
Abstract
Background
Chronic inflammation and cumulative oxidative stress have been theorized as two common pathways of the interconnection between periodontitis and diabetes. Improvement in oxidizing status has been demonstrated in periodontal patients with diabetes treated with proper non-surgical periodontal treatment. In addition to periodontal treatment, Gaseous ozone therapy has been reported to possess anti-inflammatory properties and the ability to stimulate the endogenous antioxidant defence mechanism. To date, the antioxidant effect of gaseous ozone, in addition with periodontal treatment in diabetic patients, has been examined in only one study. The aim of this study was to determine the efficacy of gaseous ozone therapy as an alternative approach to supporting non-surgical periodontal therapy (NSPT), aimed at improving antioxidant machinery and interfering with ROS production on plasma levels in diabetic individuals diagnosed with moderate or severe periodontitis.
Methods
One hundred and eighty patients with periodontitis and type 2 diabetes mellitus were randomly assigned to receive non-surgical periodontal treatment (NSPT) plus gaseous ozone therapy (A) NSPT alone (B). Clinical and periodontal parameters -Bleeding on probing (BOP), Periodontal pocket depth (PPD), and Clinical attachment Level (CAL)- and plasma levels of oxidant-antioxidant (TOS- TAOS) levels, glutathione (GSH), and malondialdehyde (MDA) were recorded at baseline and at 3- (T1) and at 6-months (T2) after treatment.
Results
Both treatments were efficacious in reducing clinical parameters. However, there were no significant differences regarding oxidative stress parameters in group A compared to group B.
Conclusions
In the present study, gaseous ozone therapy did not enhance the effect of periodontal treatment in reducing oxidative stress in plasma levels of periodontitis patients with type II diabetes.
Trial registration
The study was registered with ISRCTN1728169 (23/07/2022).
Similar content being viewed by others


Background
Over the past decade, the interactions between periodontal inflammation and systemic reactions have become better understood, and this has motivated the recognition that periodontitis has pathogenic effects on diabetes, depending on biological circumstances and a highly orchestrated immune response [1,2,3]. Periodontitis is one of the most common infectious-inflammatory diseases involving the periodontium, distinguished by the gradual and progressive deterioration of periodontal tissues with concomitant structural and functional changes [4]. The paroxysmal host response to the etiologic agents and its products is the primary determinant of the periodontal reaction, mediated through inflammatory pathways that are regulated with support of environmental and epigenetic mechanisms [5, 6]. Periodontitis is significantly related to a reduction in total antioxidant status (TAS TAOS) and an increase in reactive oxygen metabolites [7,8,9]. The immune response and oxidative stress progressively catalyse degenerative changes that ultimately affect periodontal architecture. Under physiological conditions, equilibrium is maintained by the balance between ROS production and ROS scavenging [10,11,12]. Conversely, oxidative stress occurs when the antioxidant protective system becomes pathologically unbalanced [13]. ROS are the most abundant intracellular oxidizing substances and act as essential mediators and signalling molecules in many biological processes [14, 15]. The biological task of ROS is dichotomous, contributing to physiologic and pathological conditions. In the physiological state, the proteolytic-anti proteolytic equilibrium exists, and ROS can act as a second messenger in innate and adaptive immune cells that regulate the activities of proteins specific to the maintenance of biological functions [16,17,18]. In the pathological condition, the enhanced generation of free radicals is observed, responsible for the modification of proteolytic -antiproteolytic balance [19]. The rise in ROS levels is crucial to orchestrate the peripheral response to chronic periodontal infection by promoting hyperactivation of the inflammatory cascade [20,21,22]. Periodontitis occurs three times more often in diabetic patients than in healthy individuals, although there is considerable heterogeneity in patients in terms of phenotypic expression [23,24,25]. Common factors clarify the increased risk of increased inflammation. Clinical studies examining the association between periodontitis and diabetes have indirectly demonstrated the role of periodontal inflammation, by IL-6 -, TNF-α-, IL-1β-, and C-reactive protein-induced pro-inflammatory process [26]. Oxidative stress and chronic inflammation in humans promote the dysregulation of adipokines (e.g., leptin, TNF-α, IL-6, adiponectin, etc.) synthesis and secretion which can lead to secondary metabolic disorders including insulin resistance [27]. The phenomenon of low-grade inflammation related to periodontitis results in a chain of events leading to an increase levels in oxidative stress and the release of free radicals in diabetes. Oxidative stress plays a pivotal role in the development of diabetes complications by causing excess mitochondrial hydrogen peroxide emission in the skeletal muscle, altering redox status and promoting insulin resistance [23,24,25, 28]. Disruption of appropriate physiological function and debilitation of the antioxidant defence system can advance the evolution of diabetes by increasing the frequency of oxidative damage to erythrocytes [29,30,31]. The supraphysiological production of reactive oxygen and nitrogen species (ROS/NOS) and ineffective antioxidant defence modify the structural and mechanical properties of erythrocytes, which result in changes in mechanical properties, elevate susceptibility to the mechanic and osmotic shock, and damaging of N-terminal of band-3 proteins (B3p) by modifying the anion exchange process, and glycophorin, resulting in decline in the cell’s surface area [32]. Erythrocyte imbalance can make them dysfunctional and impede efficient tissue oxygenation.
