
Abstract
Background
Ameloblastoma (AM), the benign counterpart of ameloblastic carcinoma, is a benign odontogenic tumor of epithelial origin, naturally aggressive, with unlimited growth potential and a high tendency to relapse if not adequately removed. Patients with AM treated surgically can benefit from dental implant therapy, promoting oral rehabilitation and improving their quality of life. The present study aimed to determine the survival rate of dental implants placed after surgical treatment of patients affected by AM. In addition, there were two secondary objectives: 1) To evaluate which dental implant loading protocols are most frequently used and 2) To determine the type of prosthetic restoration most commonly used in these patients.
Methods
The Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines were followed during the study. Searches were performed in three databases (PubMed/MEDLINE, Scopus, and Google Scholar) until November 2023. Additionally, the electronic search was enriched by an iterative hand search of journals related to oral pathology and medicine, maxillofacial surgery, and oral prosthodontics and implantology. Only reports and case series in English from January 2003 to date were included. The Joanna Briggs Institute tool (JBI-Case Reports/Case Series) was used for the study quality assessment.
Results
The total number of patients and implants studied were 64 and 271, respectively, all with surgically treated AM. The patient’s ages ranged from 8 to 79 years, with a mean (SD) age of 37.3 ± 16.4. Fifty-three percent were male and 47% were female. The range of follow-up duration was 1 to 22 years. An implant survival/success rate of 98.1% was reported. In addition, most of them were conventionally loaded (38.3%). Hybrid implant-supported fixed dentures were the most commonly used by prosthodontists (53%).
Conclusions
Oral rehabilitation with dental implants inserted in free flaps for orofacial reconstruction in surgically treated patients with AM can be considered a safe and successful treatment modality.
Similar content being viewed by others


Background
Ameloblastoma (AM) is a benign odontogenic tumor of epithelial origin, naturally aggressive, with unlimited growth potential and a high tendency to relapse if not adequately removed [1]. It represents 1% of tumors affecting the oral cavity and is the second most common benign neoplasm after odontoma, constituting approximately 9–11% of odontogenic tumors [2]. It shows a higher incidence between the fourth and fifth decade of life; however, it has no predilection for sex or race [3]. Regarding its location, 80% of all AM affects the posterior region of the mandible (corresponding to the site of the mandibular ramus, angle, and body), followed by the anterior part of the mandible and the posterior and anterior maxillary segments [4]. Nasal tract, orbital, and intracranial involvement are rare; however, they have been reported and can cause serious consequences [5,6,7]. AM are usually asymptomatic and, in most cases, are diagnosed in advanced stages. In this regard, the lesions that progress can reach a considerable size, generating erosion of bone tissue and invasion of neighboring tissues. Therefore, clinically, patients show swelling in the affected area, loss of teeth, malocclusion, airway obstruction, pathological fractures, and sometimes the tumor can become infected [8]. Radiographically, the classic pattern of AM is shown as a radiolucent, unilocular, or multilocular, well-defined lesion, which may show displacement of adjacent teeth and/or root resorption. Computed tomography is helpful for the evaluation of its extension and the degree of bone destruction [9].
According to the new classification of odontogenic tumors and maxillofacial lesions published by the World Health Organization (WHO) in 2022, five types are distinguished: conventional AM, formerly called solid/multicystic, unicystic (intraluminal, luminal, and mural), extraosseous/peripheral, metastatic and adenoid (recently introduced) [10]. Conventional AM is the most frequent and represents approximately 86–90% of all cases. According to its histologic findings, it can be classified into follicular, plexiform, acanthomatous, desmoplastic, basal, and granular. These patterns can occur individually or in combination; however, the follicular variant is the most frequent, followed by the plexiform variant [11]. The follicular pattern is characterized by the epithelial cells being arranged in islands or follicles surrounded by connective tissue, whereas, in the plexiform pattern, the epithelial cells are arranged in an interwoven plexiform network that outlines the adjacent connective tissue [3]. Thus, clinical features, imaging, and histopathological examination are needed together to confirm the definitive diagnosis of the lesion.
The management of AM remains a significant challenge for surgeons despite being one of the most common odontogenic neoplasms [12]. Some studies demonstrated a higher recurrence rate in patients after being treated by a conservative approach versus a radical one [13, 14]. Furthermore, a significant improvement in the quality of life of patients after surgical treatment of AM has been demonstrated [15]; therefore, the treatment of choice for this type of tumor remains surgical resection, which includes marginal or segmental resection with or without disarticulation depending on the extent of the tumor, together with periodic long-term follow-up (> 10 years). In addition, sufficient safety margins of 1.5 to 2 cm are recommended to prevent possible recurrence, followed by reconstruction of the resulting anatomical bone defect [16] using bone graft biomaterials such as autogenous grafts (derived from the same individual), which can be non-vascularized bone grafts or vascularized free flaps, allogenic (derived from another individual of the same species), xenogeneic (acquired from other species), alloplastic (commercially prepared) and customized (use of active biomolecules to regenerate bone) [17].
Patients with AM can benefit from dental implant therapy, which can be placed during surgery (primary placement) or after completion of surgical treatment (secondary placement), followed by implant-supported prosthetic rehabilitation using a fixed dental prosthesis, which can be cemented, screw-retained, or hybrid and/or a removable dental prosthesis [18]. In fact, it has been shown that patients with oral cancer mainly benefit from primary placement of dental implants for prosthetic rehabilitation with a 5-year survival rate of 92.8% compared to secondary placement (86.4%) [19], as well as a higher survival rate has been observed in those immediately [20] and delayed placed implants that had not received radiotherapy compared to previously irradiated sites [21]. On the other hand, a recent systematic review and meta-analysis reported an overall survival rate of 97% after 1 year of prosthetic loading following surgical resection of oral tumors and subsequent mandibular reconstruction with fibula free-flap. In this study, 69% of the tumors analyzed were benign and included AM. In addition, as part of the secondary objectives, the authors demonstrated a survival rate of 98% with immediate implants and 97% with delayed implants [22]. However, research on the survival rate of dental implants and subsequent implant-supported rehabilitation in surgically treated AM patients is scarce. Therefore, the present study aimed to determine the survival rate of dental implants placed subsequent to surgical treatment of patients affected by AM. In addition, two secondary objectives were set: 1) To evaluate which dental implant loading protocols are most frequently used and 2) To determine the type of prosthetic restoration most commonly used in these patients.
Methods
Protocol and methods
For the literature search and selection of studies, the present work was constructed following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines [23]. The protocol was not registered.
The electronic databases PubMed/MEDLINE, Scopus, and Google Scholar were consulted to investigate all available evidence on studies describing implant-supported prosthetic rehabilitation in surgically treated AM patients in detail. For this purpose, the Boolean terms “OR” and “AND” were used together with search header terms (MeSH). The PICO strategy was used, which consisted of Population (P)-patients affected by ameloblastoma, Intervention (I)-subjected to surgical treatment and subsequent implant-supported rehabilitation, Control (C)-not applicable, and Outcome (OR)-dental implant survival rate, loading protocol, type and functionality of prosthetic restorations used. Thus, the following research question was formulated: “What is the survival rate of dental implants placed after surgical treatment of patients affected by ameloblastoma?” with the following sub-questions: “What is the most frequent loading protocol?” and “What is the most common type of implant-supported prosthetic restoration used in these patients?”
Eligibility criteria
The following characteristics were considered to select the best articles related to this research topic: On the one hand, articles from 2000 to date (2023) written in English were included. Regarding their design, only reports and case series were included. The articles included had to clearly present the confirmation of the histopathologic diagnosis of ameloblastoma, detail the type of intervention and reconstructive technique, the implant loading protocol, and the type of prosthetic restoration used, with a minimum follow-up of > 1 year. On the other hand, articles published before 2000 and those written in a language other than English were not considered. Cross-sectional clinical studies, cohort studies, narrative reviews, comprehensive reviews, systematic reviews, and meta-analyses were also excluded. Finally, studies showing insufficient data (lack of confirmatory tumor diagnosis, type of intervention, reconstructive technique, implant loading protocol, type of prosthetic restoration without follow-up or a follow-up < 1 year) were excluded from this study.
