
Abstract
Background
Primiparous women experience various challenges if not provided with social support in the early postpartum period. Support in form of postpartum education programs is needed to improve mental well-being in primiparous women. The aim of this study was to determine the effect of a postnatal supportive education program for husbands on the perceived social support (primary outcome), and stress and maternal self-efficacy (secondary outcome) of their primiparous wives.
Methods
This randomized clinical trial was performed on pregnant women referring to healthcare centers for routine care from September to November 2021 in Kermanshah, Iran. One hundred pregnant women were randomly divided in to intervention and control groups. Four 45–90 min online training sessions were held weekly for the husbands of the intervention group. The primiparous women completed the Postpartum Partner Support Scale, Perceived Stress Scale, and Postpartum Parental Expectations Survey before (third day after delivery, immediately and one month after completing the intervention. Data were analyzed using Fisher's exact test, Chi-square test, independent t-test, and repeated measures analysis of variance in SPSS version 24, and p < 0.05 was considered statistically significant.
Results
In the control and intervention groups before the intervention, socio-demographic characteristics (P > 0.05), the mean scores of perceived social support (P = 0.11), maternal self-efficacy (p = 0.37) and perceived stress (p = 0.19) were not statistically significant. However, in the intervention group compared to the control group the mean scores of perceived social support (79.42 ± 7.17 vs. 37.26 ± 7.99, P < 0.001), maternal self-efficacy (186.22 ± 39.53 vs. 106.3 ± 32.88, P < 0.001) and perceived stress (16.36 ± 6.65 vs. 43.3 ± 7.39, P < 0.001) immediately after the intervention and the mean scores of perceived social support (84.4 ± 5.91 vs. 37.14 ± 6.63, P < 0.001), maternal self-efficacy (191.24 ± 38.92 vs. 112.34 ± 37.12, P < 0.001) and perceived stress (13.98 ± 4.84 vs. 39.06 ± 7.25, P < 0.001) one month after the intervention changed significantly.
Conclusion
The postpartum supportive education program for husbands was effective in promoting social support for primiparous women. Thus it can be introduced as routine care in the postpartum period.
Trial registration
Clinical trial registration Iranian Registry of Clinical Trials; https://en.irct.ir/user/trial/56451/view (IRCT20160427027633N8), registered (15/06/2021).
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
The early postpartum period is an exciting and joyful time for many parents, yet it is a stressful transient period during which most primiparous women face a variety of physical and emotional challenges, including fatigue and difficult responsibilities of caring for the baby and profound changes in the couple's roles and responsibilities [1].
The postpartum period is characterized by the vulnerability of primiparous women to stress. Postpartum stress not only impairs the health of primiparous women but also reduces their self-esteem, impedes adaptation to the role of mother, and impairs maternal bond with the baby [2]. Common stressors of the postpartum period include breastfeeding problems, sleep deprivation, fatigue, responsibility for caring for the baby, hormonal changes, and lack of social support [3].
Maternal self-efficacy refers to the mother’s belief in her abilities as an efficient mother and is greatly influenced by the sense of motherhood, self-confidence and perception of empowerment [4]. High self-efficacy is associated with positive thoughts, higher self-esteem, better adjustment, and more positive emotions [5]. Various studies have shown a negative relationship between maternal self-efficacy and maternal stress and postpartum depression [1, 6]. Some studies have shown that education during pregnancy is insufficient for the woman to play the maternal role and has no effect on maternal skills [7, 8].
Barnard (1994) emphasizes the importance of social support in the first year after childbirth [9]. Perceived social support refers to the amount of love, companionship, care, respect, attention, and help a person receives from others, such as family members, friends, etc. [10] There are three main types of social support: 1. Emotional support, which means having someone available to rely on and trust when needed. 2- Information support, which indicates receiving useful information (including guidelines, suggestions, advice, and feedback) from others to adapt to personal problems, and 3- Instrumental support, which is the material, objective and actual help received by a person from others [11]. A previous study found that pregnant women who received high social support from their husbands during pregnancy experienced less stress [12].
The results of a randomized controlled trial demonstrated the effectiveness of the postnatal psychoeducation program in improving maternal parental self-efficacy, social support and reducing postnatal depression of primiparous women [13]. Also, various studies have shown that social support is negatively correlated with the risk of postnatal depression [14, 15]. Hence, providing strong social support to primiparous women can potentially prevent them from developing postnatal depression (PND). Supportive interventions can be facilitated by providing social support in the form of education and maintaining the continuity of cares postnatal [16]. Shorey et al. (2017) demonstrated that the educational programs based on mobile applications are effective in improving parental self-efficacy and social support, recommending it to be introduced and performed by nurses in routine care [17]. However, the provision of supportive interventions is not widely practiced during the postnatal period as the focus has been mainly limited to pregnancy and childbirth [18]. Primiparous women often cite their family members, especially their husbands, as the main source of social support [1]. According to the opinion of most women, a woman's husband is the most important and closest person who can support her in coping with the problems by carefully understanding her sensitive psychological and physical condition [19]. Fletcher et al. showed that fathers’ participation in classes before delivery was effective in their supportive role [20]. The results of various studies have shown that fathers’ participation in pregnancy and childbirth care has positive consequences for the mother and baby, including reduced maternal stress, pregnancy complications (e.g., preterm delivery) and fear of childbirth, proper weight gain of premature infants, and successful breastfeeding. This is even true with long-term effects such as improved language learning and children’s academic achievement [21, 22]. Various studies recommended husband counseling and education as effective interventions to increase social support for pregnant and postpartum women [23,24,25,26].
