
Abstract
Background
Women of childbearing age are vulnerable to weight gain. This scoping review examines the extent and range of research undertaken to evaluate behavioral interventions to support women of childbearing age to prevent and treat overweight and obesity.
Methods
Eight electronic databases were searched for randomized controlled trials (RCT) or systematic reviews of RCTs until 31st January 2018. Eligible studies included women of childbearing age (aged 15–44 years), evaluated interventions promoting behavior change related to diet or physical activity to achieve weight gain prevention, weight loss or maintenance and reported weight-related outcomes.
Results
Ninety studies met the inclusion criteria (87 RCTs, 3 systematic reviews). Included studies were published from 1998 to 2018. The studies primarily focused on preventing excessive gestational weight gain (n = 46 RCTs, n = 2 systematic reviews), preventing postpartum weight retention (n = 18 RCTs) or a combination of the two (n = 14 RCTs, n = 1 systematic review). The RCTs predominantly evaluated interventions that aimed to change both diet and physical activity behaviors (n = 84) and were delivered in-person (n = 85).
Conclusions
This scoping review identified an increasing volume of research over time undertaken to support women of childbearing age to prevent and treat overweight and obesity. It highlights, however, that little research is being undertaken to support the young adult female population unrelated to pregnancy or preconception.
Similar content being viewed by others

Background
Prevalence of women affected by obesity is increasing globally, with prevalence rates increasing from 6.4% in 1975 to 14.9% in 2014 [1]. Women of childbearing age (15 to 44 years) are particularly vulnerable to weight gain, with many large cohort studies demonstrating this life stage is the time of greatest weight gain [2,3,4,5]. For example, the Australian Longitudinal Study of Women’s Health has found women in their younger cohort (aged 18–23 years at survey 1) experience an average weight gain of 6.3 kg over 10 years [3]. Notably, in women of childbearing age, pregnancy has been investigated as a potential trigger for excessive weight gain and the development of overweight and obesity. The results however are inconsistent, with some studies in women of childbearing age demonstrating an association between parity and weight gain and/or the development of overweight and obesity, while others have shown no association [6, 7].
Weight gained during the childbearing years is strongly associated with adverse health outcomes later in life. For example, the Nurses’ Health Study (n = 92,837) identified that for every additional 5 kg of weight gained from 21 years of age there were 142.6 additional cases of Type 2 diabetes (per 100,000 person-years from age 55 onwards), 458.8 for hypertension, 36.9 for cardiovascular disease, 36.9 for cancer, and 76.7 for overall mortality [8]. Furthermore, obesity during the childbearing years has been associated with adverse pregnancy outcomes for the mother (e.g. gestational diabetes, pre-eclampsia, gestational hypertension, antenatal anxiety and postpartum depression), as well as for the babies (e.g. pre-term birth, and large for gestational age babies) [9, 10].
Behavioral interventions to support women to prevent weight gain during the childbearing years, or treat overweight or obesity, have the potential to have an impact on the health and well-being of women, as well as their offspring. Behavioral interventions are those designed to influence individuals’ actions, more specifically for weight management, interventions include those which influence physical activity and sedentary and/or dietary behaviors. A large number of systematic reviews have been undertaken to determine the most effective interventions to support women during this life stage to prevent and treat overweight and obesity [11,12,13,14,15,16,17,18,19,20,21,22,23]. However, reviews published to date have typically been limited to one type of intervention (e.g. treatment or prevention of obesity, preventing excessive gestational weight gain (GWG)), population group (e.g. pregnant/postpartum women) or mode of delivery (e.g. web-based), or combined a variety of intervention approaches (e.g. behavioral, surgical, pharmacological) in the one review. Therefore, previous systematic reviews are unable to determine the most appropriate time for intervention during this life stage (e.g. pre-conception, postpartum), the most efficacious behavioral intervention approach (e.g. treatment, prevention) nor the optimal mode of delivery for intervention.
To our knowledge, no single review has identified all behavioral interventions aiming to support women of childbearing age to prevent weight gain, or achieve weight loss or weight loss maintenance. Therefore, the aim of this scoping review is to examine the extent and range of research undertaken to evaluate behavioral interventions that support women of childbearing age to prevent or treat overweight and obesity. The scoping review methodology allows mapping of the range of research that has been undertaken over time. The scoping review is the first step in determining the most efficacious intervention approach. It will help identify gaps in research undertaken to date, and determine whether a full systematic review can be undertaken.
Methods
A scoping review was undertaken using a predefined protocol following the methodological framework of Arksey and O’Malley, [24] including identifying the research question, searching for relevant studies, selecting studies, charting the data and collating, summarizing, and reporting the results. The conduct and reporting of the scoping review is consistent with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist. Preliminary findings of the scoping review were previously presented [25].
Identifying the research question
The research question was operationalized using the Population-Intervention-Comparison-Outcome-Study design (PICOS) format. Inclusion criteria for the scoping review were therefore as follows:
Participants
Women of childbearing age (i.e. aged 15 to 44 years as per US Centre for Disease Control Definition).
Interventions
Interventions promoting behavior change (e.g. dietary behavior, physical activity and/or sedentary behavior) to prevent weight gain or overweight and obesity, or achieve weight loss or weight loss maintenance were included. Non-behavioral interventions, including very low energy diets (including meal replacements), weight loss medications and surgery alone or in combination with behavioral interventions will be excluded.
Comparators
No intervention control group, wait-list control group, standard/usual care or another active behavioral intervention.
Outcomes
To be included in the review studies must have measured and reported weight-related outcomes (e.g. weight, BMI, percentage body fat, waist circumference).
Study design
Systematic reviews of randomized control trials (RCTs) and RCTs as the two highest levels of evidence for evaluating interventions [26].
Selection of studies relevant to the research question
Search strategy
The search strategy, including database selection and search teams, was developed in consultation with an expert medical librarian. The search aimed to find peer reviewed journal articles published in English. All sources were searched from the date of inception up until the 31st January 2018 (Additional file 1: Table S1). The databases searched were MEDLINE (Ovid), MEDLINE in process (Ovid), EMBASE (Ovid), PsycINFO (Ovid), Scopus, CINAHL (EbscoHost) and Cochrane Library (Wiley). The reference lists of all included articles and reports were also searched for additional studies.
Screening
Screening was managed using Covidence (www.covidence.org). Title, abstract and keywords of all identified papers were each assessed by two independent reviewers (Reviewer 1: MMH; Reviewer 2: MH, JG, SL, LM, LV). Full text screening was conducted by two independent reviewers, and reasons for exclusions recorded (MMH, MH). A third reviewer was consulted for all conflicts for both abstract and full text screening (MR).
Charting of information and data within the included studies
Data were extracted by one reviewer (MMH) and checked by a second reviewer (LV, LM, SL, JH, MR). Any differences between the first and second extractor were resolved by a third reviewer (HB). Data extracted included: study characteristics (i.e. year study conducted/published, country of origin, study design, number of study arms and comparators, intervention duration); participants (i.e. study inclusion criteria relating to age, BMI, ethnicity, socio-economic status, parity, clinical conditions or pregnancy); interventions (i.e. goal [weight loss, weight loss maintenance, weight gain prevention, excessive gestational weight gain prevention], behavior change promoted [dietary behavior, physical activity and/or sedentary behavior], setting [e.g. clinic, community], mode of delivery [i.e. individual, group or combination] and medium of delivery [e.g. in-person, website] and profession of intervention deliverer) and outcomes (i.e. what weight-related outcomes were measured and when, and other outcomes measured).
