
Abstract
Background
Palliative care addresses multiple unmet needs of people with chronic obstructive pulmonary disease (COPD) or interstitial lung diseases (ILD) and their family and/or friend caregivers, but it remains highly underused. Pulmonary rehabilitation (PR) may provide a key opportunity to introduce palliative care. We aim to explore the effects of palliative care education as part of PR on knowledge about this field in people with COPD or ILD and their family and/or friend caregivers.
Methods
A randomized controlled study will compare PR with palliative care education (experimental) with traditional PR (control) in people with COPD or ILD and their family and/or friend caregivers. Family and/or friend caregivers will be invited to take part in education and psychosocial support sessions. In addition to the usual educational content, the experimental group will have a session on palliative care, a “Peer-to-peer session”, two “Get-apart sessions” and online sessions. The “Peer-to-peer session” and the “Get-apart sessions” will be discussions about topics suggested by participants. The “Get-apart sessions” will be dedicated to people with COPD or ILD apart from their family and/or friend caregivers and vice versa. The online sessions will be zoom meetings to discuss any health-related issues raised by participants, at a flexible time. A mixed-methods approach will be used to evaluate the outcomes. The primary outcome will be knowledge about palliative care. Secondary outcomes will include attitude towards palliative care referral, symptoms, disease impact, health-related quality of life, needs, knowledge about the disease, burden of providing care, adherence, adverse events and referral to a specialist palliative care team. Quantitative and qualitative data will be collected at baseline and end of PR. At 6-months post-PR, only patient-reported outcomes will be collected. For the primary outcome, time*group interaction will be analyzed with mixed analysis of variance.
Discussion
This study aims to demonstrate the impact of integrating palliative care into the PR education program.
Trial registration
The trial was registered in the ClinicalTrials.gov U.S. National Library of Medicine, on 1st September, 2023 (NCT06046547).
Similar content being viewed by others


Background
Chronic respiratory diseases, including chronic obstructive pulmonary disease (COPD) and interstitial lung diseases (ILD) are among the most common non-communicable diseases worldwide [1]. They are leading causes of mortality and constitute 4.1% of disability-adjusted life-years (DALYs) for all causes, with a significant and increasing individual, societal and economic burden [1, 2].
People with COPD or ILD suffer from physical and psychological symptom burden, multiple limitations in activities and restrictions in participation in daily life, and uncertain expectations about the future, which all have a tremendous impact on their health-related quality of life (HRQoL) [3,4,5,6,7,8]. Family and/or friend caregivers are their main source of support, throughout the whole disease trajectory [5]. They fulfill many roles such as housekeeping and shopping, encouraging adherence to treatments, assisting to coordinate care across providers and settings, recognizing and managing emergency situations and providing emotional and spiritual support over time [5, 9, 10]. Indeed, they facilitate the overcoming of daily challenges and contribute to improved health outcomes e.g., reduce hospitalizations [10, 11]. So, not surprisingly, caring for a person with COPD or ILD can be highly demanding and has major influence on various domains of family and/or friend caregivers’ lives, including physical, psychological, social and financial [5, 12]. In daily clinical practice, this impact of the caring role is undervalued and not addressed by healthcare professionals. In fact, there is limited literature on interventions that include family and/or friend caregivers of people with COPD or ILD [9, 13,14,15,16,17].
Pulmonary rehabilitation (PR) and palliative care are two multicomponent interventions crucial for people with COPD or ILD irrespective of their prognosis [3, 7, 18, 19]. They have been recognized as “two sides of the same coin” [20], by sharing several key characteristics such as: 1) specific aims of managing symptoms, optimizing functional independence and improving HRQoL; 2) a holistic and person-centered approach; 3) individualized goal setting; 4) family and/or friend caregivers involvement and support; and 5) access based on needs [3, 18]. Differences have also been described, namely in the type of treatment interventions used. For example, exercise training is a core component of PR and infrequently used in palliative care. On the other hand, advance care planning is an important element in palliative care and scarcely discussed in PR, even nowadays [3].
Recognizing family and/or friend caregivers as a cornerstone of the unit of care has been consistently advocated by palliative care in different chronic progressive diseases [7, 21] and is clearly stated in the most recent recommendations for serious respiratory illness [18, 22]. Less explored has been the role of PR to support family and/or friend caregivers [9, 13, 15,16,17]. To date, only one randomized controlled trial has been performed in this area [17]. This study showed that involving the family in PR improves the coping strategies and the psychosocial adjustment to illness of the whole family (not only people with COPD).
In recent years, universal PR and upstream palliative care have been advocated, based on unmet needs [3, 18, 22]. Needs of patients and family and/or friend caregivers living with COPD or ILD encompass multiple life dimensions and include e.g., validation and support throughout the disease, public awareness, need to act and be treated normally, meeting others in similar circumstances, coping strategies, open communication, be included in decision-making, understand the disease, strategies for social participation, support from others but allowing autonomy and medication management/equipment handling [5, 6, 23, 24]. However, palliative care remains highly underused in people with chronic respiratory diseases [18]. One of the reasons reported is the unclear awareness of the potential role of palliative care allied to inadequate knowledge and misperceptions of this field among patients [18, 25, 26].
