
Abstract
Background
The oral cavity is home to various ecological niches, each with its own unique microbial composition. Understanding the microbial communities and gene composition in different ecological niches within the oral cavity of oral cancer (OC) patients is crucial for determining how these microbial populations contribute to disease progression.
Methods
In this study, saliva and dental plaque samples were collected from patients with OC. Metagenomic sequencing was employed to analyze the microbial community classification and functional composition of the different sample groups.
Results
The results of the study revealed significant differences in both the function and classification of microbial communities between saliva and dental plaque samples. The diversity of microbial species in saliva was found to be higher compared to that in plaque samples. Notably, Actinobacteria were enriched in the dental plaque of OC patients. Furthermore, the study identified several inter-group differential marker species, including Prevotella intermedia, Haemophilus parahaemolyticus, Actinomyces radius, Corynebacterium matruchitii, and Veillonella atypica. Additionally, 1,353 differential genes were annotated into 23 functional pathways. Interestingly, a significant correlation was observed between differentially labeled species and Herpes simplex virus 1 (HSV-1) infection, which may be related to the occurrence and development of cancer.
Conclusions
Significant differences in the microbial and genetic composition of saliva and dental plaque samples were observed in OC patients. Furthermore, pathogenic bacteria associated with oral diseases were predominantly enriched in saliva. The identification of inter-group differential biomarkers and pathways provide insights into the relationship between oral microbiota and the occurrence and development of OC.
Similar content being viewed by others


Introduction
The oral cavity serves as the initial stage of the human digestive system, where daily feeding actions gradually establish a diverse ecosystem of up to 1,000 total microbial species that can have either positive, negative, or digestive-supporting effects on humans [1]. Over time, researchers have reported Streptococcus species as dominant in a diverse and balanced community of key bacterial species found in a healthy oral microbiota, which include Lactobacillus, Actinomyces, Veillonella, Haemophilus, and Neisseria that makes up to 85.4% of all adults’ genera and 71.1% of youth genera in their respective samples [2]. This diverse ecosystem of oral microbiota plays a crucial role through functional pathways in maintaining oral health, preventing dental diseases, promoting proper digestion and nutrient absorption [3]. Although, factors such as poor oral hygiene practice, unhealthy diet and genetic disorders can result to development of oral disease [4].
OC is the predominant type among the Head and Neck cancer, ranking as the sixteenth most common cancer globally [5, 6]. Research has shown a close association between the oral microbiota and tumor development [7]. This oral microbiota normally resides in both saliva and surface areas of the oral cavity as planktonic bacteria and dental plaque respectively [8]. Dental plaque is a structured microbial biofilm, and the organic acids produced by the sugar metabolism of dental plaque biofilm play a crucial role in lowering the pH of the tooth surface and demineralization [9]. Poor dietary habits such as frequent consumption of sugar can induce dysbiosis of the microbial community on the gum, leading to the development of dental caries [10]. The oral diseases caused by dysbiosis in the oral microbiota (such as periodontitis) are associated with various systemic disorders [11]. Oral bacteria and their metabolic products enter the bloodstream, increasing oral and systemic inflammation through the release of toxins or microbial by-products [12, 13]. Much research has reported the associated risk of periodontal disease and systemic diseases such as cardiovascular disease, diabetes, respiratory infections, and adverse pregnancy outcomes, with a 19% increased risk in cardiovascular diseases and an elevated risk of gaining the critical COVID-19 infection [14, 15]. AlsoMoreover, the dysbiosis of the oral microbiota can be used to potentially predict the risk of cancer, and colonization by specific microbiota might be important for the development of OC and related diseases [16]. The host’s immune response to certain oral bacteria and their byproducts can trigger chronic inflammation, which subsequently results in development and progression of oral cancer [17].
Exploring the microbial changes that occur during oral carcinogenesis is crucial in identifying diagnostic and prognostic biomarkers for early detection and monitoring of oral cancer [18]. Investigating oral microbiota functional pathways in oral cancer patients can reveal disease mechanisms and intricate interactions between microbial species, host cells, and the immune system [19]. Furthermore, conducting longitudinal studies would provide researchers with the opportunity to assess dynamic changes that may occur over time and potentially identify precise therapeutic agents for the treatment of OC. With the advent of metagenomic sequencing technology and a deeper understanding of bacterial communities, the relationship between the dysbiosis of the human microbiota and the pathogenesis of various diseases is gradually becoming clearer [20]. However, the oral cavity harbors numerous ecological niches, each with its own unique microbial community, with a lack of exploration into the utilization of metagenomic sequencing technology to analyze the oral microbiota [21]. The characteristics and differences in the composition and functional features of the saliva and dental plaque microbiomes in oral cancer patients remain unknown. Additionally, there remains a limited understanding of the comprehensive mechanisms underlying the development of oral cancer, and it continues globally to have a high incidence rate and low survival rate among its patients [22].
