
Abstract
Objectives
Traumatic dental injury occurs during sports competitions, training, and practice and can be prevented by the use of mouthguards. For this reason, this study aimed to evaluate the knowledge and attitudes of sports science faculty students, physical education teachers, and athletes about mouthguards.
Methods
Five hundred thirty-two participants were reached via social media. In the questionnaire consisting of 20 questions, questions about the sociodemographic characteristics of the participants were asked in part 1, and questions about their level of knowledge and attitudes about the mouthguards were asked in part 2. Descriptive statistical analysis and a chi-square test were used to evaluate the data.
Results
The number of people who think that mouthguards protect the athlete from traumatic dental injury is 381 (71.6%). The number of people who think that mouthguards affect the performance of the athlete is positively 228 (42.9%). To protect against traumatic dental injury, 51.48% of the participants preferred the custom-made; 39.3% of them preferred the boil-bite; 33.22% of them preferred the standard/stock type mouth guard; and 22.96% of them preferred the helmet, and 18.26% of them preferred the face mask.
Conclusions
The knowledge and attitude of sports science faculty students, physical education teachers, and athletes are low about mouthguards. Since these people who are engaged in sports have a high exposure to traumatic dental injuries, education should be given to increase their awareness about mouthguards.
Similar content being viewed by others


Introduction
Physical activities and sports contribute to the physical and mental positive developments of the individual [1]. However, retrospective reviews have reported that traumatic dental injury can be seen in almost one out of every 5 children between the ages of 11–13 in sports activities [2]. It was concluded that more than half of these injuries were seen during the competition and the rest during training [3]. According to the Federation Dentaire International classification, American football, ice hockey, hockey, martial arts, ice skating, skateboarding, lacrosse, rugby, and mountain biking are at high risk in terms of dental trauma, while basketball, socccer, handball, water polo, squash, gymnastics, diving, and, parachuting are at moderate risk [4]. In the meta-analysis including all sports injuries, the sports with the most dentofacial injuries were reported as rugby, basketball, handball, field hockey, and soccer [5].
Since these injuries cause aesthetic, functional, physical, economic, psychological, and social problems in the individual, the use of mouthguards during sports activities becomes meaningful [6]. Dentofacial injury is prevented by absorbing the energy of the incoming impact and reducing the force on the dental hard tissues [7, 8], mandibular condyle, and articular disc [9, 10]. Positive results of using a mouthguard on protection and performance have been seen in many studies [3, 11]. Contact athletes are advised to use safety equipment such as mouthguards to minimize impacts [12]. In general, there are 3 types of mouthguards: standard/stock, boil-bite (mouth-formed), and specially prepared by the dentist (custom-made). Properly fitted mouthguards absorb the high energy from traumatic blows, preventing the transfer of energy directly to the underlying teeth [7]. It has been reported that improper use of standard/stock and boil-bite may affect some problems such as discomfort, speech, and breathing problems [13, 14] and adversely affect exercise [15, 16]. On the other hand, it has been reported that a mouthguard specially prepared by a well-adapted dentist does not impair general sports activities and/or performance [15, 17, 18], has a negligible effect on cardiorespiratory endurance, and does not impair respiratory function [19,20,21], does not affect speech, does not cause nausea and has a longer service life [22, 23]. In the literature, there are some studies which are about the poor level of awareness for the prevention and emergency management of traumatic dental injuries and the use of mouthguards [24,25,26]. Accordingly, this study aims to evaluate the knowledge and attitudes of sports science faculty students, physical education teachers, and athletes about mouthguards.
Methods
The study ethics committee was taken from the Kahramanmaraş Sütçü İmam University’s Non-Interventional Clinical Research Ethics Committee (2021/14).