PR could be an ideal setting to identify and assess unmet needs of people with COPD or ILD and their family and/or friend caregivers and introduce palliative care [3, 19, 27]. Education and psychosocial support sessions are a well-established component of PR. Including palliative care educational content (e.g., concept, role and goals of palliative care, symptom control, disease impact, psychosocial support and planning for the future) in these sessions and actively involving family and/or friend caregivers represents an important opportunity to introduce palliative care in PR. Indeed, already a decade ago advance care planning was mentioned as one of the educational topics in PR [28], which has been well received by patients [29]. Moreover, across the PR program, individuals could be timely referred to a specialist palliative care team, which has the potential to add particular benefit in breathlessness management, advance care planning and psychosocial support. Another possible strategy to improve patients’ and family and/or friend caregivers’ care is educating and training rehabilitation staff in palliative care issues and advanced communication skills [3, 7, 22, 27]. In fact, placing focus on palliative care in PR has the potential to provide the best chance of timely addressing unmet needs of those with COPD or ILD and their family and/or friend caregivers. However, the direct effects of this integrated care model on patients’ and family and/or friend caregivers’ outcomes have not been studied before.
We hypothesize that by integrating palliative care education in PR for people with COPD or ILD and their family and/or friend caregivers we will improve knowledge about palliative care. Furthermore, we hypothesize that by enhancing educational opportunities, namely including the topic of palliative care in PR we will change the attitude towards palliative care referral, improve symptoms, disease impact, HRQoL, needs, knowledge about the disease and reduce burden of providing care.
The primary aim of this study is to explore the effects of palliative care education as part of PR on people with COPD or ILD and their family and/or friend caregivers’ knowledge about palliative care. Secondary aims are to: a) understand the perspectives of people with COPD or ILD and their family and/or friend caregivers about integrating palliative care education in PR; and b) explore the effects of PR with more educational opportunities, namely including the topic of palliative care on people with COPD or ILD and their family and/or friend caregivers’ attitude towards palliative care referral, symptoms, disease impact, HRQoL, needs, knowledge about the disease and burden of providing care.
This article describes the study protocol in detail and provides an overview of its strengths and limitations.
Methods
Study design
A randomized controlled study to compare PR with palliative care education (experimental) with traditional PR (control) in people with COPD or ILD and their family and/or friend caregivers has been deigned. The study was registered in the ClinicalTrials.gov U.S. National Library of Medicine (NCT06046547) and will follow the Consolidated Standards of Reporting Trials (CONSORT) statement for nonpharmacological treatments [30], Template for Intervention Description and Replication (TIDieR) checklist and guide [31], Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines [32] and Good Reporting of A Mixed Methods Study (GRAMMS) framework [33].
Participants will be randomized into an experimental group (EG) and a control group (CG), using a 1:1 allocation ratio and random block sizes of two and four. An independent researcher will use an online software tool (https://www.sealedenvelope.com/simple-randomiser/v1/lists) to generate a computer-based random allocation list and will inform the lead researcher (MAM) about their group allocation via phone call.
Assessors and the researcher responsible for moderating the focus groups will not be involved in PR provision and will be blinded to group allocation. Participants and the researcher conducting the intervention will not be blinded to group allocation, due to the nature of the intervention. The blindness of the researcher performing the data analysis will be ensured by anonymizing all data.
Participants
People with COPD or ILD and their family and/or friend caregivers will be recruited from the outpatient pulmonary rehabilitation unit at Centro Hospitalar do Baixo Vouga (CHBV), a secondary hospital. Recruitment started in August 2023, with final data collection expected to be completed in June 2026. The pulmonologist of the PR program will identify eligible participants and explain the study. Patients will be eligible if they are adults with a diagnosis of COPD according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria [34] or with a multidisciplinary diagnosis of ILD [35] and are clinically stable in the previous month (i.e., without acute exacerbation). Patients will be excluded if they present a musculoskeletal, neurological or psychiatric condition which may limit their participation in PR, had participated in any PR program in the last 6 months, had received specialist palliative care in the last 12 months or are unable to understand Portuguese. Family and/or friend caregivers will be eligible if they are adults identified by the participating people with COPD or ILD as caregivers. For this purpose, it will be explained to people with COPD or ILD that a family and/or friend caregiver is any relative, partner, friend, neighbor, or significant other with personal relationship with them, and who provides a broad range of unpaid assistance, namely with activities of daily living (e.g., toileting, feeding and bathing) and instrumental activities of daily living (e.g., shopping, meal preparation and managing finances)] [36]. Family and/or friend caregivers will be excluded if they present a neurological or psychiatric condition which may limit their participation or are unable to understand Portuguese. An appointment with those willing to participate will be scheduled to clarify any doubts, gather informed consents and conduct baseline assessments.
Intervention
Both groups will follow a multidisciplinary team-based PR model at CHBV delivered by a pulmonologist, a physiotherapist and a nurse, and will include supervised exercise sessions and education and psychosocial support sessions in a group setting over a 12-week period. Other healthcare professionals, including a psychologist and a nutritionist will be involved in coordinating education and psychosocial support sessions.