In this study, we compared the differences in the oral microbiota and genomic composition of saliva and dental plaque between OC patients, identifying a set of potential differential markers and genes. The relationship between microorganisms and functional pathways was revealed through functional enrichment and correlation analysis, which was expected to provide further understanding of the relationship between microorganisms and the occurrence and development of OC. This comparative study could further improve our understanding of the pathogenesis of OC and propose potential therapeutic targets for treating or improving the quality of life for patients with OC.
Materials and methods
Subject recruitment and sample collection
To investigate the microbial and functional genetic features in OC patients, a total of 5 saliva samples and 5 dental plaque samples were collected from patients with OC at Hunan Cancer Hospital. All participants providing samples informed consent and had complete clinical and pathological data. To minimize potential confounding factors, the inclusion criteria for participants were as follows: (1) No other malignant tumors were detected during systemic examination, excluding distant metastasis. (2) Avoidance of smoking, alcohol consumption, and eating for at least 30 minutes prior to sample collection. (3) No immunosuppressive medication within the past 6 months. (4) No history of severe periodontal disease, severe dental caries, or oral mucosal diseases in the past 3 months; no other systemic diseases; no history of oral surgery; and no history of antibiotic use. (5) Patients without a history of oral infectious diseases or bleeding. In accordance with the Helsinki Declaration, the cases included in this study were collected and approved by the ethics committee of Hunan Cancer Hospital (Ethics Approval Number: KYJJ-2023-025). Patients were informed about the sample collection procedures and signed informed consent forms.
Before collecting the samples, the participants were instructed to rinse their mouths with distilled water to remove any residual food debris. The swab was gently rubbed back and forth three times on the upper and lower incisors, first molars, and first bicuspid. It was then placed in a sterile collection tube. 1 ml of sterile PBS buffer was added to a sterile collection tube, ensuring that the swab was fully immersed in the elution buffer to allow for complete dissolution of the sample. Subsequently, the sample tube was centrifuged at 12,000 rpm for 10 minutes at 21 ℃ (Glanlab, Changsha, China). This step was repeated three times to collect the eluted buffer. Saliva was collected in a sterile tube with a minimum volume of 1 ml.
DNA extraction and metagenomic sequencing
All samples were accessed for metagenomic sequencing. Total microbial genomic DNA was extracted using the QIAGEN DNeasy Power Water Kit (14900-100-NF). The microbial DNA that was extracted underwent processing to create metagenomic sequencing libraries with 400 bp insert sizes, utilizing the Illumina TruSeq Nano DNA LT Library Preparation Kit. Subsequently, each library underwent sequencing on the Illumina HiSeq X-ten platform (Illumina, USA), employing the PE150 strategy. Potential 3' end adapter sequences were identified, and the sequence was truncated at the identified adapter sequence (R1: AGATCGGAAGAGCACACGTCTGAACTCCAGTCA; R2: AGATCGGAAGAGCGTCGTGTAGGGAAAGAGTGT).
Data processing
The raw sequencing data contained various issues, such as short sequences, excessive ambiguous bases, and contamination from adapters. To ensure data accuracy, we performed further quality control on the raw sequences, primarily to remove contamination and human host sequences. Initially, we utilized Fastp (version 0.23.2) to eliminate low-quality reads, specifically those with an average quality score < 15 and a length less than 15 bases [23]. FastUniq (version 1.1.0) was utilized as a tool to remove duplicate sequences, processing PCR duplicates, or redundant sequences caused by PCR amplification in DNA sequencing data [24]. We employed Bowtie2 (version 2.5.1) to align the sequences against the human genome database (hg38) and filter out sequences of human origin [25]. Initially, species annotation on the gene sequences was performed using Kraken2 (version 2.1.2), resulting in taxids (unique identifiers for NCBI taxonomic units) being obtained for every gene [26]. Following that, the names and taxonomy of these taxids were translated into corresponding species information, ranging from phylum to species. Then, the high-quality reads were reconstructed from the quality-controlled data using MEGAHIT (version 1.2.9) [27]. Following the assembly, gene prediction was performed on the MEGAHIT assembly contigs using Prodigal (version 2.6.3) [28]. EggNOG-mapper (version 2.0.1) was used to perform the function annotation for the gene catalog [29]. Subsequently, clustering and redundancy removal of the gene sequences were carried out using CD-HIT (version 4.7) with a 90% global sequence similarity threshold [30]. The relative abundance of differential genes was then estimated using salmon (version 0.13.1) [31].