In some Western countries, mothers and their infants are discharged early to facilitate family-centered postnatal care and encourage a sense of parental involvement. [27] In Iran, the average length of hospital stay of mothers after childbirth is 1 to 2 days [28]. Due to the mother’s short stay in the hospital, there is not sufficient time for educational interventions [17]. Moreover, the period immediately after delivery is not a good opportunity for education due to the discomfort that mothers experience during this period [29]. Parents are often overwhelmed by the amount of information they are given during their short hospital stay. Some complain that they have difficulty retaining this information after discharge and prefer to receive the information continuously after discharge early in the postpartum period [27]. To address these issues, healthcare providers need to develop the knowledge and tools needed to improve the quality of postnatal care that parents expect [30].
Given the importance of primiparous women’s mental health in facilitating adaptation to changes and new roles in the during the postpartum period, many husbands have a vital and decisive role in supporting their wives during this period. However, there is no sufficient time to provide all the necessary information in a short period of hospitalization, and according to a conducted survey, no study was found on the effectiveness of a postnatal supportive education program for husbands on perceived social support, stress and maternal self-efficacy of their primiparous wives. Therefore, the present study was conducted to determine the effect of a postnatal supportive education program for husbands on perceived social support (primary outcome), and stress and maternal self-efficacy (secondary outcome) of their primiparous wives.
Hypothesis of study
Education to the husbands of primiparous women will lead increased perceived social support and maternal self-efficacy and reduced stress of these women in the postpartum period.
Primary aim
Determine the effect of a postnatal supportive education program for husbands on perceived social support of their primiparous wives.
Secondary aim
Determine the effect of a postnatal supportive education program for husbands on stress and maternal self-efficacy of their primiparous wives.
Methods
Study design and participants
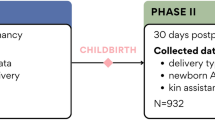
This randomized, controlled clinical trial study using two parallel groups was performed on 100 pregnant women referring to health centers in Kermanshah, Iran from September to November 2021. Figure 1 shows the CONSORT flowchart of the study. Women meeting the following criteria were eligible to participate in the study: first pregnancy, singleton term pregnancy, willingness to participate in the study, married and living with her husband, husband’s willingness to participate in the study, media literacy (familiarity with how the Skype app works), having a smartphone, knowing how to install and work with Skype, access to the Internet, and being available at least within the next 8 weeks. Exclusion criteria included: being husband's unable or unsure of the ability to attend all training sessions, presence of cardiovascular disease, high blood pressure, liver disease, diabetes or other chronic diseases (as reported by the woman), neuropsychiatric diseases, having recent calamities for the participant’s first-degree relatives (as reported by the woman) (such as death or incurable disease), and attending similar training or counseling classes by the husband before the study.

CONSORT flowchart of the study
Sample size calculation
The sample size was calculated based on the main variable of the study (social support) according to Khanzadeh and Moghaddam Tabrizi [31] using the following formula with type I error (α) set as two-sided 5% (Z1 − α/2 = 1.96), type II error (β) set as 20% (Z1 − β = 0.85) and power of 80%. The sample size for both groups was obtained 86 subjects and considering a 10% attrition rate, the final sample size was calculated to be 96 for both groups (48 each). Based on the opinion of the research team, we rounded the number 96 to 100 (50 each group).
μ1: mean difference of the social support in the intervention group (11.25), μ2: mean difference of the social support in the control group (4.95), SD1: standard deviation of the social support before intervention (14.21), and SD2: standard deviation of the social support after intervention (\(10.00\)).