Collating, summarizing and reporting results of the review
As is convention in scoping reviews, a numerical analysis was undertaken to elucidate the number of the studies, as well as changes overtime (based on publication date). In addition, results are presented by intervention goal, with studies group as general weight loss, post-partum weight loss/preventing weight retention, general weight gain prevention, excessive GWG, and combine excessive GWG prevention and post-partum weight loss. ‘General’ weight loss and weigh gain prevention includes those interventions unrelated to pregnancy status.
Results
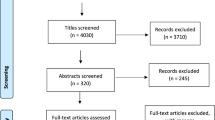
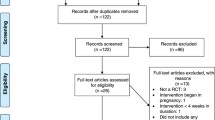
Of the 8543 articles identified, 307 full text articles were assessed for eligibility and 115 articles met the inclusion criteria (Fig. 1). The articles described 87 RCTs and three systematic reviews.

Flow diagram of included studies
Randomized control trials
Table 1 describes the study characteristics of the included RCTs overall, and by intervention goal. Individual study characteristics are described in Additional file 1: Table S2. Of the 87 included RCTs, 52.9% (n = 46) focused on preventing excessive GWG, [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71] 20.7% (n = 18) on weight loss or preventing weight retention in the postpartum period, [72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89] and 16.1% (n = 14) focused on both preventing excessive GWG and preventing weight retention in the postpartum period [90,91,92,93,94,95,96,97,98,99,100,101,102,103]. Few studies supported general reproductive-aged women (i.e. not specifically related to current or recent pregnancy) in weight loss (4.6%, n = 4) [104,105,106,107] or weight gain prevention (5.7%, n = 5) [108,109,110,111,112]. Most of the included studies were conducted in the United States (46.0%, n = 40), followed by Australia (16.1%, n = 14).
Figure 2 demonstrates the year of publication of the included RCTs, by weight focus. Studies were published from 1998 up until 2018, but with no studies published from 1998 to 2000, and only zero to two studies published per year from 2000 to 2008. From 2009 to 2017 the number of studies conducted per year ranged from three (2010) to 14 (2014). The intervention goal of included studies varied over time. While the number of studies focusing solely on postpartum weight loss/preventing weight retention has remained consistent focus over time, the number of weight gain prevention and weight loss studies unrelated to pregnancy decreased overtime, with more of a focus on prevention of excessive GWG, and the prevention of excessive GWG combined with postpartum weight loss/preventing postpartum weight retention.

Number of included RCTs per year by weight focus
Across the included RCTs there were 26,750 participants (Mean: 307.5). Many of the RCTs (59.8%, n = 52) recruited women of childbearing age as per our definition for inclusion (i.e. 18 to 44 years) or did not specifically define the age range for participant inclusion but implied they were ‘of childbearing’ age due to other inclusion criteria (i.e. pregnancy) (19.5%, n = 17). A significant number of RCTs (41.4%, n = 36) recruited only women who were affected by overweight or obesity, while many also did not report a BMI inclusion criteria (24.1%, n = 21).
Only five studies required women to be of a specific parity, with all five recruiting women during their first pregnancy. Twelve studies recruited participants from specific ethnicities, including African American (6.9%, n = 6) and Latina/Hispanic (5.7%, n = 5) women, and one study (1.1%) recruited only ‘white’ women. Ten RCTs (11.5%) had participant recruitment criteria related to the socio-economic status of the participant, with all specifically recruiting women of lower socio-economic status (e.g. lower income). Five studies recruited women with specific clinical conditions, including three studies (3.4%) that recruited women with gestational diabetes, one (1.1%) recruited women who were infertile, and one (1.1%) recruited women who were breastfeeding.
Table 2 describes the outcomes measured across the included RCTs. All studies measured weight related outcomes, with 78.2% (n = 62) having a weight-related primary outcome [27, 29,30,31,32,33,34, 36, 38, 40,41,42,43,44, 46, 47, 50, 51, 54, 56,57,58,59, 61,62,63,64,65,66, 68, 69, 71,72,73,74,75,76,77,78,79,80, 82,83,84,85,86,87, 90,91,92,93,94,95,96,97,98,99,100,101,102,103, 105, 106, 108,109,110,111]. Over half of the included RCTs (62.1%, n = 54) measured dietary and physical activity-related outcomes, with eight RCTs (9.2%) having a diet-related [45, 49, 51, 67, 71, 73, 75, 80] and five (5.7%) a physical activity related primary outcome [45, 49, 51, 73, 80]. At a minimum, all studies measured outcomes twice (i.e. baseline and follow-up), but the mean number of data collection points were 3.7 ± 2.0 (Range 2–14). There was a notable greater number of data collection points among studies focusing on GWG and preventing weight retention in the postpartum period (mean 5.1 ± 2.8).
Across the 87 included RCTs, there were 105 active intervention arms. Table 3 describes the characteristics of the 105 interventions overall and by weight focus. The majority (80.0%, n = 84) of the interventions focused on promoting both changes to dietary behavior and physical activity to achieve changes to weight-related outcomes. The interventions were most commonly delivered by those with expertise in nutrition, such as dietitians or nutritionists (42.9%, n = 45), or clinicians involved in the women’s care, such as midwives and/or general practitioners (GPs) (29.5%, n = 31). The setting for the interventions were commonly within the hospital or clinic (30.5%, n = 32), the participant’s home (28.6%, n = 30), or was not reported (27.6%, n = 29). Two-thirds (66.7%, n = 70) of interventions were delivered individually, 14 (13.3%) were group-based, and 23 (21.9%) used a combination of individual and group-based delivery.
Approximately half (49.5%, n = 52) of the interventions were delivered using one medium, and approximately one third (35.2%, n = 37) using two media. One study used five media to deliver the intervention. Most interventions (81.0%, n = 85) included components delivered in-person. A variety of other delivery mediums however were used across studies, including telephone (29.5%, n = 31), paper-based (27.6%, n = 29) (e.g. brochures), text message (10.5%, n = 11) and websites (9.5%, n = 10). Figure 3 shows the number of studies using different delivery modes by year of publication, demonstrating that the number of different delivery mediums utilized had increased over time.

Medium of intervention delivery across included RCTs per year
Systematic reviews
Three systematic reviews of RCTs were included in the scoping review, [15, 18, 113] which are described in detail in Additional file 1: Table S3. They included a total of 12 RCTs published from 1998 to 2011. Two of the reviews simply included studies with women of childbearing age, [18, 113] while the third included women of childbearing age ≥ 18 years of age [15]. Only one of the reviews specified that it only included participants affected by overweight or obesity [18]. None of the reviews had inclusion criteria related to participant’s ethnicity, clinical conditions or socio-economic status.
In terms of the reviews’ inclusion criteria for interventions, all reviews included studies with interventions that focused on modifying dietary intake, and two on modifying physical activity levels [15, 113]. Two of the reviews focused on prevention of excessive GWG, [15, 18] and one on prevention of excessive GWG and preventing weight retention in the postpartum period [113]. The reviews had no other specific inclusion criteria related to intervention types (e.g. mode of delivery, setting etc).
All three reviews required weight be reported as an outcome in the included studies, with one requiring it to be the primary outcome of the study [15]. There was no requirement in the three systematic reviews for diet or physical activity outcomes to be measured for the studies to be included in the review.
Discussion
This is the first scoping review, to our knowledge, to comprehensively examine the extent and range of research undertaken to evaluate behavioral interventions that support women of childbearing age to prevent and treat overweight and obesity. The review identified 87 RCTs and three systematic reviews published in the last two decades. All of the systematic reviews addressed gestational weight gain, [15, 18, 113] and one also focused on postpartum weight retention [113]. There has been an increasing volume of research on supporting this age group of women through weight-related behavioral interventions over time, particularly in the last decade. The majority of studies were conducted in the United States and Australia although there was representation of studies from middle income (although not lower income) countries, supporting evidence from global data on the rising prevalence of women affected by overweight and obesity, that supporting women of childbearing age in weight management is an international issue [114].