Statistical analysis and visualization
The data analysis and visualization in this study were performed using R (v.4.2.3). Based on the Spearman correlation matrix, two co-occurrence networks were constructed. The False Discovery Rate (FDR) correction by the Benjamini-Hochberg (BH) method was applied to correct for multiple hypothesis testing. The Spearman correlation coefficient was found to be 0.8, and the adjusted P-value was 0.05. Subsequently, the co-occurrence networks were visualized using Gephi software (v.0.9.5) [32]. The visualization of microbial community composition was conducted using the ggbarplot function from the ggpubr package (v.0.6.0). The Wilcoxon test was utilized to compare the relative abundance differences of different species between groups, and the ggboxplot was utilized for visualization. A p-value less than 0.05 was considered statistically significant. Alpha diversity was calculated based on species abundance using the diversity function from the vegan package (v.2.6-4) [33]. To describe the degree of similarity among various microbial communities within various groups, beta diversity was employed. In this work, the diversity index of the microbiota in saliva and dental plaque samples was determined using the “vegdist” function, which is based on the Bray-Curtis distance. The sample groups were subjected to PCoA analysis using the PERMANOVA method, with 999 permutations used for statistical significance testing. ANOSIM was used to test the significance of differences between two groups [34]. Non-metric multidimensional scaling (NMDS) was conducted using the metaMDS function from the vegan package for ordination analysis [35]. The volcano plot was generated using the DEseq2 package, with labeling of species and genes that met the criteria of |log2FoldChange| > 2 and P < 0.05 [36]. To show the link between genes in various samples, the Pearson correlation coefficient was employed. Better biological repeatability was suggested by a correlation coefficient near 1, which showed a closer biological link between the genes in the samples [37]. Similarly, the Pearman correlation coefficient was also employed to assess the correlation between different microbial species and genes [38]. A T-test was employed to calculate the abundance differences in functional pathways between groups.
Result
Characteristics of microbial community composition in saliva and dental plaque
To investigate the microbial composition of saliva and dental plaque, a total of 6,234 ASVs (Amplicon Sequence Variant) were extracted from all the samples. Dental plaque and saliva shared 4,919 ASVs, while dental plaque had 328 unique ASVs and saliva had 926 unique ASVs. At the species level, a total of 4,947 species were detected, of which 3,996 species were shared by both sample groups (Fig. 1A). A network diagram was used to visualize the overall community characteristics of dental plaque and saliva microbiota (Fig. 1B). There were differences in the microbial network structure between dental plaque and saliva. The modularization coefficient, which reflects the degree of modularity in the microbial network, was higher in dental plaque (0.641) compared to saliva (0.367). At the phylum level, Actinobacteria was significantly enriched in dental plaque (P < 0.01) (Supplementary Figure S1), whereas Proteobacteria, Firmicutes, and Bacteroidetes showed a higher relative abundance in saliva compared to dental plaque (Fig. 1E). At the genus level, Rothia, Actinomyces, and Corynebacterium were predominantly enriched in dental plaque, while Prevotella, Streptococcus, Neisseria, and Veillonella exhibited a higher relative abundance in saliva (Fig. 1C, D). Additionally, a greater diversity of low-abundance bacteria (other bacteria) was found in saliva, and we also observed a higher relative abundance of Porphyromonas gingivalis in saliva (Supplementary Figure S2).

Composition of microbiota in saliva and dental plaque samples. (A) The Venn plot shows the overlap and differences between the microbiota of dental plaque and salivaa. The blue area represents saliva samples, and the yellow area represents dental plaque samples. (B) Microbial network composition of dental plaque and saliva, with different colored points denoting different species and each species' contribution indicated by the size of the point. (C) Relative abundance of species composition at the genus level in the two groups, with lines connecting samples from saliva (blue) and dental plaque (yellow). (D) Wilcoxon test, indicating significance levels for Actinomyces, Corynebacterium, and Prevotella (* P < 0.05, ** P < 0.01). E Relative abundance of species composition at the phylum level
Analysis of microbial community diversity and species differences
The Shannon-Weaver, Gini-Simpson, Chao1, ACE, Richness, and Pieou indices were calculated at the species level (Fig. 2A). The results showed the six indices for saliva microbiota were significantly higher than those for dental plaque. It demonstrated that the species richness and diversity of microbial communities in the saliva of OC patients were significantly higher than those in dental plaque. The PCoA analysis indicated that the microbial community composition of the two groups was different (Fig. 2B). The ANOSIM test (R = 0.748, P = 0.012) further demonstrated that the inter-group differences in microbial composition were significantly greater than the intra-group differences (Supplementary Figure S3). The composition of the microbial community was effectively simulated by the NMDS analysis (Supplementary Figure S4). The NMDS analysis result revealed that samples in the two groups had different community compositions (Stress = 0.092) (Fig. 2B). Then, a batch of differential marker species was chosen from the top 100 species based on their relative abundance (P < 0.05, |log2FoldChange| > 2). Prevotella spp., Haemophilus spp., Actinomyces spp., Corynebacterium matruchotii, and Veillonella atypica were identified as differential species between the two groups. Prevotella spp. and Haemophilus spp. were significantly enriched in saliva, while Actinomyces spp. and Corynebacterium matruchotii were significantly enriched in dental plaque (Fig. 2C).