Sampling and random allocation method
The present study was approved by the committee of ethics of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1399.401) and was registered in Iranian Registry of Clinical Trials (IRCT20160427027633N8). First, According to the information of Kermanshah health center, Kermanshah city was divided into 4 geographical regions (or 4 classes) based on socio-economic status of the residents. These four regions included 76 healthcare centers, and from the healthcare centers of each region, one was selected by simple random method (drawing lots). These centers were Taleghani, Hafezieh, Shahid Souri, and Haj Daei, from which 28, 34, 22, and 16 women were selected by convenience sampling method (based on the share of each center). After making the necessary arrangements and obtaining a permit, the researcher went to these centers and selected eligible women. In this way, by referring to the Sib system, information about the women who were covered by the center and met the study entry criteria was extracted and they were contacted by phone to come to the health center to participate in the study. The study aims and method were explained to pregnant women and their husbands in a face-to-face meeting and informed written consent was gained from them (pregnant women and their husbands). The telephone numbers of the women and their husbands were taken, and the researcher gave her telephone number to them, and they were advised to inform the researcher when the mother gave birth to the baby. After the women completed the questionnaires online on the third day after delivery, the educational content was offered to the intervention group. It should be noted that the membership of the husbands in the virtual (Skype) group was monitored by checking whether or not they had installed Skype on their cellphones, and in case they had not, it was installed on their cellphones. Necessary training on how to use Skype was given to them.
The women were randomly divided into 6 blocks with an allocation ratio of 1:1 to the intervention and control groups. Blocked randomization was performed by a person who was not involved in data collection, and in order to conceal random allocation, opaque sealed packets in random sequence were used. To this aim, first, a random sequence was created by a table of random numbers and recorded on a card and the cards were placed in packets according to the random sequence. Packets were opened in the order of woman entry in the study and they were allocated into either the intervention or control group. Data analysis was performed by a statistician who was unaware of the nature of the codes. Due to the nature of the intervention, it was not possible to blind neither the participants nor the researchers.
Intervention
Training was performed for intervention group in Skype. While the control group received only routine care. Training involved 4 online sessions of 45 to 90 min in Skype, held weekly (one session per week) by the researcher. Due to the different nature of education on natural childbirth and cesarean section, the women in the intervention group were divided according to the type of delivery (32 women who were supposed to have a normal delivery were in 4 groups of 8, and 18 women who were going to deliver their baby by a cesarean section were in 3 groups of 6). Topics of training sessions included: first session: the importance of maternal health in the postpartum period and the importance of social support for the mother in this period, second session: anatomical and physiological changes in the postpartum period, the impact of these changes on the mothers mental state, and the way she should be cared for, third session: baby care, the principles of breastfeeding and how to deal with its challenges, fourth session: the father’s responsibilities in the postpartum period and his supportive role in helping mothers adapt to changes (Interventional group educational content sessions are available in Additional file 1: Table 1).
The educational content was prepared by referring to the available library resources and with the guidance of supervisors and consultants and also based on the instructions and guidelines of the Iranian Ministry of Health. The validity of the educational content was evaluated qualitatively and approved by 10 relevant experts and faculty members related to the subject under study, including four reproductive health specialists, one midwifery specialists, three gynecologists and two psychologists. Each week after the review session, the content was presented in text, video and audio formats to the intervention group until the next session. Meetings were held upon agreement of the husbands. Each week, the researcher reminded the audience of the time of the training sessions by phone and text messages. In addition, the intervention group provided access to the researcher to ask questions via WhatsApp. Immediately and one month after completing the intervention (i.e., the fourth and eighth weeks after delivery), the questionnaire was completed by primiparous women online. In the end, in order to observe the ethical considerations, the educational materials were provided to the control group.
Study outcomes
In this study, the study outcomes (primary outcome: social support and secondary outcome: maternal self-efficacy and stress) were measured at three time intervals: baseline or before intervention (third day after delivery), immediately after the intervention (fourth week after delivery), and one month after the intervention (eighth week after delivery). The outcome measures were completed by primiparous women online.
Data collection tools
Data collection tools included socio-demographic questionnaire, Postpartum Partner Support Scale, Perceived Stress Scale, and Postpartum Parental Expectations Survey.
Socio-demographic questionnaire
This questionnaire includes questions related to age, husband’s age, age gap with husband, educational of the woman and her husband, employment status of the woman and her husband, economic status, husband’s disease, weight at birth, type of baby feeding, breastfeeding problems, delivery method, pregnancy status, and baby’s gender and parental satisfaction with.
Primary outcome
Postpartum Partner Support Scale (PPSS)
This scale was developed in 2017 by Dennis et al. This questionnaire has a four-point Likert scale (from strongly disagree: 1 to strongly disagree: 4). Scores of this questionnaire range from 20 to 100, and higher scores indicate receiving higher husband support in the postpartum period [32]. The reliability of this questionnaire in the original version was reported by obtaining a Cronbach’s alpha coefficient of 0.96 [23]. In Iran, Moghaddam Tabrizi and Khanzadeh (2020) reported a Cronbach’s alpha of 0.96, an internal stability index was 0.7, and alpha and reliability of 0.98. Also, the content validity index (CVI) and the content validity ratio (CVR) of this scale were 70% and 81%, respectively, which are both acceptable [31].