Almost 90% of the RCTs aimed to support women to gain an appropriate amount of weight during pregnancy, and/or support weight loss or prevent weight retention following pregnancy. The surge in studies addressing excess gestational weight gain aligns with the 2009 publication of the revised United States Institute of Medicine (IOM) Weight Gain during Pregnancy: Re-examining the Guidelines [115]. National pregnancy guidelines of many countries, including Canada [116] and Australia, [117] follow the pregnancy weight gain recommended ranges established by the IOM (i.e. total weight gain during pregnancy of 12.5–18.0 kg for pre-pregnancy BMI < 18.5 kg/m2 [Underweight], 11.5–16.0 kg for pre-pregancy BMI of 18.5–24.9 kg/m2 [Normal weight], 7.0–11.5 kg for pre-pregnancy BMI of 25.0–29. 9 kg/m2 [Overweight], and 5.0–9.0 kg for pre-pregnancy BMI ≥30.0 kg/m2 [Obese]). There are many strengths to the approach of engaging women in weight management interventions during or following pregnancy. Pregnancy has been proposed as a time when effective behavioral interventions can impact the health of two generations, [118] potentially increasing the return for investment. There may be a heightened level of interest and motivation by women to address weight, healthy eating and physical activity behaviors to improve pregnancy and health outcomes for themselves and their child [118, 119]. It may also be easier to reach women through existing routine antenatal and postnatal health care services when they come in to regular contact with a range of health care providers including doctors, midwives, nurses, dietitians, pharmacists, and reproductive health specialists [120].
However, there are limitations to heavily relying on pregnancy and postpartum interventions. Pregnant women are typically recruited to participate in gestational weight gain behavioral interventions midway through their second trimester [121]. This limits the potential impact of the intervention to support weight management since women who conceive with an obese, overweight or healthy weight BMI on average surpass their recommended weight gain by 18, 20 and 30 weeks of pregnancy, respectively [122]. First trimester weight gain in excess of 0.5–2 kg is also predictive of excess gestational weight gain during pregnancy [123]. Behavioral interventions that engage and support women to gain an appropriate amount of weight from earlier in pregnancy are needed [124]. However, this brings further clinical practice implementation challenges when up to 30–40% of woman do not begin receiving antenatal care until their second trimester [125, 126]. Given that pregnancy behavioral interventions have resulted in only modest reductions in gestational weight gain (of about 0.7 kg), and few have improved maternal and child health outcomes, there are compelling calls for future intervention research to also focus on the preconception period [127].
There is growing evidence on the role of obesity in preconception as a major determinant of offspring health in childhood and later adult life through the developmental origins of health and disease hypothesis [128]. In pregnant women, a higher pre-pregnancy BMI has been consistently identified as a strong predictor of pregnancy complications [129] and adverse offspring non-communicable health trajectories [130,131,132]. For example, when compared to a healthy pre-pregnancy BMI (18.5–24.9 kg/m2) a pre-pregnancy BMI of ≥40 kg/m2 has been shown to be associated with increased risk of gestational diabetes (Odds Ratio: 11.01 95% confidence interval 10.25–11.82), preeclampsia (OR: 4.44, 95%CI:4.17–4.72) and pre-term birth (OR: 2.91 95% CI: 2.21–3.81) [129]. The scoping review identified only one behavioral intervention directly supporting women in the preconception period who were planning a pregnancy. While the opportunity to support women at the individual level who are actively planning a pregnancy is important, it is also limited by low preconception care engagement (60–80% of women don’t receive preconception care [133,134,135]) and unplanned pregnancies, with global estimates that 44% of all pregnancies are unintended [136].
By only addressing weight management associated with a pregnancy event, an opportunity is missed to support weight management in the young female population, regardless of their intention or ability to have children. Only nine intervention studies that were unrelated to pregnancy were identified through the scoping review demonstrating a substantial research gap. Women tend to gain 0.5–1 kg each year from early adulthood until middle-age, [137, 138] with all young women, not only those who bear children, at risk of unhealthy weight gain [7]. An 18 year follow-up of 92,837 women from early to mid-adulthood in the Nurses’ Health Study found that women who gained between 2.5–10 kg had an increased incidence of type II diabetes, cardiovascular disease, obesity-related cancer, and mortality [8]. Effective behavioral interventions to support the entire young adult female population to improve health behaviors and weight management will improve chronic disease health trajectories more broadly, with added reproductive and intergenerational health benefits for women whose future pregnancies are both planned and unplanned.
Few weight management behavioral studies, with weight as the primary focus, have been conducted with women with clinical conditions. Engaging young women with existing or previous clinical conditions, such as type II diabetes, polycystic ovary syndrome, pre-eclampsia, and women who are experiencing obesity-related infertility, may help to reach and support young women at higher risk of obesity. More than half of the studies in this scoping review only recruited women who were affected by overweight and/or obesity. Weight gain prevention research to support young women to maintain their weight is needed if the rising obesity epidemic is to be halted. More research is also needed with populations under-represented in this review, such as women from lower socioeconomic groups and culturally diverse populations who may experience other barriers to weight management and have different patterns of health service engagement. Researchers should draw on existing behavioral modification research with lower socioeconomic groups and culturally diverse population groups to inform intervention design. Developing a better understanding of effective socially and culturally appropriate behavioral support, and clinician barriers to providing best practice care (e.g. clinician BMI and personal weight satisfaction may influence their confidence in providing best practice care [139]), could inform the delivery of population and primary health care initiatives for weight management.
The interventions included a variety of delivery modes and mediums, with individual and in-person delivery most commonly used. While the number of different delivery mediums used has increased over-time, no consistent or proven delivery medium has emerged [140]. Half of the interventions used more than one type of medium, such as in-person, telephone and text messages. Interventions delivered in the postpartum period tended to use more than one medium, and a greater variety of mediums. The use of multiple communication avenues may highlight efforts to overcome the difficulty of reaching new mothers who face complex barriers to participation, including a lack of time and need for childcare [141, 142]. Identifying whether one or more of the delivery modes and mediums are more effective in helping young women to manage their weight could help to inform the delivery of future interventions. Assessment of the intervention feasibility and acceptability by those delivering, and women receiving, weight management care should also be undertaken. Interventions were commonly provided by dietitians or nutritionists, or health care providers such as midwives and GPs. However, half of the studies did not deliver care through a dietetic or exercise professional, despite the professions’ expertise in nutrition [143, 144] and physical activity [145] for weight management. Systematic review evidence has shown that weight management interventions delivered by health care providers, [146] including dietitians, [147] are more effective than those delivered by non-health care providers.
This review has several strengths. It is the first scoping review to comprehensively examine the extent and range of research undertaken to evaluate behavioral interventions that support women of childbearing age to prevent and treat overweight and obesity. The review employed a comprehensive search strategy across numerous databases, and summarized the evidence from systematic reviews and RCTs, the two highest levels of evidence [26]. However, by limiting to systematic reviews and RCTs, evaluations of relevant interventions using other experimental study designs (e.g. pre-post studies, non-randomized control trials) were excluded from the review. In addition, the review only considered the extent and range of studies, and did not explore the efficacy of the interventions. Another main limitation of the scoping review was the challenge of combining data of studies that spanned different life periods (e.g. preconception, pregnancy, postpartum, non-pregnancy related) to accurately describe intervention duration and the timing of measurement outcomes, as they were variable within studies (e.g. due to timing of intervention delivery approximately based on weeks’ gestation in pregnancy) and across studies (e.g. due to differences in health service delivery, and the timing of when women are seen during and after pregnancy). Further, while 92 and 85% of studies reported interventions that targeted diet and/or physical activity behaviour change, respectively, only 62% of studies measured diet and 62% measured physical activity as outcomes. There is a need for studies to include valid and reliable diet and physical activity outcomes, particularly to investigate changes in diet and physical activity as a mediator of weight change. Finally, the scoping review included studies published up until 31st January 2018, therefore it is possible that additional studies meeting the inclusion criteria have been published since that time.
