
Abstract
Purpose
This study aimed to investigate the link between depression and untreated dental caries among adults in the United States.
Methods
Data were collected from the National Health and Nutrition Survey (2015–2018); respondents aged 20 years or older who completed a patient health questionnaire and underwent a comprehensive oral examination were included. Participants were categorized into three groups according to depressive symptoms as follows: those with no, mild, or moderate to severe depression. Data were weighted, and multiple potential covariates were included in the analysis to provide national estimates and account for the complex sample design. A multivariable weighted logistic regression model was performed to test the hypothesis that varying degrees of depression in American adults are associated with untreated dental caries. Subgroup analyses were performed based on age and gender after adjusting for potential covariates. A P value of <.05 was considered significant.
Results
Among 8740 participants, the prevalence of untreated coronal and root caries was 20.50% and 12.92%, respectively. Moderate to severe depression was a significant risk factor (odds ratio, 1.25; 95% confidence interval, 1.09–1.66) for untreated root caries. The risk of untreated root caries increased by 87% in young adults (aged 20–44 years) and by 46% in women with moderate to severe depression. The suest analysis revealed that the impact of moderate to severe depressive disorder on untreated root caries was non-significantly different between the age subgroup (p=0.09) and sex subgroup (p=0.51). However, depression was non-significantly associated with untreated coronal caries (mild depression: OR, 1.07; 95% CI, 0.85–1.34; moderate to severe depression 1.06; 95% CI, 0.83–1.36; respectively).
Conclusion
The results of this study suggested a significant association between moderate and severe depression and untreated root caries; however, the association with untreated coronal caries was non-significant. In the United States, moderate and severe depression in adults is associated with root caries.
Similar content being viewed by others


Introduction
Depression is a common disease in contemporary society that negatively impacts patients’ feelings, behaviors, and ways of thinking [1]. In addition, this condition is also a public health problem with a significant economic impact [2]. In 2019, the annual prevalence of a major depressive episode among US adults was 7.1% [3], and its relationship with other chronic diseases has been previously studied extensively [4,5,6].
Dental caries is also a common condition; according to statistics, more than 1 in 5 adults in the United States had untreated dental caries between 2017 and 2020 [7]. As material demands among individuals continue to rise across generations, the retention of teeth increases, leading to the anticipation of root caries emerging as a notable challenge in the field of dentistry [8]. Reports indicate that 14% of adults aged 20 and above in the United States experienced root caries between 2017 and 2020 [9]. According to research conducted in the United States, the exact prevalence of coronal and root caries was 17.9% and 10.1%, respectively [10].
In 2015, oral diseases and depression were among the top ten causes of disability worldwide [11], and an increasing number of researchers have begun to pay attention to the link between oral diseases and depression [12]. People with depression often experience symptoms of fatigue or lack of concentration [13], which can lead to an increased intake of carbohydrates and sugary foods, less brushing and flossing of the teeth, and fewer visits to the dentist. These symptoms ultimately increase the risk of dental caries [14]. Studies of associations between depression and oral health outcomes have increased over the years [15, 16]; however, few have explored the association between depressive symptoms and untreated dental caries [17]. Wiener noted in their report that the association between depressive symptoms and untreated coronal caries did not remain significant after tobacco use was added in 2017 [18]. Additionally, Aldosari also published a study in 2020 that linked depressive symptoms to mild periodontitis and a high number of missing teeth but did not explore the relationship between depressive states and untreated caries [19]. In contrast, Skokiewicz-Malinowska's findings indicated that among people 65 and older, the severity of depression increased with the number of missing teeth, number of cavities, and worsening dry mouth symptoms [20]. Lastly, Cademartori concluded in their study that the effect of dental caries on depression depends on oral health perceptions [21]. Therefore, in this study, we used a nationally representative sample to determine whether depression in American adults is associated with untreated dental caries. We hypothesized that varying degrees of depression are related to untreated root and coronal caries in adults. As no previous reports have examined the relationship between depression and untreated root and corona caries, our study fills a gap in the current literature.