Exercise sessions
The exercise sessions will follow the same structure for both groups and will be delivered in accordance with international guidelines [35, 37, 38]. It will occur twice per week for a maximum of 90 min. Continuous telemetry with electrocardiogram and oxygen saturation will be used and perceived dyspnoea and fatigue will be monitored with modified Borg scale throughout the session [39]. Intensity of the aerobic and resistance training will be prescribed using the 6-min walking test (6-MWT) or the cardiopulmonary exercise testing (if available) and the one-repetition maximum (1-RM), respectively. Exercise sessions will include 10 min of warm up, 30 to 40 min of aerobic cycle ergometer and/or treadmill training at 80% of the average speed achieved during the 6-MWT or 60% of their work peak [37, 40], 20 to 30 min of resistance training at 60 to 70% of 1-RM [37], and 10 min of cool down. Progression of training intensity will be tailored according to the perceived dyspnoea and fatigue (4–6 in the modified Borg scale) [39]. Adjunct components such as airway clearance techniques, balance training, inspiratory muscles training and electric neuromuscular electrical stimulation will be prescribed according to individuals’ needs within this timeframe.
Education and psychosocial support sessions
The education and psychosocial support sessions will follow the same structure for both groups, however the number of sessions will be different, and the content areas will sometimes vary, as described below.
Each education and psychosocial support session will be delivered after the exercise training and will last approximately 60 min. Family and/or friend caregivers will be invited and encouraged to take part in all sessions. They will be led by healthcare professionals of the multidisciplinary team and all participants will sit in a circular arrangement. An interactive style will be followed, to engage people with COPD or ILD and their family and/or friend caregivers in an active dialogue and reflection about the topic being discussed. The healthcare professional will avoid medical jargon and facilitate participation of the group e.g., asking open questions that lead to meaningful interaction. An active effort will be conducted to adapt the education process to the characteristics of participants at an individual level e.g., revising topics covered at the end to confirm the achievement of the core knowledge and skills. Moreover, written materials will be provided at the end of each session.
Sessions dedicated to both groups
The following topics will be explored in both groups (i.e., EG and CG): a) information on chronic respiratory diseases; b) medication, inhaler techniques, oxygen therapy and non-invasive ventilation; c) symptom management and exacerbations; d) exercise and physical activity; e) action plan; f) anxiety and depression management; and g) nutrition.
Sessions dedicated only to the experimental group
For the EG there will be four additional face-to-face sessions: a palliative care session, a “Peer-to-peer session” and two “Get-apart sessions” (i.e., one dedicated exclusively to people with COPD or ILD and another one dedicated exclusively to their family and/or friend caregivers); and online sessions, within the 12-week period.
In “Peer-to-peer session” and “Get-apart sessions” the focus will be to discuss participants’ own issues with the multidisciplinary team but opinions about how to optimize PR for them will also be gathered. Moreover, every two weeks and for approximately 40 min, people with COPD or ILD and their family and/or friend caregivers will have the opportunity to discuss any health-related issues with a healthcare professional from the multidisciplinary team via zoom platform (i.e., online sessions). These sessions will be individualized according to participants learning needs and perspectives identified during PR. Moreover, participants that cannot attend to face-to-face sessions will have this opportunity to discuss the most relevant information to manage their disease.
Individual cases from both groups will also be referred for evaluation by a specialist palliative care team or by any other health and social care professional (e.g., psychologist or social worker) according to the specific unmet needs identified.
Education session on palliative care
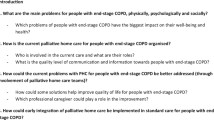
The education session on palliative care will be facilitated by two healthcare professionals, a medical doctor and a nurse, both specialized in the field. The main topics that will be discussed are presented in Table 1. A written leaflet summarizing the main information about palliative care will be given to people with COPD or ILD and their family and/or friend caregivers.
“Peer-to-peer session” and “Get-apart sessions”
People with COPD or ILD and their family and/or friend caregivers will be the primary communicators in the “Peer-to-peer session”, and the dialogue will be based on participants suggestions. This session will provide participants with an opportunity to share their knowledge, competences and experiences, listen to other people living with the same disease, and to some extent give and receive support from peers. In the week before, people with COPD or ILD will receive a total of nine cards with printed statements corresponding to the Patient Reported Experience Measure in Chronic Obstructive Pulmonary Disease (PREM-C9) [41] items. People will be asked to select one or two cards of most important personal meaning and value, and the session will be initiated talking about the statements’ themes. This strategy will capture some possible topics that people with COPD or ILD would like to discuss, prioritize content, as well as promote participant engagement.
In the “Get-apart sessions”, people with COPD or ILD will have the opportunity to discuss their issues apart from their family and/or friend caregivers and vice versa. This can be particularly helpful for people who feel more reluctant, ashamed or even stigmatized to reveal private concerns, doubts and thoughts in front of their loved ones. Both the “Peer-to-peer session” and “Get-apart sessions” will be supervised by healthcare professionals from the multidisciplinary team.