The microbial diversity and differential abundance analysis of microbial communities. (A) Alpha diversity was described using Shannon-weaver, Gini-Simpson, ACE, Chao, Richness, Pielou indices. (B) Beta diversity was presented by PCoA (ANOSIM, R = 0.748, P = 0.012) and NMDS analysis (Stress = 0.092). (C) Significant analysis of differential species by DEseq2 at the genus level (|log2 Fold Change| > 2, P < 0.05)
Screening of differential gene and correlation analysis between species and functional pathways
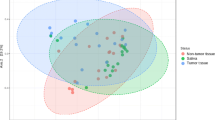
From the perspective of gene composition, the gene results from metagenomic sequencing were transformed into a two-dimensional coordinate system using NMDS analysis. The genomic composition of the two groups differed significantly, as seen by the distinct confidence ellipses of the saliva and dental plaque samples (P < 0.05) (Fig. 3A). To further explore the similarity of samples, the Pearson correlation coefficients for gene correlations between different samples were calculated. It was evident from the heatmap that samples within the same group exhibit higher Pearson coefficients, indicating greater genetic similarity within the sample groups and closer microbial relatedness (Fig. 3B). Through T-test analysis, a total of 23 functional gene pathways with significant differences were identified in both saliva and dental plaque samples, including Carbohydrate metabolism, Amino acid metabolism, and Metabolism of cofactors and vitamins (P < 0.05) (Fig. 3C). The relative abundance of 1,353 genes showed significant differences between saliva and dental plaque samples (P < 0.05, |log2FoldChange| > 2). Using dental plaque samples as the control, 735 genes were significantly elevated in saliva samples, whereas 618 were significantly downregulated (Fig. 3D).

Gene composition and functional annotation of saliva and dental plaque in cancer patients. (A) PCoA analysis (80% confidence interval). (B) Correlation test between samples at the genetic composition level. The distance between points in a scatter plot represents the correlation between two genes. (C) Analysis of inter group differences in functional pathways with the top 50 abundances at level 2 of the KEGG database (T-test, P < 0.05). The color of the bars represents different groups, and the length of the bars represents abundance information. (D) Volcano plot showing the relative abundance differences of genes, where red points indicate significantly higher relative abundance of the gene in the saliva group (P < 0.05, log2FoldChange > 2). Blue points indicate significantly lower relative abundance in the saliva group (P < 0.05, log2FoldChange < -2), and grey points indicate no significant difference
Furthermore, based on the gene abundance ranking, we identified a total of 14 differential genes among the top 50 ranked genes in abundance. A bubble plot was generated to illustrate the abundance levels of the genes across different samples, with K18955 enriched in dental plaque samples and the remaining 13 genes enriched in saliva samples (Fig. 4A). According to functional annotation, the K18955 gene enriched in dental plaque was involved in the pathway of transcription factors [BR: ko03000], which involved multiple transcription factors participating in the process of gene transcriptional regulation. Among the top ten genes in abundance, five genes (K09228, K00341, K09229, K12855, and K18955) showed significant differences in abundance between the two groups. Especially, K09228 and K00341 were genes with the highest relative abundance across all samples. Based on functional annotations, the K09228 gene was primarily involved in the functional pathways of transcription factors [BR: ko03000] and Herpes simplex virus 1 infection [PATH: ko05168]. The K00341 gene was mainly associated with the pathway of oxidative phosphorylation [PATH: ko00190]. Next, Pearson correlation analysis was performed between the top 5 differentially abundant genes and the top 5 phylum-level species based on relative abundance ranking (Fig. 4B). A strong inverse relationship (P < 0.01) between Actinobacteria and oxidative phosphorylation [PATH: ko00190] was revealed. This implied that these two factors could be in mutual competition or inhibited under certain circumstances, suggesting that Actinobacteria growth and survival may be impacted by oxidative phosphorylation-related metabolic processes. Moreover, based on the relative abundance ranking, the top 50 genes and species with significant differences in relative abundance between groups were selected for correlation analysis (P < 0.05, |log2 Fold Change| > 2) (Fig. 4C). Oxidative phosphorylation exhibited a significant negative correlation with species mainly belonging to Actinomyces, and a significant positive correlation with species such as Haemophilus parahaemolyticus, Tannerella forsythia, Porphyromonas gingivalis, and Prevotella intermedia. A significant positive correlation between Haemophilus parahaemolyticus, Prevotella denticola, Prevotella intermedia, Porphyromonas gingivalis, Tannerella forsythia, and HSV-1 infection was also observed. Furthermore, Prevotella intermedia mostly affected genes K01872, K03406, K12855, and K18955, whereas Porphyromonas gingivalis considerably affected the pathways ko02035, ko02020, ko02030, and ko03000.

Correlation analysis between differential genes and species. (A) Bubble plot (left): composition of the abundance of the top 14 differential genes among different groups. Rows represent differential genes, and each column represents a different sample. Sankey diagram (right): proteins associated with the top 14 differential genes and their corresponding functional pathways. (B) Correlation analysis between the top 5 differential genes and the top 5 species at the phylum level based on relative abundance. (C) Correlation analysis between the top 14 differential genes and the top 26 differentially abundant species. The size of the circular dots is used to indicate the magnitude of the correlation coefficient, while the color represents the sign of the correlation coefficient. A separate square color block is added to indicate the p-value of the correlation test
Discussion
The study discovered that the genomic composition, microbial community composition, alpha diversity, beta diversity, and ecological networks of saliva and dental plaque in OC patients were altered. Genes and microorganisms that showed differences were chosen for correlation analysis. Saliva had a greater variety of microorganisms than dental plaque, including a greater number of low-abundance microorganisms and a microbial network with less modularity. Differential marker candidates were found. The genomic composition was screened for 1,353 differential genes, and the relationship between differential microorganisms and genes was investigated. Most microorganisms and functional pathways exhibited significant correlations.