Secondary outcome
Postpartum Parental Expectations Survey (PPES)
This scale designed by Reese in 1992, was used to measure maternal self-efficacy. This questionnaire has 25 affirmatively worded items scored based on a 10-point Likert scale (from I can't: 1 to I definitely can: 10). The minimum score of this questionnaire is 25 and the maximum is 250, with scores less than 25 indicating lack of self-efficacy of the mother and those higher indicating more self-efficacy of the mother. The validity and reliability of this questionnaire was first confirmed by Reese in 1992 [33]. The validity and reliability of this questionnaire in Iran was confirmed by Jafarnejad et al. in 2014 by obtaining a Cronbach's alpha coefficient of 0.87, a content validity index of 0.79, and a content validity ratio of 0.62 [34].
Perceived Stress Scale (PSS)
Perceived Stress Scale was developed in 1983 by Cohen et al. to measure general perceived stress over the past month. Thoughts and feelings about stressful events, as well as controlling, overcoming, coping with stress. In the present study, the 14-item version was used which is answered based on a 5-point Likert scale (from Never: 0 to Most of the time: 4). Total Scores range from zero to 56, with higher scores indicating more perceived stress. The reliability of this questionnaire in the original version using Cronbach’s alpha coefficient method has been reported between 0.84 and 0.86, and its correlations with the constructs measured are also high (0.52 to 0.76) [35]. In Iran, the reliability of this questionnaire was calculated by Bastani et al. using the internal consistency method and obtaining a Cronbach’s alpha coefficient of 0.74 [36]. Dolatian et al. (2014) reported a content validity index of 95% and a content validity ratio of 90% for this questionnaire [37].
Data analysis
The collected data were analyzed using descriptive statistics (frequency, percentage, mean and standard deviation) and inferential statistics using SPSS version 24. P < 0.05 was considered statistically significant. Kolmogorov–Smirnov test was used to evaluate the normality of quantitative data. Fisher’s exact test, Chi-square test, and independent t-test were used to examine the demographic characteristics. Independent t-test and analysis of variance with repeated measures were used to compare the mean scores of social support as well as perceived stress, and maternal self-efficacy in groups at each time interval and over time, respectively.
Results
In this study, of the 373 primiparous women referring to health centers who were initially enrolled, 273 were excluded from the study due to not meeting inclusion criteria. No attrition was observed in both groups during the study period, and all participants (50 in the intervention group and 50 in the control group) were analyzed at two intervals (immediately and one month after the intervention) after the follow-up period (Fig. 1). The demographic characteristics of the participants are shown in Table 1. The mean age of women and their husbands were 29.3 ± 6.16 and 35.08 ± 5.58 in the intervention group and 28.14 ± 5.98 and 33.56 ± 5.13 in the control group, respectively. There was no significant difference between the two groups in terms of demographic characteristics.
Based on independent t-test, the mean scores of perceived social support (P = 0.11), maternal self-efficacy (p = 0.37) and perceived stress (p = 0.19) before intervention were not significantly different in the two groups. In the intervention group, the mean scores of perceived social support, self-efficacy and perceived stress of primiparous women immediately and one month after completing the intervention were significantly different from those in the control group (P < 0.001). Analysis of variance with repeated measures showed that the perceived social support (mean difference = 30.72; 95% confidence interval = 28.61 to 32.82; p < 0.001), maternal self-efficacy (mean difference = 55.29; 95% confidence interval = 41.85 to 68.73; p < 0.001) and perceived stress (mean difference = -16.7; 95% confidence interval = -18.71 to -14.70; p < 0.001) of primiparous women in the intervention group changed significantly over time, and the interaction analysis showed that there was a significant cross impact between group and time (P < 0.001) (Table 2). As shown in Figs. 2, 3 and 4, the mean scores of perceived social support and maternal self-efficacy in the intervention group increased over time while the mean scores of perceived stress decreased over time.

The mean scores of perceived social support in the intervention and control groups across the three measurement times

The mean scores of Maternal self-efficacy in the intervention and control groups across the three measurement times

The mean scores of Perceived postpartum stress in the intervention and control groups across the three measurement times
Discussion
The results of this study showed that the postnatal supportive education program for husbands enhanced the understanding of social support for their primiparous women in the fourth and eighth weeks after delivery. It can be argued that providing education and consultation services to husbands in order to increase their awareness about the characteristics and issues of women in the postpartum period is one of the tools for promoting husbands’ social support to their wives, which has a positive effect on the couple’s knowledge, attitude and practice with respect to postpartum health [31]. Various studies have introduced the husband as the most important source of support in stressful life situations of women [38, 39].