Search strategy
The search was limited to case reports and case series only. A combination of keywords was used, including “Ameloblastoma,” “Dental implants,” “Fixed and removable dental prosthesis,” and/or “Implant-supported prosthetic rehabilitation.” The electronic search was enriched by an iterative hand search of journals related to oral pathology and medicine, maxillofacial surgery, and oral prosthodontics and implantology. The journals were the following: “Journal of Oral Pathology & Medicine,” “Oral Surgery Oral Medicine Oral Pathology Oral Radiology,” “British Journal of Oral & Maxillofacial Surgery,” “Oral and Maxillofacial Surgery Clinics of North America,” Journal of Cranio-Maxillofacial Surgery“ and “Dentomaxillofacial Radiology,” Journal of Prosthodontics-Implant Esthetic and Reconstructive Dentistry, Journal of Prosthodontic Research, Journal of Advanced Prosthodontics, International Journal of Prosthodontics, European Journal of Prosthodontics and Restorative Dentistry, Journal of Esthetic and Restorative Dentistry, Journal of Prosthetic Dentistry, Journal of Indian Prosthodontics Society and Journal of Prosthodontics. Table 1 shows the search strategy employed.
Study selection
Initially, the studies were selected considering the articles’ titles and abstracts; any ambiguity in these sections was resolved by resorting to a full-text article. The articles found in the databases were subjected to a second review according to the eligibility criteria. If any conflict arose between the principal investigators (M.A.A.S and J.S.B.R), a third investigator (A.H) was consulted to resolve the debate.
Quality assessment
Study quality was assessed following the guidelines (https://jbi.global/critical-appraisal-tools) in the individual case report and case series sections [24]. All included articles underwent quality assessment independently by two investigators (M.A.A.S and J.S.B.R). The instrument is based on a series of questions grouped according to the type of studies included in the systematic review that can be rated as: “Yes,” “No,” “Unclear” or “Not applicable.” According to the assessment tool, the risk of bias was classified as high when the study reached up to 49% of the “Yes” scores, moderate from 50 to 69%, and low when it reached above 70%.
Data extractions and statistical analysis
From the previously selected articles, data extraction was performed by a third reviewer (A.H), and all relevant information such as The year of publication, first author, country, number of cases, study design, age, gender, characteristics of ameloblastoma such as histological type, location, clinical and imaging findings, type of surgical treatment, type of reconstruction, time after surgical reconstruction and the characteristics of the implant-supported prosthetic rehabilitation such as number of implants, the system used, position, size, loading protocol, complications, recurrence of MA after implant placement, survival rate, type of prosthesis, biomaterials used for the construction of the restorations and the follow-up period were extracted and recorded first in a standardized Excel data sheet and then in a database in the statistical program STATA V15. Finally, the selected articles were analyzed by descriptive statistics representing the data with mean ± standard deviation (SD), range (minimum-maximum), absolute and relative frequency. All the data were taken together to construct the systematic review.
Results
Selection of studies
Initially, 2669 articles were found. Duplicates were eliminated, and based on the title and abstract, the remaining 2649 studies were reviewed. After analyzing the full text of the remaining articles, 2612 records were excluded as irrelevant. A total of 37 articles were assessed for eligibility, of which two studies were excluded because patient prosthetic rehabilitation was not fully described. Therefore, 35 articles were included in this systematic review (Fig. 1).

PRISMA flow diagram. PRISMA: Preferred Reporting Items for Systematic and Meta-Analyses
Characteristics of the studies
Thirty-five investigations were reviewed in this study, of which 5 (14.3%) were case series [25,26,27,28,29] and 30 (85.7%) were case reports [30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59]. The total number of patients studied in the included investigations was 64, all with a history of surgically treated ameloblastomas and their subsequent implant-supported prosthetic rehabilitation. Most articles were published after 2013 (25: 71.4%). Four (24%) studies were conducted in India [42, 44, 55, 58], Turkey [27, 32, 47, 49] and Brazil [37, 46, 52], 3 (18%) in the USA [30, 35, 41], Spain [31, 50, 57], China [28, 33, 43], Korea [38, 39, 53], 2 (12%) in Italy [36, 48], Finland [29, 40] and other studies (6%) in Japan [54], Colombia [59], Iran [56], Taiwan [25], Austria [26] and Romania [45] (Tables 2 and 4).
Clinicopathologic characteristics of the patients
The ages of the patients ranged from 8 to 79 years; the mean ± (SD) age of the patients studied was 37.3 ± 16.4 years, of whom 53% were male and 47% were female. A total of 12 (19%) cases were reported as recurrent AM, which were reintervened. It was also observed that 94% of patients had conventional/multicystic AM [25, 27,28,29,30, 32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49, 51,52,53,54,55,56,57,58,59], and only 4 (6%) cases were diagnosed as unicystic type AM [26, 31, 42, 50]. The most common histologic variant was the plexiform type (11%) [26, 37, 39, 49], followed by the follicular variant (8%) [26, 34, 38, 45, 46]. The most affected anatomical region was the mandible (94%) [25, 27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49, 51,52,53,54,55,56, 58, 59], mainly the posterior (58.3%) and left side of the face (42%), followed by the posterior maxilla (75%) [26, 50, 57]. Clinically, 97% of patients were asymptomatic (did not report pain) [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51, 53, 54, 57,58,59], and 91% presented cortical expansion [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41, 44,45,46,47, 49,50,51,52, 55, 56, 59]. Radiographically, 97% of the lesions were radiolucent [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53, 55, 56, 58, 59], multilocular (89.10%) [25, 27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53, 56, 58, 59], well-defined (73.43%) [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43, 45,46,47,48,49,50,51,52,53, 56, 58, 59]. Bone resorption was present in 50% [27, 29, 31, 32, 35,36,37,38,39,40,41,42,43, 45,46,47,48,49,50,51,52,53, 56] of the cases, and 45.31% of the cases had a displacement of teeth adjacent to the tumor lesion [27, 29, 31, 32, 35,36,37,38,39,40,41,42, 56]. The treatment of choice was surgical resection of the tumor (100%) [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59], with segmental mandibulectomy being the most frequent procedure (77%) [25, 28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47, 49, 50]. For reconstruction of the resulting bone defect, 41% of the cases were reconstructed by fibula free-flap [25, 28, 32, 34, 36, 41, 55, 57, 58], followed by iliac bone graft (31.2%) [26, 27, 31, 33, 35, 37, 38, 42, 45, 47, 49, 56]. Finally, the mean time after maxillofacial reconstruction for dental implant placement was 23.00 ± 34.00 months, equivalent to 1.9 years (Tables 2 and 4).
Characteristics of the implant-supported prosthetic rehabilitation of patients
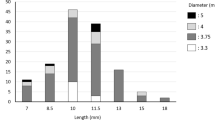
A total of 261 implants were studied in the included investigations, of which only 4 (2%) [29, 40, 53, 56] failed. In addition, no relapses of the tumor lesion after dental implant placement were reported. The survival rate was 98.1%, and the range of follow-up duration was 1–22 years. After implant placement, 38.3% were conventionally loaded [28, 30, 31, 33, 36,37,38,39,40, 43, 45, 48, 54, 56, 58], followed by the immediate loading protocol (28%) [25, 34, 35, 41, 42, 52]. In total, 62 implant-supported restorations were placed, of which 79% corresponded to fixed dentures [25, 28, 29, 31,32,33,34,35,36, 38, 39, 41,42,43,44, 46,47,48,49,50,51,52, 54,55,56,57,58,59] and 21% to removable dentures [26, 27, 30, 33, 37, 40, 45, 53]. Regarding fixed prostheses, the most used types were hybrid prostheses (53%) [43, 49, 52, 56,57,58,59], followed by cemented restorations (27%) [35, 42, 44, 55]. Of the removable prosthesis, metal bar retention was the most frequently used anchorage system (86%) [26, 27, 30, 33, 37, 55]. The most commonly used biomaterials for the construction of prosthetic devices were metal-ceramic (55%) [34, 35, 42, 44,45,46] for the fixed systems and acrylic resin (27.3%) for the removable systems [30, 33, 55] (Tables 3 and 4).