A total of 532 participants, including sports science faculty students, physical education teachers, and athletes, were included in the study via Google form. The questionnaires of that study were developed from former articles [14, 27, 28]. The study has a total of 20 questions, and there are total of 7 questions (1–7), including age, gender, educational status, sports branch they are interested in, their position and status in sports, and professional experience in the first part. In the second part, there are a total of 13 questions (8–20) about mouthguard and sports dentistry. The responses to questions are based on multiple-choice and ‘yes/no/dont’ know’. After answering the questions, the authors which are one pediatric dentist and two sports scientists determined the ingredient validity of the questionnaire. The reliability of the questionnaire was evaluated with a test–retest approach to a total of 15 participants, 5 participants from each group, with an interval of 10 days. Subsequently, these participants were not included in the work. The kappa coefficient was between 0.78 to 0.83 for several questions indicating a good test–retest reliability [29].
For the calculation of the statistical analysis, the Jamovi statistical program (Version: 2.3.28) was used. The frequency of the participants according to demographic characteristics was calculated, and descriptive statistics were made. The answers to the questions about trauma were examined by chi-square analysis according to age, gender, and education level. Significance was set as p < 0.05.
Results
Five hundred thirty-two people, including 160 females (30%) and 372 males (70%), participated in the study. 26% of the participants were 18–20; 53% of them were 21–30; 12% of them were 31–40; and 8.8% of them were 40 years of age or older. Of the participants, 306 (58%) were sports science faculty students; 142 (27%) were physical education teachers; 84 (16%) were athletes. The sports branches that the participants are interested in are respectively as follows: 141 (27%) football, 66 (12%) basketball, 64 (12%) volleyball, 58 (11%) wrestling, 49 (9.2%) swimming, 41 (7.7%) athletics, 28 (5.3%) boxing, 20 (3.8%) taekwondo, 15 (2.8%) handball and none, 14 (2.6%) skiing, 11 (2.1%) amateur kickboxing, 4 (0.8%) ice hockey, 1 (0.2%) water polo. Of the participants, 381 (72%) were amateurs, and 151 (28%) were professionals. Participants with 1–5 years of professional experience are 166 (31%); those with 6–10 years are 164 (31%), and those with more than 10 years are 202 (38%) (Table 1).
There were 137 (25.8%) people with a previous history of trauma in sports dentistry. While there was a statistically significant difference between gender and trauma history (p = 0.037), there was no statistically significant difference between age and education levels (p = 0.093 and 0.104) (Table 2). The number of people who think that the mouthguards affect the performance of the athlete is 228 (42.9%) positively. While there was a statistically significant difference between gender and the belief that the mouthguards affected the athlete’s performance positively (p = 0.023), there was no statistically significant difference between age and education levels (p = 0.083 and 0.319) (Table 2). The number of people who previously knew about mouthguards was 156 (29.3%). The number of people who like to have more information about mouthguards is 354 (66.5%). While a statistically significant difference was observed in terms of age and gender in the respondents to this question (p = 0.011 and 0.046), there was no significant difference in terms of the education levels of the participants (p = 0.124) (Table 2). In avulsion injury, 200 people (37.6%) preferred treatment in the emergency department, 308 people (57.9%) in the dentist, and 24 (4.5%) at the scene. While there was a statistically significant difference in terms of age and treatment of avulsion injury (p = 0.013), there was no difference in terms of gender and education level (p = 0.59 and 0.073) (Table 2).
Participants listed the disadvantages of mouthguarding with multiple responses, to which they may respond more than once, as follows: 50.78% of participants reported discomfort; 43.13% reported breathing problems, 35.48% reported nausea; 28.7% reported dry mouth; 16.87% reported not providing adequate protection; 15.48% reported smell; 13.22% reported cost; 10.61% reported speaking; 9.22% reported problems accessing the material (Fig. 1).

Disadvantages of the mouthguards
Participants discussed the advantages of the mouthguards with multiple responses respectively: 72.87% of them reported protecting the tooth crown and root, 43.83% of them reported protecting soft tissues such as lips and tongue, 43.48% of them reported preventing aesthetic, psychological, and economic losses, 40.87% of them reported preventing jaw bone and head injury, and 24% of them reported preventing teeth that had not erupted or were in progress (Fig. 2).