To the best of our knowledge, no study has yet been conducted on the effect of husband education or counseling on social support, maternal self-efficacy, and stress in postpartum women. However, previous studies have shown the overall impact of participation and counseling of pregnant women's husbands, primiparous women and couples in this respect. Mohammadpour et al. (2020), for instance, conducted a randomized clinical trial to determine the effect of husband counseling on social support perceived by their pregnant wives. Their intervention involved four 60-min sessions of group counseling (each group consisting of 7 to 10 people) once a week for four consecutive weeks. The results showed that the mean score of social support 4 weeks after the intervention in the intervention group increased significantly compared to the control group [23]. Another study in Singapore conducted by Shorey et al. (2017) examined the effectiveness of a postpartum psychiatric educational mobile application called "Home—but not Alone" in improving parenting outcomes. Parents in the intervention group received a training program in addition to routine care while the control group received only routine care. The results showed that parental self-efficacy and social support significantly improved four weeks after delivery in the intervention group compared to the control group [17]. The results of studies of Turan et al. and Sahip et al. showed that husbands’ education led to improvement their more appropriate supportive behaviors with women during pregnancy [25, 26]. The results of the present study are in line with those mentioned above, which indicates the positive effect of husband education or counseling on mothers’ social support. Therefore, it is necessary to increase the awareness of husbands about their positive role in the postpartum period and their participation in promoting the health of mother and baby. In fact, in the present study, online education through social networking provided a virtual community for husbands, and facilitated social support between members of this community through sharing personal information and experiences, and at the same time, and created the opportunity of making friends with other men in this community.
The results of the present study showed that the postnatal supportive education program for husbands of primiparous women promoted maternal self-efficacy in these women in the fourth and eighth weeks after delivery. It can be argued that educating men to promote support for their primiparous wives can play an effective role in reinforcing the mother’s abilities and her interpretation of the competence she has to play the role of a mother, thus increasing her self-efficacy [40]. The results of previous studies confirm our findings with respect to the positive effect of educational intervention on the promotion of maternal self-efficacy, and this was achieved in our study 4 and 8 weeks after delivery [34, 41]. In line with the present study, the results of a randomized clinical trial showed the significant effect of a postpartum psychological education program on increasing maternal self-efficacy and social support and reducing postpartum depression among primiparous women in their 6th and 12th weeks of postpartum. The final results of this trial indicated that the postpartum psychological education program is effective in improving maternal outcomes [13]. The main difference between this study and the present study was that in the former the training program involved a face-to-face meeting and presentation of a booklet for primiparous women, while in our study the training program included 4 online training sessions for husbands. In fact, the training sessions in our study were for husbands only. In these sessions, the need for spouse support in the postpartum period was taught for fathers and we assessed the effects of education on their primiparous women indirectly.
Salonen et al. (2010) investigated the effect of an online educational intervention on increasing maternal satisfaction and self-efficacy. Mothers in the intervention group had access to an educational website offering infant care training content from the 20th week of pregnancy whereas the control group received only the routine training. No statistically significant difference was observed between the two groups 6 to 8 weeks after delivery in terms of self-efficacy and parental satisfaction compared to before the intervention [42]. This finding is contrary to the results of the present study. This discrepancy can be attributed to the fact that participants in their study included a combination of primiparous and multiparous women with full-term or pre-term pregnancies as well as normal or abnormal birth weight. In addition, a number of women in both groups in their study had a depression score higher than 10, which was not the case in the present study.
In the present study, participants had access to information through education. This useful information helped the men to acquire the right knowledge independently and, by providing support to the mother, they managed to perform the challenging parenting tasks and increase the mother’s self-efficacy. The helpful feedback given to the husbands served as verbal encouragement, thus allaying their concerns and increasing their self-confidence and motivation to promote maternal self-efficacy.
The results of the present study showed that the postnatal supportive education program for husbands of primiparous women reduced the perceived stress in these women in the fourth and eighth weeks after delivery. This can be attributed to the fact that educating husbands on providing emotional, informational, and instrumental support to the mother reduces her physical and psychological stress. Therefore, among the available support sources, the support provided by sexual partners is very important [43]. This finding is consistent with the results of studies by Cohen et al. (2014) and Dafie et al. (2021) where providing counseling services to couples based on cognitive-behavioral methods during pregnancy has been found to exert a positive effect on reducing stress and depression. In this method, perinatal stress and depression is reduced and post-natal mental health is promoted by enhancing the couples’ understanding about pregnancy and its changes, minimizing negative behaviors and attitudes, increasing emotional support, and promoting empathetic communication during pregnancy. Given the relationship between mental health during pregnancy and postpartum mental health, the use of educational and counseling methods in care centers to promote maternal mental health is strongly recommended [44, 45].
Also, study of Alio et al. (2013) showed that the primary benefits of male partner involved during pregnancy were the reduction of maternal stress levels and the encouragement of positive maternal behaviors [46]. In another study, the results showed that 4 sessions of consultation with fathers had no effect on reducing stress in pregnant mothers [23], which is contrary to the results of the present study. It seems that the difference is attributable to the type of intervention, educational content, number and type of participants, follow-up period, or different assessment tools. Research has shown that educational information provided by health care providers during pregnancy is rarely adhered to by mothers themselves during the postpartum period [47], indicating the mothers’ need for support to cope with stress correctly, which explains the results of the present study.