Quality evaluation
Tables 5 and 6 show the results of the quality assessment of the included studies. Based on the checklist used to score the articles, all studies achieved scores > 70 [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59], resulting in a low risk of bias in all selected studies.
Discussion
Odontogenic tumors (OTs) are a heterogeneous group of lesions whose pathogenesis is associated with alterations in components of signaling pathways involved in tooth formation (Wnt, BMP, FGF, Shh, and Eda) [60, 61]. The first accepted classification of OTs was published by WHO in 1971, then revised and updated in 1992, 2005, and 2017 [62], and finally, 5 years later, in 2022, thanks to advances in the technology of molecular tools used for clinical and research purposes. This new classification presents some modifications; however, based on the biological behavior and the origin of the tumor tissue, OTs are classified into benign and malignant; in turn, benign OTs are classified into epithelial, mixed (epithelial and mesenchymal), and mesenchymal, while malignant OTs are classified into carcinomas, sarcomas, and carcinosarcomas respectively [1].
Focusing on benign tumor lesions of epithelial origin, in particular AM, which are the benign counterpart of ameloblastic carcinoma, five types are currently distinguished, of which conventional AM remains the most common type, followed by unicystic and extraosseous/peripheral AM [63].
AM is a neoplasm originating from the epithelium that constitutes the enamel organ during odontogenesis [64]. It was first described in 1827 by Cusack et al. and was named “Adamantinoma” by Malassez in 1890; later, Ivy and Churchill introduced the term “Ameloblastoma” in 1930 [3, 9]. Annually, it is estimated that 0.5 cases per million population occur [65], making it one of the most frequent OTs.
A systematic review constituting the most extensive dataset (n = 3677) of patients with AM in different countries and regions concluded that AM presents as a painless bone swelling over the mandible, mainly in patients with a mean age of 36 years and an equal distribution by gender, very similar to the results reported in the present study. However, at the same time, there are some minor differences in the sociodemographic and clinical characteristics of AM in different countries and regions [66].
The data presented in this review are comparable with several retrospective studies published in different parts of the world. In general, it has been shown that the average age of presentation of AM ranges between the fourth and fifth decade of life [3], with a maximum age of 79 years, according to the data reported in this research. In Europe, the mean age has been reported to be 48.2 years [67]; in North America, 40.7 years [68]; in South America, 35.1 years [69]; in Africa, 31.3 years [70] and in Asia 30.35 years [71]. There is no gender predilection, although a slight male predominance has been reported, with a male-to-female ratio 3:2 [70]. Clinically, regarding their site of appearance, AM most frequently affects the posterior part of the mandible, followed by the maxilla [4, 67,68,69,70,71,72]. However, other rare extraoral presentation sites of particular interest have also been reported, such as involvement of the nasal tract (sinonasal AM), which histologically is very similar to AM of the gnathic bones, but its clinical presentation is different. It can cause partial or total obstruction of the nasal cavities and paranasal sinuses, in addition to showing typical signs of rhinorrhea and nosebleeds. Furthermore, it affects an older group of patients (59 years) [5]. On the other hand, involvement of the orbital cavities has also been reported, and the most frequent ophthalmological manifestations are decreased or loss of vision, proptosis, displacement of the eyeball, limitation of extraocular movement, diplopia, cavernous sinus syndrome, edema of the lower eyelid and ptosis [6].
The uncontrolled growth of tumors affecting the jaws can be so exaggerated that it can extend to the intracranial compartment [7], leading to severe consequences. These rare and quite dangerous locations are because the maxillary bone is very thin, fragile, and porous compared to the mandible, making it susceptible to invasion of adjacent structures without any restriction [73]. AM of the gnathic bones are usually asymptomatic and are diagnosed in advanced stages [8]. However, some authors have reported pain symptoms in the affected area [67, 74]. The presence of swelling, ulceration, malocclusion, mobility, and loss of teeth are these patients’ most frequent clinical manifestations [8]. Radiographically, the radiolucent and multilocular appearance is the most common, followed by the unilocular appearance [9, 71]. Furthermore, these lesions are characterized by displacement of adjacent teeth, root resorption, and bone expansion [67, 75]. The follicular and plexiform variants are the most frequent histological types, which can occur individually or in combination [10, 11, 67, 76].
The treatment of AM is surgical and can be performed using a conservative approach, which includes enucleation, curettage/curettage, and/or marsupialization, as well as a radical approach that provides for marginal and segmental resection, hemimandibulectomy and/or hemimaxylectomy, depending on the extent and severity of the lesion. In fact, according to scientific evidence, treatment strategy is the main factor influencing recurrence rates and the risk of developing postoperative complications [13,14,15,16]. A study that analyzed 158 cases showed that the risk of recurrence of AM treated by enucleation was 4.62 times higher than that of AM treated radically [77]. Very similarly, another study reported a higher recurrence rate in patients undergoing bone curettage and enucleation compared to patients treated radically; however, the latter presented a more significant number of complications (facial asymmetry, temporal paresthesia of the inferior alveolar nerve, infection, and swelling), aesthetic and functional deficiencies that could compromise the quality of life of patients [78]. This agrees with another study comparing surgically treated AM patients’ pre- and post-operative quality of life. The authors found that quality of life decreased immediately after surgery, then gradually improved and exceeded preoperative values 6 months after the surgical procedure [15]. Therefore, surgical excision with wide safety margins (1.5 to 2 cm) is the mainstay for treating conventional AM since conservative approaches show high recurrence rates.
Secondary defects of the oral and maxillofacial region that occur as a consequence of radical surgical procedures can often lead to severe aesthetic and functional alterations, requiring complex reconstructive techniques with the primary purpose of achieving oral rehabilitation, that is, restoring the patient’s symmetry and functionality, as close as possible to their premorbid state and, therefore, improve their quality of life [79].
Scientific evidence has suggested that the vascularized fibula free-flap is the most widely used autogenous bone graft for the reconstruction of orofacial anatomical defects as a consequence of surgery [80], which is consistent with the results of our study. This flap type provides adequate bone length, a long vascular pedicle that easily adapts to the mandible, and a bicortical architecture, which increases the primary fixation of dental implants [81]. In this sense, high success rates (91%) have been reported through the use of this type of graft [82], the most frequent complications being the presence of infections and wound dehiscence, loss of skin graft in the donor site, complete flap loss and percutaneous fistulas [83]. Furthermore, oral health-related quality of life has been shown to improve markedly in these patients [84]. Finally, it is expected that, with new technologies, such as virtual surgical planning with 3D models and cone beam computed tomography, more precise reconstructions can be made, reducing the risk of postoperative complications and favoring subsequent implant-supported prosthetic rehabilitation.
Of the studies evaluated, none reported recurrences of the tumor lesion after dental implant placement, demonstrating the surgical treatment’s high effectiveness. Furthermore, the survival rate of dental implants was 98.1%. In general, survival/success rates of 83.9% [85], 97% [22], and 98.8% [86] have been reported, demonstrating that oral rehabilitation with dental implants inserted in free flaps for reconstruction maxillofacial surgery after ablative surgery can be considered a safe treatment modality with successful results.
On the other hand, in cancer, it has been shown that patients mainly benefit from the primary placement of dental implants for prosthetic rehabilitation with a 5-year survival rate of 92.8% compared to secondary placement (86, 4%) [19], as well as, for those patients who have not received radiotherapy compared to previously irradiated sites [21]. Wuster et al. [87] reported high survival rates in patients who had undergone surgery for a head and neck tumor. A survival rate of 99.1% after 3 years and 93.1% after 5 years was reported in patients without vestibuloplasty, compared to a survival and implant success rate of 100% after 5 years in patients with vestibuloplasty, which improved considerably. During the observation period, six implants were lost. Therefore, the authors suggest that vestibuloplasty should always be considered and applied if the anatomical conditions require it to achieve high implant success rates in patients with head and neck tumors.