Methods
Study population and design
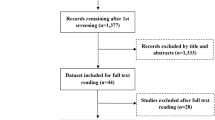
This study used the 2015–2016 and 2017–2018 National Health and Nutrition Examination Survey (NHANES) data. Conducted by the US Center for Disease Control and Prevention, the NHANES survey is a cross-sectional study of non-institutionalized civilians selected to represent the US population of all ages. The survey includes detailed demographic and health questionnaires, laboratory assays, and clinical examination measures of health outcomes. Data is collected on an annual basis and has been publicly released in two-year intervals since 1999. NHANES uses a complex multistage sampling strategy to select a representative sample of the US population. Households are randomly selected within counties and eligible individuals within each household are selected to participate in the survey, with oversampling of certain subpopulations such as minorities to ensure adequate representation [22]. The NHANES methods and data collection procedures are described in detail at www.cdc.gov/nchs/nhanes.htm [23]. The total sample size included 19,225 participants in the two pooled cycles from the 2015 to 2018 National Health and Nutrition Examination Survey. We excluded participants with an age younger than 20 years (n=7937), incomplete overall oral examination (n=1032), lack of a measure of depression (n=805), edentulous jaw (n=672), absence of root caries (n=1), lack of education level records (n=6), smoking record (n=5), dentist visits (n=22) and diabetes (n=5). Ultimately, data from 8740 adults aged 20 years or older who completed the Patient Health Questionnaire and underwent a full oral examination with at least one sound permanent or primary tooth present (excluding the third molar) were extracted and included in the data analysis. The survey protocols for this study were approved by the National Center for Health Statistics Research Ethics Review Committee, and written informed consent was obtained from all participants or their representatives for data collection and analysis.
Study variables
Outcome variable: untreated coronal and root caries
Licensed dentists performed NHANES oral health assessments following strict protocols, and data were recorded using a separate dental recorder. After rinsing the mouth, food debris was removed with 2×2-in sponges. All teeth (except the third molars) were dried with air when needed and examined using a no. A #23 dental explorer and surface-reflecting mirrors. The teeth of each participant were examined in standardized order, and the presence of untreated coronal and root caries was recorded. The diagnostic criteria for untreated coronal caries included the presence of gross cavitation; a deep pit or fissure with softness at the base or an adjacent opacity indicating undermining or demineralization; white spots or subsurface demineralization found to be soft on probing with an explorer; proximal caries diagnosed using similar criteria as for deep pits, fissures, or smooth surfaces; breaks in enamel or subsurface shadowing on proximal tooth surfaces; and loss of translucency identified via transillumination on proximal surfaces of anterior teeth only. Untreated root caries were considered present if active lesions were found on exposed root surfaces after drying including yellow or orange, tan, or light brown lesions, lesions soft on probing, or lesions with cavitation below the cementoenamel junction. The primary outcome variable was the presence of untreated coronal caries or root caries (yes or no). The prevalence of untreated coronal or root caries was defined as the percentage of participants with at least one untreated coronal or root caries. The process for acquiring the outcome variables can be found at www.cdc.gov/nchs/nhanes.
Exposure variable: depressive symptoms
The primary exposure variable was the category of depressive symptoms (none, mild, or moderate to severe). Severity was determined based on answers provided during the interview utilizing the Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 is a screening tool consisting of nine questions specifically designed to assess depression. Participants were questioned about their depressive status during the previous two weeks and asked to express how troubled they were by the situation presented. The answers were scored as “not at all” (0), “several days” (1), “more than half of the time” (2), and “nearly every day” (3). The scores for all nine questions were summed. The total score ranged from 0 to 27. A total score of 0–4 represents no depressive symptoms (reference group); a total score of 5–9 indicates mild depressive symptoms; a total score of 10 and higher indicates moderate to severe depressive symptoms. A PHQ-9 score of 10 has been recommended in the literature as the cut-off point for determining major depression [24].
Other independent variables
The following independent variables were considered as potential covariates in this analysis.