One of the limitations of this study was that women in this study had no neuropsychiatric diseases. This may affect the generalizability of the results to women who are depressed. The second limitation was that data collection was based solely on participants’ own reports, and the researchers did not use other sources of data collection such as observation. The third limitation was that due to the nature of the intervention, the researchers were not blind to data collection after the intervention. Also, no data was collected from husbands. The last limitation was the cultural component. This prevents generalization to other realities. There is no homosexual culture in Iran, and families made up of a man and a woman and who are married. Other family models (single parent, mixed families, not married, formed by people of the same sex), which are not considered here and could be considered in other studies. These limitations notwithstanding, this study is worthwhile considering the following: Random allocation, concealment of allocation, random selection of women from health centers in 4 districts of the city, long-term follow-up, providing telephone numbers to answer participants’ questions, and providing educational content to the control group at the end of the study. Also, the intervention was designed around the planned delivery method. Therefore, we suggest that a similar study be done in women with a history of depression or suffering from that with more sophisticated statistical analysis.
Conclusion
This study demonstrated the effectiveness of a postnatal supportive education program for husbands (male partners) in improving perceived social support, maternal self-efficacy, and stress in primiparous women. Therefore, policymakers in postpartum care are advised to consider the participation of husbands in the postpartum care process and to devise plans to increase the awareness of husbands and their role in promoting maternal and infant health. Also, to confirm the results of this study, a randomized controlled trial with a larger sample size from the whole population is suggested.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- PND:
-
Postnatal Depression
- PSS:
-
Perceived Stress Scale
- PPES:
-
Postpartum Parental Expectations Survey
- PPSS:
-
Postpartum Partner Support Scale
- CVI:
-
Content Validity Index
- CVR:
-
Content Validity Ratio
References
Shorey S, Chan SWC, Chong YS, He HG. Perceptions of primiparas on a postnatal psychoeducation programme: the process evaluation. Midwifery. 2015;31(1):155–63. https://doi.org/10.1016/j.midw.2014.08.001.
Ohoka H, Koide T, Goto S, Murase S, Kanai A, Masuda T, et al. Effects of maternal depressive symptomatology during pregnancy and the postpartum period on infant–mother attachment. Psychiatry Clin Neurosci. 2014;68(8):631–9. https://doi.org/10.1111/pcn.12171.
MoghaddamTabrizi F, Nournezhad H. The effect of family support based counselling on postnatal perceived stress and mother-child bonding in nulliparous women to health centers in Urmia in 2016–2017. Nurs Midwifery J. 2018;16(2):109–21 (http://unmf.umsu.ac.ir/article-1-3439-en.html).
Teti DM, Gelfand DM. Behavioral competence among mothers of infants in the first year: The mediational role of maternal self-efficacy. Child Dev. 1991;62(5):918–29. https://doi.org/10.1111/j.1467-8624.1991.tb01580.x.
Mazaheri M, Bahramian SH. Prediction of Psychological Well-Being based on the Positive and Negative Affection and Coping Self – Efficacy. J Posit Psychol. 2016;1(4):1–14.
Law KH, Dimmock J, Guelfi KJ, Nguyen T, Gucciardi D, Jackson B. Stress, depressive symptoms, and maternal self-efficacy in first-time mothers: Modelling and predicting change across the first six months of motherhood. Appl Psychol: Health Well-Being. 2019;11(1):126–47. https://doi.org/10.1111/aphw.12147.
Serçekuş P, Mete S. Effects of antenatal education on maternal prenatal and postpartum adaptation. J Adv Nurs. 2010;66(5):999–1010. https://doi.org/10.1111/j.1365-2648.2009.05253.x.
Deave T, Johnson D, Ingram J. Transition to parenthood: the needs of parents in pregnancy and early parenthood. BMC Pregnancy Childbirth. 2008;8(1):1–11.
Barnard K. Parent-child interaction model. Nursing theorists and their work. 1994. 406–22.
Saeedi H, Ashoori J. The relationship between social capital, perceived social support and organizational citizenship behavior, and mental health, case study of police force employees in south eastern Tehran. MCS. 2016;3(2):90–9. https://doi.org/10.18869/acadpub.mcs.3.2.90.
Sarafino EP, Smith TW. Health psychology: Biopsychosocial interactions: John Wiley & Sons; 2014.
Mohammadpour M, Charandabi SM-A, Malekuti J, Mohammadi M, Mirghafourvand M. Perceived stress and its relationship with social support in pregnant women referring to health centers of Ardabil, Iran. CJMBS. 2019;6:505–10.
Shorey S, Chan SW, Chong YS, He HG. A randomized controlled trial of the effectiveness of a postnatal psychoeducation programme on self-efficacy, social support and postnatal depression among primiparas. J Adv Nurs. 2015;71(6):1260–73. https://doi.org/10.1111/jan.12590.