A high survival rate of dental implants has been demonstrated in patients with systemic autoimmune diseases with repercussions in the oral cavity. In patients with lichen planus, and after a follow-up period of 44,6 months, the survival rate of dental implants was 98,3%. In patients with epidermolysis bullosa it was 98,7% at 32,6 months. For patients with Sjögren’s syndrome it was 94,2% after 45,2 months. In patients with systemic sclerosis it was 97,7% after 37,5 months. In patients with pemphigus, and systemic lupus erythematosus it was 100% after 24 months [88] Thus, it appears that the autoimmune status had no discernible impact on the survival rate of dental implants, however, a comprehensive risk assessment is recommended before starting implant therapy [89].
Stable anchorage of fixed and/or removable implant-supported dental prostheses represents successful clinical treatment approaches in partially edentulous patients [90]. To achieve an adequate osseointegration process, implants should be immersed in the bone without placing any type of load for 3 to 4 months (early loading) up to 6 to 8 months (conventional/late loading) [91]. In the present study, the conventional approach was the most used by surgeons, and although the immediate loading (placement of the provisional/definitive on the same day of surgery) of dental implants has benefited by shortening the treatment period. Available randomized clinical trials suggest that this protocol is associated with a higher incidence of implant failure [92]. To allow immediate placement or provisionalization, good initial stability of the implant is required (> 35 N/cm2), and an implant stability coefficient value > 60 will allow a good prognosis for the patient. However, good primary stability is not always possible, and some factors such as local anatomy, bone density, implant milling protocol, and macro-design may influence it [93,94,95]. Finally, hybrid prosthetic restorations represent an excellent option for reconstructing alveolar ridges with moderate to severe resorption. They correspond to a screw-retained structure with cemented crowns fabricated of different materials (porcelain, lithium disilicate, zirconia). These restorations splint the implants together, provide adequate resistance, and meet aesthetic demands [56, 96,97,98,99,100,101].
Conclusions
Based on the findings found in this review, the following conclusions can be drawn:
-
1.
Conventional AM follicular histological variant was the most common type of tumor lesion.
-
2.
The treatment of choice was surgical resection of the tumor using segmental mandibulectomy.
-
3.
The fibula-free flap was used most frequently for the reconstruction of the orofacial defect, and on average, the time elapsed after the maxillofacial reconstruction for the placement of dental implants was 23 months, equivalent to 1.9 years.
-
4.
An implant survival/success rate of 98.1% was reported. Furthermore, most of them were loaded conventionally.
-
5.
Hybrid implant-supported fixed dental prostheses were the most used by prosthodontists.
Availability of data and materials
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Abbreviations
- AM:
-
Ameloblastoma
- OTs:
-
Odontogenic tumors
- WHO:
-
World Health Organization
- Wnt:
-
Wnt/B-catenin signaling
- BMP:
-
Bone morphogenic protein
- FGM:
-
Fibroblast growth factor
- Shh:
-
Sonic hedgehog
- Eda:
-
Ectodysplasin A
References
El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ. Who Classification of Head and Neck Tumours. International Agency; 2017. p. 215–31.
Kokubun K, Yamamoto K, Nakajima K, Akashi Y, Chujo T, Takano M, Katakura A, Matsuzaka K. Frequency of Odontogenic Tumors: A Single Center Study of 1089 Cases in Japan and Literature Review. Head Neck Pathol. 2022;16(2):494–502. https://doi.org/10.1007/s12105-021-01390-w. Epub 2021 Oct 30. PMID: 34716904; PMCID: PMC9187835.
Ghai S. Ameloblastoma: an updated narrative review of an enigmatic tumor. Cureus. 2022;14(8):e27734.
Lu Y, Zhang X, Li X. Molecular biology exploration and targeted therapy strategy of Ameloblastoma. Arch Oral Biol. 2022;140:105454.
Mehta V, Sarode GS, Obulareddy VT, Sharma T, Kokane S, Cicciù M, Minervini G. Clinicopathologic profile, management and outcome of Sinonasal Ameloblastoma-a systematic review. J Clin Med. 2023;12(1):381. https://doi.org/10.3390/jcm12010381. PMID: 36615180; PMCID: PMC9821057.
Abtahi MA, Zandi A, Razmjoo H, Ghaffari S, Abtahi SM, Jahanbani-Ardakani H, Kasaei Z, Kasaei-Koupaei S, Sajjadi S, Sonbolestan SA, Abtahi SH. Orbital invasion of ameloblastoma: a systematic review apropos of a rare entity. J Curr Ophthalmol. 2017;30(1):23–34. https://doi.org/10.1016/j.joco.2017.09.001. PMID: 29564405; PMCID: PMC5859465.
Armocida D, Berra LV, Pucci R, Battisti A, Della Monaca M, Valentini V, Santoro A. Ameloblastoma and Intracranial Involvement: The Current Challenge of the Radical Surgical Treatment. Comprehensive Review of the Literature and Institution experience. J Maxillofac Oral Surg. 2022;21(1):34–43. https://doi.org/10.1007/s12663-021-01643-9. Epub 2021 Sep 24. PMID: 35400903; PMCID: PMC8934804.
da Silva LAM, Filho SRC, Saraiva MJD, Maia CR, Santos CDFDP, Santos PPA. Clinical, Radiographic and histopathological analysis of Craniopharyngiomas and Ameloblastomas: a systematic review. Head Neck Pathol. 2022;16(4):1195–222. https://doi.org/10.1007/s12105-022-01473-2. Epub 2022 Aug 3. PMID: 35920974; PMCID: PMC9729483.
Effiom OA, Ogundana OM, Akinshipo AO, Akintoye SO. Ameloblastoma: current etiopathological concepts and management. Oral Dis. 2018;24(3):307–16. https://doi.org/10.1111/odi.12646. Epub 2017 Mar 9. PMID: 28142213.
Vered M, Wright JM. Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Odontogenic and Maxillofacial Bone Tumours. Head Neck Pathol. 2022;16(1):63–75. https://doi.org/10.1007/s12105-021-01404-7. Epub 2022 Mar 21. PMID: 35312978; PMCID: PMC9019005.
Jurado-Castañeda, et al. Conventional Ameloblastoma. A case report with microarray and Bioinformatic analysis. Diagnostics. 2022;12:3190.
Adeel M, Rajput MSA, Arain AA, Baloch M, Khan M. Ameloblastoma: management and outcome. Cureus. 2018;10(10):e3437. https://doi.org/10.7759/cureus.3437. PMID: 30546984; PMCID: PMC6289562.
Hendra FN, Natsir Kalla DS, Van Cann EM, de Vet HCW, Helder MN, Forouzanfar T. Radical vs conservative treatment of intraosseous ameloblastoma: systematic review and meta-analysis. Oral Dis. 2019;25(7):1683–96. https://doi.org/10.1111/odi.13014. Epub 2019 Jan 1. PMID: 30548549.
Troiano G, Dioguardi M, Cocco A, Laino L, Cervino G, Cicciu M, Ciavarella D, Lo ML. Conservative vs radical approach for the treatment of solid/multicystic Ameloblastoma: a systematic review and Meta-analysis of the last decade. Oral Health Prev Dent. 2017;15(5):421–6. https://doi.org/10.3290/j.ohpd.a38732. PMID: 28748232.
Lawal HS, Adebola RA, Arotiba JT, Amole IO, Efunkoya AA, Omeje UK, Amole TG, Adeoye JB. Quality of life of patients surgically treated for ameloblastoma. Niger Med J. 2016;57(2):91–8. https://doi.org/10.4103/0300-1652.182069. PMID: 27226682; PMCID: PMC4872498.