Age was a continuous variable in this study, and participant sex was categorized as male or female, while race was classified as Caucasian, Mexican American, Non-Hispanic Black, or other race. Education level was grouped as ≤ high school or more than high school. Family income level was determined using the family income-to-poverty ratio (PIR) and categorized as < 1.3, 1.3–3.5, and >3.5 [25]. Smoking status was self-reported and classified as never smoked, current smoker, or former smoker. Participants' diabetes mellitus status was self-reported and categorized as either yes or no. Filled root caries and filled coronal caries were categorized as yes or no based on history of previous restorations. The number of teeth was recorded (1–28, excluding the third molars). Recent dental visits were categorized as within the past year or more than one year. CRP levels were categorized into three levels (<1.0 mg/L; 1.0–3.0 mg/L; and > 3.0 mg/L) according to CDC/AHA recommendations [19]. Total sugar intake in the first 24-h dietary recall data was categorized by tertiles as low, middle, and high. All potential covariates were obtained directly from the dataset of NHANES.
Statistical analysis
All statistical analyses were performed using the Stata 15 Software (Stata Corp LLC, College Station, TX, USA). Associations were presented using odds ratios [OR] with 95% confidence intervals [CI], and p < 0.05 was considered significant. Survey methods were employed to analyze the intricate sampling structure of the NHANES dataset. National-level results were generated using four-year survey sample weights. Although the 2015-2016 and 2017-2018 NHANES datasets are independent, according to the formula provided by the NHANES dataset, new multi-year sample weights can be calculated by dividing the two-year sample weights by the number of two-year periods considered in the analysis. Categorical variables were assessed using chi-square tests, while continuous variables were evaluated using analysis of variance tests to examine differences between participants categorized by their depression status.
After adjusting for covariates, we constructed six logistic regression models using weighted data to explore the association between depression status and untreated dental caries. These models were divided into two groups: three for root caries (Models I, II, III) and three for coronal caries (Models IV, V, VI).
Model I was unadjusted. Model II was adjusted for age, sex, race, education, family PIR, diabetes, untreated coronal caries, filled root caries, tooth count, CRP, and sugar intake. Model III extended Model II by including smoking and dentist visits.
Model IV remained unadjusted. Model V mirrored Model II's adjustments but substituted untreated coronal caries and filled root caries with untreated root caries and filled coronal caries, respectively. Model VI extended Model V by including smoking and dentist visits.
Additionally, the same covariates were adjusted for subgroup analysis stratified by age and sex in the model III and model VI. Responses of "Refused," "Don't know," and "Missing" among the adjusted variable were combined into a single missing category. This missing category of the variable was then incorporated into the multifactorial logistic regression to ensure that its potential impact on the outcomes was considered. All ORs for the two models were reported. The seemingly unrelated estimation (suest) method was employed to assess the differences in the impact of depression across subgroups, allowing for the comparison of coefficients between subgroups by performing the adjusted Wald test to evaluate the statistical differences in the effect of depression.
Results
Baseline characteristics
Data for the 8740 participants were all taken from the NHANES database. Approximately 203 million adults were identified by weighing the samples. The average age of the study sample was 47.34 ± 0.41 years, and 48.64% of participants were men. Among the participants, 76.22% were depression-free, 16.08% had mild depression, and 7.70% had moderate to severe depression. The prevalence of untreated root and coronal caries in adults was 12.92% and 20.50%, respectively, and individuals with moderate to severe depression were more likely to be young, female, non-Hispanic Black, diabetic, and current smokers. They also have lower levels of education and income. They intake more sugar, have fewer dental caries restorations and higher CRP levels, have periodontal diseases, have more untreated dental caries, and have fewer teeth. In addition, these individuals had fewer dental visits (Table 1).
Relationship between depression and untreated root caries
The unadjusted results indicate that depressed participants had a higher risk of root caries than those without depression (Table 2). In model II, the moderate to severely depressed participants were 50% more likely to develop root caries than those without depression (OR, 1.50; 95% CI, 1.20–1.87). Even after adjusting for covariates that increased dental visits and smoking status in model III, the moderate to severely depressed participants were 25% more likely to develop root caries than those without depression (OR, 1.25; 95% CI, 1.09–1.66) (Table 2). The comparison of results between models II and III also suggested that the two covariates of dental visits and smoking status had minimal effect on our study.
