
Abstract
Background
There are differences in vitamin D levels between periodontitis and healthy individuals, but the effect of vitamin D on periodontitis is controversial. The purpose of this Meta-analysis is twofold: (1) compare vitamin D levels in individuals with or without periodontitis; (2) assess the effects of vitamin D supplementation during scaling and root planing (SRP) on periodontal clinical parameters in individuals with periodontitis.
Methods
A systematic search was conducted in five databases (PubMed, Web of Science, MEDLINE, EMBASE, and Cochrane library), published from the database inception to 12 September 2022. The Cochrane Collaboration Risk of bias (ROB) assessment tool, the risk of bias in non-randomized studies of intervention (ROBINS-I) tool, the Newcastle–Ottawa Quality Assessment Scale (NOS), and Agency for Healthcare Quality and Research (AHRQ) were used to evaluate randomized controlled trial (RCT), non-RCT, case–control study, and cross-sectional study, respectively. Statistical analysis was performed using RevMan 5.3 and Stata 14.0 software, with weighted mean difference (WMD), standardized mean difference (SMD) and 95% confidence intervals (CI) as the effect measures, and heterogeneity was tested by subgroup analysis, sensitivity analysis, Meta-regression.
Results
A total of 16 articles were included. The results of Meta-analysis showed that periodontitis was associated with lower serum vitamin D levels compared to normal population (SMD = -0.88, 95%CI -1.75 ~ -0.01, P = 0.048), while there was no significant difference in serum or saliva 25(OH)D levels between periodontitis and normal population. Additionally, the Meta-analysis showed that SRP + vitamin D and SRP alone had a statistically significant effect on serum vitamin D levels in individuals with periodontitis (SMD = 23.67, 95%CI 8.05 ~ 32.29, P = 0.003; SMD = 1.57, 95%CI 1.08 ~ 2.06, P < 0.01). And SRP + vitamin D could significantly reduce clinical attachment level compared to SRP alone (WMD = -0.13, 95%CI -0.19 ~ -0.06, P < 0.01), but had no meaningful effect on probing depth, gingival index, bleeding index, respectively.
Conclusion
The evidence from this Meta-analysis suggests that the serum vitamin D concentration of individuals with periodontitis is lower than that of normal people, and SRP along with vitamin D supplementation has been shown to play a significant role in improving periodontal clinical parameters. Therefore, vitamin D supplementation as an adjuvant to nonsurgical periodontal therapy has a positive impact on the prevention and treatment of periodontal disease in clinical practice.
Similar content being viewed by others


Introduction
Periodontitis is a chronic infectious disease caused by microorganisms in dental plaque, which can lead to inflammation and the progressive destruction of the periodontal support tissues [1, 2]. A guide issued by the World Health Organization (WHO) in 2021 showed that more than 3.5 billion people suffered from oral disease in 2017, and severe periodontal disease, which is estimated to be detrimental to 796 million people, especially the elderly, has emerged as the leading cause of tooth loss [3, 4]. The reason is that bacteria in periodontal pockets can induce an immune response that leads to gingival inflammation, periodontal pocket formation, attachment loss, and alveolar bone resorption, ultimately resulting in tooth loss and oral dysfunction [5, 6]. In addition, evidence has shown that the potential risk factors for periodontitis include certain systemic factors, such as hormones, diabetes, stress, genetic susceptibility, tobacco use, alcohol consumption, dietary patterns, and reduced intake of certain nutrients apart from oral factors [7, 8].
Vitamin D is an essential nutrient and precursor hormone that plays an important role in numerous biochemical functions in the body [9]. It is a lipid-soluble vitamin that is mainly ingested in the form of vitamin D2 and D3 via dietary intake and exposure to sunlight. Both forms of vitamin D are metabolized and activated to 25-hydroxyvitamin D (25(OH)D) in the liver, and subsequently converted to the active form of vitamin D, 1, 25-dihydroxyvitamin D3 (1,25(OH)2D3), in the kidney. As the main circulating metabolite in the blood, 25(OH) D is the most representative indicator of vitamin D storage in the human body [10, 11]. Vitamin D deficiency has become a significant public health issue worldwide [12]. Studies have found that low levels of vitamin D can lead to an increased risk of periodontitis [13]. This may be due to vitamin D playing an important role in maintaining calcium and bone homeostasis as well as immune function, it is inferred that vitamin D may affect the development of periodontitis by the regulation of bone metabolism and immunological reaction [14].