Neagu D, Escuder-de la Torre O, Vázquez-Mahía I, Carral-Roura N, Rubín-Roger G, Penedo-Vázquez Á, Luaces-Rey R, López-Cedrún JL. Surgical management of ameloblastoma. Review of literature. J Clin Exp Dent. 2019;11(1):e70–5. https://doi.org/10.4317/jced.55452. PMID: 30697397; PMCID: PMC6343988.
Janjua OS, Qureshi SM, Shaikh MS, Alnazzawi A, Rodriguez-Lozano FJ, Pecci-Lloret MP, Zafar MS. Autogenous tooth bone grafts for repair and regeneration of maxillofacial defects: a narrative review. Int J Environ Res Public Health. 2022;19:3690. https://doi.org/10.3390/ijerph19063690.
Kumar BP, Venkatesh V, Kumar KA, Yadav BY, Mohan SR. Mandibular Reconstruction: Overview. J Maxillofac Oral Surg. 2016;15(4):425–41. https://doi.org/10.1007/s12663-015-0766-5. Epub 2015 Apr 19. PMID: 27833334; PMCID: PMC5083680.
Alberga JM, Vosselman N, Korfage A, Delli K, Witjes MJH, Raghoebar GM, Vissink A. What is the optimal timing for implant placement in oral cancer patients? A scoping literature review. Oral Dis. 2021;27(1):94–110. https://doi.org/10.1111/odi.13312. Epub 2020 Mar 19. PMID: 32097511; PMCID: PMC7818452.
In 't Veld M, EAJM S, FKJ L. Immediate dental implant placement and restoration in the edentulous mandible in head and neck cancer patients: a systematic review and meta-analysis. Curr Opin Otolaryngol Head Neck Surg. 2021;29(2):126–37. https://doi.org/10.1097/MOO.0000000000000685. PMID: 33278135; PMCID: PMC7969163.
Camolesi GCV, Veronese HRM, Celestino MA, Blum DFC, Márquez-Zambrano JA, Carmona-Pérez FA, Jara-Venegas TA, Pellizzon ACA, Bernaola-Paredes WE. Survival of osseointegrated implants in head and neck cancer patients submitted to multimodal treatment: a systematic review and meta-analysis. Support Care Cancer. 2023;31(12):641. https://doi.org/10.1007/s00520-023-08088-5. PMID: 37851170.
Illand C, Destruhaut F, Porporatti AL, Wulfman C, Naveau A, Rignon-Bret C. Implant survival rate in mandible reconstructed with free fibula flaps after Oral tumors: a systematic review and Meta-analysis. Int J Oral Maxillofac Implants. 2023;38(5):976–85. https://doi.org/10.11607/jomi.10373. PMID: 37847839.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 Statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
National Heart, Lung, and Blood Institute. Study quality assessment tools Available at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed 11 Jan 2020.
Chana JS, Chang YM, Wei FC, Shen YF, Chan CP, Lin HN, Tsai CY, Jeng SF. Segmental mandibulectomy and immediate free fibula osteoseptocutaneous flap reconstruction with endosteal implants: an ideal treatment method for mandibular ameloblastoma. Plast Reconstr Surg. 2004;113(1):80–7. https://doi.org/10.1097/01.PRS.0000097719.69616.29. PMID: 14707625.
Zemann W, Feichtinger M, Kowatsch E, Kärcher H. Extensive ameloblastoma of the jaws: surgical management and immediate reconstruction using microvascular flaps. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(2):190–6. https://doi.org/10.1016/j.tripleo.2006.05.004. Epub 2006 Sep 25. PMID: 17234534.
Tözüm TF, Sönmez E, Askin SB, Tulunoglu I, Safak T. Implant stability and peri-implant parameters in free vascularized iliac graft transplantation patients: report of three ameloblastoma cases. J Periodontol. 2011;82(2):329–35. https://doi.org/10.1902/jop.2010.100339. Epub 2010 Oct 8. PMID: 20932154.
Cheung LK, Chua HD, Hariri F, Pow EH, Zheng L. Alveolar distraction osteogenesis for dental implant rehabilitation following fibular reconstruction: a case series. J Oral Maxillofac Surg. 2013;71(2):255–71. https://doi.org/10.1016/j.joms.2012.09.028. PMID: 23351759.
Wolff J, Sándor GK, Miettinen A, Tuovinen VJ, Mannerström B, Patrikoski M, Miettinen S. GMP-level adipose stem cells combined with computer-aided manufacturing to reconstruct mandibular ameloblastoma resection defects: experience with three cases. Ann Maxillofac Surg. 2013;3(2):114–25. https://doi.org/10.4103/2231-0746.119216. PMID: 24205470; PMCID: PMC3814659.
Becker W, Wong J. Early functional loading in the fully edentulous mandible after mandibular resection and reconstruction due to an ameloblastoma: case report. Clin Implant Dent Relat Res. 2003;5(1):47–51. https://doi.org/10.1111/j.1708-8208.2003.tb00181.x. PMID: 12831728.
Mareque Bueno J, Mareque Bueno S, Pamias Romero J, Bescos Atín MS, Huguet Redecilla P, Raspall MG. Mandibular ameloblastoma. Reconstruction with iliac crest graft and implants. Med Oral Patol Oral Cir Bucal. 2007;12(1):E73–5. PMID: 17195835.
Kürkcü M, Benlidayi ME, Kurtoğlu C, Kesiktaş E. Placement of implants in the mandible reconstructed with free vascularized fibula flap: comparison of 2 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105(3):e36–40. https://doi.org/10.1016/j.tripleo.2007.09.023. PMID: 18280944.
Wong TL, Wat PY, Pow EH, McMillan AS. Rehabilitation of a mandibulotomy/onlay/graft-reconstructed mandible using a milled bar and a tooth- and implant-supported removable dental prosthesis: a clinical report. J Prosthet Dent. 2010;104(1):1–5. https://doi.org/10.1016/S0022-3913(10)00095-8. PMID: 20620364.
Paranque AR, Steve M, Vazquez L, Bolleyn A, Roze-Pellat MA, Dohan Ehrenfest DM. Esthetic and functional reconstruction of the posttumoral interrupted mandible with double-barrel fibular free flap graft: rationale for a microsurgical and prosthodontic approach. J Oral Implantol. 2011;37(5):571–7. https://doi.org/10.1563/AAID-JOI-D-10-00060. Epub 2010 Aug 16. PMID: 20712447.
Minichetti JC, D'Amore JC, Schwarz E. Complete oral rehabilitation of a postresection ameloblastoma patient: a clinical case report. J Oral Implantol. 2011;37(6):735–44. https://doi.org/10.1563/AAID-JOI-D-11-00155. Epub 2011 Sep 28. PMID: 21955211.
Oteri G, Ponte FS, Pisano M, Cicciù M. Five years follow-up of implant-prosthetic rehabilitation on a patient after mandibular ameloblastoma removal and ridge reconstruction by fibula graft and bone distraction. Dent Res J (Isfahan). 2012;9(2):226–32. https://doi.org/10.4103/1735-3327.95241. PMID: 22623943; PMCID: PMC3353703.
Dos Santos PR, Boos FB, Lourenço EJ, Hochuli-Vieira E, da Costa RP, Homsi N. Five-year follow-up of modified implant-supported overdenture in an iliac crest autograft failure: clinical report. J Craniofac Surg. 2013;24(5):e523–6. https://doi.org/10.1097/SCS.0b013e3182a23777. PMID: 24036834.
Kim A, Kar K, Nowzari H, Cha HS, Ahn KM. Immediate free iliac bone graft after nonsegmental mandibular resection and delayed implant placement: a case series. Implant Dent. 2013;22(5):438–43. https://doi.org/10.1097/ID.0b013e31829f1ed0. PMID: 24013392.