Conclusions
There is a substantial body of research from the two highest levels of evidence on behavioral interventions that support women of childbearing age to prevent and treat overweight and obesity, particularly from research published within the last decade. The majority has focused on weight management during or after a pregnancy event, demonstrating a research gap to support weight management in the young adult female population in preconception and unrelated to pregnancy to improve their own chronic disease health trajectories, with reproductive and intergenerational health benefits for future planned and unplanned pregnancies. Future research to examine delivery modes and mediums, optimal intervention duration and intensity, involvement of health care providers, and involvement of under-represented populations should be considered, both to understand effective behavioral interventions, and to ensure that interventions are scalable and can be implemented within policy and practice, such as through population and primary health care.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its supplementary information files]. The databases utilized in the search strategy were accessed via institutional licenses of the University of Newcastle, and therefore public access to the databases is closed.
Abbreviations
- BMI:
-
Body mass index
- GWG:
-
Gestational weight gain
- IOM:
-
Institute of Medicine
- RCT:
-
Randomized controlled trial
References
NCD Risk Factor Collaboration. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet. 2016;387(10026):1377–96.
Dutton GR, Kim Y, Jacobs DR Jr, Li X, Loria CM, Reis JP, Carnethon M, Durant NH, Gordon-Larsen P, Shikany JM, et al. 25-year weight gain in a racially balanced sample of U.S. adults: the CARDIA study. Obesity. 2016;24(9):1962–8.
Adamson L, Brown W, Byles J, Chojenta C, Dobson A, Fitzgerald D, Hockey R, Loxton D, Powers J, Spallek M, et al. Women's weight: findings from the Australian longitudinal study on Women’s health. Canberra: Australian Government Department of Health and Ageing; 2007.
Norman JE, Bild D, Lewis CE, Liu K, West DS. The impact of weight change on cardiovascular disease risk factors in young black and white adults: the CARDIA study. Int J Obes Relat Metab Disord. 2003;27(3):369–76.
Gordon-Larsen P, The NS, Adair LS. Longitudinal trends in obesity in the United States from adolescence to the third decade of life. Obesity. 2010;18(9):1801–4.
Robinson WR, Cheng MM, Hoggatt KJ, Sturmer T, Siega-Riz AM. Childbearing is not associated with young women's long-term obesity risk. Obesity. 2014;22(4):1126–32.
Davis D, Brown WJ, Foureur M, Nohr EA, Xu F. Long-term weight gain and risk of overweight in parous and nulliparous women. Obesity. 2018;26(6):1072–7.
Zheng Y, Manson JE, Yuan C, Liang MH, Grodstein F, Stampfer MJ, Willett WC, Hu FB. Associations of weight gain from early to middle adulthood with major health outcomes later in life. JAMA. 2017;318(3):255–69.
Athukorala C, Rumbold AR, Willson KJ, Crowther CA. The risk of adverse pregnancy outcomes in women who are overweight or obese. BMC Pregnancy Childbirth. 2010;10:56.
Oteng-Ntim E, Kopeika J, Seed P, Wandiembe S, Doyle P. Impact of obesity on pregnancy outcome in different ethnic groups: calculating population attributable fractions. PLoS One. 2013;8(1):e53749.
Hutchesson MJ, Hulst J, Collins CE. Weight management interventions targeting young women: a systematic review. J Acad Nutr Diet. 2013;113(6):795–802.
Farpour-Lambert NJ, Ells LJ, Martinez de Tejada B, Scott C. Obesity and Weight Gain in Pregnancy and Postpartum: an Evidence Review of Lifestyle Interventions to Inform Maternal and Child Health Policies. Front Endocrinol. 2018;9:546.
Berger AA, Peragallo-Urrutia R, Nicholson WK. Systematic review of the effect of individual and combined nutrition and exercise interventions on weight, adiposity and metabolic outcomes after delivery: evidence for developing behavioral guidelines for post-partum weight control. BMC Pregnancy Childbirth. 2014;14:319.
Dalrymple KV, Flynn AC, Relph SA, O'Keeffe M, Poston L. Lifestyle Interventions in Overweight and Obese Pregnant or Postpartum Women for Postpartum Weight Management: A Systematic Review of the Literature. Nutrients. 2018;10:11.
Brown MJ, Sinclair M, Liddle D, Hill AJ, Madden E, Stockdale J, et al. PLoS ONE. 2012;7(7):e39503.
Thangaratinam S, Rogozinska E, Jolly K, Glinkowski S, Duda W, Borowiack E, Roseboom T, Tomlinson J, Walczak J, Kunz R, et al. Interventions to reduce or prevent obesity in pregnant women: a systematic review. Health Technol Assess. 2012;16(31):iii–v 1-191.
Kuhlmann AK, Dietz PM, Galavotti C, England LJ. Weight-management interventions for pregnant or postpartum women (structured abstract). Am J Prev Med. 2008;34:523–8.
Quinlivan JA, Julania S, Lam L. Antenatal dietary interventions in obese pregnant women to restrict gestational weight gain to Institute of Medicine recommendations: a meta-analysis. Obstet Gynecol. 2011;118(6):1395–401.
Dodd JM, Grivell RM, Crowther CA, Robinson JS. Antenatal interventions for overweight or obese pregnant women: a systematic review of randomised trials. BJOG. 2010;117(11):1316–26.
Flynn AC, Dalrymple K, Barr S, Poston L, Goff LM, Rogozinska E, van Poppel MN, Rayanagoudar G, Yeo S, Barakat Carballo R, et al. Dietary interventions in overweight and obese pregnant women: a systematic review of the content, delivery, and outcomes of randomized controlled trials. Nutr Rev. 2016;74(5):312–28.
Tanentsapf I, Heitmann BL, Adegboye AR. Systematic review of clinical trials on dietary interventions to prevent excessive weight gain during pregnancy among normal weight, overweight and obese women. BMC Pregnancy Childbirth. 2011;11:81.
O'Brien CM, Grivell RM, Dodd JM. Systematic review of antenatal dietary and lifestyle interventions in women with a normal body mass index. Acta Obstet Gynecol Scand. 2016;95(3):259–69.
Spencer L, Rollo M, Hauck Y, MacDonald-Wicks L, Wood L, Hutchesson M, Giglia R, Smith R, Collins C. The effect of weight management interventions that include a diet component on weight-related outcomes in pregnant and postpartum women: a systematic review protocol. JBI Database System Rev Implement Rep. 2015;13(1):88–98.
Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Hutchesson M, de Jonge Mulock Houwer M, Rollo M, Hollis J, Lim S, Vincze L, Moran L. Behavioural interventions to treat and prevent overweight and obesity among women of childbearing age: A scoping review, vol. 2018. Melbourne: Australian and New Zealand Obesity Society-Breakthrough Discoveries Joint Annual Scientific Meeting 2018; 2018.
Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg. 2011;128(1):305.
Abdel-Aziz SB, Hegazy IS, Mohamed DA, MMA AEK, Hagag SS. Effect of dietary counseling on preventing excessive weight gain during pregnancy. Public Health. 2018;154:172–81.
