect in the past year [1]. Beyond the immediate impact of such violence, it is critical to understand the lasting effects on a child’s life trajectory.
A growing body of evidence suggests that early exposure to violence can have lasting effects, increasing the risk of victimization both in childhood and later in life [2, 3]. This phenomenon, referred to as revictimization, has been studied extensively, particularly with regard to the association between childhood sexual abuse and subsequent vulnerability in adulthood. Empirical evidence, such as Walker et al.‘s (2019) meta-analysis of 80 studies involving 12,252 survivors of child sexual abuse, suggests that nearly half of these individuals were sexually victimized later in life [4]. This is consistent with Classen et al. (2005), who concluded in a review of 90 studies that a history of childhood sexual abuse significantly increased the risk of later sexual victimization [5]. Yet the literature has focused disproportionally on sexual abuse in particular, often overshadowing other forms of child victimization, such as emotional abuse and neglect, particularly within the family [6,7,8]. In light of the profound impact of different forms of abuse on the holistic development of children, shaping their emotional, cognitive, and social trajectories in distinctive ways, analysing them separately might yield relevant insights into the complex interplay between violence, revictimization and mental health.
Accordingly, a growing body of studies presents evidence that various forms of childhood maltreatment are related to victimization later in life [9, 10]. In one of these studies, experiences of emotional abuse increased the odds of a later victimization in females by 10%, even when controlling for physical and sexual abuse [11]. Furthermore, the statistical association between physical maltreatment and later victimization diminished when controlling for experiences of emotional maltreatment. Accordingly, it has been suggested that the mechanisms linking early life adversities to later life victimization differ between sexual, physical, and emotional maltreatment. For emotional forms, it has been suggested that deficits in emotion processing impair individuals’ abilities to respond appropriately to social interactions and form healthy relationships [11, 12].
Current research on childhood maltreatment is biased towards high-income countries, which significantly marginalizes the experiences and challenges faced by people residing in low- and middle-income countries (LMICs). This is a gap in the scientific discourse, especially given that an estimated 85% of the world’s population lives in LMICs [13]. It is therefore not only essential, but urgent to attempt for a more comprehensive understanding of the long-term psychosocial effects of child maltreatment in contexts of different cultural traditions, societal norms, and histories in LMICs.
A critical dimension that is often overlooked is the long history of collective and structural forms of violence, i.e., war, civil conflict, and political instability that many LMICs have endured. These historical traumas have been shown to be strongly related to social attitudes, family relationships, and mental health [14,15,16]. It seems the aftermath of war and conflict goes beyond the immediate physical and infrastructural damage and can leave lasting psychosocial marks on survivors for decades [17].
The interplay between violence on the societal level and individual experiences of child maltreatment can potentially magnify the harmful effects on victims. However, most of the existing studies conducted in LMICs, especially those dealing with post-conflict situations, tend to focus either on the effects of displacement - which include changes in social roles, domestic and intimate partner violence (IPV), the stresses of daily life, the intricacies of residency status - or instead investigate the psychological consequences of war, focusing on mental health conditions such as depression, anxiety, or post-traumatic stress disorder (PTSD) [18,19,20,21,22]. Such a binary perspective, which primarily addresses either post-displacement conditions or trauma experienced during war and displacement, may unintentionally overlook the intricate relationships between non-war-related life experiences, such as childhood events, and the emergence of other psychosocial issues among war-affected populations. A more integrative and holistic approach is needed to understand the complexities that arise from the linking of childhood experiences with larger societal events and historical trauma. For example, little research has attempted to understand how cultural norms, family characteristics and structures in LMICs, particularly in war-affected regions, regarding age of marriage, polygamy, and kinship marriage contribute to the later victimization such as IPV of women who have been maltreated in childhood.
IPV is one of the most common forms of violence against women, occurring across various societal contexts, both in stable and conflict-affected regions [23, 24]. The World Health Organization (WHO) estimates that approximately one-third of women globally experience IPV at some point in their lives, either from current or former partners [25]. However, the ensuing disruption and social breakdown that accompanies armed conflict often exacerbate structural violence like pre-existing gender inequalities, which may put women at increased risk of interpersonal violence from their intimate partners [26]. In both conflict and post-conflict settings, degraded social infrastructure, attitudes about women’s roles, diminished security, and rising economic pressures seem to exacerbate women’s vulnerability to IPV [27,28,29,30].
In this context, when examining the impact of interpersonal trauma on women, it is important to consider polyvictimization, which refers to the experience of multiple forms of violence in different contexts and at different times, including childhood maltreatment, IPV, and other war and non-war related traumatic events [31]. This notion emphasizes the intersectional nature of violence and recognizes that individuals may experience multiple, interacting, and compounding forms of violence [32]. Particularly, displaced women are likely face polyvictimization as the trauma of war and displacement intersects with personal histories of abuse, including IPV and other forms of gender-based violence [32, 33]. Such prolonged exposure to multiple forms of violence can have a significant impact on mental health, increasing the risk of depression, anxiety, PTSD, and other mental health disorders [34, 35].