Our study revealed significant differences in the microbial composition of saliva and dental plaque between cancer patients. The site-specific hypothesis proposed that the microbial communities in different oral sites vary in composition and proportion, and the microbial composition also varies among different ecological niches [39]. The microbes in the saliva were dominated by the Streptococcus, Prevotella, and Veillonella genera, which comprise 70% of this microbiota [8]. Their transient and free-floating nature classifies them as planktonic bacteria with a unique ability to interact with and influence various factors, such as oral hygiene. Although, attached bacteria species such as Streptococcus mutans, Porphyromonas gingivalis, Prevotella intermedia, Fusobacterium nucleatum, and Actinomyces formed the dental plaque through a process of pellicle formation, bacterial adhesion, colonization, matrix formation, and maturation, forming dental plaque to develop synergistic or antagonistic relationships that could influence oral health or contribute to the development of oral diseases [2].
Based on our results, the relative abundance of Prevotella, Porphyromonas gingivalis, and Streptococcus was also found to be more enriched in saliva. Previous studies have shown that Prevotella is frequently present in oral tumor tissues [40, 41]. Prevotella intermedia and Porphyromonas gingivalis were associated with the occurrence and development of cancer [42]. According to reports, it was because the proteases they secrete can degrade host tissues such as the extracellular matrix (ECM), modulate host immune responses, and participate in cell proliferation and apoptosis [43, 44]. Pathogenic bacteria like Porphyromonas gingivalis and Fusobacterium nucleatum in the oral cavity can upregulate inflammatory mediators and facilitate invasion and spreading to adjacent cells, promoting chronic inflammation. This chronic inflammation can lead to changes in cell metabolism, proliferation, and the development of tumors [45]. Genetically, Lactobacilli and Streptococci species produce reactive oxygen species, nitrogen reactive species, sulfides, nitrosamines, and acetaldehydes that can lead to DNA damage in epithelial cells and thus promote tumorigenesis [46, 47]. Hypomethylation of interleukin-6 and interleukin-8 gene promoters has been linked to overexpression of these cytokines in inflamed periodontal disease tissues compared to control tissues. Consequently, the release of proinflammatory mediators can stimulate human gingival epithelial cells, leading to the recruitment and activation of inflammatory cells, potentially facilitating oral malignant transformation [48].
Additionally, the diversity and abundance of species in saliva exceeded those in dental plaque. On one hand, the fluid nature of saliva allows it to collect and carry microbial communities from different oral sites, such as the tongue coating and buccal mucosa. It can lead to a higher diversity of microorganisms in saliva, as it may be influenced by other parts of the oral cavity. However, it is important to note that many microorganisms in saliva do not exhibit high abundance [49]. On the other hand, due to the lubricating, protective, and digestive functions of saliva within the oral environment, various microorganisms may have a broader distribution and survival in the oral cavity through saliva. In contrast, dental plaque is a biofilm that adheres to the tooth surface, and its relatively enclosed environment may result in a relatively lower diversity and abundance of microorganisms [50]. A microbial comparative study of periodontitis and a healthy group in terms of alpha diversity reported much more substantial differences in bacterial diversity than the supra-gingival plaque in a saliva sample [51]. The more diverse and abundant microbial community in the saliva are implicated in periodontal diseases with Porphyromonas gingivalis, Tannerella forsythia, and Fusobacterium alocis as causative agents. These causative agents have proven to be moderately accurate at distinguishing the severity of periodontal disease in a full mouth probe [52].
In our research findings, the saliva microbiota of OC patients exhibited a dysbiotic state, characterized by an increased abundance of Neisseria, Prevotella, Haemophilus, Corynebacterium, Streptococcus, Capnocytophaga, and Porphyromonas. Numerous studies have indicated a close correlation between the increased abundance of these bacteria and the occurrence and progression of cancer, but the specific mechanisms underlying this relationship require further investigation [53, 54]. Another study of the salivary microbiota reported Streptococcus dominance with approximately 25 and 50% of all DNA and RNA reads respectively. Also, a significant disease-associated higher relative abundance of periodontal pathogens such as Porphyromonas gingivalis and Filifactor alocis was found using both metagenomic and metatranscriptomic analysis [55]. Further comparison of the microbiota in dental plaque and saliva of OC patients revealed that Actinomyces was highly enriched in dental plaque. A previous study indicated that Actinomyces, as a key microorganism, contributes to the formation of oral biofilms, dental plaque, halitosis, and dental caries by inducing acid and gas production on the tooth surface [56]. However, current studies on the pathogenesis of OC are still very limited, and the relationship between microorganisms and cancer occurrence and development cannot be ignored [22].