Subgroup analysis for the association of depression with untreated root caries
After adjusting for all covariates, younger adults (20–44 years) with moderate to severe depression had an 87% higher risk of untreated root caries (OR, 1.87; 95% CI, 1.29–2.71) compared to those without depression. This association was not observed among middle-aged and older adults (aged ≥45). Women with moderate to severe depression had a 46% higher risk of untreated root caries (OR, 1.46; 95% CI, 1.05–2.04) compared to those without depression. This association was not observed in men.
However, the suest analysis indicated that the impact of moderate to severe depression on untreated root caries did not exhibit significant differences across age groups (p=0.09) or sex subgroups (p=0.51) (Table 3).
Association of depression with untreated coronal caries
The unadjusted results indicated that depressed participants were more likely to have untreated coronal caries than those without depression (mild depression: OR, 1.48; 95% CI, 1.25–1.76; moderate to severe depression 1.96; 95% CI, 1.54–2.49; respectively) (Table 4). After adjustment for covariates in models V and VI, the significant association between mild and moderate to severe depression and untreated coronal caries disappeared. Depressed participants were not found to have an increased likelihood of developing coronal caries compared to non-depressed participants (Table 4). Additionally, the comparison between models V and VI indicated that dental visits and smoking status, as covariates, had minimal impact on our study.
Subgroup analysis for the association of depression with untreated coronal caries
Separate subgroup analyses showed no significant association between depression and the prevalence of untreated coronal caries, regardless of age or sex (Table 5).
Discussion
Our study investigated the relationship between untreated dental caries and depression using nationally representative NHANES data. The findings indicate a link between depression and untreated root caries, highlighting a significantly higher risk of root caries among adults with moderate to severe depression. depression is non-significantly associated with untreated coronal caries.
Several studies have investigated the relationship between depression and untreated dental caries. Wiener et al found no association between categories of depressive symptoms and untreated coronal dental caries after adjusting for tobacco use and other socio-economic variables in the logistic regression model [18]. Aldosari et al discovered that the link between the severity of depressive symptoms and dental caries disappeared after accounting for confounding factors [19]. However, Guo identified a relationship between decayed, missing, filled teeth index (DMFT) and depressive symptoms in Chinese adolescents [26]. Two systematic reviews and meta-analyses suggest an association between depression and dental caries [27, 28]. Except for Wiener, no other studies have differentiated between crown caries and root caries, and there is a lack of similar studies in the literature on the association between root caries and depression. Discrepancies between our results and those in the literature may stem from variations in depression assessment methods, differences in the studied populations, or disparities in oral examination protocols and diagnoses.
Dental caries are multifactorial diseases related to the host, environment, bacteria, and time [29, 30]. Bacteria use carbohydrates in the oral environment to produce acidic products that demineralize the tooth root surface, resulting in root caries. First, depression negatively affects the patients’ feelings, thinking, and behavior. Patients with depression, especially those with moderate to severe depression, often have symptoms of malnutrition and overeating and consume large amounts of high-sugar foods[31,32,33]. Second, the oral health control of patients with depression is inadequate[34]; As the symptoms of depression worsen, people with depression need to invest more energy and economy in the treatment and care of depression, the importance of oral health gradually decreases, and the investment in oral care will also decrease. This could also explain why adults with mild depression do not have a significantly increased risk of root caries, but adults with moderate to severe depression do [35, 36]. The third possible cause is dry mouth. Depression-related physiological responses may reduce salivary production owing to sympathetic stimulation[37, 38]. However, antidepressants, which are often prescribed for long-term use, can also decrease oral saliva production, especially in those with anticholinergic effects [39, 40]. Fourth, studies have shown that depression often leads to a decrease in immunity, facilitating the reproduction of oral flora, and the central role of bacteria in the development of caries has been shown [41, 42].