Adamo KB, Ferraro ZM, Goldfield G, Keely E, Stacey D, Hadjiyannakis S, Jean-Philippe S, Walker M, Barrowman NJ. The maternal obesity management (MOM) trial protocol: a lifestyle intervention during pregnancy to minimize downstream obesity. Contemp Clin Trials. 2013;35(1):87–96.
Althuizen E, Poppel MNM, Seidell JC, Wijden C, Mechelen W. Design of the New Life(style) study: a randomised controlled trial to optimise maternal weight development during pregnancy. In. BMC Public Health. 2006;6:168.
Asbee SM, Jenkins TR, Butler JR, White J, Elliot M, Rutledge A. Preventing excessive weight gain during pregnancy through dietary and lifestyle counseling: a randomized controlled trial. Obstet Gynecol. 2009;113(2, Part 1):305–12.
Asci O, Rathfisch G. Effect of lifestyle interventions of pregnant women on their dietary habits, lifestyle behaviors, and weight gain: a randomized controlled trial. J Health Popul Nutr. 2016;35:7.
Bogaerts A, Devlieger R, Nuyts E, Witters I, Gyselaers W, Van den Bergh B. Effects of lifestyle intervention in obese pregnant women on gestational weight gain and mental health: a randomized controlled trial. Int J Gynaecol Obstet. 2013;37(6):814.
Brownfoot FC, Davey MA, Kornman L. Routine weighing to reduce excessive antenatal weight gain: a randomised controlled trial. BJOG. 2016;123(2):254–61.
Clements V, Leung K, Khanal S, Raymond J, Maxwell M, Rissel C. Pragmatic cluster randomised trial of a free telephone-based health coaching program to support women in managing weight gain during pregnancy: the get healthy in pregnancy trial. BMC Health Serv Res. 2016;16:454.
Daley AJ, Jolly K, Jebb SA, Lewis AL, Clifford S, Roalfe AK, Kenyon S, Aveyard P. Feasibility and acceptability of regular weighing, setting weight gain limits and providing feedback by community midwives to prevent excess weight gain during pregnancy: Randomised controlled trial and qualitative study. BMC Obesity. 2015;2(1):35.
Di Carlo C, Iannotti G, Sparice S, Chiacchio MP, Greco E, Tommaselli GA, Nappi C. The role of a personalized dietary intervention in managing gestational weight gain: a prospective, controlled study in a low-risk antenatal population. Arch Gynecol Obstet. 2014;289(4):765–70.
Dodd JM, Cramp C, Sui Z, Yelland LN, Deussen AR, Grivell RM, Moran LJ, Crowther CA, Turnbull D, McPhee AJ, et al. The effects of antenatal dietary and lifestyle advice for women who are overweight or obese on maternal diet and physical activity: The LIMIT randomised trial. BMC Med. 2014;12(1):161.
Farajzadegan Z, Pozveh ZA. The design of maternal centered life-style modification program for weight gain management during pregnancy - a study protocol. J Res Med Sci. 2013;18(8):683–7.
Gesell SB, Katula JA, Strickland C, Vitolins MZ. Feasibility and initial efficacy evaluation of a community-based cognitive-behavioral lifestyle intervention to prevent excessive weight gain during pregnancy in Latina women. Matern Child Health J. 2015;19:1842–52.
Graham ML, Strawderman MS, Demment M, Olson CM. Does usage of an eHealth intervention reduce the risk of excessive gestational weight gain? Secondary analysis from a randomized controlled trial. J Med Internet Res. 2017;19(1):e6.
Guelinckx I, Devlieger R, Mullie P, Vansant G. Effect of lifestyle intervention on dietary habits, physical activity, and gestational weight gain in obese pregnant women: a randomized controlled trial. Am J Clin Nutr. 2010;91(2):373–80.
Haby K, Glantz A, Hanas R, Premberg A. Mighty mums - an antenatal health care intervention can reduce gestational weight gain in women with obesity. Midwifery. 2015;31(7):685–92.
Harden SM, Beauchamp MR, Pitts BH, Nault EM, Davy BM, You W, Weiss P, Estabrooks PA. Group-based lifestyle sessions for gestational weight gain management: a mixed method approach. Am J Health Behav. 2014;38(4):560–9.
Harrison CL, Lombard CB, Strauss BJ, Teede HJ. Optimizing healthy gestational weight gain in women at high risk of gestational diabetes: a randomized controlled trial. Obesity. 2013;21(5):904–9.
Hawkins M, Hosker M, Marcus BH, Rosal MC, Braun B, Stanek EJ 3rd, Markenson G, Chasan-Taber L. A pregnancy lifestyle intervention to prevent gestational diabetes risk factors in overweight Hispanic women: a feasibility randomized controlled trial. Diabet Med. 2015;32(1):108–15.
Hui A, Back L, Ludwig S, Gardiner P, Sevenhuysen G, Dean H, Sellers E, McGavock J, Morris M, Bruce S, et al. Lifestyle intervention on diet and exercise reduced excessive gestational weight gain in pregnant women under a randomised controlled trial. BJOG. 2012;119(1):70–7.
Hui AL, Back L, Ludwig S, Gardiner P, Sevenhuysen G, Dean HJ, Sellers E, McGavock J, Morris M, Jiang D, et al. Effects of lifestyle intervention on dietary intake, physical activity level, and gestational weight gain in pregnant women with different pre-pregnancy body mass index in a randomized control trial. BMC Pregnancy Childbirth. 2014;14:331.
Hui AL, Ludwig S, Gardiner P, Sevenhuysen G, Murray R, Morris M, Shen GX. Community-based exercise and dietary intervention during pregnancy:a pilot study. Can J Diab. 2006;30(2):1–7.
Jackson RA, Stotland NE, Caughey AB, Gerbert B. Improving diet and exercise in pregnancy with video doctor counseling: a randomized trial. Patient Educ Couns. 2011;83(2):203–9.
Jeffries K, Shub A, Walker SP, Hiscock R, Permezel M. Reducing excessive weight gain in pregnancy: a randomised controlled trial. Med J Aust. 2009;191(8):429–33.
Jing W, Huang Y, Liu X, Luo B, Yang Y, Liao S. The effect of a personalized intervention on weight gain and physical activity among pregnant women in China. Int J Gynaecol Obstet. 2015;129(2):138–41.
Kinnunen TI, Raitanen J, Aittasalo M, Luoto R. Preventing excessive gestational weight gain-a secondary analysis of a cluster-randomised controlled trial. Eur J Clin Nutr. 2012;66(12):1344–50.
Koivusalo SB, Rono K, Klemetti MM, Roine RP, Lindstrom J, Erkkola M, Kaaja RJ, Poyhonen-Alho M, Tiitinen A, Huvinen E, et al. Gestational diabetes mellitus can be prevented by lifestyle intervention: the Finnish gestational diabetes prevention study (RADIEL): a randomized controlled trial. Diab Care. 2016;39(1):24–30.
LeBlanc ES, Vesco KK, Funk KL, Karanja N, Smith N, Stevens VJ. Prepare, a randomized trial to promote and evaluate weight loss among overweight and obese women planning pregnancy: study design and rationale. Contemp Clin Trials. 2016;49:174–80.
McCarthy EA, Walker SP, Ugoni A, Lappas M, Leong O, Shub A. Self-weighing and simple dietary advice for overweight and obese pregnant women to reduce obstetric complications without impact on quality of life: a randomised controlled trial. BJOG. 2016;123(6):965–73.
Nagle C, Skouteris H, Hotchin A, Bruce L, Patterson D, Teale G. Continuity of midwifery care and gestational weight gain in obese women: a randomised controlled trial. BMC Public Health. 2011;11:174.