Considering these factors, the present research focuses on exploring polyvictimization among Iraqi and Syrian refugee women. More specifically, this study attempts to examine the relationship between different forms of childhood maltreatment and IPV victimization, taking into account other traumatic events such as war, displacement, and events in their daily lives. Drawing parallels with global data [36], we hypothesize that experiences of childhood maltreatment are significantly associated with IPV exposure, indicating increased risk of re-victimization and ongoing cycles of violence.
Methods
Participants
The study sample consisted of 332 displaced married women living in the Arbat displacement camps in Iraqi Kurdistan. The age of the participants at the time of the interview ranged from 20 to 62 years (M = 38.68, SD = 7.05). Participants’ ages at the time they married ranged from 11 to 33 (M = 18.77, SD = 3.83), and the number of children per participant ranged between one and fourteen (M = 5.73, SD = 2.26). A significant proportion of participants (81.3%) were in marriages arranged by their parents. Approximately three in five women (59.6%) were married to relatives. In terms of employment status, the vast majority of women (96.7%) reported no employment and identified themselves primarily as homemakers. Additional details on the socio-demographic characteristics of the participants are provided in Table 1.
Procedure
Data for this study were collected through a comprehensive quantitative triadic family survey of displaced families from Iraq and Syria living in the Arbat camps in the Sulaymaniyah governorate of the Kurdistan Region of Iraq (KRI). The survey was conducted in March and April 2019, with trained paraprofessionals conducting interviews in participants’ tents or homes. All interviewers had at least a bachelor’s degree in psychology, they were fluent in both Kurdish and Arabic, and had an in-depth understanding of the culture and experiences of Iraqi and Syrian women.
Participants were recruited through the aforementioned survey. Detailed participant recruitment procedures have been described elsewhere [37, 38]. To protect the safety and privacy of participants who may have experienced IPV, the interviews were not framed as domestic violence investigations, but rather as general surveys exploring trauma, mental health, and the living conditions of displaced families. Women selected to participate were explicitly informed individually prior to beginning of the interviews that they would be asked about their childhood experiences and current IPV issues, in addition to questions about their war and displacement experiences, and all women consented. To ensure their confidentiality, the interviews were conducted in private locations where no one else was present during the interviews.
A comprehensive risk management process was implemented to protect both participants and staff. If a woman disclosed severe violence or mental health issues during the interview, immediate counselling was provided by staff trained in case management and mental health first aid. Participants were also referred to additional health care providers as needed to ensure continuity of care. All participating women were given contact information for emergency services and violence prevention hotlines at the end of the interview. They were also given information on how to reach local support organizations both inside and outside the camps. This approach ensured that participants had access to resources to seek help and support beyond the scope of the research study. Approval for the research was obtained from the respective ethics committees of the University of Bielefeld in Germany (reference number EUB 2015-046) and Koya University in KRI (reference number SHETC-1). In addition, the study and its protocols were approved by the local government authorities, including the camp administration, the Directorate of Social Affairs (DoSA) of the Ministry of Labor and Social Affairs, and the Protection Office of the Joint Crisis Coordination Center (JCC) of the Ministry of Interior in the KRI. A detailed description of the research procedures, ethical considerations, and risk management is described elsewhere [37, 39].
Instruments
The War and Adversity Exposure Checklist (WAEC) was used to assess potentially traumatic events that women had experienced in their lifetime [40]. The WAEC was specifically designed to capture the experiences of Middle Eastern populations, particularly those who have been displaced in Iraq and Syria. It includes 26 potentially traumatising events, including both war-related events, which comprise 10 items (such as witnessing armed combat or experiencing forced separation from family members due to war), and adverse life experiences, which comprise 16 items (including natural disasters and life-threatening illnesses). Participants were asked to indicate whether or not they had experienced each of these events. The Cronbach’s alpha coefficient for the WAEC in the current study was α = 0.77.
The Gendered Violence in Partnerships Scale (GVPS) was used to assess IPV reported by women within the past year [41]. The GVPS is a validated and reliable instrument developed specifically to measure IPV among Iraqi and Syrian women. It consists of 18 items that assess various aspects of IPV, including husbands’ controlling behaviors (e.g., controlling their clothing, preventing them from working or studying, and isolating them from family or friends), impulsive aggression, whether verbal or physical (e.g., name-calling, hitting, kicking, slapping, and punching), aggregated physical assaults (e.g., attempted strangulation, attempted murder, or assault with a weapon), and existential threats (e.g., threats of divorce or taking another wife/partner). Each item of the scale is answered with a binary yes or no response. The Cronbach’s alpha coefficient for the IPV checklist in this sample was α = 0.88.
Childhood maltreatment was assessed using a brief version of the Adverse Experiences Checklist at Home, which focuses on various negative events experienced at home [42]. The checklist consisted of 12 items related to physical, sexual, and emotional abuse and neglect by family members. Participants were asked to report whether they had ever experienced such events during their childhood. In addition, the checklist included two questions about the consequences of such maltreatment. Participants were asked whether they had ever been injured as a result of family violence and whether they had ever required medical treatment for injuries resulting from family violence. The Cronbach’s alpha coefficient in this sample was α = 0.86.