However, our study found that depression does not increase the risk of untreated coronal caries. While root and coronal caries share similar risk factors, our investigation yielded contrasting results, which we attribute to subtle differences between the two types. Despite individuals with identical dentition theoretically facing equal probabilities of developing both coronal and root caries due to external and internal bodily conditions, oral hygiene plays a crucial role in caries control. The coronal area is easier to clean compared to the root area, which requires more attention. Consequently, with the same level of effort, the risk of root caries rises. As depression worsens, oral hygiene attention declines, leading to a disparity between root and coronal caries. Moreover, the rougher root surface is more prone to microbial attachment, resulting in more caries compared to the enamel on the crown surface [43, 44]. The root surface, consisting of cementum and dentin, is more susceptible to dental caries than the coronal enamel [45].
Furthermore, periodontal disease significantly links root caries and depression. Depression can exacerbate periodontal disease development as individuals with depression often exhibit negative attitudes towards life and engage in health-risk behaviors like smoking, alcohol consumption, and poor oral hygiene, known contributors to periodontal disease [16, 46, 47]. Alterations in the hypothalamic-pituitary-adrenal axis activity in depressed individuals lead to adrenal and cortisol interference, immune dysregulation, and increased secretion of pro-inflammatory cytokines such as IL-6, TNF-α, and C-reactive protein [48,49,50]. Psychological stress and cortisol level changes are suggested to heighten the risk of periodontal disease [51].
Studies have demonstrated a positive association between periodontal disease and root caries. As periodontal disease advances, gingival atrophy and increased root surface exposure in the oral cavity elevate the risk of root caries [43, 44]. Receding gums and root surface exposure to oral aerobic flora are common in periodontitis, in which the buffering effect of saliva neutralizes pH and alters the root environment, fostering the growth of cariogenic bacteria. This process may elucidate the role of periodontitis in root caries formation.
In addition, our results indicate that neither age nor sex significantly affected the correlation between depression and dental caries. Additionally, as covariates dental visits or smoking had minimal impact on our study. Studies by Dahl et al. have shown that depression can affect oral health in older adults independently of other factors, such as smoking and reduced tooth count [52], which is consistent with our findings. Other previous studies have mostly looked at the relationship between age, sex, smoking, dental visits and depression, or dental caries, but few have examined the impact of these factors on the relationship between dental caries and depression [14, 53, 54]. Therefore, further research is needed to explore the nature of this relationship.
This study had a few limitations. First, its cross-sectional design limited the ability to determine a causal relationship between depression and untreated root and coronal caries. Second, the NHANES database only shows the prevalence of root caries and excludes the number and severity of root caries, which limits further study on the association of depression with root caries. Third, depression was determined using the PHQ-9 scores; while this questionnaire is an established and validated tool for assessing depression, there are still some deviations from a true clinician’s diagnosis [55].
However, our study, which relied on the NHANES database, significantly increased the validity of the findings and extended the findings to adults across the United States. At the same time, this study is the beginning of a series aimed at exploring the direct relationship between depression and root caries. The ultimate purpose of this study was to provide a reference and theoretical basis for the clinical screening of depression. Therefore, additional studies are required to explore the association between depression and root caries. Given the findings of this study, we believe it is justified to promote integrated oral and mental healthcare services.
Conclusion
The findings of this study suggest that depression was non-significantly associated with untreated coronal caries. However, a significant association was found between moderate and severe depression and untreated root caries. These results indicate that in the United States, moderate and severe depression in adults is associated with root caries.
Availability of data and materials
NHANES data are available for public download through the website (http://wwwn.cdc.gov/nchs/nhanes/). The code files for processing this study are available from the corresponding author upon request.
Abbreviations
- NHANES:
-
National Health and Nutrition Survey
- CEJ:
-
Cementoenamel junction
- PHQ-9:
-
Patient Health Questionnaire-9
- PIR:
-
Poverty income ratio
References
Levinson DF. The genetics of depression: a review. Biol Psychiatry. 2006;60(2):84–92.
Righolt AJ, Jevdjevic M, Marcenes W, Listl S. Global-, Regional-, and Country-Level Economic Impacts of Dental Diseases in 2015. J Dent Res. 2018;97(5):501–7.