Proper periodontal treatment has beneficial effects on the reduction of oxidative stress [33,34,35,36,37]. Because of its strong antimicrobial and anti-inflammatory properties, ozone is frequently employed in dentistry [38,39,40]. Thus, it was tempting to speculate that gaseous ozone therapy add-on periodontal treatment might be effective in reducing oxidative stress outcomes in diabetic patients. We speculated that non-surgical periodontal therapy (NPTS) in combination with ozone therapy would counteract the oxidative stress of patients with diabetes with periodontitis.
Methods
Study setting and Ethics
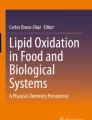
Between June 2018 and September 2019, this prospective, controlled, one-blind, randomized clinical trial enrolled 180 diabetic subjects who were outpatients at the Clinic of Periodontology of the Faculty of Dental Medicine of Albanian University. All participants provided informed written consent prior to patient enrolment and randomization. The study protocol was approved by the Institutional Review Board at Albanian University (reference number 2018/224) and was performed in compliance with good clinical practice and followed the ethical standards established in the Declaration of Helsinki. The study was registered with ISRCTN17281691. Patients consenting to participate in the study were randomly assigned to one of two treatment groups. The study design followed the CONSORT guidelines [41]. Figure 1 shows the flow diagram of the study’s progress through all phases.

Participant flow diagram
Study population
Eligibility criteria for the study were assessed at in-person screening visits involving laboratory blood assessment, comprehensive clinical periodontal examination, and detailed medical history. To be eligible to participate in this study, patients had to meet the T2DM diagnostic criteria recommended by the American Diabetes Association (ADA) in 2020: FPG ≥ 126 mg/dL (7.0 mmol/L), or 2-h PG ≥ 200 mg/dL (11.1 mmol/L) during OGTT, or HbA1C ≥ 6.5% (48 mmol/mol), or a random plasma glucose ≥ 200 mg/dL (11.1 mmol/L).
Inclusion criteria included poorly controlled (HbA1c > 7%) T2DM, adult patients (age ≥ 18 years); having no significant comorbidity, being not involved in any trial/study related to diabetes and periodontitis during last 12 months and able to attend regular visits, the presence of at least 16 natural teeth that were distributed in all four quadrants. Among the teeth, at least six had to exhibit one site with a pocket depth (PD) ≥ 5 mm at baseline. Periodontitis was graded according to the diagnostic criteria co-presented the American Academy of Periodontology (AAP) and the European Federation of Periodontology (EFP) in the World Workshop on the Classification of Periodontal and Peri-Implant Disease and Conditions [42]. Key exclusion criteria included gestational and type 1 diabetes mellitus and cognitive impairments, pregnancy and lactation, subjects who had received periodontal therapy or taken an antibiotic during the previous six months.
Study enrolment and randomization
Randomizing software was used to randomly allocate patients on a 1:1 ratio to non-surgical periodontal therapy (NSPT) + Ozone group, and NSPT. The patients in group A (n = 90) received non-surgical periodontal treatment plus gaseous ozone therapy. Patients in Group B (n = 90) received non-surgical periodontal treatment. All follow-up periodontal evaluations were performed by the same two calibrated operators. The unblinded clinician determined the treatment for the subjects. Participants were not blinded because the motivation session was carried out according to the allocation. Prior to a consultant appointment, patients visit the department of Dentistry for periodontal clinical parameters assessments. During this phase, patients were provided with a general information sheet. Patients who met study eligibility criteria signed the informed consent, after which they were enrolled into the research study and, randomized to either NSPT + Ozone treatment (Test Group, A) or the control treatment (Control Group, B) according to the randomization sequence. Secondly, eligible patients were actively involved in the research study by screening phase. Subjects provided informed consent prior to initiation of any study procedures. Individuals were excluded if they presented declined cognitive function and unable to make informed consent, underwent periodontal treatment within least 12 months, and systemic antibiotic therapy within the last 6 months, pregnancy, or breast feeding, having uncontrolled hypertension, history of heart disease or stroke which might interfere with systemic antioxidative status.