Various factors, such as bacteria, viruses, diet, radiation, and genetic mutations, can all contribute to the development of OTSCC [57]. In our study, significant positive correlations were observed between bacteria such as Porphyromonas gingivalis, Haemophilus parahaemolyticus, Prevotella intermedia, and HSV-1 infection. The presence of these bacteria alongside HSV-1 infection may indicate a microbial community that could collectively influence the oral environment and potentially contribute to the development or progression of OC. Further research is needed to explore the mechanisms underlying these correlations and their implications for oral health management and disease prevention strategies. Previous studies have linked oral tongue squamous cell carcinoma (OTSCC) to HSV-1, which may interfere with the cell cycle, activate cell proliferation pathways, and inhibit immune responses, potentially contributing to OC [58]. Furthermore, HSV-1 infection may increase OC risk through interaction with other carcinogenic factors. HSV-1 is believed to act in conjunction with other carcinogens, enhancing tumorigenic effects in the development of oral squamous cell carcinoma (OSCC) [59]. Previous studies detected HSV DNA in 15% to 56% of oral cancer patients [60, 61]. These findings underscore the potential role of HSV-1 in the development of oral cancer and highlight the importance of further research in this area.
This small-scale study aimed to elucidate the differences in saliva and dental plaque microbiota and genomic composition in OC patients. However, the study has certain limitations. Firstly, the sample collection was limited to saliva and dental plaque samples from OC patients, with a relatively small sample size and a lack of data from a control group of healthy individuals. Secondly, while the study observed a significant correlation between oral microbiota and HSV-1 infection, the specific mechanisms underlying this correlation remain unclear. Lastly, the precise role of the microbiota in the pathogenesis of OC is still not well understood.
Conclusion and future perspectives
Our study found that OC patients exhibit significant differences in microbial composition, gene composition, and function between saliva and dental plaque. OC patients had higher diversity and richness of saliva microbiota, as well as a higher relative abundance of bacteria associated with oral diseases. We also analyzed the close relationship between microorganisms and functional pathways, which may be related to the development of OC. In future, we need to further explore the mechanism of microbial impact on OC through a combination of multidisciplinary and multi omics approaches. This is essential for the early detection and monitoring of diagnostic and prognostic biomarkers, as well as understanding disease mechanisms and complex interactions between microorganisms, host cells, and the immune system.
Availability of data and materials
The raw sequence data reported in this paper have been deposited in the Genome Sequence Archive [62] in National Genomics Data Center [63], China National Center for Bioinformation / Beijing Institute of Genomics, Chinese Academy of Sciences (GSA: CRA013876) that are publicly accessible at https://ngdc.cncb.ac.cn/gsa.
Abbreviations
- OC:
-
Oral cancer
- ASV:
-
Amplicon Sequence Variant
- PCoA:
-
Principal co-ordinates analysis
- ANOSIM:
-
Analysis of similarities
- NMDS:
-
Non-metric multidimensional scaling
- PERMANOVA:
-
Permutational multivariate analysis of variance
- HSV-1:
-
Herpes simplex virus 1
- ECM:
-
Extracellular matrix
- OTSCC:
-
Oral tongue squamous cell carcinoma
- OSCC:
-
Oral squamous cell carcinoma
References
Radaic A, Kapila YL. The oralome and its dysbiosis: new insights into oral microbiome-host interactions. Comput Struct Biotechnol J. 2021;19:1335–60.
Li X, Liu Y, Yang X, et al. The oral microbiota: community composition, influencing factors, pathogenesis, and interventions. Front Microbiol. 2022;13:895537.
Sedghi L, DiMassa V, Harrington A, et al. The oral microbiome: role of key organisms and complex networks in oral health and disease. Periodontol 2000. 2021;87(1):107–31.
Mahmoud SA, El Moshy S, Rady D, et al. The effect of unhealthy dietary habits on the incidence of dental caries and overweight/obesity among Egyptian school children (a cross-sectional study). Front Public Health. 2022;10:953545.
Doghish AS, El-Husseiny AA, Khidr EG, et al. Decoding the role of miRNAs in oral cancer pathogenesis: a focus on signaling pathways. Pathol Res Pract. 2023;252:154949.
Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
Sun J, Tang Q, Yu S, et al. Role of the oral microbiota in cancer evolution and progression. Cancer Med. 2020;9(17):6306–21.
Morrison AG, Sarkar S, Umar S, et al. The contribution of the human oral microbiome to oral disease: a review. Microorganisms. 2023;11(2):318.
PaesLeme AF, Koo H, Bellato CM, et al. The role of sucrose in cariogenic dental biofilm formation–new insight. J Dent Res. 2006;85(10):878–87.
Rudney JD, Jagtap PD, Reilly CS, et al. Protein relative abundance patterns associated with sucrose-induced dysbiosis are conserved across taxonomically diverse oral microcosm biofilm models of dental caries. Microbiome. 2015;3:69.
Tan X, Wang Y, Gong T. The interplay between oral microbiota, gut microbiota and systematic diseases. J Oral Microbiol. 2023;15(1):2213112.
Kurtzman GM, Horowitz RA, Johnson R, et al. The systemic oral health connection: Biofilms. Medicine (Baltimore). 2022;101(46):e30517.
Bui FQ, Almeida-da-Silva CLC, Huynh B, et al. Association between periodontal pathogens and systemic disease. Biomed J. 2019;42(1):27–35.