Referral of individual cases to the specialist palliative care team
Participants from both groups might be referred to the specialist palliative care team by the pulmonologist of the PR program, who has interest and basic training in the field. The decision will be taken after considering the input of all members of the multidisciplinary team and the holistic assessment of the person with COPD or ILD and the family and/or friend caregiver. Multiple aspects will be considered such as symptom severity, indicators of clinical deterioration, functional status decline and respiratory function, as well as family and/or friend caregiver’ needs [18, 22, 42]. People with COPD or ILD and family and/or friend caregivers who manifest willingness to be evaluated by a specialist palliative care team will also be referred. Participants might be referred at any time point during the intervention, and such decision (refer or not refer) will carefully be reviewed at the end of PR.
Baseline assessments
Quantitative data will be collected from all participants at baseline
The following data will be collected from people with COPD or ILD through self-report, healthcare records and direct measurements: a) sociodemographic information (i.e., age, sex, educational level, marital and employment status); b) health status [smoking status, comorbidity(ies), medication, oxygen treatment, non-invasive ventilation and exacerbation(s), hospital admission(s) and fall(s) within the last 12 months]; c) health literacy (European Health Literacy Survey in Portuguese, HLS-EU-PT) [43]; d) cognitive status (six-item cognitive impairment test, 6CIT) [44]; e) anthropometry [height and weight to calculate the body mass index (BMI)]; and f) respiratory function [residual volume (RV), total lung capacity (TLC), RV/TLC ratio, pre and post bronchodilator forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC), and diffusing capacity for carbon monoxide (DLCO)].
Family and/or friend caregivers will provide information on their: a) sociodemographics (i.e., age, sex, educational level, marital and employment status); b) health status [disease(s), limitation(s) in activities of daily living, medication and fall(s) within the last 12 months]; c) health literacy (HLS-EU-PT); d) cognitive status (6CIT); and e) role of caring [relationship with the care receiver, additional help (if any) from other co-caregiver(s), caregiver tasks and amount of time performing these tasks, length of caring, geographical distance to the care receiver house, and single vs multiple care receiver(s) at once].
Outcomes
The primary outcome will be knowledge about palliative care evaluated with the Palliative Care Knowledge Scale (PaCKS) [45]. Data will be collected at baseline (T0) and end of PR (T1). At 6-months post-PR (T2), only patient-reported outcome measures will be collected. Table 2 provides a detailed description of primary and secondary outcomes that will be assessed throughout the study period. Some outcomes, such as functional capacity, peripheral muscle strength and balance are not expected to be influenced by education, however they are important to assess the effectiveness of PR delivery.
Focus groups
Qualitative data will be collected only from the EG, at baseline and end of PR. Each focus group will last approximately 90 min and will be audio-recorded and transcribed verbatim, with field notes taken to capture participants’ nonverbal expressions. Participant’s identifying information will not be recorded on the transcripts. We will attribute fictitious names to each participant to ensure anonymity. Interview guides using open-ended questions were developed to explore: a) pre-intervention – knowledge, perceptions, experiences and perceived needs of palliative care (e.g., “What words do you associate with palliative care?”; “Can you remember the first time that you heard about palliative care?”, in affirmative cases: “Please, share your experience. When was it? What did it mean to you?”); and general opinion on integrating palliative care education in PR; and b) post-intervention – acceptability, perceived benefits, added value and impact of integrating palliative care education in PR (e.g., “When do you think is the most appropriate time for assessment by a specialist palliative care team?” and “Did the integration of palliative care education in the PR program had any impact on your physical, psychosocial and spiritual well-being?”); and suggestions for its improvement. The researcher moderating the focus groups will be responsible to get all participants to talk and fully explain their answers, remaining neutral and listening attentively with sensitivity and empathy.
Sample size calculation
The sample size was estimated for the primary outcome measure, PaCKS, in G*Power 3.1.9.4, for the time*group interaction of a mixed analysis of variance (ANOVA) with two groups (control and experimental) and two timepoints (at baseline and end of PR). We considered an α of 0.05, a power of 0.80, a correlation among repeated measures of 0.5, a nonsphericity correction of 1 and an expected effect size f of 0.25 [76]. The calculated sample size was 34 and considering a possible 40% dropout and missing data rate [77], the final sample size was determined to be 58 (29 in each group).
Statistical analysis plan
A mixed-methods approach [78] will be used to explore the effects of the intervention. First, quantitative and qualitative data will be analyzed separately, in a parallel process.
Quantitative data will be processed using IBM SPSS Statistics version 29.0 and RStudio 2022.12.0. Categorical variables will be presented as counts(percentages). Quantitative variables will be summarized using mean ± standard deviation or median[interquartile range], based on the normality of data distribution which will be explored with Shapiro–Wilk test. The EG will be compared with the CG for the primary outcome with a mixed ANOVA if assumptions are met, followed by a multiple pairwise comparison with Bonferroni correction; otherwise, an aligned rank transform-ANOVA will be performed instead. Imputation methods will be used to deal with missing data as appropriate, followed by sensitivity analyses. For all statistical analyses, a p value < 0.05 will be considered statistically significant.