PTSD symptoms were assessed using the Kurdish and Arabic adaptations of the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5) [43,44,45]. The PCL-5 consists of 20 items that are consistent with the DSM-5 diagnostic standards for PTSD. Each item on the PCL-5 is rated on a five-point scale ranging from 0 (indicating “not at all”) to 4 (indicating “extremely”). According to the Kurdish and Arabic versions of the PCL-5, the optimal cut-off score for a probable diagnosis of PTSD is 23 [43]. The reliability of the PCL-5, as measured by Cronbach’s alpha coefficient in the context of this study, was reported to be α = 0.94.
Data analysis
The levels of different traumatic events experienced (war-displacement-related events, adverse life events, IPV, and childhood maltreatment) were assessed using descriptive statistics that analysed the frequency of each reported event. The prevalence of probable PTSD diagnosis was determined by applying a cut-off score of 23 on the Kurdish and Arabic version of PCL-5 and examining its frequency. Relationships between variables were examined using Spearman correlation coefficients.
Hierarchical regression analysis was conducted to investigate potential variables contributing to IPV experienced by women from their current husbands within the past year. In the first stage of the analysis, sociodemographic variables such as age, number of children, and the presence of kinship marriage were included. In the second stage of the regression model, we included the sum score of PTSD symptoms and the number of non-war adverse life events that women had previously experienced. In addition, sum scores of different forms of childhood maltreatment were also included in our model. Due to violations of the normality assumption for certain variables, such as the number of wives a husband has and the number of negative life events, bootstrapping was used in the regression analysis. This involved generating 1000 random resamples with replacement. Bootstrapping is a modern statistical approach specifically designed to correct for potential biases associated with non-normally distributed predictor and dependent variable data [46, 47] and to provide greater precision than traditional methods such as data transformations or classic nonparametric methods [48]. All analyses were performed using Statistical Package for the Social Sciences (SPSS) version 29 (IBM Corp.).
Results
IPV
Participating women reported that their husbands had perpetrated between 0 and 16 incidents of IPV in the past 12 months (M = 1.24, SD = 2.61). A total of 121 (36.4%) had experienced at least one act of IPV perpetrated by their husbands in the past 12 months.
Threats to remarry were the most commonly reported IPV event, affecting 18.1% of women. This was followed by name-calling, with an occurrence of 12%. Sexual objectification, which includes forcing a woman to become pregnant against her will or neglecting her needs during sex, was reported by 9.9% of women. Finally, physical violence, such as hitting, kicking, biting, punching, twisting arms, or pulling hair, was reported by 8.4% of participants (see Fig. 1).
Childhood maltreatment
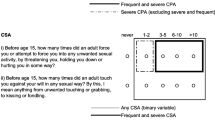
Participating women reported experiencing between 0 and 12 childhood maltreatment events (M = 1.11, SD = 2.08) perpetrated by their family members during their childhood. The most common forms of emotional maltreatment were verbal insults or yelling (24.4%) and verbal threats (19.6%). Physical abuse took several forms, including being hit with a hand (20.5%) or an object (8.1%) and having objects thrown at them (9.6%). An additional 2.7% reported experiencing sexual abuse, specifically rape, by immediate or extended family members during childhood. In addition, a small proportion of participants (0.6%) reported experiencing inappropriate touching of genitals by family members who were significantly older.
Childhood maltreatment resulted in serious physical injuries in 12% of participants, ranging from cuts and bruises to burns, fractures, and eye hematomas. In addition, 10.2% of participants reported the need for medical treatment due to the severity of the abuse they experienced. A detailed representation of the types of childhood maltreatment reported by participants is shown in Fig. 2.
Traumatic events and PTSD symptoms
90.9% of participants had experienced at least one lifetime traumatic event (M = 4.37, SD = 3.29; range: 0–20). War-related events were the most commonly reported events, with 88.5% of participants having experienced at least one war-related traumatic event (M = 2.94, SD = 2.02; range: 0–10) and 58.1% having experienced at least one non-war and adverse lifetime traumatic event (M = 1.41, SD = 1.83; range: 0–16). The mean PTSD symptom score on the PCL-5 was 23.85 (SD = 17.79). Using the contextually validated cut-off score of the PCL-5, half (50.09%) of the participants met criteria for a probable PTSD diagnosis.
Childhood maltreatment, trauma and PTSD symptoms predict IPV
Results from correlation coefficients indicate that childhood maltreatment was significantly correlated with IPV, number of non-war adverse life events, and symptoms of PTSD (rs = 0.39, rs = 33, and rs = 0.33, respectively; ps < 0.001), presented in Table 2. To predict last year’s IPV, using hierarchical regression analysis, potential predictors of IPV, including sociodemographic variables, lifetime history of trauma, symptoms of PTSD, and childhood maltreatment were examined. A significant association was found between increased IPV and polygamy. This was demonstrated by the number of additional wives a husband had. Conversely, variables such as kinship-based marriage and number of children were negatively correlated with levels of IPV. Furthermore, among the various types of childhood maltreatment, only emotional maltreatment was identified as a robust indicator of IPV (Table 3. presents a bootstrapped multiple hierarchical regression analysis for the prediction of IPV among the study sample).
Discussion
This study explores the relationship between exposure to childhood maltreatment and IPV victimization in adulthood among refugee women. The findings reveal that among displaced women interviewed in a refugee camp in northern Iraq, exposure to childhood maltreatment was associated with IPV victimization experienced in the past year. However, when accounting for trauma, PTSD, and demographic variables, only emotional childhood maltreatment emerged as a statistically significant predictor of IPV.