Previous studies have compared vitamin D levels in individuals with and without periodontitis, however, the results remain controversial [15,16,17]. Most studies have shown that periodontitis was associated with lower vitamin D levels compared with non-periodontitis [18,19,20], while other studies have revealed no correlation among them [21, 22]. In addition, the existing systematic reviews of vitamin D and periodontitis mainly focus on polymorphisms of the vitamin D receptor with periodontal susceptibility [23, 24]. Lack of studies on the quantitative synthesis of vitamin D in individuals with and without periodontitis, and regarding the recent increase in studies of vitamin D as an adjunct to scaling and root planing (SRP) on periodontal outcome indicators, both observational and interventional. Hence, the aim of this Meta-analysis is twofold, to compare vitamin D levels in individuals with or without periodontitis, and to evaluate the effects of SRP + vitamin D on periodontal clinical parameters in individuals with periodontitis.
Materials and methods
The systematic review and Meta-analysis was reported by following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guideline.
Search strategy and data sources
Five electronic databases including PubMed, Web of Science, MEDLINE, EMBASE, and the Cochrane library were searched from the inception of the database until september 12, 2022. And the search was carried out by means of subject headings combined with free text words to encompass all articles related to administration of vitamin D and periodontal non-surgical treatment. The specific search strategy was (“periodontitis OR periodontal disease* OR periodontal OR gum disease* OR gingivitis OR chronic periodontitis OR periodontal infection* OR periodontal health”) and (“vitamin D OR 25-hydroxy-vitamin OR Twenty five-hydroxy vitamin D OR 25OHD OR 25-hydroxyvitamin D OR 25(OH)D OR calcitriol OR vitamin D supplementation OR vitamin D deficiency OR vitamin D receptor OR VDR”). In addition, the reference lists of all selected articles were also reviewed for potentially relevant studies.
Inclusion and exclusion criteria
Inclusion criteria: (a) Type of studies: human experimental studies (randomized controlled trial (RCT)/non-RCT/observational studies). (b) Subjects: individuals with periodontitis. (c) Intervention or exposure factors: SRP or SRP + vitamin D. (d) Outcome measures: periodontal clinical parameters, including probing depth (PD), clinical attachment level (CAL), gingival index (GI), and bleeding index (BI); vitamin D indicators, including serum/saliva vitamin D levels or serum/saliva levels of 25(OH)D.
Exclusion criteria: (a) Animal studies or vitro studies. (b) Review or Meta-analysis. (c) Case reports or conference papers. (d) Duplicate publication. (e) Combined with other systemic diseases. (f) Pregnant and lactating women. (g) Qualitative research. (h) Incomplete data and the original articles could not be found.
Data extraction
Based on the inclusion and exclusion criteria, two reviewers independently screened the literature and extracted the data (FF. Liang & YZ. Zhou). In the event of disagreement, a third author was consulted for confirmation (Z. Zhang). The extracted data included: first author, publication year, study time, country, age, gender, sample size, study design, periodontitis diagnostic criteria, periodontitis severity, interventions, influence/ confounding factor, follow-up time, and outcome.
Quality and risk-of-bias assessments
Two researchers independently evaluated and cross-checked the literature (FF. Liang & YZ. Zhou), and the Cochrane Collaboration Risk of bias (ROB) assessment tool was used for RCT. It consists of six aspects with seven elements: selection (random sequence production and allocation concealment), implementation (blinding of participants and personnel), measurement (blinding of outcome assessment), follow-up (incomplete outcome data), report (selective outcome reporting) and other bias, every item was classified as "low risk of bias", "high risk of bias" and "unclear" [25]. The risk of bias in non-randomized studies of intervention (ROBINS-I) tool was used for assessing non-RCT. It included seven dimensions, pre-intervention (confounding bias, selection of participants bias), in-intervention (intervention classification bias), and post-intervention (deviation from intended intervention bias, missing data bias, outcome measurement bias, and selection of reported result bias), every item was classified as “low risk”, “moderate risk”,“serious risk”, “critical risk” and “no information” [26].The NOS was used for case–control studies. It is an 8-items scale with 3 dimensions including selection, comparability, and exposure, and the maximum score of the scale is nine [27]. The AHRQ composed of 11 items was used to assess the quality of cross-sectional studies, and responses to each item were "yes," "no," or "unclear," and only one point was scored for yes, and all other responses were 0. A third researcher was consulted in case of disagreement (Z. Zhang).
Statistical analysis
Revman 5.3 software (Review Manager (RevMan), The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen) and Stata 14.0 software (StataCorp, College Station, TX, USA) were used to statistical analysis. Categorical data were combined by relative risk (RR) or odds ratio (OR), and quantitative data were combined by weighted mean difference (WMD) or standardized mean difference (SMD). Heterogeneity was tested by Q test and I2 analysis. In the chi-square test, P ≤ 0.10 was considered as heterogeneity. In the I2 test, when the I2 value was 25%, 50% and 75%, it was suggested low, moderate and high heterogeneity among studies [28]. According to the Cochrane handbook, significant heterogeneity was considered to exist if I2 ≥ 50% [29]. Therefore, in the present study, if P < 0.10 and I2 < 50%, it was considered that there was no significant heterogeneity, the fixed effects model was used for analysis. On the contrary, the random effect model was used to merge, and further subgroup analysis and sensitivity analysis were used to find the source of heterogeneity.