Advantages of the mouthguards
Participants responded to the question about the sport branch that requires the need for mouthguards, to which they can give more than one response, as follows; 72.35% of them as amateur kickboxing, 66.96% of them as taekwondo, 64.87% of them as karate, 53.22% of them as boxing, 33.91% of them as basketball, 30.61% of them as ice hockey, 22.96% of them as wrestling, 19.13% of them as football, 15.48% of them as handball, 13.04% of them as skiing, 6.96% of them as volleyball, 4.87% of them as water polo, 2.26% of them as athletics, and 1.74% of them swimming (Fig. 3).

Do you think that which sports require using the mouthguards?
Participants listed the branches with the obligation to use mouthguards, to which they can give more than one response, as follows; 78.09% of them as amateur kickboxing, 56.17% as karate, 54.09% as boxing, 53.57% as taekwondo, 16.17% as ice hockey, 15.3% as wrestling, 11.13% as basketball, 5.74% as football, 4.87% as skiing, 3.3% as handball, 2.78% as volleyball, 1.39% as athletics and water polo (Fig. 4).

Do you think that which sports have obligation about using mouthguards in our country?
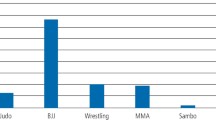
To protect against traumatic dental injury, 51.48% of the participants preferred the custom-made; 39.3% of them preferred the boil-bite; 33.22% of them preferred the standard /stock type mouthguard; and 22.96% of them preferred the helmet; and 18.26% of them preferred the face mask (Fig. 5).

Dou you think that which method may be used to protect against traumatic dental injury?
Discussion
Athletes, coaches, athletic directors, families, doctors and dentists should be aware of the risk, history, and treatment of dental injuries in individuals who play, train, and practice sports. These individuals have a good command of the type and treatment of orofacial injuries treat the athlete during the competition and contribute to the continuity of the game [30]. Thus, the physical and psychological damage that will be created in the athlete is minimized [31]. This study aimed to measure the awareness of sports science faculty students, physical education teachers, and athletes about mouthguards.
The American Academy of Pediatric Dentistry (AAPD) states that falls, bumps, hard surfaces, and contact with sports-related equipment pose a risk of orofacial injury in all sports activities. Most of these injuries are prevented by the use of mouthguards, face masks, and helmets [32].
When the studies in the literature are examined, the participants with a previous history of trauma vary between 17.5-83% [14, 33,34,35], while, in this study, this rate is low (25.8%). Similar to this study, this rate is 22.3% in the study conducted by Tulunoğlu and Özbek [36]. In this study, male exposed to trauma in a similar way to a study by Özbay et al. [37] were statistically significantly higher than female (p = 0.037) (Table 2). This result may be related to the fact that male reflects their strong physical structure to the sports competition. In a study, although it was reported that males had more injuries than females, it was found that injuries in females resulted in more surgeries [38]. On the other hand, Traebert et al. [39] argued that females have similar risk factors for orofacial injuries as male. Another interesting result found in this study is that although there is no statistically significant difference between age and trauma history (p = 0.093) (Table 2), similar to Tulunoglu and Ozbek [36]’s study, the trauma history of the participants increases as they get older. The history of trauma may have also increased, possibly as the number of sports competitions experienced increased as individuals got older. On the other hand, in the study conducted by Esmaeilpoor et al. [14], it was reported that young athletes had a higher history of trauma than older people. Also, sports-related orofacial injury is associated with multiple components like the kind of sport, geographical location, specimen size, age, level of match, requirements for the use of safety equipment, and duration of exposure [4, 40, 41].
In the study by Sepet et al. [33], Galic et al. [42] and Elareibi et al. [25] 55.4%, 97.3% and 89.4% of the participants knew that they should use mouthguards, respectively; only 11.2% of participants, 41% and 14.8% of them used mouthguards. Similarly, in our study, although most of the participants knew that they should use mouthguards (71.6%), very few chose to use them (14.8%) (Table 2). When the studies conducted in Turkey are examined, the rate of mouthguards use is 0–55.8% [27, 36, 37]. On the other hand, the study conducted by Vidovic-Stesevic et al. [43] included 420 athletes, and 98% reported using mouthguards.