Major Depression. National Institute of Mental Health. 2019. Accessed November 28, 2019. https://www.nimh.nih.gov/health/statistics/major-depression.shtml
Olaya B, Moneta MV, Koyanagi A, Lara E, Miret M, Ayuso-Mateos JL, Chatterji S, Leonardi M, Koskinen S, Tobiasz-Adamczyk B, Lobo A, Haro JM. The joint association of depression and cognitive function with severe disability among community-dwelling older adults in Finland. Poland and Spain Exp Gerontol. 2016;76:39–45.
Rugulies R. Depression as a predictor for coronary heart disease a review and meta-analysis. Am J Prev Med. 2002;23(1):51–61.
Wulsin LR. Is depression a major risk factor for coronary disease? A systematic review of the epidemiologic evidence. Harv Rev Psychiatry. 2004;12(2):79–93.
Bashir NZ. Update on the prevalence of untreated caries in the US adult population, 2017–2020. J Am Dent Assoc. 2022;153(4):300–8. https://doi.org/10.1016/j.adaj.2021.09.004. Epub 2021 Dec 22 PMID: 34952680.
Hariyani N, Setyowati D, Spencer AJ, Luzzi L, Do LG. Root caries incidence and increment in the population - a systematic review, meta-analysis and meta-regression of longitudinal studies. J Dent. 2018;77:1–7.
Mobin T, Khan TZ, Mobin A, Tahir MR, Imran Q. The Association Between Seeking Urgent Dental Care and the Prevalence of Root Caries Among Patients in the United States, National Health And Nutrition Examination Survey 2017–2020: A Cross-Sectional Study. Cureus. 2023;15(7): e41797. https://doi.org/10.7759/cureus.41797.PMID:37575787;PMCID:PMC10421965.
Bashir NZ. Update on the prevalence of untreated caries in the US adult population, 2017–2020. J Am Dent Assoc. 2022;153:300–8.
GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015 a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545–602.
Araújo MM, Martins CC, Costa LC, Cota LO, Faria RL, Cunha FA, Costa FO. Association between depression and periodontitis: a systematic review and meta-analysis. J Clin Periodontol. 2016;43(3):216–28.
Simon GE, Von Korff M. Medical co-morbidity and validity of DSM-IV depression criteria. Psychol Med. 2006;36(1):27–36.
Anttila S, Knuuttila M, Ylöstalo P, Joukamaa M. Symptoms of depression and anxiety in relation to dental health behavior and self-perceived dental treatment need. Eur J Oral Sci. 2006;114(2):109–14.
Cademartori MG, Gastal MT, Nascimento GG, Demarco FF, Corrêa MB. Is depression associated with oral health outcomes in adults and elders? A systematic review and meta-analysis. Clin Oral Investig. 2018;22(8):2685–702.
Kisely S, Sawyer E, Siskind D, Lalloo R. The oral health of people with anxiety and depressive disorders - a systematic review and meta-analysis. J Affect Disord. 2016;200:119–32.
Fure S. Ten-year cross-sectional and incidence study of coronal and root caries and some related factors in elderly Swedish individuals. Gerodontology. 2004;21(3):130–40.
Wiener RC, Shen C, Findley PA, Dwibedi N, Sambamoorthi U. Depressive symptoms and untreated coronal dental caries among adults ages 21–64 years, NHANES 2013–2014. Community Dent Health. 2018;35(3):179–85.
Aldosari M, Helmi M, Kennedy EN, Badamia R, Odani S, Agaku I, Vardavas C. Depression, periodontitis, caries and missing teeth in the USA, NHANES 2009-2014. Fam Med Community Health. 2020;8(4):e000583.
Skośkiewicz-Malinowska K, Malicka B, Ziętek M, Kaczmarek U. Oral health condition and occurrence of depression in the elderly. Medicine (Baltimore). 2018;97(41):e12490.
Cademartori MG, Demarco FF, Freitas da Silveira M, Barros FC, Corrêa MB. Dental caries and depression in pregnant women: The role of oral health self-perception as mediator. Oral Dis. 2022;28(6):1733–40.