Results
Literature search
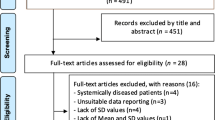
One thousand seven hundred twenty literatures were retrieved from five electronic databases, and 16 literatures [17, 22, 30,31,32,33,34,35,36,37,38,39,40,41,42,43] were finally included. The literature screening process is shown in Fig. 1.

Flow diagram of the study selection
Study characteristics
A total of 16 articles [17, 22, 30,31,32,33,34,35,36,37,38,39,40,41,42,43] with 1455 subjects were included in this study. There were five intervention studies (two RCTs, three non-RCTs) [33, 36, 39,40,41], nine case–control studies [17, 22, 30,31,32, 34, 35, 38, 43], and two cross-sectional studies [37, 42]. The basic characteristics of the included literature are shown in Tables 1 and 2.
Quality assessment
The NOS scores of the nine case–control studies [17, 22, 30,31,32, 34, 35, 38, 43] ranged from 7 to 9, and the AHRQ scores ranged from 8 to 9 in the two cross-sectional studies [37, 42]. The two RCTs [33, 41] elaborated on the specific methods of randomization and allocation concealment in detail, and had a low risk of of bias for blinding of participants, personnel, and outcome assessors. Meanwhile, three non-RCTs [36, 39, 41] had a low risk of bias in terms of selection of participants, intervention classification, outcome measurement and selection of reported result (Figs. 2, and 3 and Supplementary Material Table S1, S2, S3).

Risk of bias for five intervention studies

Risk of bias summary for five intervention studies
Comparison of Vitamin D levels in individuals with and without periodontitis
As shown in Fig. 4. Six articles [30,31,32,33, 35, 43] compared the difference in serum 25(OH)D levels between periodontitis and healthy individuals, and serum 25(OH)D levels in periodontitis has no significant difference from the normal population (SMD = -0.30, 95%CI -0.73 ~ 0.13, P = 0.17). At the same time, four articles [17, 34, 39, 42] compared the difference in serum vitamin D levels between periodontitis and healthy individuals, and periodontitis was found to be associated with lower serum vitamin D levels compared to normal population (SMD = -0.88, 95%CI -1.75 ~ -0.01, P = 0.048).

Forest plot of studies evaluating serum 25(OH)D/vitamin D levels in individuals with and without periodontitis. A Serum 25(OH)D levels. B Serum vitamin D levels. Gao, W-1: Gao, W-2000 IU/d vitamin D; Gao, W-2: Gao, W-1000 IU/d vitamin D; Ketharanathan,V–N: Ketharanathan,V-Norwegian; Ketharanathan,V-T: Keth- aranathan, V-Tamil; SMD: standardized mean difference; a: case–control study; b: RCT; c: Non-RCT; d: cross-sectional study
As shown in Fig. 5. Two articles [22, 38]compared the difference in saliva 25(OH)D levels between periodontitis and healthy individuals, and there was no significant difference in saliva 25(OH)D levels with periodontitis compared to normal population (SMD = 1.05, 95%CI 1.98 ~ 4.07, P = 0.50).

Forest plot of studies evaluating saliva 25(OH)D levels in individuals with and without periodontitis. SMD: standardized mean difference; a: case–control study
Due to the large heterogeneity among the studies, sensitivity analysis was conducted by eliminating study one by one. And the results of sensitivity analysis showed that excluding any study did not change the direction of the outcome, which indicated that the study was relatively stable (Supplementary Material Figure S1).
Changes in vitamin D levels after SRP + vitamin D/SRP treatment of periodontitis
There were three intervention trails [33, 40, 41] assessed the effects of SRP + vitamin D versus SRP on serum vitamin D levels in individuals with periodontitis, and the result of Meta-analysis showed that SRP + vitamin D was beneficial to increase the serum vitamin D concentration in individuals with periodontitis compared to SRP (SMD = 23.67, 95%CI 8.05 ~ 32.29, P = 0.003). At the same time, two intervention trails [36, 39] studied the effects of SRP on serum vitamin D levels in individuals with periodontitis, and the result showed that there was a statistically significant difference in serum vitamin D levels of individuals with periodontitis between before and after SRP (SMD = 1.57, 95%CI 1.07 ~ 2.06, P < 0.01). As shown in Fig. 6.