Protective equipment provided to children interested in football, lacrosse, and ice hockey has been observed to significantly reduce dental and facial injuries. Sports such as baseball, basketball, football, softball, wrestling, volleyball, and gymnastics are insufficient to protect boys and girls from injury. Young people who participate in free activities such as skateboarding, skating, and cycling use more protective equipment [44,45,46]. In this study, in the multiple-choice question related to sports requiring the need for mouthguards, the most answers were given to close contact sports such as 72.35% amateur kickboxing, 66.96% taekwondo, 64.87% karate, and 53.22% boxing respectively, and the least responses were given to sports such as 1.74% swimming, 2.26% athletics and 4.87% water polo (Fig. 3). Differences in the rates of mouthguards use may be related to the study group’s age, education level, and the sport they are interested in (team sport or individual sport).
According to an interesting result found in this study, 51.48% of the participants preferred the custom-made, 39.3% preferred the boil-bite, 33.22% preferred the standard/stock type mouth guard (Fig. 5). In some studies, in the literature, mouthguards shaped in the mouth were preferred [27, 36], while there were also participants who preferred the stock type [14]. In our study, the participants preferred custom-made mouthguards (51.48%). AAPD recommends custom-made mouthguards for all sports activities due to the risk of traumatic dental injury [32].
In this study, the participants stated the feeling of discomfort as the most common disadvantage of using mouthguards, which is a multiple-choice question (Fig. 1), and this result is consistent with the literature [47,48,49]. Nevertheless, since screaming in combat sports contributes to the physical and mental motivation of the athlete during the competition, the use of mouthguards can be considered a disadvantage [36]. In some studies, athletes have reported that stock or mouth-formed mouthguards cause breathing and speech problems or jaw and muscle fatigue, but this problem is solved by custom-made mouthguards that adapt well to the gums and teeth [48,49,50,51,52].
In the study conducted by Yeşil Duymuş and Gungor [28] and Cetınbas and Sönmez [27], 78% and 95.5% of the participants liked to have more about mouthguards; in this study, this rate was 66.5%. Since pediatric dentistry is the branch of dentistry that deals with children and adolescents with a higher frequency of trauma, it supports directing athletes and coaches to raise more awareness about mouthguards. The National Association of Athletics Coaches recommends that coaches be trained in the use of a properly placed mouthguard and that athletes should participate in activities associated with the risk of orofacial injury [53]. Thus, athletes will adopt the mouthguard and reflect it in routine use [24, 38]. Regarding the question of which branch should be used as mouthguard in Turkey, 78.09% of participants answered as kickboxing, 56.17% as karate, and 54.09% as boxing (Fig. 4). Similar to the General Directorate of Youth Sports [54], in this study, the necessity of using mouthguards in sports related to direct contact was more accepted. Due to the increasing number of athletes around the world, dental trauma is an important dental health problem. For this purpose, sports committees need to regulate the use of mouthguards as mandatory protective equipment. It makes sense for dentists to encourage the use of customizing mouthguards for athletes [24]. This protects the athlete from orofacial injury and contributes to the quality of life of the athlete due to its aesthetic, speech, economic and psychological effects.
Limitations
In the study in question, the participants were asked questions in the form of Google surveys, and social networks such as WhatsApp, e-mail, Facebook, and Instagram were also tried to reach participants. Conducting a face-to-face survey can make participants more willing. In addition, this led to data loss, and some participants were excluded from the study because they did not respond to every question. The study data were obtained only from participants in Turkey, and the inclusion of international athletes may increase the scope of the study.
Conclusion
The results of the study have revealed that there was not enough knowledge about the use of mouthguards. The use of mouthguards should not be left to personal preference, as it may make a difference in the quality of life of the athlete. For this purpose, the use of mouthguards should be mandatory in medium-risk sports as well as high-risk sports. To create oral protective awareness of physical education teachers and athletes against injuries in sports dentistry, it may be necessary to provide training on this subject in the faculty of sports science to put courses in the curriculum and to organize symposiums with posters and videos.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- AAPD:
-
American Academy of Paediatric Dentistry
References
Liu T, Li D, Yang H, Chi X, Yan J. Associations of sport participation with subjective well-being: a study consisting a sample of Chienese school-attending students. Front Publich Health. 2023;11:1199782.