Kim BC, Yoon JH, Choi B, Lee J. Mandibular reconstruction with autologous human bone marrow stem cells and autogenous bone graft in a patient with plexiform ameloblastoma. J Craniofac Surg. 2013;24(4):e409–11. https://doi.org/10.1097/SCS.0b013e318292c91d. PMID: 23851884.
Sándor GK, Tuovinen VJ, Wolff J, Patrikoski M, Jokinen J, Nieminen E, Mannerström B, Lappalainen OP, Seppänen R, Miettinen S. Adipose stem cell tissue-engineered construct used to treat large anterior mandibular defect: a case report and review of the clinical application of good manufacturing practice-level adipose stem cells for bone regeneration. J Oral Maxillofac Surg. 2013;71(5):938–50. https://doi.org/10.1016/j.joms.2012.11.014. Epub 2013 Feb 1. PMID: 23375899.
Levine JP, Bae JS, Soares M, Brecht LE, Saadeh PB, Ceradini DJ, Hirsch DL. Jaw in a day: total maxillofacial reconstruction using digital technology. Plast Reconstr Surg. 2013;131(6):1386–91. https://doi.org/10.1097/PRS.0b013e31828bd8d0. PMID: 23714799.
Natashekar M, Chowdhary R, Chandraker NK. Rehabilitation of recurrent unicystic ameloblastoma using distraction osteogenesis and dental implants. Niger J Clin Pract. 2011;14(4):486–91. https://doi.org/10.4103/1119-3077.91763. PMID: 22248957.
Wang W, Mao CY, Gu XH. Prosthodontic rehabilitation of malpositioned implants after ameloblastoma followed by mandibulectomy and costal bone graft: a clinical report. Implant Dent. 2013;22(1):16–9. https://doi.org/10.1097/ID.0b013e31827afbb0. PMID: 23287980.
Christian J, Grover M, Veeravalli PT. Replacement of mandibular posterior teeth with implants in a postmandibular resection case: a case report. J Oral Implantol. 2013;39(2):210–3. https://doi.org/10.1563/AAID-JOI-D-11-00024. Epub 2011 Sep 9. PMID: 21905914.
Ibric Cioranu V, Iorgulescu D, Petrescu Seceleanu V, Ibric Cioranu S, Toma C, Fronie AI, Făgeţan IM, Nicolae V. Malignant ameloblastoma in an 8-year-old child with metastasis to the lung: case report with a clinicopathologic analysis. Romanian J Morphol Embryol. 2014;55(1):183–7. PMID: 24715186.
Lustosa RM, Macedo Dde V, Iwaki LC, Tolentino Ede S, Hasse PN, Marson GB, Iwaki FL. Continuity resection of the mandible after ameloblastoma - feasibility of oral rehabilitation with rhBMP-2 associated to bovine xenograft followed by implant installation. J Craniomaxillofac Surg. 2015;43(8):1553–60. https://doi.org/10.1016/j.jcms.2015.06.030. Epub 2015 Jun 27. PMID: 26190695.
Askin SB, Aksu AE, Calis M, Tulunoğlu İ, Safak T, Tözüm TF. Report of multidisciplinary treatment of an extensive mandibular ameloblastoma with free iliac crest bone flap, dental implants, and acellular dermal matrix graft. J Oral Implantol. 2015;41(1):107–11. https://doi.org/10.1563/AAID-JOI-D-13-00003. Epub 2013 Mar 18. PMID: 23506101.
Bucci T, Nocini PF. Functional reconstruction of nonsegmental Mandibular defect with fresh frozen bone graft and delayed implants placement. J Craniofac Surg. 2017;28(3):810–2. https://doi.org/10.1097/SCS.0000000000003378. PMID: 28060092.
Ozen J, Erol B, Dikicier S, Alp G. Rehabilitation with an implant-supported metal-acrylic fixed prosthesis after Ameloblastoma resection in mandible: clinical case letter. J Oral Implantol. 2017;43(5):365–9. https://doi.org/10.1563/aaid-joi-D-17-00024. Epub 2017 Aug 25. PMID: 28841384.
Sanz-Alonso J, Martínez-Rodríguez N, Martín-Ares M, Barona-Dorado C, Cortés Bretón-Brinkmann J, Martínez-González JM. Unicystic Ameloblastoma: rehabilitation with Chin graft harvested and implant-supported fixed prosthesis. Oral Implantol (Rome). 2017;10(4):448–56. https://doi.org/10.11138/orl/2017.10.4.448. PMID: 29682262; PMCID: PMC5892667.
Touré G, Gouet E. Use of a 3-dimensional custom-made porous titanium prosthesis for Mandibular body reconstruction with prosthetic dental rehabilitation and Lipofilling. J Oral Maxillofac Surg. 2019;77(6):1305–13. https://doi.org/10.1016/j.joms.2018.12.026. Epub 2018 Dec 31. PMID: 30689966.
Ribeiro-Junior PD, Momesso NR, Padovan LEM, Oreadi D, Matsumoto MA. Immediate Oral rehabilitation using dental implants after marginal Mandibulectomy: a case report. J Oral Implantol. 2020;46(1):73–9. https://doi.org/10.1563/aaid-joi-D-19-00143. PMID: 31815591.
Lee JH, Kim SH, Yoon HI, Yeo IL, Han JS. Implant-assisted removable prosthetic rehabilitation after distraction osteogenesis in a patient with ameloblastoma recurrence: a case report. Medicine (Baltimore). 2019;98(49):e18290. https://doi.org/10.1097/MD.0000000000018290. PMID: 31804373; PMCID: PMC6919522.
Ishihara Y, Arakawa H, Nishiyama A, Kamioka H. Occlusal reconstruction of a patient with ameloblastoma ablation using alveolar distraction osteogenesis: a case report. Head Face Med. 2020;16(1):12. https://doi.org/10.1186/s13005-020-00227-1. PMID: 32487178; PMCID: PMC7265233.
Nag PVR, Bhagwatkar T. Prosthetic management of a hemimandibulectomy patient using tilted implant protocol with 3-year follow-up. J Indian Prosthodont Soc. 2020;20(3):326–30. https://doi.org/10.4103/jips.jips_415_19. Epub 2020 Jul 17. PMID: 33223704; PMCID: PMC7654194.
Niakan S, Yaghoobi N. Oral reconstruction with hybrid implant-supported fixed prostheses in cases of mandibular defect using two methods along with 3 years of follow-up: a case report. Clin Case Rep. 2021;9(9):e04854. https://doi.org/10.1002/ccr3.4854. PMID: 34594553; PMCID: PMC8462366.
Garrido-Martínez P, Peña-Cardelles JF, Pozo-Kreilinger JJ, Esparza-Gómez G, Montesdeoca-García N, Cebrián-Carretero JL. Jaw in a day: Osseointegration of the implants in the patient's leg before reconstructive surgery of a maxilla with ameloblastoma. A 4-year follow-up case report. J Clin Exp Dent. 2021;13(1):e81–7. https://doi.org/10.4317/jced.57823. PMID: 33425236; PMCID: PMC7781221.
Srivastava G, Padhiary SK, Nayak TK, Mishra N. Rehabilitation using implants in free fibula flap of a patient with ameloblastoma: Case report with 4-year follow-up. Natl J Maxillofac Surg. 2022;13(Suppl 1):S194–8. https://doi.org/10.4103/njms.NJMS_239_20. Epub 2022 Aug 20. PMID: 36393960; PMCID: PMC9651219.
Ardila CM, Hernández-Arenas Y, Álvarez-Martínez E. Mandibular body reconstruction utilizing a three-dimensional custom-made porous titanium plate: a four-year follow-up clinical report. Case Rep Dent. 2022;2022:5702066. https://doi.org/10.1155/2022/5702066. PMID: 35251720; PMCID: PMC8896956.
Guimarães LM, Coura BP, Gomez RS, Gomes CC. The molecular pathology of odontogenic tumors: expanding the Spectrum of MAPK pathway driven tumors. Front Oral Health. 2021;2:740788. https://doi.org/10.3389/froh.2021.740788. PMID: 35048058; PMCID: PMC8757814.