Nazir MA. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int J Health Sci (Qassim). 2017;11(2):72–80.
Lohiya DV, Mehendale AM, Lohiya DV, et al. Effects of periodontitis on major organ systems. Cureus. 2023;15(9):e46299.
Li S, He M, Lei Y, et al. Oral microbiota and tumor-a new perspective of tumor pathogenesis. Microorganisms. 2022;10(11):2206.
Hu SW, Yang JJ, Lin YY. Mapping the scientific landscape of bacterial influence on oral cancer: a bibliometric analysis of the last decade’s medical progress. Curr Oncol. 2023;30(10):9004–18.
Wu J, Pang T, Lin Z, et al. The key player in the pathogenesis of environmental influence of systemic lupus erythematosus: aryl hydrocarbon receptor. Front Immunol. 2022;13:965941.
Nouri Z, Choi SW, Choi IJ, et al. Exploring connections between oral microbiota, short-chain fatty acids, and specific cancer types: a study of oral cancer, head and neck cancer, pancreatic cancer, and gastric cancer. Cancers (Basel). 2023;5(11):2898.
Shi C, Cai L, Xun Z, et al. Metagenomic analysis of the salivary microbiota in patients with caries, periodontitis and comorbid diseases. J Dent Sci. 2021;16(4):1264–73.
Huang Y, Zhao X, Cui L, et al. Metagenomic and metatranscriptomic insight into oral biofilms in periodontitis and related systemic diseases. Front Microbiol. 2021;12:728585.
Perera M, Al-Hebshi NN, Speicher DJ, et al. Emerging role of bacteria in oral carcinogenesis: a review with special reference to perio-pathogenic bacteria. J Oral Microbiol. 2016;8:32762.
Chen S, Zhou Y, Chen Y, et al. fastp: an ultra-fast all-in-one FASTQ preprocessor. Bioinformatics. 2018;34(17):i884–90.
Xu H, Luo X, Qian J, et al. FastUniq: a fast de novo duplicates removal tool for paired short reads. PLoS One. 2012;7(12):e52249.
Langdon WB. Performance of genetic programming optimised Bowtie2 on genome comparison and analytic testing (GCAT) benchmarks. BioData Min. 2015;8(1):1.
Wood DE, Lu J, Langmead B. Improved metagenomic analysis with Kraken 2. Genome Biol. 2019;20(1):257.
Li D, Liu CM, Luo R, et al. MEGAHIT: an ultra-fast single-node solution for large and complex metagenomics assembly via succinct de Bruijn graph. Bioinformatics. 2015;31(10):1674–6.
Hyatt D, Chen GL, Locascio PF, et al. Prodigal: prokaryotic gene recognition and translation initiation site identification. BMC Bioinformatics. 2010;11:119.
Huerta-Cepas J, Forslund K, Coelho LP, et al. Fast genome-wide functional annotation through orthology assignment by eggNOG-mapper. Mol Biol Evol. 2017;34(8):2115–22.
Li W, Godzik A. Cd-hit: a fast program for clustering and comparing large sets of protein or nucleotide sequences. Bioinformatics. 2006;22(13):1658–9.
Patro R, Duggal G, Love MI, et al. Salmon provides fast and bias-aware quantification of transcript expression. Nat Methods. 2017;14(4):417–9.
Yuan MM, Guo X, Wu L, et al. Climate warming enhances microbial network complexity and stability. Nat Clim Change. 2021;11:343–8.
Oksanen JAI, Blanchet FG, Kindt R, et al. vegan : Community Ecology Package. R package version 1.8-5. 2007.
Wang L, Dankert H, Perona P, et al. A common genetic target for environmental and heritable influences on aggressiveness in Drosophila. Proc Natl Acad Sci U S A. 2008;105(15):5657–63.
de Goffau MC, Jallow AT, Sanyang C, et al. Gut microbiomes from Gambian infants reveal the development of a non-industrialized Prevotella-based trophic network. Nat Microbiol. 2022;7(1):132–44.
Topper MJ, Vaz M, Chiappinelli KB, et al. Epigenetic therapy ties MYC depletion to reversing immune evasion and treating lung cancer. Cell. 2017;171(6):1284–1300.e21.
Sacco F, Seelig A, Humphrey SJ, et al. Phosphoproteomics reveals the GSK3-PDX1 axis as a key pathogenic signaling node in diabetic islets. Cell Metab. 2019;29(6):1422–1432.e3.
Wang B, Chen T, Li CJ, et al. Radial growth of Qinghai spruce (Picea crassifolia Kom.) and its leading influencing climate factor varied along a moisture gradient. For Ecol Manag. 2020;476:118474.
Mark Welch JL, Ramírez-Puebla ST, Borisy GG. Oral Microbiome geography: micron-scale habitat and niche. Cell Host Microbe. 2020;28(2):160–8.
Zhang L, Liu Y, Zheng HJ, et al. the oral microbiota may have influence on oral cancer. Front Cell Infect Microbiol. 2019;9:476.
Bolz J, Dosá E, Schubert J, et al. Bacterial colonization of microbial biofilms in oral squamous cell carcinoma. Clin Oral Investig. 2014;18(2):409–14.