Petti S, Glendor U, Andresson L. World traumatic dental injury and incidence, a meta-analysis-one billion living people have had traumatic dental injuries. Dent Traumatol. 2018;34:71–86.
Azadani EN, Peng J, Townsend JA, Collins CL. Traumatic dental injuries in high school athletes in the United States of America from 2005 to 2020. Dent Traumatol. 2023;39:109–18.
Glendor U. Aetiology and risk factors related to traumatic dental injuries-a review of the literature. Dent Traumatol. 2009;25:19–31.
Oliveira Werlich M, Honnef LR, Silva Bett JV, Luiz Domingos F, Pauletto P, et al. Prevalence of dentofacial injuries in contact sports players: a systematic review and meta-analysis. Dent Traumatol. 2020;36:477–88.
Tuna EB, Ozel E. Factors affecting sports-related orofacial injuries and the importance of mouthguards. Sports Med. 2014;44:777–83.
Parker K, Marlow B, Patel N, Gill DS. A review of mouthguards: effectiveness types, characteristics and indications for use. Br Dent J. 2017;222:629–33.
Bochnig MS, Oh M-J, Nagel T, Ziegler F, Jost-Brinkmann P-G. Comparison of the shock absorption capacities of different mouthguards. Dent Traumatol. 2017;3:205–13.
Tribst JPM, Dal Piva AMO, Bottino MA, Kleverlaan CJ, Koolstra JH. Mouthguard use and TMJ injury prevention with different occlusions: a three-dimensiol finite element analysis. Dent Traumatol. 2020;36:662–9.
Tanaka Y, Tsugawa T, Maeda Y. Effect of mouthguards on impact to the craniomandibular complex. Dent Traumatol. 2017;33:51–6.
Starr CL, McGrew C. TMJ disorders in athletes. Curr Sports Med Rep. 2023;22:10–4.
Ahmed I, Fine P. ‘Injury prevention versus performance’:has the time come to mandate the use of mouthguards in all contact sports? BMJ Open Sport Exerc Med. 2021;7:e000828.
Queiróz AFVR, de Brito Jr RB, Ramacciato JC, Motta RHL, Flório FM. Influence of mouthguards on the physical performance of soccer players. Dent Traumatol. 2013;29:450–4.
Esmaeilpoor A, Mohebbi SZ, Moghadam N, Ahmadian M, Razeghi S, et al. Self-reported experience of orofacial injury, preventive practice, and knowledge of Iranian adolescent martial art athletes towards sports-related orofacial injuries. BMC Sports Sci Med Rehabil. 2021;13:134.
Lässing J, Falz R, Schulze A, Pökel C, Vondran M, et al. Decreased exercise capacity in young athletes using self-adapted mouthguards. Eur J Appl Physiol. 2021;121:1881–8.
Fronza HP, Stolf SC, Taguchi CMC, Coto NP, Padilha ACL. Determinants for traumatic orofacial injuries in sport: extrinsic factors in scoping review. Dent Traumatol. 2020;36:598–606.
Drum SN, Swisher AM, Buchanan CA, Donath L. Effects of a custom bite-aligning mouthguard on performance in collage football players. J Strength Cond Res. 2016;30:1409–15.
Ferreira GB, Guimaraes LS, Fernandes CP, Dias RB, Coto NP, et al. Is there enough evidence that mouthguards do not affect athletic performance? A systematic literature review. Int Dent J. 2019;69:25–34.
Mańka-Malara K, Zelik-Świech D, Jagielska A, Kozłowska A, Łuniewska M, et al. The impact of mouhguards usage on aerobic capacity of athletes. J Stoma. 2019;4:167–71.
Raimundo JAG, Pires KM, Padilha ACL, Penteado R, Lisbôa FD, et al. Influence of occlusal thickness of custom-made mouthguards on ventilatory parameters, rate of perceived exertion, and peak velocity attained during an incremental test. Kinesiology. 2019;2:246–52.