With 36% of participants reporting IPV in the past year, the results of our study are nearly four times higher than what a recent global review based on WHO data estimated - about 10% of women aged 15 and older experienced violence from an intimate male partner in the past year [49]. While there is a lack of meta-analyses providing accurate rates of IPV specifically against women in the Arab region, systematic reviews reveal that IPV rates vary significantly across Arab nations [50, 51] indicating a range of different social and socioeconomic factors influencing IPV occurrence in these countries. Examining the long-standing histories of conflict, political instability, and economic hardship in the region is necessary to understand IPV against women in Iraq and Syria. Notable events, including the Iran-Iraq War, Gulf Wars, US sanctions in 1990, the 2003 US invasion, post-Arab Spring war and displacement, and the rise of the Islamic State terrorist group, have significantly impacted the socioeconomic landscapes of the two countries. It is likely that these events have contributed to the emergence of diverse violent patterns including violence against women.
Research from other conflict-affected regions indicates a connection between war-induced forced displacement and a higher likelihood of IPV [52,53,54]. The instability of socio-economic conditions during war can shift power dynamics within households. For example, men may lose their primary role as breadwinners or suffer psychological trauma as a result of the conflict, which may lead to higher rates of IPV against women [30, 55,56,57]. Furthermore, living in refugee camps can increase women’s vulnerability to IPV. The refugee camp environments often present barriers to victims seeking formal protection and support, as broader family and community structures are disrupted. Furthermore, amidst the complexity of supply issues around basic needs, there seems to be a significant gap in the camps residents’ awareness of available protection services in the Iraqi and Syrian refugee context. While an increasing number of national and international NGOs are working with the government of Iraqi Kurdistan to address IPV, women often find it difficult to identify the right resources, leading to uncertainty about which organisations to approach for support. There seems to be an urgent need to establish clear and accessible service-mapping systems to ensure that all individuals, regardless of their educational background, can effectively identify and connect with service providers. In addition, while the study didn’t look in depth at the reasons why women might not report IPV to the authorities, feedback from the local research assistants who conducted the study’s interviews suggests that social stigma, fear and a lack of knowledge about the support available might prevent them from doing so.
The correlation and regression analyses showed significant statistic associations between exposure to childhood maltreatment, symptoms of PTSD, and IPV. This finding is consistent with numerical meta-analyses and systematic reviews, which indicated that exposure to childhood maltreatment increases the likelihood of mental health problems. For example, Norman et al. (2012) systematically reviewed and analysed 124 studies on the long-term mental health effects of child maltreatment and found indications for a causal relationship between child maltreatment and various mental health disorders, substance abuse, and suicide attempts [58]. These findings were also supported by a meta-analysis conducted by Gardner et al. (2019) on the association between child maltreatment and PTSD symptoms, which found that individuals exposed to child maltreatment had a threefold increased risk of PTSD [59]. Additionally, our study reveals that among various forms of childhood maltreatment, emotional childhood maltreatment is strongly associated with current PTSD symptoms. This finding underscores the significant psychological impact of childhood emotional maltreatment. Previous research has also confirmed this association, showing that emotional maltreatment has a significant and unique impact on adult mental well-being, over and above the effects of other forms of maltreatment. For instance, a recent meta-analysis and systematic review that included studies from the general population across various geographic regions found that emotional childhood maltreatment was associated with an increased risk of adulthood mental health problems, including depression, anxiety, PTSD, and other psychological symptoms [60]. Likewise, the correlation between childhood maltreatment and IPV aligns with earlier findings from meta-analyses (for review see [61,62,63]) indicating that experiencing maltreatment during childhood, and emotional maltreatment in particular, increases the likelihood of victimization by an intimate partner.
Although an association between past childhood maltreatment and recent IPV was observed in this study, it does not establish a causal relationship or clarify the potential mechanisms underlying the lasting psychological effects of childhood maltreatment, such as PTSD and revictimization. Meta-analyses suggest that child maltreatment may lead to emotional dysregulation, thereby enhancing the probability of developing PTSD and IPV in adulthood, particularly after experiencing other traumatic events [64, 65]. Longitudinal research indicates that emotion dysregulation is a significant predictor of the severity of common PTSD symptoms, such as intrusive memories, flashbacks, and distressing nightmares [66, 67]. Furthermore, emotional maltreatment disrupts attachment formation, leading to difficulty in developing secure relationships and obtaining support during times of distress [68]. This may also explain this study’s findings.
Our study has identified specific family characteristics and structures that are associated with IPV. Significantly, our findings demonstrate that women who marry at a young age and those who are in polygamous relationships are more likely to experience IPV. Although the practice of early marriages and polygamy is often allowed by legal and cultural norms in both Iraqi and Syrian societies, it is important to note that young brides may lack the resources and independence to address or escape from abusive partners. This observation is particularly relevant in less privileged regions of Iraq and Syria, where social norms and economic constraints are often incentives for early marriage [69]. In addition, the nature of polygamous relationships can lead to competition, jealousy, and complex power dynamics, all of which can potentially increase IPV [70].