Ngai FW, Chan SWC. Learned resourcefulness, social support, and perinatal depression in Chinese mothers. Nurs Res. 2012;61(2):78–85. https://doi.org/10.1097/NNR.0b013e318240dd3f.
Pourkhaleghi N, Askarizadeh G, Fazilat-Pour M. Predicting post-partum depression of nulliparous women: Role of social support and delivery type. J Health Care. 2017;19(1):18–29.
Shorey S, Chan SW, Chong YS, He HG. Maternal parental self-efficacy in newborn care and social support needs in S ingapore: a correlational study. J Clin Nurs. 2014;23(15–16):2272–83. https://doi.org/10.1111/jocn.12507.
Shorey S, Lau YY, Dennis CL, Chan YS, Tam WW, Chan YH. A randomized-controlled trial to examine the effectiveness of the ‘Home-but not Alone’mobile-health application educational programme on parental outcomes. J Adv Nurs. 2017;73(9):2103–17. https://doi.org/10.1111/jan.13293.
Ngai FW, Chan SW, Ip WY. The effects of a childbirth psychoeducation program on learned resourcefulness, maternal role competence and perinatal depression: a quasi-experiment. Int J Nurs Stud. 2009;46(10):1298–306. https://doi.org/10.1016/j.ijnurstu.2009.03.007.
Taghani R, Ashrafizaveh A, Soodkhori MG, Azmoude E, Tatari M. Marital satisfaction and its associated factors at reproductive age women referred to health centers. J Educ Health Promot. 2019;8:133. https://doi.org/10.4103/jehp.jehp_172_18.
Fletcher R, Silberberg S, Galloway D. New fathers’ postbirth views of antenatal classes: Satisfaction, benefits, and knowledge of family services. J Perinat Educ. 2004;13:18–26.
Tokhi M, Comrie-Thomson L, Davis J, Portela A, Chersich M, Luchters S. Involving men to improve maternal and newborn health: a systematic review of the effectiveness of interventions. PloS ONE. 2018;13(1):e0191620. https://doi.org/10.1371/journal.pone.0191620.
Yogman M, Garfield CF, Bauer NS, Gambon TB, Lavin A, Lemmon KM, et al. Fathers’ roles in the care and development of their children: the role of pediatricians. Pediatrics. 2016;138(1):e20161128. https://doi.org/10.1542/peds.2016-1128.
Mohammadpour M, Mohammad-Alizadeh Charandabi S, Malakouti J, Nadar Mohammadi M, Mirghafourvand M. Effect of counselling with men on perceived stress and social support of their pregnant wives. J Reprod Infant Psychol. 2020:1–15 https://doi.org/10.1080/02646838.2020.1792428
Sharifipour F, Javadnoori M, Moghadam ZB, Najafian M, Cheraghian B, Abbaspoor Z. Interventions to improve social support among postpartum mothers: A systematic review. HPP. 2022;12(1):2.
Turan JM, Nalbant H, Bulut A, Sahip Y. Including expectant fathers in antenatal education programmes in Istanbul. Turkey Reprod Health Matters. 2001;9:114–25. https://doi.org/10.1016/S0968-8080(01)90098-9.
Sahip Y, Molzan TJ. Education for expectant fathers in workplaces in Turkey. J Biosoc Sci. 2007;39:843–60. https://doi.org/10.1017/S0021932007002088.
Danbjørg DB, Wagner L, Clemensen J. Designing, developing, and testing an app for parents being discharged early postnatally. J Nurse Pract. 2014;10(10):794–802. https://doi.org/10.1016/j.nurpra.2014.07.023.
Ministry of Health and Medical Education. Family and Population Health Office. Maternal Health Office. Country guide for midwifery and childbirth services. Tehran: Charsavi Honar; 2015.
Arcamone AA, editor The Effect of Prenatal Education on Adaptation to Motherhood After Vaginal Birth in Primiparous Women. 38th Biennial Convention-Clinical Sessions; 2005.
Aghakhani N, Nia HS, Ranjbar H, Rahbar N, Beheshti Z. Nurses’ attitude to patient education barriers in educational hospitals of Urmia University of Medical Sciences. Iran J Nurs Midwifery Res. 2012;17(1):12.
Khanzadeh Z, Mogaddam Tabrizi F. The Effect of Supportive Couple-Centered Counselling on Perception of Support for Spouse and Maternal Attachment in Parturients Referring to Health Centers of Urmia University of Medical Sciences in 2018–19. Avicenna J Nurs Midwifery Care. 2020;28(2):112–26. https://doi.org/10.30699/ajnmc.28.2.112.
Dennis C-L, Brown HK, Brennenstuhl S. The Postpartum Partner Support Scale: Development, psychometric assessment, and predictive validity in a Canadian prospective cohort. Midwifery. 2017;54:18–24. https://doi.org/10.1016/j.midw.2017.07.018.