Silveira FM, Macedo CCS, Borges CMV, Mauramo M, Vasconcelos ACU, Soares AB, Martinez EF, de Araujo VC, Vered M, Salo T, Passador-Santos F. Odontogenic tumors: an 11-year international multicenter study. Oral Dis. 2021;27(2):320–4. https://doi.org/10.1111/odi.13550. Epub 2020 Aug 31. PMID: 32657453.
Magliocca KR. Proceedings of the 2023 North American Society of Head and Neck Pathology Companion Meeting, New Orleans, LA, March 12, 2023: Odontogenic Tumors: Have We Achieved an Evidence-Based Classification. Head Neck Pathol. 2023;17(2):313–24. https://doi.org/10.1007/s12105-023-01561-x. Epub 2023 Jun 6. PMID: 37278887; PMCID: PMC10293512.
Escobar E, Gómez-Valenzuela F, Peñafiel C, Ortega-Pinto A. Odontogenic tumours in a Chilean population: a retrospective study of 544 cases based on 2022 WHO classification. Med Oral Patol Oral Cir Bucal. 2023;12:26008. https://doi.org/10.4317/medoral.26008. Epub ahead of print. PMID: 37823289.
Kreppel M, Zöller J. Ameloblastoma-clinical, radiological, and therapeutic findings. Oral Dis. 2018;24(1–2):63–6. https://doi.org/10.1111/odi.12702. PMID: 29480593.
Jurado-Castañeda E, Ramírez-Martínez CM, Alonso-Moctezuma A, Páramo-Sánchez JT, Rivera-Reza DI, Chanes-Cuevas OA, Ortiz-Solís CL, Téliz-Meneses MA, Hernández-Ortega OR, Vizzuete-Bolaños MX, Olmedo-Bastidas P, Jacinto-Alemán LF. Conventional Ameloblastoma. A case report with microarray and Bioinformatic analysis. Diagnostics (Basel). 2022;12(12):3190. https://doi.org/10.3390/diagnostics12123190. PMID: 36553196; PMCID: PMC9777305.
Reichart PA, Philipsen HP, Sonner S. Ameloblastoma: biological profile of 3677 cases. Eur J Cancer B Oral Oncol. 1995;31B(2):86–99. https://doi.org/10.1016/0964-1955(94)00037-5. PMID: 7633291.
Kelppe J, Hagström J, Sorsa T, Suominen AL, Apajalahti S, Haglund C, Thorén H. Ameloblastoma: a retrospective single institute study of 34 subjects. Acta Odontol Scand. 2019;77(1):82–7. https://doi.org/10.1080/00016357.2018.1532530. Epub 2018 Nov 7. PMID: 30404552.
Santos Tde S, Piva MR, Andrade ES, Vajgel A, Vasconcelos RJ, Martins-Filho PR. Ameloblastoma in the northeast region of Brazil: a review of 112 cases. J Oral Maxillofac Pathol. 2014;18(Suppl 1):S66–71. https://doi.org/10.4103/0973-029X.141368. PMID: 25364183; PMCID: PMC4211242.
Renapurkar SK, Broccoli P, Carrico C, Glass S. Are incisional biopsies reliable for selecting definitive treatment of ameloblastomas? A 15-year interdisciplinary retrospective study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2022;133(4):388–95. https://doi.org/10.1016/j.oooo.2021.07.008. Epub 2021 Jul 18. PMID: 34511343.
Bwambale P, Yahaya JJ, Owor G, Wabinga H. Histopathological patterns and biological characteristics of ameloblastoma: a retrospective cross-sectional study. J Taibah Univ Med Sci. 2021;17(1):96–104. https://doi.org/10.1016/j.jtumed.2021.09.007. PMID: 35140571; PMCID: PMC8801468.
Dandriyal R, Lal V, Giri KY, Indra Bavanthabettu N, Chaurasia A, Pant S. Ameloblastoma: Retrospective study and analysis of 102 cases over 10 years, single Centre, institutional experience. J Maxillofac Oral Surg. 2022;21(2):730–8. https://doi.org/10.1007/s12663-022-01694-6. Epub 2022 Mar 17. PMID: 35712387; PMCID: PMC9192859.
Evangelou Z, Zarachi A, Dumollard JM, Peoc'h M, Komnos I, Kastanioudakis I, Karpathiou G. Maxillary Ameloblastoma: A Review With Clinical, Histological and Prognostic Data of a Rare Tumor. In Vivo. 2020;34(5):2249–58. https://doi.org/10.21873/invivo.12035. PMID: 32871747; PMCID: PMC7652510.
Ogle OE, Weinstock RJ, Friedman E. Surgical anatomy of the nasal cavity and paranasal sinuses. Oral Maxillofac Surg Clin North Am. 2012;24(2):155–66. https://doi.org/10.1016/j.coms.2012.01.011. vii. Epub 2012 Mar 2. PMID: 22386856.
Nwoga MC. Recurrent tumours of ameloblastoma: Clinicopathologic features and diagnostic outcome. Niger J Clin Pract. 2022;25(9):1529–34. https://doi.org/10.4103/njcp.njcp_82_22. PMID: 36149215.
Kitisubkanchana J, Reduwan NH, Poomsawat S, Pornprasertsuk-Damrongsri S, Wongchuensoontorn C. Odontogenic keratocyst and ameloblastoma: radiographic evaluation. Oral Radiol. 2021;37(1):55–65. https://doi.org/10.1007/s11282-020-00425-2. Epub 2020 Feb 6. Erratum in: Oral Radiol 2021 Oct;37(4):715–717. PMID: 32030659.
Kajla P, Lata J, Aggarwal S. A combination of follicular and plexiform ameloblastoma: A rare case report. Natl J Maxillofac Surg. 2022;13(Suppl 1):S212–5. https://doi.org/10.4103/njms.NJMS_82_16. Epub 2022 Aug 20. PMID: 36393941; PMCID: PMC9651216.
Bi L, Wei D, Hong D, Wang J, Qian K, Wang H, Zhu H. A retrospective study of 158 cases on the risk factors for recurrence in Ameloblastoma. Int J Med Sci. 2021;18(14):3326–32. https://doi.org/10.7150/ijms.61500. PMID: 34400902; PMCID: PMC8364459.
Hresko A, Burtyn O, Pavlovskiy L, Snisarevskyi P, Lapshyna J, Chepurnyi Y, Kopchak A, Karagozoglu KH, Forouzanfar T. Controversies in ameloblastoma management: evaluation of decision making, based on a retrospective analysis. Med Oral Patol Oral Cir Bucal. 2021;26(2):e181–6. https://doi.org/10.4317/medoral.24104. PMID: 33037802; PMCID: PMC7980285.
Ettinger KS, Arce K, Bunnell AM, Nedrud SM. Mandibular reconstruction: when to graft, when to flap, and when to say no. Atlas Oral Maxillofac Surg Clin North Am. 2023;31(2):91–104. https://doi.org/10.1016/j.cxom.2023.03.002. Epub 2023 May 12. PMID: 37500204.
Abbate V, Togo G, Committeri U, Zarone F, Sammartino G, Valletta A, Elefante A, Califano L, Dell'Aversana OG. Full digital workflow for Mandibular Ameloblastoma management: showcase for technical description. J Clin Med. 2023;12(17):5526. https://doi.org/10.3390/jcm12175526. PMID: 37685596; PMCID: PMC10488923.
Ch'ng S, Skoracki RJ, Selber JC, Yu P, Martin JW, Hofstede TM, Chambers MS, Liu J, Hanasono MM. Osseointegrated implant-based dental rehabilitation in head and neck reconstruction patients. Head Neck. 2016;38(Suppl. S1):E321–7.
Shah SA, Irfanullah BM, Shinwari MH, Ahmad A, Ullah E. Mandibular reconstruction with free fibula flap: experience at Hayatabad medical complex, Peshawar. J Islamabad Med Dent Coll. 2019;8:198–202. https://doi.org/10.35787/jimdc.v8i4.374.