Forest plot of studies evaluating the effect of SRP + vitamin D versus SRP (before SRP versus after SRP). A SRP + vitamin D VS SRP. B Before SRP VS after SRP. Gao, W-1: Gao, W-2000 IU/d vitamin D; Gao, W-2: Gao, W-1000 IU/d vitamin D; SRP: scaling and root planing. SMD: standardized mean difference; a: RCT; b: Non-RCT
Meta-analysis of SRP + vitamin D on periodontal clinical parameters
There were three studies [33, 37, 40] evaluated the effects of SRP + vitamin D on PD compared to SRP alone, and no significant difference was found in PD between SRP + vitamin D and SRP in individuals with periodontitis (WMD = -0.11, 95%CI -0.23 ~ 0.01, P = 0.07). There were three studies [33, 37, 40] evaluated the effects of SRP + vitamin D on CAL compared to SRP alone. The results of Meta-analysis showed that vitamin D as an adjunct to SRP was demonstrated to be beneficial to reduce CAL in individuals with periodontitis (WMD = -0.13, 95%CI -0.19 ~ -0.06, P < 0.01). As shown in Fig. 7.

Forest plot of studies evaluating the effect of SRP + vitamin D on PD and CAL compared to SRP alone. A Probing depth (PD). B Clinical attachment level (CAL). Gao, W-1: Gao, W-2000 IU/d vitamin D; Gao, W-2: Gao, W-1000 IU/d vitamin D; WMD: weighted mean difference;a: Non-RCT; b: cross-sectional study; c: RCT
There were two studies [37, 40] evaluated the effects of SRP + vitamin D on GI compared to SRP alone, and no significant difference was found in GI between SRP + vitamin D and SRP in individuals with periodontitis (WMD = -0.55, 95%CI -1.11 ~ 0.01, P = 0.05). There was one study [33] evaluated the effects of SRP + vitamin D (2000 IU/d, 1000 IU/d) on BI compared to SRP alone. The results of Meta-analysis showed that there was no significant difference in GI between SRP + vitamin D and SRP in individuals with periodontitis (WMD = -0.05, 95%CI -0.15 ~ 0.05, P = 0.32) (Supplementary Material Figure S2).
Publication bias
Publication bias was tested by Begg's test and Egger's test by Stata 14.0 software. All P-values from the Begg’s Test and Egger’s test were greater than 0.05, the results did not show any evidence of publication bias. So it was believed that there was no publication bias among the studies of SRP + vitamin D on periodontal clinical parameters (Supplementary Material Table S4). Also, the funnel plot did not reveal any significant publication bias regarding serum vitamin D levels in individuals with and without periodontitis (Supplementary Material Figure S3).
Discussion
The Meta-analysis included both intervention and observational studies of varying quality, which will influence the interpretation of results. And high quality scores for both cross-sectional studies [37, 42] and case–control studies [17, 22, 30,31,32, 34, 35, 38, 43]. Two RCTs [33, 41] were at low risk of bias in all aspects except other bias, and three Non-RCTs [36, 39, 41] had a low risk of bias in terms of selection of participants, intervention classification, outcome measurement and selection of reported result, however, one of the studies [36]had a moderate risk of bias in confounding factors and deviation from intended intervention, two studies [39, 41] had a serious risk of bias in missing data. Therefore, more high-quality literature is required to validate this result in the future.
The results of this meta-analysis showed that SRP + vitamin D could significantly reduce CAL compared to SRP alone. And similar to Machado V, et al. [16], this systematic review supported that periodontitis was associated with lower serum vitamin D levels compared to normal population, while there was no significant difference in serum or saliva 25(OH)D levels between periodontitis individuals and normal population. Although Machado V, et al. [16] performed descriptive analysis in vitamin D supplementation during nonsurgical periodontal therapy, there was a lack of quantitative evidence to support the effect of vitamin D in adjunctive periodontal nonsurgical treatments such as SRP. Therefore, this Meta-analysis compared the effect of SRP + vitamin D and SRP alone in the treatment of periodontitis, and it was found that SRP + vitamin D could significantly reduce CAL compared to SRP alone, but had no meaningful effect on PD, GI and BI.
At the same time, considering the large heterogeneity among the results of the Meta-analysis, stata14.0 software was used for sensitivity analysis through one-by-one elimination, which found that none of the results changed the direction, indicating that the included studies were stable. And subgroup analysis of study types, publication year, samples source (serum or saliva), measurement method of vitamin D (Elisa, HPLC–MS, CLIA), country, and gender showed that none of the above factors were sources of heterogeneity for the included studies. Given the lack of evidence of clinical heterogeneity, this Meta-analysis was performed using random-effects models.