Chen TC, Clark J, Riddles MK, Mohadjer LK, Fakhouri THI. National Health and Nutrition Examination Survey, 2015–2018: Sample Design and Estimation Procedures. Vital Health Stat 2. 2020(184):1–35.
Johnson CL, Paulose-Ram R, Ogden CL, Carroll MD, Kruszon-Moran D, Dohrmann SM, Curtin LR. National health and nutrition examination survey: analytic guidelines, 1999-2010. Vital Health Stat 2. 2013;(161):1–24.
Manea L, Gilbody S, McMillan D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): a meta-analysis. CMAJ. 2012;184(3):E191–6.
Zhou F, Ma N, Su R, He X, Wang X, Zhou Y, Shi J. Serum 25-hydroxyvitamin D is negatively associated with severe periodontitis: a cross-sectional study. BMC Oral Health. 2021;21(1):479.
Guo P, Zou C, An N, Huang J, Yang J, Lu Q. Emotional symptoms, dietary patterns and dental caries: A cross-sectional study in adolescents. Oral Dis. 2023.
Kisely S, Sawyer E, Siskind D, et al. The oral health of people with anxiety and depressive disorders - a systematic review and metaanalysis. J Affect Disord. 2016;200:119–32.
Cademartori MG, Gastal MT, Nascimento GG, et al. Is depression associated with oral health outcomes in adults and elders? A systematic review and meta-analysis. Clin Oral Investig. 2018;22:2685–702.
Wagenknecht DR, BalHaddad AA, Gregory RL. Effects of nicotine on oral microorganisms, human tissues, and the interactions between them. Curr Oral Health Rep. 2018;5:78–87
Mandel ID. Impact of saliva on dental caries. Compend Suppl. 1989;(13):S476–81.
Bardow A, Nyvad B, Nauntofte B. Relationships between medication intake, complaints of dry mouth, salivary flow rate and composition, and the rate of tooth demineralization in situ. Arch Oral Biol. 2001;46(5):413–23.
Lewis S, Jagger RG, Treasure E. The oral health of psychiatric in-patients in South Wales. Spec Care Dentist. 2001;21(5):182–6.
Ramon T, Grinshpoon A, Zusman SP, Weizman A. Oral health and treatment needs of institutionalized chronic psychiatric patients in Israel. Eur Psychiatry. 2003;18(3):101–5.
Almohaimeed B, Dube SR, Luo R. Investigating oral health among individuals with depression: NHANES 2015-2016. Saudi Dent J. 2022;34(3):249–58. https://doi.org/10.1016/j.sdentj.2022.01.001.
Park SJ, Ko KD, Shin SI, Ha YJ, Kim GY, Kim HA. Association of oral health behaviors and status with depression: results from the Korean National Health and Nutrition Examination Survey, 2010. J Public Health Dent. 2014;74(2):127–38.
Dahl KE, Calogiuri G, Jönsson B. Perceived oral health and its association with symptoms of psychological distress, oral status and socio-demographic characteristics among elderly in Norway. BMC Oral Health 2018;18:93.
Boyapati L, Wang HL. The role of stress in periodontal disease and wound healing. Periodontol 2000 2007;44:195–210.
Hugo FN, Hilgert JB, Corso S, Padilha DM, Bozzetti MC, Bandeira DR, Pawlowski J, Gonçalves TR. Association of chronic stress, depression symptoms and cortisol with low saliva flow in a sample of south-Brazilians aged 50 years and older. Gerodontology. 2008;25(1):18–25.
Ciancio SG. Medications' impact on oral health. J Am Dent Assoc. 2004;135(10):1440-8; quiz 1468-9.
Anttila SS, Knuuttila ML, Sakki TK. Depressive symptoms favor abundant growth of salivary lactobacilli. Psychosom Med. 1999;61:508–12.
Engeland CG, Hugo FN, Hilgert JB, Nascimento GG, Junges R, Lim HJ, Marucha PT, Bosch JA. Psychological distress and salivary secretory immunity. Brain Behav Immun. 2016;52:11–17.