Qualitative data will be processed using Web Qualitative Data Analysis (WebQDA) for inductive thematic analysis [79]. The proposed six-step procedure will be followed: 1. familiarizing with the data; 2. generating initial codes; 3. searching for themes; 4. reviewing themes; 5. defining and naming themes; and 6. producing the report [79]. Trustworthiness of the qualitative research will be ensured using the credibility, transferability, dependability, and confirmability criteria [80]. Credibility will be ensured by a) researcher triangulation i.e., each focus group will be transcribed and preliminary coded by one researcher (MAM); then, data will be independently analyzed by two researchers (MAM and AM), which will agree on themes and subthemes; and finally, all the research team (MAM, AM and DJ) will review the themes and subthemes until consensus is reached; and, b) engagement with data by all the research team. Transferability will be ensured by a comprehensive and detailed description of the research setting and participants. Dependability will be ensured by having an independent researcher that will examine, explore and challenge the processes of data collection, analysis and interpretation. Confirmability will be ensured by researcher reflexivity, peer debriefing and member checking among people with COPD or ILD and their family and/or friend caregivers.
Afterwards, we will compare quantitative and qualitative data and merge them through joint displays for integration of both methods in the final interpretation of the results.
Discussion
Living with COPD or ILD imposes enormous daily challenges, especially at advanced stages, not just to patients but also to family and/or friend caregivers. Their needs are not fully addressed by disease-modifying treatments. A key strategy to improve their well-being is the early integration of palliative care into routine management of COPD and ILD [14, 18, 22]. The current study is designed to explore the effects of palliative care education as part of PR in people with COPD or ILD and their family and/or friend caregivers.
Strengths
This study has several strengths that should be acknowledged. First, it is an innovative approach in PR dedicated to the person with COPD or ILD/caregiver dyad. Second, the education session on palliative care will be led by a medical doctor and a nurse with expertise in this field and directly involved in the session design. Third, a variety of teaching methods will be used (e.g., interactive lecturing and written material) which may enhance the capacity of learning. Fourth, the availability of an education session directed to each stakeholder is an opportunity to personalize care at an individual level and to tailor support to their distinct needs and experiences [5]. Fifth, online sessions with a flexible meeting schedule may minimize temporal and geographical barriers (e.g., work schedule and/or lack of transportation) to engage in face-to-face education and psychosocial support sessions. Sixth, the study will be described according to the most relevant guidelines [30,31,32,33], to allow its replication. Finally, a mixed-methods approach with complementary strengths of the quantitative and qualitative data will provide in-depth understanding of the effects of this intervention [78].
Limitations
This study has some limitations that should be considered. First, it is a single centre study, hence, results may not be generalized to other contexts (i.e., potentially limited external validity). Second, the heterogeneity of people with COPD or ILD can impact the main findings of the study. Nevertheless, some similarities across experiences and needs of people with different chronic respiratory diseases and their family and/or friend caregivers seem to exist. Therefore, it is likely that they will all benefit from the intervention. Third, recruiting family and/or friend caregivers, that are rarely included in PR, may be difficult. Family and/or friend caregivers are frequently active people with a multiplicity of roles often also unaware of the potential benefits of PR for the person with COPD or ILD and for the whole family. These circumstances may result in reluctance to participate in the study. However, we will use some strategies to minimize this limitation, such as explore potential barriers to participation, be flexible with online sessions and appeal to their fundamental role in disease management intervention studies. Finally, participants and the researcher conducting the intervention will not be blinded, which may influence the results.
Clinical implications
This study may be a first step towards a greater personalization of PR which integrates palliative care education to people with COPD or ILD and their family and/or friend caregivers. If successful, it will provide preliminary evidence of an innovative model that involves family and/or friend caregivers as pivotal players in daily clinical management of COPD and ILD and includes palliative care education as a core component of PR.
Availability of data and materials
Not applicable.
Abbreviations
- 1-RM:
-
One-repetition maximum
- 6CIT:
-
Six-item cognitive impairment test
- 6-MWT:
-
6-minute walking test
- BCKD:
-
Bristol COPD Knowledge Questionnaire
- BMI:
-
Body mass index
- Brief-BESTest:
-
Brief-Balance Evaluation Systems Test
- CAT:
-
COPD Assessment Test
- CG:
-
Control group
- COPD:
-
Chronic obstructive pulmonary disease
- CSNAT:
-
Carer Support Needs Assessment Tool
- DAILYs:
-
Disability-adjusted life-years
- DLCO:
-
Diffusing capacity for carbon monoxide
- EG:
-
Experimental group
- FACIT-FS:
-
Fatigue Functional Assessment of Chronic Illness Therapy-Fatigue Subscale
- FEV1 :
-
Forced expiratory volume in the first second
- FVC:
-
Forced vital capacity
- HADS:
-
Hospital Anxiety and Depression Scale
- HHD:
-
Hand-held dynamometer
- HRQoL:
-
Health-related quality of life
- ILD:
-
Interstitial lung diseases
- LCADL:
-
London Chest Activities of Daily Living
- LCQ:
-
Leicester Cough Questionnaire
- MCID:
-
Minimal clinically important difference
- mMRC:
-
Modified Medical Research Council questionnaire
- PaCKS:
-
Palliative Care Knowledge Scale
- PR:
-
Pulmonary rehabilitation
- PREM-C9:
-
Patient Reported Experience Measure in Chronic Obstructive Pulmonary Disease
- RV:
-
Residual volume
- SGRQ:
-
Saint George’s Respiratory Questionnaire
- SNAP:
-
Support Needs Approach for Patients
- TLC:
-
Total lung capacity
- VAS:
-
Visual analogue scale
- ZBI:
-
Zarit Burden Interview
References
Momtazmanesh S, Moghaddam SS, Ghamari S-H, Rad EM, Rezaei N, Shobeiri P, et al. Global burden of chronic respiratory diseases and risk factors, 1990–2019: an update from the Global Burden of Disease Study 2019. EClinicalMedicine. 2023;59:101936.