Interestingly, our study found a significant link between having more children and experiencing less IPV among displaced Arab and Kurdish women. One explanation for this could be the cultural importance placed on family ties in Iraq and Syria, where larger families may strengthen these ties [71]. Such families often have a stronger sense of unity, resulting in shared household and childcare responsibilities among siblings. Notably, older children in Iraqi and Syrian households often contribute financially, which may reduce the likelihood of triggering IPV between the parents. In Iraqi and Syrian cultural traditions, marriage between close relatives, particularly cousins, is common. The results of the current study suggest that these marriages are associated with lower rates of IPV, possibly due to strong family support systems and established family ties. Further research is needed to clarify the influence of this cultural practice on family structure, family cohesion, and the quality of partner relationships.
This study addresses a commonly overlooked issue in war-traumatized and displaced populations by examining associations between childhood maltreatment and current IPV among displaced women from Syria and Iraq. The findings provide important insights into the challenges faced by women in refugee camps. The strength of the study is enhanced by the involvement of trained female psychologists in conducting interviews and the application of valid and reliable screening instruments. This methodology created a supportive environment for discussing sensitive topics such as domestic violence, which likely enhanced the depth and comprehensiveness of the data. However, a number of limitations of this study have to be noted. Even with trained local interviewers’ involvement, participants’ responses might be influenced by deep-seated feelings of shame, mistrust, and the social stigma related to domestic violence. These deep-rooted emotions may impact the accuracy of reported childhood maltreatment and IPV rates. Moreover, the cross-sectional design of our study limits our ability to determine causal relationships among childhood maltreatment, IPV, and mental health issues. The assessment instruments used in this study to evaluate IPV and childhood maltreatment had limitations that may have limited the depth and precision of the conclusions drawn from our findings. These instruments did not provide a complete evaluation of the frequency and severity of different types of abuse. Rather, they focused on identifying whether women had experienced abuse or not. Understanding the frequency, chronicity, and severity of abusive acts is crucial for understanding the intricacies of marital dynamics and for distinguishing between different forms of abuse, such as intimate terrorism and isolated incidents in the context of conflict. Also, the specific displacement context in Iraq limits the generalizability of our findings to other populations. The study also did not explore potential mediating or moderating factors between childhood maltreatment and its long-term negative impacts, such as emotional regulation or attachment styles or perceptions of violence which should be researched using qualitative methods as well.
Future research initiatives should use a longitudinal methodology that integrates both qualitative and quantitative approaches to better understand the long-term effects of childhood trauma on mental health and the risk of re-victimization in adulthood. In addition, our understanding of these lasting effects will be enhanced by studying diverse cultural populations.
Moreover, in a practical term, addressing the needs of refugee populations suffering from IPV requires a multidimensional and socio-ecological approach that considers individual, family and structural level factors. At the individual level, all psychosocial interventions should be culturally sensitive and trauma-informed, recognizing that refugees’ experiences may be influenced by their cultural backgrounds, historical trauma, and their own individual past trauma. In addition, it is essential to provide access to mental health support and counselling services that are tailored to the specific needs of each woman survivor of IPV and child maltreatment. Interventions at the family level should focus on addressing the dynamics within refugee families affected by IPV. This can be facilitated through family counselling, parenting support, and educational programs aimed at promoting healthy relationships and communication. Furthermore, survivors should be empowered within their families and communities and provided with the necessary tools to break the cycle of violence. Lastly, interventions should address the systemic challenges faced by refugee women at the structural and societal levels. These challenges include limited access to health care, legal barriers, and social isolation. Collaboration with community organizations, advocacy groups, and policymakers is essential to creating an empowering environment that facilitates women refugees’ access to resources, support, and protection.
Conclusion
The current study highlights the multifaceted interplay between childhood maltreatment and IPV within the specific sociocultural context of displaced women from Iraq and Syria. While the findings are consistent with previous literature on impacts of childhood trauma, they also highlight the need for in-depth scientific research and the formulation of interventions to address the unique needs and challenges of displaced women and their communities.

Percentage of IPV perpetrated by husbands in the past 12 months

Percentage of reported childhood maltreatment perpetrated by family member
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to the terms of consent agreed upon by the participants. However, they are available from the corresponding author upon reasonable request.
Abbreviations
- IPV:
-
Intimate Partner Violence
- PTSD:
-
Post-Traumatic Stress Disorder
- WAEC:
-
War and Adversity Exposure Checklist
- PCL-5:
-
PTSD Checklist for DSM-5
- GVPS:
-
Gendered Violence in Partnerships Scale
- KRI:
-
Kurdistan Region of Iraq
References
Hillis S, Mercy J, Amobi A, Kress H. Global prevalence of past-year violence against children: a systematic review and minimum estimates. Pediatrics. 2016;137.
Finkelhor D, Ormrod RK, Turner HA. Re-victimization patterns in a national longitudinal sample of children and youth. Child Abuse Negl. 2007;31:479–502.
Scrafford KE, Grein K, Miller-Graff LE. Legacies of Childhood victimization: Indirect effects on adult Mental Health through Re-victimization. J Child Adolesc Trauma. 2018;11:317–26.