Piero M, Simone U, Jonathan M, Maria S, Giulio G, et al. Influence of a custom-made maxillary mouthguard on gas exchange parameters during incremental exercise in amateur road cyclists. J Strength Cond Res. 2015;29:672–7.
Vuvic S, Drost RW, Ongkosuwito EM, Wolvius EB. Dentofacial trauma and players’ attitude towards mouthguard use in field hockey: a systematic review and meta-analysis. Br J Sports Med. 2016;50:298–304.
Chowdhury RU, Churei H, Tanabe G, Yoshida Y, Hayashi K, et al. Useful design of custom-made mouthguard for athletes undergoing orthodontic treatment with brackets and wires. J Dent Sci. 2022;17:308–15.
Fernandes LM, Neto JCL, Lima TF, Magno MB, Santiago BM, et al. The use of mouthguards and prevalence of dento-alveolar trauma among athletes: A systematic review and meta-analysis. Dent Traumatol. 2019;35:54–72.
Elareibi I, Fakron S, Gaber A, Lambert M, Tantawi ME, et al. Awareness of sports-related dental emergencies and prevention practices among Libyan contact sports coaches: A cross-sectional study. Health Sci Rep. 2022;6:e977.
Knapik JJ, Hoedebecke BL, Rogers GG, Sharp MA, Marshall SW. Effectiveness of mouthguards for the prevention of orofacial injuries and concussions in sports: systematic review and meta-analysis. Sports Med. 2019;49:1217–32.
Cetınbas T, Sonmez H. Mouthguard utilization rates during sport activities in Ankara. Turkey Dent Traumatol. 2006;22:127–32.
Yeşil Duymuş Z, Gungor H. Use of mouthguard rates among university athletes during sport activities in Erzurum. Turkey Dent Traumatol. 2009;25:318–22.
McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012;22:276–82.
Cohenca N, Roges RA, Roges R. The incidence and severity of dental trauma in intercollegia athletes. J Am Dent Assoc. 2007;138:1121–6.
Andreasen JO, Andreasen FM, Andersson L (Eds.). Textbook and Color Atlas of Traumatic Injuries to the Teeth. 5th ed. John Wiley & Sons; 2018.
American Academy of Pediatric Dentistrty. Policy on prevention of sports-related orofacial injuries 2021. https://www.aapd.org/media/policies_guidelines/p_sports.pdf. Accessed 20 Apr 2021.
Sepet E, Aren G, Dogan Onur O, Erdem Pınar A, Kuru S, et al. Knowledge of sports participants about dental emergency procedures and the use of mouthguards. Dent Traumatol. 2014;30:391–5.
Mori GG, de Mendonça Janjáacomo DM, Castilho LR, Poi WR. Evaluating the knowledge of sports participants regarding dental emergency procedures. Dent Traumatol. 2009;25:305–8.
Iglesias-Porqueras N, Zamora-Olave C, Williart E, Martinez-Gomis J. Attitudes and opinions towards the prevention of orofacial injuries among water polo coaches in Catalonia: a cross-sectional study. Dent Traumatol. 2021;37:623–30.
Tulunoglu I, Ozbek M. Oral trauma, mouthguard awareness, and use in two contact sports in Turkey. Dent Traumatol. 2006;22:242–6.
Ozbay G, Bakkal M, Abbasoglu Z, Demirel S, Kargul B, et al. Incidence and prevention of traumatic injuries in paediatric handball players in Istanbul. Turkey Eur Arch Paediatr Dent. 2013;14:41–5.
Schneider S, Seither B, Tönges S, Schmitt H. Sports injuries: population based representative data on incidence, diagnosis, sequale, and high risk groups. Br J Sports Med. 2006;40:334–9.
Traebert J, Bittencourt DD, Peres KG, Peres MA, De Lacerda JT, et al. Aetiology and rates of treatment of traumatic dental injuries among 12-year-old school children in a town in southern Brazil. Dent Traumatol. 2006;22:173–8.