Petrella E, Malavolti M, Bertarini V, Pignatti L, Neri I, Battistini NC, Facchinetti F. Gestational weight gain in overweight and obese women enrolled in a healthy lifestyle and eating habits program. J Matern Fetal Neonatal Med. 2014;27(13):1348–52.
Pollak KI, Alexander SC, Bennett G, Lyna P, Coffman CJ, Bilheimer A, Farrell D, Bodner ME, Swamy GK, Ostbye T. Weight-related SMS texts promoting appropriate pregnancy weight gain: a pilot study. Patient Educ Couns. 2014;97(2):256–60.
Polley B, Wing R, Sims C. Randomized controlled trial to prevent excessive weight gain in pregnant women. Int J Obes. 2002;26(11):1494–502.
Quinlivan JA, Lam LT, Fisher J. A randomised trial of a four-step multidisciplinary approach to the antenatal care of obese pregnant women. Aust N Z J Obstet Gynaecol. 2011;51(2):141–6.
Rauh K, Gabriel E, Kerschbaum E, Schuster T, Kries R, Amann-Gassner U, Hauner H. Safety and efficacy of a lifestyle intervention for pregnant women to prevent excessive maternal weight gain: a cluster-randomized controlled trial. BMC Pregnancy Childbirth. 2013;13:151.
Rauh K, Kunath J, Rosenfeld E, Kick L, Ulm K, Hauner H. Healthy living in pregnancy: a cluster-randomized controlled trial to prevent excessive gestational weight gain - rationale and design of the GeliS study. BMC Pregnancy Childbirth. 2014;14:119.
Renault KM, Carlsen EM, Haedersdal S, Nilas L, Secher NJ, Eugen-Olsen J, Cortes D, Olsen SF, Halldorsson TI, Norgaard K. Impact of lifestyle intervention for obese women during pregnancy on maternal metabolic and inflammatory markers. Int J Obes. 2017;41(4):598–605.
Ronnberg AK, Ostlund I, Fadl H, Gottvall T, Nilsson K. Intervention during pregnancy to reduce excessive gestational weight gain - a randomised controlled trial. BJOG. 2015;122:537–44.
Skouteris H, McPhie S, Hill B, McCabe M, Milgrom J, Kent B, Bruce L, Herring S, Gale J, Mihalopoulos C, et al. Health coaching to prevent excessive gestational weight gain: a randomized-controlled trial. Br J Health Psychol. 2016;21(1):31–51.
Smith K, Lanningham-Foster L, Welch A, Campbell C. Web-based behavioral intervention increases maternal exercise but does not prevent excessive gestational weight gain in previously sedentary women. J Phys Act Health. 2016;13(6):587–93.
Szmeja MA, Cramp C, Grivell RM, Deussen AR, Yelland LN, Dodd JM. Use of a DVD to provide dietary and lifestyle information to pregnant women who are overweight or obese: a nested randomised trial. BMC Pregnancy Childbirth. 2014;14:409.
Thornton YS. Preventing excessive weight gain during pregnancy through dietary and lifestyle counseling: a randomized controlled trial. Obstet Gynecol. 2009;114(1):173 author reply 173-174.
Vinter CA, Jensen DM, Ovesen P, Beck-Nielsen H, Jorgensen JS. The LiP (lifestyle in pregnancy) study: a randomized controlled trial of lifestyle intervention in 360 obese pregnant women. Diab Care. 2011;34(12):2502–7.
Willcox J, Wilkinson S, Lappas M, Ball K, Crawford D, McCarthy E, Fjeldsoe B, Whittaker R, Maddison R, Campbell K. A mobile health intervention promoting healthy gestational weight gain for women entering pregnancy at a high body mass index: the txt4two pilot randomised controlled trial. BJOG. 2017;124:1718.
Wolff S, Legarth J, Vangsgaard K, Toubro S, Astrup A. A randomized trial of the effects of dietary counseling on gestational weight gain and glucose metabolism in obese pregnant women. Int J Obes. 2008;32(3):495–501.
Berry D, Verbiest S, Hall EG, Dawson I, Norton D, Willis S, McDonald K, Stuebe A. A postpartum community-based weight management intervention designed for low-income women: feasibility and initial efficacy testing. J Natl Black Nurses Assoc. 2015;26(1):29–39.
Bertz F, Brekke HK, Ellegard L, Rasmussen KM, Wennergren M, Winkvist A. Diet and exercise weight-loss trial in lactating overweight and obese women. Am J Clin Nutr. 2012;96(4):698–705.
Chang MW, Brown R, Nitzke S. Results and lessons learned from a prevention of weight gain program for low-income overweight and obese young mothers: mothers in motion. BMC Public Health. 2017;17(1):182.
Colleran HL, Lovelady CA. Use of MyPyramid menu planner for moms in a weight-loss intervention during lactation. J Acad Nutr Diet. 2012;112(4):553–8.
Craigie AM, Macleod M, Barton KL, Treweek S, Anderson AS. Supporting postpartum weight loss in women living in deprived communities: design implications for a randomised control trial. Eur J Clin Nutr. 2011;65(8):952–8.
Gilmore LA, Klempel MC, Martin CK, Myers CA, Burton JH, Sutton EF, Redman LM. Personalized Mobile health intervention for health and weight loss in postpartum women receiving women, infants, and children benefit: a randomized controlled pilot study. J Women's Health (Larchmt). 2017;26(7):719–27.
Haire-Joshu DL, Schwarz CD, Peskoe SB, Budd EL, Brownson RC, Joshu CE. A group randomized controlled trail integrating obesity prevention and control for postpartum adolescents in a home visiting program. Int J Behav Nutr Phy. 2015;12:88.
Herring SJ, Cruice JF, Bennett GG, Davey A, Foster GD. Using technology to promote postpartum weight loss in urban, low-income mothers: a pilot randomized controlled trial. J Nutr Educ Behav. 2014;46(6):610–5.
Huseinovic E, Bertz F, Agelii ML, Johansson EH, Winkvist A, Brekke HK. Effectiveness of a weight loss intervention in postpartum women: results from a randomized controlled trial in primary health care. Am J Clin Nutr. 2016;104(2):362–70.
Keller C, Ainsworth B, Records K, Todd M, Belyea M, Vega-Lopez S, Permana P, Coonrod D, Nagle-Williams A. A comparison of a social support physical activity intervention in weight management among post-partum Latinas. BMC Public Health. 2014;14:971.
Krummel D, Semmens E, MacBride AM, Fisher B. Lessons learned from the mothers' overweight management study in 4 West Virginia WIC offices. J Nutr Educ Behav. 2010;42(3 Suppl):S52–8.
Leermakers EA, Anglin K, Wing RR. Reducing postpartum weight retention through a correspondence intervention. Int J Obesity Related Metabol Disord. 1998;22(11):1103–9.
Nicklas JM, Zera CA, England LJ, Rosner BA, Horton E, Levkoff SE, Seely EW. A web-based lifestyle intervention for women with recent gestational diabetes mellitus: a randomized controlled trial. Obstet Gynecol. 2014;124(3):563–70.
Østbye T, Krause KM, Lovelady CA, Morey MC, Bastian LA, Peterson BL, Swamy GK, Brouwer RJN, McBride CM. Active mothers postpartum. A randomized controlled weight-loss intervention trial. Am J Prev Med. 2009;37(3):173–80.
O'Toole ML, Sawicki MA, Artal R. Structured diet and physical activity prevent postpartum weight retention. J Women's Health (Larchmt). 2003;12(10):991–8.