This Meta-analysis found there were statistically significant differences in serum vitamin D levels between individuals with periodontitis and healthy population, that is to say, periodontitis was associated with lower serum vitamin D levels compared with normal population. 25(OH)D is regarded as the best indicator of vitamin D status [44]. However, the present study found that there were no differences in serum or saliva 25(OH)D levels between periodontitis individuals and normal periodontal individuals. And this result was supported by the Millen et al., Antonoglou et al., and Amaliya et al. [45,46,47]. On the contrary, other studies have shown that plasma 25(OH)D levels were generally higher in individuals with periodontitis than in healthy population [38, 48], which was not consistent with the result of this study. This might be due to the fact that stages and grades of periodontitis in previous studies was different from that of the present study. In addition, the sample source of this study was different from that of previous studies, that is to say, the findings of this study were mainly based on serum samples, whereas the results of previous studies were primarily based on plasma or saliva samples, which might be partially responsible for the difference in results.
The results of this Meta-analysis showed that either SRP alone or SRP combined vitamin D could increase the serum vitamin D concentrations in individuals with periodontitis. In addition, SRP + vitamin D was helpful to improve periodontal clinical indicators. And the Meta-analysis demonstrated that SRP + vitamin D reduced CAL compared to SRP, although there was no significant difference in the improvement of PD, GI, and BI between SRP + vitamin D and SRP. Studies have shown that periodontitis is an inflammatory disease closely related to autoimmune regulation, and early recognition of early biomarkers of periodontitis, such as Transforming Growth Factor-β1 (TGF-β1) and Vascular endothelial growth factor (VEGF), is crucial for the treatment and prognosis of periodontitis [49, 50]. Vitamin D has immunomodulatory, anti-inflammatory and anti-proliferative effects, and plays an important role in bone metabolism, alveolar bone resorption and prevention of tooth loss [51,52,53]. Vitamin D can reduce gingival inflammation and promote wound healing after periodontal surgery by strengthening the antibacterial defense of gingival epithelial cells, which is an important supplement for the prevention of periodontal disease [51]. Thus, SRP + vitamin D could effectively reduce CAL in individuals with periodontitis compared to SRP, this result was in accordance with Perayil et al., Hiremath et al., and Mishra et al. [40, 54, 55], these studies found that vitamin D supplements had a dose-dependent anti-inflammatory effect in periodontitis or gingivitis individuals. However, there was no significant difference in the improvement of PD, GI, and BI between SRP + vitamin D and SRP, this might be attributed to the fact that SRP can reduce inflammatory burden by removing subgingival calculus and biofilm deposits in order to create a biocompatible root surface [56],and inadequate dose and duration of vitamin D supplementation may not have contributed to the statistical difference between SRP + vitamin D and SRP.
In a preliminary cohort study, similar to this systematical review, periodontal individuals with higher plasma vitamin D levels had lower PD and CAL [57]. Another study indicates vitamin D status in periodontal individuals was negatively correlated with GI [58]. In addition, vitamin D has a positive effect as a supplement to periodontal wound healing after non-surgical periodontal treatment, and an intervention trial showed that vitamin D supplementation contributed to improving CAL and PD after SRP [54, 59]. However, SRP + vitamin D only had a positive effect on improving CAL, but it had no advantage in PD,GI, and BI compared to SRP in the present study, this might be due to the small number and low quality of the included intervention studies. Therefore, higher quality studies are required to test the relationship between them in the future.
This study has the following shortcomings. Firstly, although a comprehensive search of five major English databases was conducted, all the included studies were in English, and there was a lack of published studies in other languages, as well as a lack of grey literature database search, which may cause publication bias to some extent. Secondly, there was a great deal of heterogeneity among studies, and the sources of clinical heterogeneity of some outcome indicators were still not fully explained by subgroup analysis and sensitivity analysis. Thirdly, due to the limited number of high-quality studies (RCTs) evaluating the relationship between vitamin D and periodontitis, observational studies and intervention studies meeting the inclusion and exclusion criteria were included in this meta-analysis in order to more comprehensively analyze the relationship between vitamin D and periodontitis. Although confounding factors were strictly controlled for observational studies and subgroup analysis was performed based on study type. However, the heterogeneity results could not be changed, and these bias factors would inevitably affect the results of the meta-analysis. Therefore, the interpretation of the results of this study should be cautious.
Conclusion
In summary, vitamin D plays a positive role in the adjuvant treatment of individuals with periodontitis. Therefore, vitamin D in combination with nonsurgical periodontal therapy such as SRP has a practical application of value on the prevention and treatment of periodontitis in clinical practice. However, Due to the small number of included studies, high heterogeneity, and lack of clear explanation of the source of heterogeneity, the actual effect of vitamin D combined with SRP in periodontitis in this study needs to be carefully interpreted, and a larger sample size and high- quality studies are still required to confirm it in the future.