Reece SM. The parent expectations survey: A measure of perceived self-efficacy. Clin Nurs Res. 1992;1(4):336–46. https://doi.org/10.1177/105477389200100404.
Jafarnejad F, Azmoudeh E, Mazloum SR, Reyhani T. The effect of self-efficacy training package on maternal self-confidence of primiparous women in infant care. IJOGI. 2014;17(104):18–2.
Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–96. https://doi.org/10.2307/2136404.
Bastani F, Rahmatnejad L, Jahdi F, Haghani H. Breastfeeding self efficacy and perceived stress in primiparous mothers. IJN. 2008;21(54):9–24.
Dolatian M, Alavi MH. Comparison of pregnancy self-care, perceived social support and perceived stress of women with gestational diabetes and healthy pregnant women. IJEM. 2014;16(3):156–64.
Soltanshahi Z, Azh N, Griffiths MD, Ranjkesh F. Effect of spouse’s participation in childbirth preparation classes in the promotion of social support among pregnant women: A field trial. Soc Health Behav. 2020;3:55–61.
Uluğ E, Öztürk S. The Effect of Partner Support on Self-Efficiency in Breastfeeding in the Early Postpartum Period. J Fam Ther. 2020;14(2):211–9.
Kuo SC, Chen YS, Lin KC, Lee TY, Hsu CH. Evaluating the effects of an Internet education programme on newborn care in Taiwan. J Clin Nurs. 2009;18(11):1592–601. https://doi.org/10.1111/j.1365-2702.2008.02732.x.
Azmoude E, Jaafarnejad F, Mazloum S. Effect of self-efficacy-based training on maternal sense of competency of primiparous women in the infants care. Evid Based Care J. 2014;4(3):7–14.
Salonen AH, Kaunonen M, Åstedt-Kurki P, Järvenpää A-L, Isoaho H, Tarkka M-T. Effectiveness of an internet-based intervention enhancing Finnish parents’ parenting satisfaction and parenting self-efficacy during the postpartum period. Midwifery. 2011;27(6):832–41. https://doi.org/10.1016/j.midw.2010.08.010.
Thompson K, Parahoo K, McCurry N, O’Doherty E, Doherty A. Women’s perceptions of support from partners, family members and close friends for smoking cessation during pregnancy—combining quantitative and qualitative findings. Health Educ Res. 2004;19(1):29–39. https://doi.org/10.1093/her/cyg013.
Cohen S, O’Leary KD, Foran HM, Kliem S. Mechanisms of change in brief couple therapy for depression. Behav Ther. 2014;45(3):402–17. https://doi.org/10.1016/j.beth.2014.01.003.
Dafei M, Shojaaddini AT. Effectiveness of group-counseling in the presence of spouse and client-oriented, using cognitive-behavioral approach during pregnancy on promoting postpartum mental health: a randomized clinical trial. Nurs Midwifery J. 2021;18(12):920–32.
Alio AP, Lewis CA, Scarborough K, Harris K, Fiscella K. A community perspective on the role of fathers during pregnancy: A qualitative study. BMC Pregnancy and Childbirth. 2013;13(1):60. https://doi.org/10.1186/1471-2393-13-60.
Razurel C, Bruchon-Schweitzer M, Dupanloup A, Irion O, Epiney M. Stressful events, social support and coping strategies of primiparous women during the postpartum period: a qualitative study. Midwifery. 2011;27(2):237–42. https://doi.org/10.1016/j.midw.2009.06.005.
Acknowledgements
The authors would like to thank all the participants in this study.
Funding
The study is part of the results of the PhD dissertation of the first author in midwifery, which was financially supported by Ahvaz Jundishapur University of Medical Sciences (AJUMS) in Iran.
Author information
Authors and Affiliations
Contributions
All authors contributed to this study; F-SH, and ZA designed the study. F-SH, MJ, ZB and MN provided the training. F-SH and ZA collected the data, B-CH analyzed the data analysis, F-SH drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for this study was obtained from the research ethics committee of Ahvaz Jundishapur University of Medical Sciences with the ethics code of IR.AJUMS.REC.1399.401. In addition, this trial registered in Iranian registry of clinical trials; https://fa.irct.ir/user/trial/56451 (IRCT20160427027633N8), registered on 15/06/2021. Written informed consent was obtained from each woman. The study was conducted in accordance with the Declaration of Helsinki and subsequent.
Consent for publication
Not applicable.
Competing interests
The authors have no conflicts of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table 1.
Intervention group educational content sessions.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Abbaspoor, Z., Sharifipour, F., Javadnoori, M. et al. Evaluation of the effectiveness of a postnatal support education program for husbands in promotion of their primiparous wives’ perceived social support: a randomized controlled trial. BMC Women's Health 23, 139 (2023). https://doi.org/10.1186/s12905-023-02270-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-023-02270-x