Phelan S, Brannen A, Erickson K, Diamond M, Schaffner A, Muñoz-Christian K, Stewart A, Sanchez T, Rodriguez VC, Ramos DI, et al. ‘Fit Moms/Mamás Activas’ internet-based weight control program with group support to reduce postpartum weight retention in low-income women: study protocol for a randomized controlled trial. Trials. 2015;16:59.
Stendell-Hollis NR, Thompson PA, West JL, Wertheim BC, Thomson CA. A comparison of Mediterranean-style and MyPyramid diets on weight loss and inflammatory biomarkers in postpartum breastfeeding women. J Women's Health (Larchmt). 2013;22(1):48–57.
Wilkinson SA, Pligt P, Gibbons KS, McIntyre HD. Trial for reducing weight retention in new mums: a randomised controlled trial evaluating a low intensity, postpartum weight management programme. J Hum Nutr Diet. 2015;28(Suppl 1):15–28.
Bechtel-Blackwell DA. Computer-assisted self-interview and nutrition education in pregnant teens. Clin Nurs Res. 2002;11(4):450–62.
Chasan-Taber L, Marcus BH, Rosal MC, Tucker KL, Hartman SJ, Pekow P, Stanek E, Braun B, Solomon CG, Manson JAE, et al. Proyecto Mama: A lifestyle intervention in overweight and obese Hispanic women: A randomised controlled trial - study protocol. BMC Pregnancy Childbirth. 2015;15(1):157.
Ferrara A, Hedderson MM, Brown SD, Albright CL, Ehrlich SF, Tsai AL, Caan BJ, Sternfeld B, Gordon NP, Schmittdiel JA, et al. The comparative effectiveness of diabetes prevention strategies to reduce postpartum weight retention in women with gestational diabetes mellitus: the gestational Diabetes' effects on moms (GEM) cluster randomized controlled trial. Diabetes Care. 2016;39(1):65–74.
Haakstad LA, Bo K. Effect of regular exercise on prevention of excessive weight gain in pregnancy: a randomised controlled trial. Eur J Contracept Reprod Health Care. 2011;16(2):116–25.
Herring SJ, Cruice JF, Bennett GG, Darden N, Wallen JJ, Rose MZ, Davey A, Foster GD. Intervening during and after pregnancy to prevent weight retention among African American women. Prev Med Rep. 2017;7:119–23.
Huang TT, Yeh CY, Tsai YC. A diet and physical activity intervention for preventing weight retention among Taiwanese childbearing women: a randomised controlled trial. Midwifery. 2011;27(2):257–64.
John E, Cassidy DM, Playle R, Jewell K, Cohen D, Duncan D, Newcombe RG, Busse M, Owen-Jones E, Williams N, et al. Healthy eating and lifestyle in pregnancy (HELP): a protocol for a cluster randomised trial to evaluate the effectiveness of a weight management intervention in pregnancy. BMC Public Health. 2014;14:439.
Martin J, MacDonald-Wicks L, Hure A, Smith R, Collins CE. Reducing postpartum weight retention and improving breastfeeding outcomes in overweight women: a pilot randomised controlled trial. Nutrients. 2015;7(3):1464–79.
Peccei A, Blake-Lamb T, Rahilly D, Hatoum I, Bryant A. Intensive prenatal nutrition counseling in a community health setting: a randomized controlled trial. Obstet Gynecol. 2017;130(2):423–32.
Phelan S, Phipps MG, Abrams B, Darroch F, Schaffner A, Wing RR. Randomized trial of a behavioral intervention to prevent excessive gestational weight gain: the fit for delivery study. Am J Clin Nutr. 2011;93(4):772–9.
Sagedal LR, Sanda B, Overby NC, Bere E, Torstveit MK, Lohne-Seiler H, Hillesund ER, Pripp AH, Henriksen T, Vistad I. The effect of prenatal lifestyle intervention on weight retention 12 months postpartum: results of the Norwegian fit for delivery randomised controlled trial. BJOG. 2017;124(1):111–21.
Tawfik MY. The impact of health education intervention for prevention and early detection of type 2 diabetes in women with gestational diabetes. J Community Health. 2017;42(3):500–10.
Thomson JL, Tussing-Humphreys LM, Goodman MH. Delta healthy sprouts: a randomized comparative effectiveness trial to promote maternal weight control and reduce childhood obesity in the Mississippi Delta. Contemp Clin Trials. 2014;38(1):82–91.
Vesco KK, Karanja N, King JC, Gillman MW, Perrin N, McEvoy C, Eckhardt C, Smith KS, Stevens VJ. Healthy moms, a randomized trial to promote and evaluate weight maintenance among obese pregnant women: study design and rationale. Contemp Clin Trials. 2012;33(4):777–85.
Ames GE, Perri MG, Fox LD, Fallon EA, De Braganza N, Murawski ME, Pafumi L, Hausenblas HA. Changing weight-loss expectations: a randomized pilot study. Eat Behav. 2005;6(3):259–69.
Chang MW, Nitzke S, Brown R. Design and outcomes of a mothers in motion behavioral intervention pilot study. J Nutr Educ Behav. 2010;42(3 Suppl):S11–21.
Lim SS, Norman RJ, Clifton PM, Noakes M. Psychological effects of prescriptive vs general lifestyle advice for weight loss in young women. J Am Diet Assoc. 2009;109(11):1917–21.
Mutsaerts M. Randomized trial of a lifestyle program in obese infertile women. Ned Tijdschr Geneeskd. 2017;161:1942.
Bennett GG, Foley P, Levine E, Whiteley J, Askew S, Steinberg DM, Batch B, Greaney ML, Miranda H, Wroth TH, et al. Behavioral treatment for weight gain prevention among black women in primary care practice: a randomized clinical trial. JAMA Intern Med. 2013;173:1770–7.
Berry D, Colindres M, Sanchez-Lugo L, Sanchez M, Neal M, Smith-Miller C. Adapting, feasibility testing, and pilot testing a weight management intervention for recently immigrated Spanish-speaking women and their 2- to 4-year-old children. Hispanic Health Care Int. 2011;9(4):186–93.
Eiben G, Lissner L. Health hunters - an intervention to prevent overweight and obesity in young high-risk women. Int J Gynaecol Obstet. 2006;30(4):691–6.
Foley P, Levine E, Askew S, Puleo E, Whiteley J, Batch B, Heil D, Dix D, Lett V, Lanpher M, et al. Weight gain prevention among black women in the rural community health center setting: the shape program. BMC Public Health. 2012;12(1):305.
Klem ML, Viteri JE, Wing RR. Primary prevention of weight gain for women aged 25-34: the acceptability of treatment formats. Int J Obes. 2000;24(2):219–25.
Kuhlmann AK, Dietz PM, Galavotti C, England LJ. Weight-management interventions for pregnant or postpartum women. Am J Prev Med. 2008;34(6):523–8.
Poston L, Caleyachetty R, Cnattingius S, Corvalán C, Uauy R, Herring S, Gillman MW. Preconceptional and maternal obesity: epidemiology and health consequences. Lancet Diab Endocrinol. 2016;4(12):1025–36.
Institute of Medicine, National Research Council. Weight Gain During Pregnancy: Reexamining the Guidelines. Washington: The National Academies Press; 2009.
Health Canada. Prenatal nutrition guidelines for health professionals. In. Ottawa: Health Canada; 2010.
Department of Health. Clinical Practice Guidelines: Pregnancy Care. Canberra: Australian Government Department of Health; 2018.
Phelan S. Pregnancy: a "teachable moment" for weight control and obesity prevention. Am J Obstet Gynecol. 2010;202(2):135.e131–8.
Kocher EL, Sternberg Lamb JM, McGarvey ST, Faiai M, Muasau-Howard BT, Hawley NL. Conceptions of pregnancy health and motivations for healthful behavior change among women in American Samoa. Women Birth. 2018;31(1):e32–41.