Riaz N, Warraich R. Reconstruction of the mandible by a free fibular flap. J Coll Physicians Surg Pak. 2010;20:723–7.
Qayyum Z, Khan ZA, Maqsood A, Prabhu N, Saad Alqarni M, Bader AK, Issrani R, Abbasi MS, Ahmed N, Sghaireen MG, Heboyan A. Outcome assessment after reconstruction of tumor-related Mandibular defects using free vascularized fibular flap-a clinical study. Healthcare (Basel). 2023;11(2):193. https://doi.org/10.3390/healthcare11020193. PMID: 36673561; PMCID: PMC9859578.
Wiesli MG, Fankhauser-De Sousa S, Metzler P, Rohner D, Jaquiéry C. Peri-implant parameters of dental implants inserted in prefabricated microvascular fibular flaps: a retrospective study. Int J Oral Maxillofac Implants. 2023;38(6):1151–60. https://doi.org/10.11607/jomi.9952. Epub ahead of print. PMID: 37672394.
Goker F, Beretta P, Baj A, Bolzoni AR, Maiorana C, Beltramini G, Russillo A, Greco Lucchina A, Rossi DS, Polo MRD, Del Fabbro M, Mortellaro C, Giannì AB. Oral rehabilitation of oncology patients with dental implants after reconstruction surgery with autogenous flaps. Eur Rev Med Pharmacol Sci. 2022;26(3 Suppl):51–61. https://doi.org/10.26355/eurrev_202212_30795. PMID: 36591879.
Wüster J, Sachse C, Sachse C, Rendenbach C, Wagendorf O, Vach K, Preissner S, Heiland M, Nelson K, Nahles S. Vestibuloplasty and its impact on the long-term survival and success of dental implants in irradiated and non-irradiated patients after head and neck tumor therapy: a retrospective study. Clin Oral Investig. 2023;27(8):4695–703. https://doi.org/10.1007/s00784-023-05096-x. Epub 2023 Jun 17. PMID: 37330421; PMCID: PMC10415447.
Strietzel FP, Schmidt-Westhausen AM, Neumann K, Reichart PA, Jackowski J. Implants in patients with oral manifestations of autoimmune or muco-cutaneous diseases - a systematic review. Med Oral Patol Oral Cir Bucal. 2019;24(2):e217–30. https://doi.org/10.4317/medoral.22786. PMID: 30818315; PMCID: PMC6441598.
Mosaddad SA, Abdollahi Namanloo R, Ghodsi R, Salimi Y, Taghva M, Naeimi DM. Oral rehabilitation with dental implants in patients with systemic sclerosis: a systematic review. Immun Inflamm Dis. 2023;11(3):e812. https://doi.org/10.1002/iid3.812. PMID: 36988245; PMCID: PMC10022424.
Tsigarida A, Chochlidakis K. A comparison between fixed and removable Mandibular implant-supported full-arch prostheses: an overview of systematic reviews. Int J Prosthodont. 2021;34:s85–92. https://doi.org/10.11607/ijp.6911. PMID: 33571328.
Al-Sawai AA, Labib H. Success of immediate loading implants compared to conventionally-loaded implants: a literature review. J Investig Clin Dent. 2016;7(3):217–24. https://doi.org/10.1111/jicd.12152. Epub 2015 May 15. PMID: 25976172.
Chen J, Cai M, Yang J, Aldhohrah T, Wang Y. Immediate versus early or conventional loading dental implants with fixed prostheses: a systematic review and meta-analysis of randomized controlled clinical trials. J Prosthet Dent. 2019;122(6):516–36. https://doi.org/10.1016/j.prosdent.2019.05.013. Epub 2019 Aug 14. PMID: 31421892.
Carosi P, Lorenzi C, Di Gianfilippo R, Papi P, Laureti A, Wang HL, Arcuri C, Immediate vs. Delayed placement of immediately Provisionalized self-tapping implants: a non-randomized controlled clinical trial with 1 year of follow-up. J Clin Med. 2023;12(2):489. https://doi.org/10.3390/jcm12020489. PMID: 36675417; PMCID: PMC9861545.
Di Stasio D, Romano A, Gentile C, Maio C, Lucchese A, Serpico R, Paparella R, Minervini G, Candotto V, Laino L. Systemic and topical photodynamic therapy (PDT) on oral mucosa lesions: an overview. J Biol Regul Homeost Agents. 2018;32(2 Suppl. 1):123–6. PMID: 29460529.
Rathi S, Chaturvedi S, Abdullah S, Rajput G, Alqahtani NM, Chaturvedi M, Gurumurthy V, Saini R, Bavabeedu SS, Minervini G. Clinical trial to assess physiology and activity of masticatory muscles of complete denture wearer following vitamin D intervention. Medicina (Kaunas). 2023;59(2):410. https://doi.org/10.3390/medicina59020410. PMID: 36837611; PMCID: PMC9961876.
Qazi N, Pawar M, Padhly PP, Pawar V, D'Amico C, Nicita F, Fiorillo L, Alushi A, Minervini G, Meto A. Teledentistry: evaluation of Instagram posts related to bruxism. Technol Health Care. 2023;31(5):1923–34. https://doi.org/10.3233/THC-220910. PMID: 36872812.
Patil P, Madhav VN, Alshadidi AAF, et al. Comparative evaluation of open tray impression technique: investigating the precision of four splinting materials in multiple implants. BMC Oral Health. 2023;23:844. https://doi.org/10.1186/s12903-023-03583-x.
Alqahtani AR, Desai SR, Patel JR, et al. Investigating the impact of diameters and thread designs on the biomechanics of short implants placed in D4 bone: a 3D finite element analysis. BMC Oral Health. 2023;23:686. https://doi.org/10.1186/s12903-023-03370-8.
Minervini G, Franco R, Marrapodi MM, Mehta V, Fiorillo L, Badnjević A, Cervino G, Cicciù M. The association between COVID-19 related anxiety, stress, depression, temporomandibular disorders, and headaches from childhood to adulthood: a systematic review. Brain Sciences. 2023;13(3):481, Cited 37 times. https://doi.org/10.3390/brainsci13030481.
Cicciù M, Fiorillo L, Cervino G, Habal MB. Bone Morophogenetic Protein Application as Grafting Materials for Bone Regeneration in Craniofacial Surgery: Current Application and Future Directions. Arch Craniofac Surg. 2021;32(2):787–93. Cited 37 times. https://doi.org/10.1097/SCS.0000000000006937.
De Stefano R, Bruno A, Muscatello MR, Cedro C, Cervino G, Fiorillo L. Fear and anxiety managing methods during dental treatments: A systematic review of recent data. Minerva Stomatol. 2019;68(6):317–31. Cited 32 times. https://doi.org/10.23736/S0026-4970.19.04288-2.
Acknowledgments
None.
Funding
No external funding was received.
Author information
Authors and Affiliations
Contributions
Conceptualization, M.A.A.-S. and J.S.B.-R.; methodology, M.A.A.-S-; software, M.A.A.-S.; validation, M.A.A.-S, J.S.B.-R and A.H.; formal analysis, A.H., J.S.B.-R and M.A.A.-S.; investigation, M.A.A.-S and J.S.B.-R resources, A.H; data curation, M.A.A.-S; writing—original draft preparation, M.A.A.-S and J.S.B.-R writing—review and editing, M.A.A.-S, J.S.B.-R, L.Y., S.A.M. and A.H.; visualization, M.A.A.-S and J.S.B.-R supervision, M.A.A.-S, J.S.B.-R and A.H.; project administration, M.A.A.-S, and A.H.. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alarcón-Sánchez, M.A., Becerra-Ruíz, J.S., Yessayan, L. et al. Implant-supported prosthetic rehabilitation after Ameloblastomas treatment: a systematic review. BMC Oral Health 23, 1013 (2023). https://doi.org/10.1186/s12903-023-03765-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03765-7