Forum of International Respiratory Societies. The global impact of respiratory disease. 3rd ed. Sheffield: European Respiratory Society; 2021.
Maddocks M, Lindell KO, Janssen DJA. Palliative care. In: Holland AE, Dal Corso S, Spruit MA, editors. Pulmonary Rehabilitation (ERS Monograph). Sheffield: European Respiratory Society; 2021. p. 132–44.
Machado A, Marques A, Burtin C. Extra-pulmonary manifestations of COPD and the role of pulmonary rehabilitation: a symptom-centered approach. Expert Rev Respir Med. 2021;15(1):131–42.
Marques A, Goldstein R. Living with chronic lung disease: the experiences and needs of patients and caregivers. In: Donner C, Ambrosino N, Goldstein R, editors. Pulmonary Rehabilitation. 2nd ed. Taylors and Francis; 2020. p. 277–90.
Sigurgeirsdottir J, Halldorsdottir S, Arnardottir RH, Gudmundsson G, Bjornsson EH. COPD patients’ experiences, self-reported needs, and needs-driven strategies to cope with self-management. Int J Chron Obstruct Pulmon Dis. 2019;14:1033–43.
Maddocks M, Lovell N, Booth S, Man WDC, Higginson IJ. Palliative care and management of troublesome symptoms for people with chronic obstructive pulmonary disease. Lancet. 2017;390(10098):988–1002.
Marx G, Nasse M, Stanze H, Boakye SO, Nauck F, Schneider N. Meaning of living with severe chronic obstructive lung disease: a qualitative study. BMJ Open. 2016;6(12): e011555.
Bryant J, Mansfield E, Boyes AW, Waller A, Sanson-Fisher R, Regan T. Involvement of informal caregivers in supporting patients with COPD: a review of intervention studies. Int J Chron Obstruct Pulmon Dis. 2016;11:1587–96.
Nakken N, van den Janssen DJ, Wouters EF, Franssen FM, Vercoulen JH, et al. Informal caregivers of patients with COPD: home Sweet Home? Eur Respir Rev. 2015;24(137):498–504.
Miravitlles M, Peña-Longobardo LM, Oliva-Moreno J, Hidalgo-Vega Á. Caregivers’ burden in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:347–56.
Cruz J, Marques A, Figueiredo D. Impacts of COPD on family carers and supportive interventions: a narrative review. Health Soc Care Community. 2017;25(1):11–25.
Grosbois JM, Gephine S, Kyheng M, Le Rouzic O, Chenivesse C. Improving the wellbeing of caregivers of patients with COPD using a home-based pulmonary rehabilitation programme. ERJ Open Res. 2022;8(4):00255.
Marques A, Cruz J, Brooks D. Interventions to support informal caregivers of people with chronic obstructive pulmonary disease: a systematic literature review. Respiration. 2021;100(12):1230–42.
Figueiredo D, Cruz J, Jácome C, Marques A. Exploring the benefits to caregivers of a family-oriented pulmonary rehabilitation program. Respir Care. 2016;61(8):1081–9.
Marques A, Gabriel R, Jácome C, Cruz J, Brooks D, Figueiredo D. Development of a family-based pulmonary rehabilitation programme: an exploratory study. Disabil Rehabil. 2015;37(15):1340–6.
Marques A, Jácome C, Cruz J, Gabriel R, Brooks D, Figueiredo D. Family-based psychosocial support and education as part of pulmonary rehabilitation in COPD: a randomized controlled trial. Chest. 2015;147(3):662–72.
Janssen DJA, Bajwah S, Boon MH, Coleman C, Currow DC, Devillers A, et al. European Respiratory Society clinical practice guideline: palliative care for people with COPD or interstitial lung disease. Eur Respir J. 2023;62(2):2202014.
Holland AE, Cox NS, Houchen-Wolloff L, Rochester CL, Garvey C, ZuWallack R, et al. Defining modern pulmonary rehabilitation. an official american thoracic society workshop report. Ann Am Thorac Soc. 2021;18(5):e12–29.
Reticker AL, Nici L, ZuWallack R. Pulmonary rehabilitation and palliative care in COPD: two sides of the same coin? Chron Respir Dis. 2012;9(2):107–16.
Palliative Care in Respiratory Disease (ERS Monograph). Claudia B, David CC, Miriam JJ, editors. Sheffield: European Respiratory Society; 2016.
Sullivan DR, Iyer AS, Enguidanos S, Cox CE, Farquhar M, Janssen DJA, et al. Palliative care early in the care continuum among patients with serious respiratory illness: an official ATS/AAHPM/HPNA/SWHPN policy statement. Am J Respir Crit Care Med. 2022;206(6):e44–69.