Walker HE, Freud JS, Ellis RA, Fraine SM, Wilson LC. The prevalence of sexual revictimization: a Meta-Analytic Review. Trauma Violence Abuse. 2019;20:67–80.
Classen CC, Palesh OG, Aggarwal R. Sexual revictimization: a review of the empirical literature. Trauma Violence Abuse. 2005;6:103–29.
Glaser D. Emotional abuse and neglect (psychological maltreatment): a conceptual framework. Child Abuse Negl. 2002;26:697–714.
Higgins DJ, McCabe MP. Multiple forms of child abuse and neglect: adult retrospective reports. Aggress Violent Behav. 2001;6:547–78.
Spinazzola J, Hodgdon H, Liang L-J, Ford JD, Layne CM, Pynoos R, et al. Unseen wounds: the contribution of psychological maltreatment to child and adolescent mental health and risk outcomes. Psychol Trauma. 2014;6(Suppl 1):S18–28.
Seedat S, Stein MB, Forde DR. Association between Physical Partner Violence, Posttraumatic Stress, Childhood Trauma, and suicide attempts in a community sample of women. Violence Vict. 2005;20:87–98.
Crawford E, O’Dougherty Wright M. The impact of childhood psychological maltreatment on interpersonal schemas and subsequent experiences of relationship aggression. J Emotional Abuse. 2007;7:93–116.
Richards TN, Tillyer MS, Wright EM. Intimate partner violence and the overlap of perpetration and victimization: considering the influence of physical, sexual, and emotional abuse in childhood. Child Abuse Negl. 2017;67:240–8.
Iffland B, Neuner F. Varying cognitive scars – Differential associations between types of Childhood Maltreatment and facial emotion Processing. Front Psychol. 2020;11:1–12.
World Bank. World Development Indicators. Washington, D.C.; 2022.
Elias A, Brown AD. The role of intergenerational family stories in mental health and wellbeing. Front Psychol. 2022;13.
Mutuyimana C, Maercker A. Clinically relevant historical trauma sequelae: a systematic review. Clin Psychol Psychother. 2023;30:729–39.
Mohatt NV, Thompson AB, Thai ND, Tebes JK. Historical trauma as public narrative: a conceptual review of how history impacts present-day health. Soc Sci Med. 2014;106:128–36.
Neldner S, Noori R, Mahmood HN, Neuner F, Ibrahim H. Evaluation of Social Acknowledgment and Mental Health among kurdish survivors of genocide in 1988. JAMA Netw Open. 2023;6:e2328793–2328793.
Steel Z, Chey T, Silove D, Marnane C, Bryant RA, Van Ommeren M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: a systematic review and meta-analysis. JAMA. 2009;302:537–49.
Morina N, Akhtar A, Barth J, Schnyder U. Psychiatric disorders in refugees and internally displaced persons after forced displacement: a systematic review. Front Psychiatry. 2018;9:433.
Buvinic M, Das Gupta M, Casabonne U, Verwimp P. Violent conflict and gender inequality: an overview. World Bank Res Obs. 2013;28:110–38.
Alfadhli K, Drury J. Psychosocial support among refugees of conflict in developing countries: a critical literature review. Intervention. 2016;14:128–41.
Murphy M, Ellsberg M, Balogun A, García-Moreno C. Risk and Protective Factors for Violence against Women and girls living in conflict and natural disaster-affected settings: a systematic review. Trauma Violence Abuse. 2022. 15248380221129304.
Devries KM, Mak JYT, García-Moreno C, Petzold M, Child JC, Falder G et al. The Global Prevalence of Intimate Partner Violence Against Women Data from 81 countries was used to estimate global prevalence of intimate partner violence against women. Science (1979). 2016;8.
Román-Gálvez RM, Martín-Peláez S, Fernández-Félix BM, Zamora J, Khan KS, Bueno-Cavanillas A. Worldwide Prevalence of intimate Partner violence in pregnancy. A systematic review and Meta-analysis. Front Public Health. 2021;9.
World Health Organization. Global status report on violence prevention 2014. Genève, Switzerland: World Health Organization; 2014.
United Nations. In-depth study on all forms of violence against women Report of the Secretary-General. A/61/122/Add.1. 2006.
Cardoso LF, Gupta J, Shuman S, Cole H, Kpebo D, Falb KL. What Factors Contribute to Intimate Partner Violence Against Women in Urban, Conflict-affected settings? Qualitative findings from Abidjan, Côte d’Ivoire. J Urb Health. 2016;93:364–78.
Wachter K, Horn R, Friis E, Falb K, Ward L, Apio C, et al. Drivers of intimate Partner Violence Against women in three Refugee Camps. Violence against Women. 2017;24:286–306.
Goessmann K, Ibrahim H, Neuner F. Association of War-related and Gender-Based Violence with Mental Health States of Yazidi Women. JAMA Netw Open. 2020;3:e2013418–2013418.
Goessmann K, Ibrahim H, Saupe LB, Ismail AA, Neuner F. The contribution of mental health and gender attitudes to intimate partner violence in the context of war and displacement: evidence from a multi-informant couple survey in Iraq. Soc Sci Med. 2019;237(July):112457.
Finkelhor D, Ormrod RK, Turner HA. Poly-victimization: a neglected component in child victimization. Child Abuse Negl. 2007;31.