Hanson M, Barker M, Dodd JM, Kumanyika S, Norris S, Steegers E, Stephenson J, Thangaratinam S, Yang H. Interventions to prevent maternal obesity before conception, during pregnancy, and post partum. Lancet DiabEndocrinol. 2017;5(1):65–76.
Deputy NP, Sharma AJ, Kim SY, Hinkle SN. Prevalence and characteristics associated with gestational weight gain adequacy. Obstet Gynecol. 2015;125(4):773.
Jarman M, Yuan Y, Pakseresht M, Shi Q, Robson PJ, Bell RC. Patterns and trajectories of gestational weight gain: a prospective cohort study. CMAJ open. 2016;4(2):E338.
Knabl J, Riedel C, Gmach J, Ensenauer R, Brandlhuber L, Rasmussen KM, Schiessl B, von Kries R. Prediction of excessive gestational weight gain from week-specific cutoff values: a cohort study. J Perinatol: official journal of the California Perinatal Association. 2014;34(5):351–6.
Hill B, Hayden M, McPhie S, Bailey C, Skouteris H. Preconception and antenatal knowledge and beliefs about gestational weight gain. Aust N Z J Obstet Gynaecol. 2019;59(5):634–640.
National Core Maternity Indicators [https://www.aihw.gov.au/reports/mothers-babies/ncmi-data-visualisations/contents/antenatal-period-indicators].
Guevarra MV, Stubbs JM, Assareh H, Achat HM. Risk factors associated with late entry to antenatal care visits in NSW in 2014. Aust N Z J Public Health. 2017;41(5):543–4.
Stephenson J, Heslehurst N, Hall J, Schoenaker DA, Hutchinson J, Cade JE, Poston L, Barrett G, Crozier SR, Barker M. Before the beginning: nutrition and lifestyle in the preconception period and its importance for future health. Lancet. 2018.
Godfrey KM, Reynolds RM, Prescott SL, Nyirenda M, Jaddoe VW, Eriksson JG, Broekman BF. Influence of maternal obesity on the long-term health of offspring. Lancet Diab Endocrinol. 2017;391(10132):1830–1841.
Marchi J, Berg M, Dencker A, Olander E, Begley C. Risks associated with obesity in pregnancy, for the mother and baby: a systematic review of reviews. Obes Rev. 2015;16(8):621–38.
Baidal JAW, Locks LM, Cheng ER, Blake-Lamb TL, Perkins ME, Taveras EM. Risk factors for childhood obesity in the first 1,000 days: a systematic review. Am J Prev Med. 2016;50(6):761–79.
Montazeri P, Vrijheid M, Martinez D, Basterrechea M, Fernandez-Somoano A, Guxens M, Iñiguez C, Lertxundi A, Murcia M, Tardon A. Maternal metabolic health parameters during pregnancy in relation to early childhood BMI trajectories. Obesity. 2018;26(3):588–96.
Ziyab AH, Karmaus W, Kurukulaaratchy RJ, Zhang H, Arshad SH. Developmental trajectories of body mass index from infancy to 18 years of age: prenatal determinants and health consequences. J Epidemiol Community Health. 2014;68(10):934–41.
Steel A, Lucke J, Adams J. The prevalence and nature of the use of preconception services by women with chronic health conditions: an integrative review. BMC Womens Health. 2015;15(1):14.
Oza-Frank R, Kachoria R, Keim SA, Klebanoff MA. Provision of specific preconception care messages and associated maternal health behaviors before and during pregnancy. Am J Obstet Gynecol. 2015;212(3):372 e371–372. e378.
Oza-Frank R, Gilson E, Keim SA, Lynch CD, Klebanoff MA. Trends and factors associated with self-reported receipt of preconception care: PRAMS, 2004–2010. Birth. 2014;41(4):367–73.
Bearak J, Popinchalk A, Alkema L, Sedgh G. Global, regional, and subregional trends in unintended pregnancy and its outcomes from 1990 to 2014: estimates from a Bayesian hierarchical model. Lancet Global Health. 2018;6(4):e380–9.
Anthropometric Reference Data for Children and Adults: United States, 2007–2010. [https://www.cdc.gov/nchs/data/series/sr_11/sr11_252.pdf].
Gomersall S, Dobson A, Brown W. Weight gain, overweight, and obesity: determinants and health outcomes from the Australian longitudinal study on Women’s health. Curr Obes Rep. 2014;3(1):46–53.
Wilkinson S, Poad D, Stapleton H. Maternal overweight and obesity: a survey of clinicians’ characteristics and attitudes, and their responses to their pregnant clients. BMC Pregnancy Childbirth. 2013;13(1):117.
Vincze L, Rollo M, Hutchesson M, Hauck Y, MacDonald-Wicks L, Wood L, Callister R, Collins C. Interventions including a nutrition component aimed at managing gestational weight gain or postpartum weight retention: a systematic review and meta-analysis. JBI Database System Rev Implement Rep. 2019;17(3):297–364.
Vincze L, Rollo ME, Hutchesson MJ, Burrows TL, MacDonald-Wicks L, Blumfield M, Collins CE. A cross sectional study investigating weight management motivations, methods and perceived healthy eating and physical activity influences in women up to five years following childbirth. Midwifery. 2017;49:124–33.
Carter-Edwards L, Østbye T, Bastian LA, Yarnall KS, Krause KM. Barriers to adopting a healthy lifestyle: insight from postpartum women. BMC Res Notes. 2009;2(1):161.
Why Choose an Accredited Practising Dietitian? [https://daa.asn.au/what-dietitans-do/choosing-your-nutrition-expert/].
Cummings S, Parham ES, Strain GW. Position of the American dietetic: association weight management. J Am Diet Assoc. 2002;102(8):1145–55.
Franklin B, Fern A, Fowler A, Spring T. Exercise physiologist’s role in clinical practice. Br J Sports Med. 2009;43(2):93–8.
Yeo S, Walker JS, Caughey MC, Ferraro AM, Asafu-Adjei JK. What characteristics of nutrition and physical activity interventions are key to effectively reducing weight gain in obese or overweight pregnant women? A systematic review and meta-analysis. Obes Rev. 2017;18(4):385–99.
Williams LT, Barnes K, Ball L, Ross LJ, Sladdin I, Mitchell LJ. How Effective Are Dietitians in Weight Management? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Healthcare (Basel). 2019;7(1):e20.
Acknowledgements
Not applicable.
Funding
The scoping review was supported by a School of Health Sciences small grant. Dr. Melinda Hutchesson is supported by a Gladys M Brawn Career Development Fellowship (Teaching Assistance).Dr. Siew Lim is supported by a National Health and Medical Research Council Early Career Fellowship. A/Prof Lisa Moran is supported by a National Heart Foundation Future Leader Fellowship. The funding bodies played no role in the study.
Author information
Authors and Affiliations
Contributions
MJH, MMH, HB, SL, LM, LV, MR, JH contributed to the design/methodology of the scoping review, as well as screening and data extraction. MJH, MMH and HB collated the results, MH and JH drafted the manuscript, and MJH, MMH, HB, SL, LM, LV, MR, JH read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1:
Table S1. Full electronic search for one database (MEDLINE). Table S2. Summary of included Randomised Control Trials. Table S3. Summary of Included Systematic Reviews.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hutchesson, M.J., de Jonge Mulock Houwer, M., Brown, H.M. et al. Supporting women of childbearing age in the prevention and treatment of overweight and obesity: a scoping review of randomized control trials of behavioral interventions. BMC Women's Health 20, 14 (2020). https://doi.org/10.1186/s12905-020-0882-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-020-0882-3