Machado A, Almeida S, Burtin C, Marques A. Giving voice to people - experiences during mild to moderate acute exacerbations of COPD. Chronic Obstr Pulm Dis. 2022;9(3):336–48.
Majellano EC, Clark VL, Gibson PG, Foster JM, McDonald VM. The needs and well-being of severe asthma and COPD carers: a cross-sectional study. Respirology. 2022;27(2):134–43.
Fu Y, Mason A, Boland AC, Linklater G, Dimitrova V, Doñate-Martínez A, et al. Palliative care needs and integration of palliative care support in COPD: a qualitative study. Chest. 2021;159(6):2222–32.
Kim JW, Atkins C, Wilson AM. Barriers to specialist palliative care in interstitial lung disease: a systematic review. BMJ Support Palliat Care. 2019;9(2):130–8.
Janssen DJ, McCormick JR. Palliative care and pulmonary rehabilitation. Clin Chest Med. 2014;35(2):411–21.
Spruit MA, Singh SJ, Garvey C, ZuWallack R, Nici L, Rochester C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13-64.
Grossman D, Katz A, Lock K, Caraiscos VB. A retrospective study reviewing interprofessional advance care planning group discussions in pulmonary rehabilitation: a proof-of-concept and feasibility study. J Palliat Care. 2019;36(4):219–23.
Boutron I, Altman DG, Moher D, Schulz KF, Ravaud P. CONSORT statement for randomized trials of nonpharmacologic treatments: a 2017 update and a consort extension for nonpharmacologic trial abstracts. Ann Intern Med. 2017;167(1):40–7.
Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348: g1687.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57.
O’Cathain A, Murphy E, Nicholl J. The quality of mixed methods studies in health services research. J Health Serv Res Policy. 2008;13(2):92–8.
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for prevention, diagnosis and management of COPD: 2023 report. 2023. Available from: https://goldcopd.org/2023-gold-report-2/.
Travis WD, Costabel U, Hansell DM, King TE Jr, Lynch DA, Nicholson AG, et al. An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733–48.
Smith P. Who is a carer? Experiences of family caregivers in palliative care. In: Payne S, Ellis-Hill C, editors. Chronic and terminal illness: new perspectives on caring and carers. Oxford University Press; 2001.
American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription. 11th ed. Liguori G, Yuri F, Fountaine C, Roy BA, editors. Lippincott Williams & Wilkins; 2021.
Gloeckl R, Zwick RH, Fürlinger U, Jarosch I, Schneeberger T, Leitl D, et al. Prescribing and adjusting exercise training in chronic respiratory diseases - expert-based practical recommendations. Pulmonology. 2023;29(4):306–14.
Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc. 1982;14(5):377–81.
Hill K, Jenkins SC, Cecins N, Philippe DL, Hillman DR, Eastwood PR. Estimating maximum work rate during incremental cycle ergometry testing from six-minute walk distance in patients with chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2008;89(9):1782–7.
Hodson M, Roberts CM, Andrew S, Graham L, Jones PW, Yorke J. Development and first validation of a patient-reported experience measure in chronic obstructive pulmonary disease (PREM-C9). Thorax. 2019;74(6):600–3.
Philip J, Collins A, Smallwood N, Chang YK, Mo L, Yang IA, et al. Referral criteria to palliative care for patients with respiratory disease: a systematic review. Eur Respir J. 2021;58(4):2004307.
Pedro AR, Amaral O, Escoval A. Literacia em saúde, Dos Dados à ação: tradução, validação e aplicação do European Health Literacy Survey em Portugal. Rev Port De Saúde Pública. 2016;34(3):259–75.
Katzman R, Brown T, Fuld P, Peck A, Schechter R, Schimmel H. Validation of a short orientation-memory-concentration test of cognitive impairment. Am J Psychiatry. 1983;140(6):734–9.
Kozlov E, Carpenter BD, Rodebaugh TL. Development and validation of the Palliative Care Knowledge Scale (PaCKS). Palliat Support Care. 2017;15(5):524–34.
Graul A, Haggerty A, Stickley C, Kumar P, Morales K, Bogner H, et al. Effect of patient education on palliative care knowledge and acceptability of outpatient palliative care services among gynecologic oncology patients: a randomized controlled trial. Gynecol Oncol. 2020;156(2):482–7.
Main CJ. Pain assessment in context: a state of the science review of the McGill pain questionnaire 40 years on. Pain. 2016;157(7):1387–99.
Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17(1):45–56.
Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken). 2011;63 Suppl 11:S240-252.
Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–6.
de Torres JP, Pinto-Plata V, Ingenito E, Bagley P, Gray A, Berger R, et al. Power of outcome measurements to detect clinically significant changes in pulmonary rehabilitation of patients with COPD. Chest. 2002;121(4):1092–8.
Webster K, Cella D, Yost K. The Functional Assessment of Chronic Illness Therapy (FACIT) measurement system: properties, applications, and interpretation. Health Qual Life Outcomes. 2003;1: 79.