Availability of data of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files. Further inquiries can be directed to the corresponding author.
References
Frencken JE, Sharma P, Stenhouse L, Green D, Laverty D, Dietrich T. Global epidemiology of dental caries and severe periodontitis - a comprehensive review. J Clin Periodontol. 2017;44(Suppl 18):S94-s105.
Yang H, Xiao L, Zhang L, Deepal S, Ye G, Zhang X. Epidemic trend of periodontal disease in elderly Chinese population, 1987–2015: a systematic review and meta-analysis. Sci Rep. 2017;7:45000.
Bernabe E, Marcenes W, Hernandez CR, et al. Global, Regional, and national levels and trends in burden of oral conditions from 1990 to 2017: a systematic Analysis for the Global Burden of Disease 2017 Study. J Dent Res. 2020;99(4):362–73.
World Health O, International Telecommunication U. Mobile technologies for oral health: an implementation guide. Geneva: World Health Organization; 2021.
Aral K, Milward MR, Kapila Y, Berdeli A, Cooper PR. Inflammasomes and their regulation in periodontal disease: a review. J Periodontal Res. 2020;55(4):473–87.
Graves DT, Li J, Cochran DL. Inflammation and uncoupling as mechanisms of periodontal bone loss. J Dent Res. 2011;90(2):143–53.
Adegboye AR, Boucher BJ, Kongstad J, Fiehn NE, Christensen LB, Heitmann BL. Calcium, vitamin D, casein and whey protein intakes and periodontitis among Danish adults. Public Health Nutr. 2016;19(3):503–10.
Zhang JC. Consideration for impacts of periodontitis on systemic health. Zhonghua Kou Qiang Yi Xue Za Zhi. 2021;56(6):507–9.
Sassi F, Tamone C, D’Amelio P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients. 2018;10(11):1656.
Garand M, Toufiq M, Singh P, et al. Immunomodulatory effects of Vitamin D supplementation in a deficient population. Int J Mol Sci. 2021;22(9):5041.
Trimboli F, Rotundo S, Armili S, et al. Serum 25-hydroxyvitamin D measurement: comparative evaluation of three automated immunoassays. Pract Lab Med. 2021;26: e00251.
Fernández-Lázaro D, Hernández JLG, Lumbreras E, Mielgo-Ayuso J, Seco-Calvo J. 25-Hydroxyvitamin D serum levels linked to Single Nucleotide Polymorphisms (SNPs) (rs2228570, rs2282679, rs10741657) in skeletal muscle aging in institutionalized elderly men not supplemented with Vitamin D. Int J Mol Sci. 2022;23(19):11846.
Jimenez M, Giovannucci E, Krall Kaye E, Joshipura KJ, Dietrich T. Predicted vitamin D status and incidence of tooth loss and periodontitis. Public Health Nutr. 2014;17(4):844–52.
Khammissa RAG, Ballyram R, Jadwat Y, Fourie J, Lemmer J, Feller L. Vitamin D deficiency as it relates to oral immunity and chronic periodontitis. Int J Dent. 2018;2018:7315797.
Perić M, Cavalier E, Toma S, Lasserre JF. Serum vitamin D levels and chronic periodontitis in adult, Caucasian population-a systematic review. J Periodontal Res. 2018;53(5):645–56.
Machado V, Lobo S, Proenca L, Mendes JJ, Botelho J. Vitamin D and Periodontitis: A systematic review and meta-analysis. Nutrients. 2020;12(8):2177.
Olszewska-Czyz I, Firkova E. Vitamin D3 serum levels in periodontitis patients: a case-control study. Medicina (Kaunas). 2022;58(5):585.
Agrawal AA, Kolte AP, Kolte RA, Chari S, Gupta M, Pakhmode R. Evaluation and comparison of serum vitamin D and calcium levels in periodontally healthy, chronic gingivitis and chronic periodontitis in patients with and without diabetes mellitus - a cross-sectional study. Acta Odontol Scand. 2019;77(8):592–9.
Isola G, Alibrandi A, Rapisarda E, Matarese G, Williams RC, Leonardi R. Association of vitamin D in patients with periodontitis: a cross-sectional study. J Periodontal Res. 2020;55(5):602–12.
Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontol 2000. 2013;62(1):59–94.
Krall EA, Wehler C, Garcia RI, Harris SS, Dawson-Hughes B. Calcium and vitamin D supplements reduce tooth loss in the elderly. Am J Med. 2001;111(6):452–6.