Sanz M, Beighton D, Curtis MA, Cury JA, Dige I, Dommisch H, Ellwood R, Giacaman RA, Herrera D, Herzberg MC, Könönen E, Marsh PD, Meyle J, Mira A, Molina A, Mombelli A, Quirynen M, Reynolds EC, Shapira L, Zaura E. Role of microbial biofilms in the maintenance of oral health and in the development of dental caries and periodontal diseases. Consensus report of group 1 of the Joint EFP/ORCA workshop on the boundaries between caries and periodontal disease. J Clin Periodontol. 2017;44 Suppl 18:S5–11.
López R, Smith PC, Göstemeyer G, Schwendicke F. Ageing, dental caries and periodontal diseases. J Clin Periodontol. 2017;44 Suppl 18:S145–52.
Saotome Y, Tada A, Hanada N, Yoshihara A, Uematsu H, Miyazaki H, Senpuku H. Relationship of cariogenic bacteria levels with periodontal status and root surface caries in elderly Japanese. Gerodontology. 2006;23(4):219–25.
AlQranei MS, Balhaddad AA, Melo MAS. The burden of root caries: Updated perspectives and advances on management strategies. Gerodontology. 2021;38(2):136–53.
Genco RJ, Ho AW, Grossi SG, Dunford RG, Tedesco LA. Relationship of stress, distress and inadequate coping behaviors to periodontal disease. J Periodontol. 1999;70(7):711–23.
Okoro CA, Strine TW, Eke PI, Dhingra SS, Balluz LS. The association between depression and anxiety and use of oral health services and tooth loss. Community Dent Oral Epidemiol. 2012;40(2):134–44.
Dumitrescu AL. Depression and Inflammatory Periodontal Disease Considerations-An Interdisciplinary Approach. Front Psychol. 2016;7:347.
Belvederi Murri M, Pariante C, Mondelli V, Masotti M, Atti AR, Mellacqua Z, Antonioli M, Ghio L, Menchetti M, Zanetidou S, Innamorati M, Amore M. HPA axis and aging in depression: systematic review and meta-analysis. Psychoneuroendocrinology. 2014;41:46–62.
Köhler CA, Freitas TH, Maes M, de Andrade NQ, Liu CS, Fernandes BS, Stubbs B, Solmi M, Veronese N, Herrmann N, Raison CL, Miller BJ, Lanctôt KL, Carvalho AF. Peripheral cytokine and chemokine alterations in depression: a meta-analysis of 82 studies. Acta Psychiatr Scand. 2017;135(5):373–87.
Castro MML, Ferreira RO, Fagundes NCF, Almeida APCPSC, Maia LC, Lima RR. Association between Psychological Stress and Periodontitis: A Systematic Review. Eur J Dent. 2020;14(1):171–9.
Dahl KE, Calogiuri G, Jönsson B. Perceived oral health and its association with symptoms of psychological distress, oral status and socio-demographic characteristics among elderly in Norway. BMC Oral Health 2018;18(1):93.
Wu Z, Yue Q, Zhao Z, Wen J, Tang L. A cross-sectional study of smoking and depression among US adults: NHANES (2005-2018). Front Public Health. 2003;30(11).
Jönsson B, Holde GE, Baker SR. The role of psychosocial factors and treatment need in dental service use and oral health among adults in Norway. Community Dent Oral Epidemiol. 2020;48(3):215–24
Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Annals. 2002;32(9):509–15.
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing.
Funding
None.
Author information
Authors and Affiliations
Contributions
ZFX and LFS contributed to data processing, analysis, and manuscript writing. LBH contributed to the study design and manuscript writing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
NHANES protocol approved by NCHS Research Ethics Review Board, and obtained informed consent from all participants. The survey protocols for this study were approved by the National Center for Health Statistics Research Ethics Review Committee, and written informed consent was obtained from all participants or their representatives for data collection and analysis.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xie, Z., Shi, L. & He, L. Depression and dental caries in US adults, NHANES 2015–2018. BMC Oral Health 24, 520 (2024). https://doi.org/10.1186/s12903-024-04288-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-024-04288-5