Rebelo P, Oliveira A, Andrade L, Valente C, Marques A. Minimal clinically important differences for patient-reported outcome measures of fatigue in patients with COPD following pulmonary rehabilitation. Chest. 2020;158(2):550–61.
Birring SS, Prudon B, Carr AJ, Singh SJ, Morgan MD, Pavord ID. Development of a symptom specific health status measure for patients with chronic cough: Leicester Cough Questionnaire (LCQ). Thorax. 2003;58(4):339–43.
Rebelo P, Oliveira A, Paixão C, Valente C, Andrade L, Marques A. Minimal clinically important differences for patient-reported outcome measures of cough and sputum in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:201–12.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–70.
Puhan MA, Frey M, Büchi S, Schünemann HJ. The minimal important difference of the hospital anxiety and depression scale in patients with chronic obstructive pulmonary disease. Health Qual Life Outcomes. 2008;6: 46.
Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–54.
Kon SS, Canavan JL, Jones SE, Nolan CM, Clark AL, Dickson MJ, et al. Minimum clinically important difference for the COPD assessment test: a prospective analysis. Lancet Respir Med. 2014;2(3):195–203.
Jones PW, Quirk FH, Baveystock CM. The St George’s respiratory questionnaire. Respir Med. 1991;85(Suppl B):25–31 (discussion 3-7).
Jones PW. St. George’s respiratory questionnaire: MCID. COPD. 2005;2(1):75–9.
Support needs approach for patients. Available from: https://thesnap.org.uk/
Gardener AC, Ewing G, Farquhar M. Enabling patients with advanced chronic obstructive pulmonary disease to identify and express their support needs to health care professionals: a qualitative study to develop a tool. Palliat Med. 2019;33(6):663–75.
Carer support needs assessment tool. Available from: https://csnat.org/.
Ewing G, Grande G. Development of a Carer Support needs Assessment Tool (CSNAT) for end-of-life care practice at home: a qualitative study. Palliat Med. 2013;27(3):244–56.
Garrod R, Bestall JC, Paul EA, Wedzicha JA, Jones PW. Development and validation of a standardized measure of activity of daily living in patients with severe COPD: the London Chest Activity of Daily Living scale (LCADL). Respir Med. 2000;94(6):589–96.
Almeida Gulart A, de Araujo CLP, Bauer Munari A, Schneider BF, Dal Lago P, Mayer AF. Minimal important difference for London Chest Activity of Daily Living scale in patients with chronic obstructive pulmonary disease. Physiotherapy. 2020;107:28–35.
Holland AE, Spruit MA, Troosters T, Puhan MA, Pepin V, Saey D, et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1428–46.
Singh SJ, Puhan MA, Andrianopoulos V, Hernandes NA, Mitchell KE, Hill CJ, et al. An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1447–78.
Oliveira A, Rebelo P, Paixão C, Jácome C, Cruz J, Martins V, et al. Minimal clinically important difference for quadriceps muscle strength in people with COPD following pulmonary rehabilitation. COPD. 2021;18(1):35–44.
Andrews AW, Thomas MW, Bohannon RW. Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther. 1996;76(3):248–59.
Mathiowetz V, Weber K, Volland G, Kashman N. Reliability and validity of grip and pinch strength evaluations. J Hand Surg Am. 1984;9(2):222–6.
Padgett PK, Jacobs JV, Kasser SL. Is the BESTest at its best? A suggested brief version based on interrater reliability, validity, internal consistency, and theoretical construct. Phys Ther. 2012;92(9):1197–207.
Paixão C, Rebelo P, Oliveira A, Jácome C, Cruz J, Martins V, et al. Responsiveness and minimal clinically important difference of the Brief-BESTest in people with COPD after pulmonary rehabilitation. Phys Ther. 2021;101(11):pzab209.
Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist. 1980;20(6):649–55.
Cohen J. Statistical power analysis for the behavioural science. New York: Academic Press; 1969.
Garrod R, Marshall J, Barley E, Jones PW. Predictors of success and failure in pulmonary rehabilitation. Eur Respir J. 2006;27(4):788–94.
Creswell J, Clark V. Designing and conducting mixed methods research. 2nd ed. Sage Publications; 2011.
Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Res Psychol. 2006;3(2):77–101.
Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qualitative Methods. 2017;16(1):1609406917733847.
Acknowledgements
Not applicable.
Funding
We are grateful to Nippon Gases Portugal for funding the PhD fees of MAM and to Gasoxmed for funding this publication. No other financing was carried out.
Author information
Authors and Affiliations
Contributions
MAM, DJ and AM were responsible for study conception and design. MAM drafted the manuscript. All authors critically revised the manuscript and approved its final version to be published.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Ethical approval was obtained from the Ethics Committee for Research in Life and Health Sciences (CE-ICVS) of the Clinical Academic Center Egas Moniz Health Alliance (CAC-EMHA). Data protection will follow the European regulation (EU 2016/679). All participants will provide written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mendes, M.A., Janssen, D.J.A. & Marques, A. Integrating palliative care education in pulmonary rehabilitation: a randomized controlled study protocol. BMC Palliat Care 23, 76 (2024). https://doi.org/10.1186/s12904-024-01363-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12904-024-01363-0