Costantini E, Sinjari B, Piscopo F, et al. Evaluation of salivary cytokines and Vitamin D levels in periodontopathic patients. Int J Mol Sci. 2020;21(8):2669.
Cai T, Yang ZY, Nie L, Zhen JX, Deng L, Zhou Z. Association between vitamin D receptor BsmI gene polymorphism and periodontitis: a meta-analysis in a single ethnic group. Cell Mol Biol (Noisy-le-grand). 2017;63(11):1–4.
Mashhadiabbas F, Neamatzadeh H, Nasiri R, et al. Association of vitamin D receptor BsmI, TaqI, FokI, and ApaI polymorphisms with susceptibility of chronic periodontitis: a systematic review and meta-analysis based on 38 case -control studies. Dent Res J (Isfahan). 2018;15(3):155–65.
Zhuang C, Yuan J, Du Y, et al. Effects of oral carotenoids on oxidative stress: a systematic review and meta-analysis of studies in the recent 20 years. Front Nutr. 2022;9: 754707.
Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355: i4919.
Wells GA, Wells G, Shea B, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2014.
Front Matter. In: Cochrane Handbook for Systematic Reviews of Interventions.2019:i-xxviii.
Baima G, Corana M, Iaderosa G, et al. Metabolomics of gingival crevicular fluid to identify biomarkers for periodontitis: a systematic review with meta-analysis. J Periodontal Res. 2021;56(4):633–45.
Abreu OJ, Tatakis DN, Elias-Boneta AR, et al. Low vitamin D status strongly associated with periodontitis in Puerto Rican adults. BMC Oral Health. 2016;16(1):89.
Alzahrani AAH, Alharbi RA, Alzahrani MSA, et al. Association between periodontitis and vitamin D status: a case-control study. Saudi Journal of Biological Sciences. 2021;28(7):4016–21.
Anbarcioglu E, Kirtiloglu T, Öztürk A, Kolbakir F, Acıkgöz G, Colak R. Vitamin D deficiency in patients with aggressive periodontitis. Oral Dis. 2019;25(1):242–9.
Gao WM, Tang HL, Wang DY, Zhou X, Song YQ, Wang ZM. Effect of short-term vitamin D supplementation after nonsurgical periodontal treatment: a randomized, double-masked, placebo-controlled clinical trial. J Periodontal Res. 2020;55(3):354–62.
Ketharanathan V, Torgersen GR, Petrovski BE, Preus HR. Radiographic alveolar bone level and levels of serum 25-OH-Vitamin D-3 in ethnic Norwegian and Tamil periodontitis patients and their periodontally healthy controls. Bmc Oral Health. 2019;19(1):83.
Laky M, Bertl K, Haririan H, et al. Serum levels of 25-hydroxyvitamin D are associated with periodontal disease. Clin Oral Invest. 2017;21(5):1553–8.
Liu KN, Meng HX, Lu RF, et al. Initial periodontal therapy reduced systemic and local 25-Hydroxy Vitamin D-3 and interleukin-1 beta in patients with aggressive periodontitis. J Periodontol. 2010;81(2):260–6.
Miley DD, Garcia MN, Hildebolt CF, et al. Cross-sectional study of Vitamin D and calcium supplementation effects on chronic periodontitis. J Periodontol. 2009;80(9):1433–9.
Miricescu D, Totan A, Calenic B, et al. Salivary biomarkers: Relationship between oxidative stress and alveolar bone loss in chronic periodontitis. Acta Odontol Scand. 2014;72(1):42–7.
Pai S, Shenoy N, John DS. Evaluation of IL-6, vitamin D level in chronic periodontitis patients after non-surgical periodontal therapy. Romanian Journal of Diabetes, Nutrition and Metabolic Diseases. 2021;28(4):376–82.
Perayil J, Menon KS, Kurup S, et al. Influence of Vitamin D & calcium supplementation in the management of periodontitis. J Clin Diagn Res. 2015;9(6):Zc35-38.
Peric M, Maiter D, Cavalier E, Lasserre JF, Toma S. The Effects of 6-Month Vitamin D supplementation during the non-surgical treatment of periodontitis in Vitamin-D-deficient patients: a randomized double-blind placebo-controlled study. Nutrients. 2020;12(10):2940.
Pradhan S, Agrawal S. Serum Vitamin D in patients with chronic periodontitis and healthy periodontium. J Nepal Health Res Counc. 2021;18(4):610–4.
Rafique S, Hingorjo MR, Mumtaz M, Qureshi MA. The relationship of 1,25-dihydroxyvitamin D and Vitamin D binding protein in periodontitis. Pakistan Journal of Medical Sciences. 2019;35(3):847–51.