Tsuchiya S, Tsuchiya M, Momma H, Sekiguchi T, Kuroki K, et al. Factors associated with sports-related dental injuries among young athletes:a cross-sectional study in Miyagi prefecture. BMC Oral Health. 2017;17:168.
Zaleckienė V, Pečiulienė V, Aleksejuniené J, Drukteinis S, Brukienė V. Dental trauma experience, attitudes and prevention in 11-to 13-year-old Lithuanian schoolchildren. Oral Health Prev Dent. 2020;18:373–8.
Galic T, Kuncic D, Pericic PT, Galic I, Mihanovic FF, et al. Knowledge and attitudes about sports-related dental injuries and moutguard use in young athletes in four different contact sports-water polo, karate, taekwondo and handball. Dent Traumatol. 2018;34:175–81.
Vidovic-Stesevic V, Verna C, Krastl G, Kuhl S, Filippi A. Facial and dental injuries facial and dental injuries in karate. Swiss Dent J. 2015;125:810–4.
Feletti F, Brymer E. Pediatric and adolescent injury in skateboarding. Res Sports Med. 2018;26:129–49.
O’Mahony-Menton C, Willmore J, Russell K. The implemention of a municipal indoor ice shating helmet policy: effects on helmet use, participation and attitudes. Inj Prev. 2015;21:425–31.
Fasciglione D, Persic R, Pohl Y, Fillippi A. Dental injuries in inline skating – level of information and prevention. Dent Traumatol. 2007;23:143–8.
Boffano P, Boffano M, Gallesio C, Roccia F, Cignetti R, et al. Rugby athletes’ awareness and compliance in the use of mouthguards in the North West of Italy. Dent Traumatol. 2012;28:210–3.
Vidovic D, Bursac D, Skrinjaric T, Glavina D, Gorseta K. Prevalence and prevention of dental injuries in young taekwondo athletes in Croatia. Eur J Paediatr Dent. 2015;16:107–10.
Lee J-W, Heo C-K, Kim S-J, Kim G-T, Lee D-W. Mouthguard use in Korean Taekwondo athletes-awareness and attitude. J Adv Prosthodont. 2013;5:147–52.
Rouhani A, Akbari M, Ghoddusi J, Rahmandust M. Knowledge of sports-men and coaches about dental trauma in 2011 in Mashhad. J Isfahan Dent Sch. 2015;11:239–47.
Zamora-Olave C, Willaert E, Parera L, Riera-Puñet N, Martinez-Gomis J. Experience with mouthguards and prevalence of orofacial injuries among field hockey players in Catalonia. Dent Traumatol. 2020;36:285–90.
Bergman L, Milardović Ortolan S, Žarković D, Viskić J, Jokić D, et al. Prevalence of dental trauma and use of mouthguards in Professional handball players. Dent Traumatol. 2017;33:199–204.
Gould TE, Piland SG, Caswell SV, Ranalli D, Mills S, et al. National athletic trainers’ association position statement: preventing and managing sport-related dental and oral injuries. J Athl Train. 2016;51:821–39.
Coşkun AG. Mouthguards Used Against Sport Injuries. EÜ Dişhek Fak Derg. 2007;28:9–17.
Acknowledgements
We thank our participants for to be included to our work.
Funding
There is no funding.
Author information
Authors and Affiliations
Contributions
A.SO., H.E. and C.A. wrote the main manuscript and its revision. H.E and C.A. sent to the questions to the participants. A.SO. prepared the all figures and tables and its revision. A.SO. and H.E. checked the references and its revision. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study and all its experimental protocols were approved by the Kahramanmaraş Sütçü İmam University’s Non-Interventional Clinical Research Ethics Committee (2021/14). A written informed consent form was obtained from all subjects and/or their legal guardians.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Soğukpınar Önsüren, A., Eroğlu, H. & Aksoy, C. Faculty of sports science students, physical education teachers, and athletes’ level of knowledge and attitude about mouthguards. BMC Oral Health 24, 57 (2024). https://doi.org/10.1186/s12903-023-03675-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03675-8