Shin YJ, Choung HW, Lee JH, et al. Association of periodontitis with oral cancer: a case-control study. J Dent Res. 2019;98(5):526–33.
Alfano M, Canducci F, Nebuloni M, et al. The interplay of extracellular matrix and microbiome in urothelial bladder cancer. Nat Rev Urol. 2016;13(2):77–90.
Lisi S, D’Amore M, Sisto M. ADAM17 at the interface between inflammation and autoimmunity. Immunol Lett. 2014;162(1 Pt A):159–69.
Pang X, Tang YJ, Ren XH, et al. Microbiota, epithelium, inflammation, and TGF-β signaling: an intricate interaction in oncogenesis. Front Microbiol. 2018;9:1353.
Radaic A, Ganther S, Kamarajan P, et al. Paradigm shift in the pathogenesis and treatment of oral cancer and other cancers focused on the oralome and antimicrobial-based therapeutics. Periodontol 2000. 2021;87(1):76–93.
Wagener FA, Carels CE, Lundvig DM. Targeting the redox balance in inflammatory skin conditions. Int J Mol Sci. 2013;14(5):9126–67.
Barros SP, Fahimipour F, Tarran R, et al. Epigenetic reprogramming in periodontal disease: dynamic crosstalk with potential impact in oncogenesis. Periodontol 2000. 2020;82(1):157–72.
Mark Welch JL, Dewhirst FE, Borisy GG. biogeography of the oral microbiome: the site-specialist hypothesis. Annu Rev Microbiol. 2019;73:335–58.
Proctor DM, Shelef KM, Gonzalez A, et al. Microbial biogeography and ecology of the mouth and implications for periodontal diseases. Periodontol 2000. 2020;82(1):26–41.
Kim YT, Jeong J, Mun S, et al. Comparison of the oral microbial composition between healthy individuals and periodontitis patients in different oral sampling sites using 16S metagenome profiling. J Periodontal Implant Sci. 2022;52(5):394–410.
Ji S, Kook JK, Park SN, et al. Characteristics of the salivary microbiota in periodontal diseases and potential roles of individual bacterial species to predict the severity of periodontal disease. Microbiol Spectr. 2023;11(3):e0432722.
Stasiewicz M, Karpiński TM. The oral microbiota and its role in carcinogenesis. Semin Cancer Biol. 2022;86(Pt 3):633–42.
Vyhnalova T, Danek Z, Gachova D, et al. The role of the oral microbiota in the etiopathogenesis of oral squamous cell carcinoma. Microorganisms. 2021;9(8):1549.
Belstrøm D, Constancias F, Liu Y, et al. Metagenomic and metatranscriptomic analysis of saliva reveals disease-associated microbiota in patients with periodontitis and dental caries. NPJ Biofilms Microbiomes. 2017;3:23.
Struzycka I. The oral microbiome in dental caries. Pol J Microbiol. 2014;63(2):127–35.
Hettmann A, Demcsák A, Decsi G, et al. Infectious agents associated with head and neck carcinomas. Adv Exp Med Biol. 2016;897:63–80.
Koivikko T, Rodrigues PC, Vehviläinen M, et al. Detection of herpes simplex virus in oral tongue squamous cell carcinoma. Front Pharmacol. 2023;14:1182152.
Sand L, Jalouli J. Viruses and oral cancer. Is there a link? Microbes Infect. 2014;16(5):371–8.
Jain M. Assesment of correlation of herpes simplex virus-1 with oral cancer and precancer- a comparative study. J Clin Diagn Res. 2016;10(8):Zc14–7.
Jalouli J, Jalouli MM, Sapkota D, et al. Human papilloma virus, herpes simplex virus and epstein barr virus in oral squamous cell carcinoma from eight different countries. Anticancer Res. 2012;32(2):571–80.
Chen T, Chen X, Zhang S, et al. The genome sequence archive family: toward explosive data growth and diverse data types. Genomics Proteomics Bioinformatics. 2021;19(4):578–83.
Database Resources of the National Genomics Data Center. China national center for bioinformation in 2022. Nucleic Acids Res. 2022;50(D1):D27–d38.
Funding
This work was funded by the National Natural Science Foundation of China (32170071 and 82273466).
Author information
Authors and Affiliations
Contributions
ZY and YL designed the experiments. MZ carried out experiments. HLZ and LRY participated in the collection of samples. MZ analyzed data prepared the figures and drafted the manuscript. YMZ, AU and JH participation in discussion and revised the manuscript. All authors contributed to this manuscript, read, and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The studies involving human participants were reviewed and approved by ethics committee of Hunan Cancer Hospital (2023-KYJJ-025) following the ethical guidelines of the Declaration of Helsinki (No. 038, 2015). The patients/participants provided their written informed consent to participate in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, M., Zhao, Y., Umar, A. et al. Comparative analysis of microbial composition and functional characteristics in dental plaque and saliva of oral cancer patients. BMC Oral Health 24, 411 (2024). https://doi.org/10.1186/s12903-024-04181-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-024-04181-1