Zhu A, Kuznia S, Niedermaier T, Holleczek B, Schöttker B, Brenner H. Distribution and determinants of Vitamin D-Binding Protein, Total, “Non-Bioavailable”, Bioavailable, and Free 25-Hydroxyvitamin D concentrations among older adults. Nutrients. 2021;13(11):3982.
Millen AE, Hovey KM, LaMonte MJ, et al. Plasma 25-Hydroxyvitamin D Concentrations and periodontal disease in postmenopausal women. J Periodontol. 2013;84(9):1243–56.
Antonoglou G, Knuuttila M, Niemea O, et al. Serum 1,25(OH)D level increases after elimination of periodontal inflammation in T1DM Subjects. J Clin Endocrinol Metab. 2013;98(10):3999–4005.
Amaliya A, Laine ML, Delanghe JR, Loos BG, Van Wijk AJ, Van der Velden U. Java project on periodontal diseases: periodontal bone loss in relation to environmental and systemic conditions. J Clin Periodontol. 2015;42(4):325–32.
Wu Y, Shu R, Luo LJ, Ge LH, Xie YF. Initial comparison of proteomic profiles of whole unstimulated saliva obtained from generalized aggressive periodontitis patients and healthy control subjects. J Periodontal Res. 2009;44(5):636–44.
Matarese G, Isola G, Anastasi GP, et al. Immunohistochemical analysis of TGF-β1 and VEGF in gingival and periodontal tissues: a role of these biomarkers in the pathogenesis of scleroderma and periodontal disease. Int J Mol Med. 2012;30(3):502–8.
Isola G, Giudice AL, Polizzi A, Alibrandi A, Patini R, Ferlito S. Periodontitis and tooth loss have negative systemic impact on circulating progenitor cell levels: a clinical study. Genes (Basel). 2019;10(12):1022.
Jagelavičienė E, Vaitkevičienė I, Šilingaitė D, Šinkūnaitė E, Daugėlaitė G. The relationship between Vitamin D and periodontal pathology. Medicina (Kaunas). 2018;54(3):45.
Schwalfenberg GK. A review of the critical role of vitamin D in the functioning of the immune system and the clinical implications of vitamin D deficiency. Mol Nutr Food Res. 2011;55(1):96–108.
Matarese G, Ramaglia L, Fiorillo L, Cervino G, Lauritano F, Isola G. Implantology and periodontal disease: the panacea to problem solving? Open Dent J. 2017;11:460–5.
Mishra SM, Ravishankar PL, Pramod V, et al. Effect of supplementation of Vitamin D in patients with periodontitis evaluated before and after nonsurgical therapy. Biomed Res Int. 2022;2022:5869676.
Hiremath VP, Rao CB, Naiak V, Prasad KV. Anti-inflammatory effect of vitamin D on gingivitis: a dose response randomised controlled trial. Indian J Public Health. 2013;57(1):29–32.
Cobb CM, Sottosanti JS. A re-evaluation of scaling and root planing. J Periodontol. 2021;92(10):1370–8.
Ribeiro LSFE, Araujo NS, Zilli Vieira CL, Dos Santos JN, Cury PR. Impact of serum vitamin D levels on periodontal healing outcomes: a preliminary cohort study. Int J Dent Hyg. 2022.
Jagelaviciene E, Vaitkeviciene I, Silingaite D, Sinkunaite E, Daugelaite G. The Relationship between Vitamin D and Periodontal Pathology. Medicina-Lithuania. 2018;54(3).
Bashutski JD, Eber RM, Kinney JS, et al. The Impact of Vitamin D status on periodontal surgery outcomes. J Dent Res. 2011;90(8):1007–12.
Acknowledgements
The authors are very grateful to all the participants in this study.
Funding
This study was supported by Tianjin Key Medical Discipline (Specialty) Construction Project (No. TJYXZDXK-078D), Tianjin Key Medical Discipline (Specialty) Sub-project of Construction Project (No.2022YTZX01, No.2022YTZX03), Tianjin Stomatological Hospital Nursing Research Fund Project (No. HL202104), and the Key Discipline Construction Project of Tianjin Stomatological Hospital (No. 2022P01).
Author information
Authors and Affiliations
Contributions
L-FF, Z-ZY, and ZZ designed the study. L-FF, Z-YZ, and Z-ZY acquired the study data. L-FF and Z-YZ analyzed and interpreted the data. L-FF, ZZ and SJ wrote the first draft of the manuscript. All authors revised the manuscript and approved it for publication.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liang, F., Zhou, Y., Zhang, Z. et al. Association of vitamin D in individuals with periodontitis: an updated systematic review and meta-analysis. BMC Oral Health 23, 387 (2023). https://doi.org/10.1186/s12903-023-03120-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03120-w