Grasso DJ, Dierkhising CB, Branson CE, Ford JD, Lee R. Developmental patterns of adverse childhood experiences and current symptoms and impairment in Youth Referred for Trauma-Specific services. J Abnorm Child Psychol. 2016;44.
Im H, Swan LET, Heaton L. Polyvictimization and mental health consequences of female genital mutilation/circumcision (FGM/C) among Somali refugees in Kenya. Women Health. 2020;60.
Nam B, Lee Y, Bright C, Negi N. Polyvictimization and psychological outcomes among North Korean Refugee women. Violence against Women. 2022;28.
Bradel-Warlick L, Rosenbaum A. Poly-victimization: The Co-occurrence of Intimate Partner Violence with Other Forms of Aggression. In: Handbook of Interpersonal Violence and Abuse Across the Lifespan: A Project of the National Partnership to End Interpersonal Violence Across the Lifespan (NPEIV). 2021.
Devries KM, Mak JYT, García-Moreno C, Petzold M, Child JC, Falder G et al. The Global Prevalence of Intimate Partner Violence Against Women. Science (1979). 2013;340:1527–8.
Ibrahim H, Goessmann K, Neuner F. Sharing for relief: associations of trauma-focused interviews and well-being among war-affected displaced populations in the Middle East. https://doi.org/101080/1050842220222122466. 2022;:1–17.
Ibrahim H, Catani C, Neuner F. The posttraumatic stress interview for children (KID-PIN): development and validation of a semi-structured interview of PTSD symptoms among displaced children in the Middle East. PeerJ. 2021;9.
Ibrahim H, Catani C, Neuner F. The posttraumatic stress interview for children (KID-PIN): development and validation of a semi-structured interview of PTSD symptoms among displaced children in the Middle East. PeerJ. 2021;9:e12403.
Ibrahim H, Ertl V, Catani C, Ismail AA, Neuner F. Trauma and perceived social rejection among yazidi women and girls who survived enslavement and genocide. BMC Med. 2018;16:1–11.
Goessmann K, Ibrahim H, Saupe LB, Neuner F. Toward a Contextually Valid Assessment of Partner Violence: Development and Psycho-Sociometric evaluation of the gendered violence in partnerships Scale (GVPS). Front Psychol. 2021;11:3840.
Catani C, Jacob N, Schauer E, Kohila M, Neuner F. Family violence, war, and natural disasters: a study of the effect of extreme stress on children’s mental health in Sri Lanka. BMC Psychiatry. 2008;8:1–10.
Ibrahim H, Ertl V, Catani C, Ismail AA, Neuner F. The validity of posttraumatic stress disorder checklist for DSM-5 (PCL-5) as screening instrument with kurdish and arab displaced populations living in the Kurdistan region of Iraq. BMC Psychiatry. 2018;18:1–8.
Ibrahim H, Neuner F. Network structure of DSM-5 PTSD symptoms: results from cross-national survey among Iraqi and Syrian displaced people. Asian J Psychiatr. 2020;54:102307.
Ibrahim H, Catani C, Ismail AA, Neuner F. Dimensional structure and cultural invariance of DSM V post-traumatic stress disorder among Iraqi and Syrian displaced people. Front Psychol. 2019;10 JULY:1505.
Chernick MR. Bootstrap Methods:A Guide for Practitioners and Researchers. 2nd edition. John Wiley & Sons; 2008.
Fox J. Applied regression analysis and generalized linear models. 3rd edition. SAGE Publications, Inc.; 2016.
Erceg-Hurn DM, Mirosevich VM. Modern Robust Statistical Methods: An Easy Way to Maximize the Accuracy and Power of Your Research. American Psychologist. 2008;63.
Sardinha L, Maheu-Giroux M, Stöckl H, Meyer SR, García-Moreno C. Global, regional, and national prevalence estimates of physical or sexual, or both, intimate partner violence against women in 2018. Lancet. 2022;399.
Elghossain T, Bott S, Akik C, Obermeyer CM. Prevalence of intimate partner violence against women in the arab world: a systematic review. BMC Int Health Hum Rights. 2019;19.
Kisa S, Gungor R, Kisa A. Domestic Violence Against Women in North African and Middle Eastern Countries: A Scoping Review. Trauma, Violence, and Abuse. 2023;24.
Sharma V, Amobi A, Tewolde S, Deyessa N, Scott J. Displacement-related factors influencing marital practices and associated intimate partner violence risk among Somali refugees in Dollo Ado, Ethiopia: a qualitative study. Confl Health. 2020;14.
Black E, Worth H, Clarke S, Obol JH, Akera P, Awor A et al. Prevalence and correlates of intimate partner violence against women in conflict affected northern Uganda: a cross-sectional study. Confl Health. 2019;13.
Eseosa Ekhator-Mobayode U, Hanmer LC, Rubiano-Matulevich E, Jimena Arango D. The effect of armed conflict on intimate partner violence: evidence from the Boko Haram insurgency in Nigeria. World Dev. 2022;153.
Krause U. A continuum of violence? Linking sexual and gender-based violence during conflict, Flight, and encampment. Refugee Surv Q. 2015;34.
Sigona N. Everyday statelessness in Italy: status, rights, and camps. Ethn Racial Stud. 2016;39.
Machisa MT, Christofides N, Jewkes R. Structural pathways between child abuse, poor mental health outcomes and male-perpetrated intimate partner violence (IPV). PLoS ONE. 2016;11.
Norman RE, Byambaa M, De R, Butchart A, Scott J, Vos T. The Long-Term Health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and Meta-analysis. PLoS Med. 2012;9.
Gardner MJ, Thomas HJ, Erskine HE. The association between five forms of child maltreatment and depressive and anxiety disorders: a systematic review and meta-analysis. Child Abuse Negl. 2019;96.
Xiao Z, Murat Baldwin M, Wong SC, Obsuth I, Meinck F, Murray AL. The Impact of Childhood Psychological Maltreatment on Mental Health Outcomes in Adulthood: a systematic review and Meta-analysis. Trauma Violence Abuse. 2022. https://doi.org/10.1177/15248380221122816.
Herrenkohl TI, Fedina L, Roberto KA, Raquet KL, Hu RX, Rousson AN et al. Child Maltreatment, Youth Violence, Intimate Partner Violence, and Elder Mistreatment: A Review and Theoretical Analysis of Research on Violence Across the Life Course. Trauma, Violence, and Abuse. 2022;23.
Li S, Zhao F, Yu G. Childhood maltreatment and intimate partner violence victimization: a meta-analysis. Child Abuse Negl. 2019;88.
Zhu J, Exner-Cortens D, Dobson K, Wells L, Noel M, Madigan S. Adverse childhood experiences and intimate partner violence: a meta-analysis. Dev Psychopathol. 2023;:1–15.
Dvir Y, Ford JD, Hill M, Frazier JA. Childhood maltreatment, emotional dysregulation, and psychiatric comorbidities. Harv Rev Psychiatry. 2014;22:149–61.
Gruhn MA, Compas BE. Effects of maltreatment on coping and emotion regulation in childhood and adolescence: a meta-analytic review. Child Abuse Negl. 2020;103:104446.
Pencea I, Munoz AP, Maples-Keller JL, Fiorillo D, Schultebraucks K, Galatzer-Levy I et al. Emotion dysregulation is associated with increased prospective risk for chronic PTSD development. J Psychiatr Res. 2020;121.
Timmer-Murillo S, Schramm AT, Geier TJ, Mcleod E, Larson CL, deRoon-Cassini TA. Facets of emotion dysregulation differentially predict depression and PTSD symptom severity following traumatic injury. Eur J Psychotraumatol. 2023;14.
Riggs SA. Childhood emotional abuse and the attachment system across the life cycle: what theory and research tell us. J Aggress Maltreatment Trauma. 2010;19.
Saleh AM, Othman SM, Ismail KH, Shabila NP. Exploring Iraqi people’s perception about early marriage: a qualitative study. BMC Womens Health. 2022;22.
Ahinkorah BO. Polygyny and intimate partner violence in sub-saharan Africa: evidence from 16 cross-sectional demographic and health surveys. SSM Popul Health. 2021;13.
Ibrahim H, Goessmann K, Araz ·, Ahmad R, Ayoub ·, Saeed K et al. Predictors of mental health symptomatology among Kurdish patients who recovered from COVID-19 in Iraq. Discover Psychology 2022 2:1. 2022;2:1–7.
Acknowledgements
We express our sincere appreciation to the women who participated in this study. We would also like to acknowledge the assistance and support of the local authorities, including the Sulaymaniyah Government Office and Sulaymaniyah’s Joint Crisis Coordination, as well as the camp managers of the Arbat camps. We acknowledge the financial support provided by the German Research Foundation (DFG) and the Open Access Publication Fund of Bielefeld University for covering the article processing charge.
Funding
Funding for this study was provided by the Volkswagen Foundation (grant number 91474-2).
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Hawkar Ibrahim and Frank Neuner: were co-principal investigators and secured the funding for the study. Hawkar Ibrahim: conceptualized and designed the study, managed the research project, trained local interviewers, supervised data collection, conducted statistical analyses, interpreted the data, and wrote the manuscript. Hawkar Ibrahim and Katharina Goessmann: managed the study’s data. Katharina Goessmann: participated in fieldwork and provided critical feedback on the manuscript. Frank Neuner and Benjamin Iffland: contributed substantially to the structure of the manuscript and provided critical feedback on the manuscript. All authors have reviewed and approved the final manuscript for submission and publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for this study was granted by the ethical review boards of both Bielefeld University in Germany (reference number: EUB 2015-046) and Koya University in Iraqi Kurdistan (reference number: SHETC-1).
Consent for publication
Not applicable.
Informed consent
Verbal informed consent was obtained from participants using a standardized written consent form. The interviewers confirmed each participant’s consent by signing the consent form. The verbal informed consent procedure was approved by the ethics committees of both the University of Bielefeld, Germany (reference number EUB 2015-046) and Koya University in the Kurdistan Region of Iraq (reference number SHETC-1).
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ibrahim, H., Goessmann, K., Neuner, F. et al. Continuous chains: childhood maltreatment and intimate partner violence victimization among displaced women in a war context. BMC Women's Health 24, 319 (2024). https://doi.org/10.1186/s12905-024-03156-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-024-03156-2