Periodontal parameters
A comprehensive periodontal charting and intraoral examination were performed for all participants, and the periodontal status was examined by measurements of prior to and after the treatment in both groups and encompassed measurements of the following clinical periodontal parameters: clinical attachment loss (CAL), probing pocket depth (PPD), and bleeding on probing (BOP). Bleeding was determined using a periodontal probe (PCP UNC-15, Hu-Friedy, Chicago, IL) that flowed along the soft tissue wall of the entrance of the gum fissure and parallel to the long axis of the tooth in the facial/ lingual sites and directed towards the column in the interproximal sites; CAL was measured as the distance from a fixed reference point (cementoenamel junction, CEJ) to base of pocket, whereas PPD was measured as the distance between the free gingival margin and the clinically base of each periodontal pocket. Full mouth series (FMS) radiographs were obtained prior all treatments for all subjects to confirm alveolar bone level. Clinical parameters assessment was performed by measuring on six sites of teeth (mesial, median, and distal points at buccal and palatal aspects) [43]. Additionally, the periodontal inflamed surface area (PISA) was assessed to quantify periodontitis severity. Clinical measurements were performed by the same blind and calibrated investigators using the same type of periodontal probe (PCP UNC-15, Hu-Friedy, Chicago, IL) with a mild probing force corresponding to approximately 25 N. About intra-examiner reproducibility, the intraclass correlation coefficient (ICC) was used to assess the agreement of findings, based on the PD measurements. The ICC was calculated using the R package irr. An intra-examiner agreement of 0.989 (95% CI, 0.916–0.999) was found.
Monitoring procedures-data collection
Medical history, and current medication were collected, and a comprehensive periodontal examination at study enrolment was performed. According to the local laboratory’s standard procedure, routine laboratory parameters were analyzed from venous blood samples. All study visits occurred in the Outpatient Laboratory of the Center for diabetes control. Each participant completed three inpatient study visits for periodontal and oxidative status assessment: a baseline visit, 3-month visit, and 6-month visit. During the initial evaluation, oxidative status assessment was carried out prior to treatment. This protocol was repeated at the three- and six-month re-evaluation to assess post-treatment oxidant and antioxidant parameters.
Interventions
The interventions in groups A and B comprised full-mouth scaling and root surface debridement completed within 6 weeks, operating one scaling session of 45 min, 4 sessions of root planning. The scaling session consisted of ultrasonic supra- and subgingival debridement of soft and hard deposits of bacterial plaque and calculus. After completing the measurements, all pockets with PPD ≥ 4 mm were scaled, and root planed under local anesthesia with Gracey curettes (Hu-Friedy®) and ultrasonic instruments (Piezon® 250; Electro Medical Systems SA) by the same clinicians. After all mechanical treatment sessions, in group A, the patients rinsed for 1 min with 15 mL of ozonized oil mouthwash (Ialozon Blu; Gemavip, Cagliari, Italy), and after mechanical instrumentation. Patients in group B did not received mouthwash. Oral hygiene instructions were given and scaling and root surface debridement was performed with piezoelectric and hand instruments. Upon leaving each session, participants were subjected to oral hygiene instruction by emphasizing the use of manual or electric toothbrushes twice daily, tongue cleaning via brushing or scraping to reduce potential pathogenic organisms residing on the dorsum of the tongue, interproximal cleaning to disrupt plaque formation. We established sequential treatment plan with three steps of gaseous ozone therapy after the instrumentation by ultrasonic devices. As our previous research [44], an ozone generator (Ozone DTA, Sweden & Martina Company; Carrara San Giorgio, Veneto, Italy), was employed, according to manufacturer’s instructions, as follows: Step (1) 2-min rinse with ozonated water at a ratio of 1:3; full-mouth decontamination; topical irrigation with ozonated water; 1–2 cycles of ozone gas at 8–10 power in correspondence of pathological pockets, under local anesthesia. Step (2) Quadrant root planning; 2-min rinse with ozonated water at a ratio of 1:3; Deplaquing; 1–2 cycles of ozone gas at 8–10 power in correspondence of pathological pockets for each quadrant, under local anesthesia. Step (3) Maintenance: 2-min rinse with ozonated water at a ratio of 1:3; Deplaquing; 1–2 cycles of ozone gas at 4–5 power in correspondence of pathological pockets for all quadrants, two weeks after completion of treatment. Patients of Group A were instructed to rinse with commercial mouthwash (Ialozon Blu; Gemavip, Cagliari, Italy) twice a day after brushing. All patients were instructed to abstain from use of all types of commercial mouthrinses.
Supportive periodontal treatment
Supportive periodontal therapy (SPT) was performed at 3 and 6 months and consisted of reinforcement of patient-performed oral hygiene and detailed monitoring of the periodontal tissues (examination of extraoral and intraoral soft tissues; dental examination and radiographic review; evaluation of the patient’s oral hygiene performance; periodontal evaluation and risk assessment). In addition, supragingival and subgingival removal of bacterial plaque and calculus was performed, and gaseous ozone therapy was applied as a maintenance treatment to each session for patients of group A. [43].
Plasma levels of oxidative status assessment
Oxidative stress assessment of participants was performed at baseline, 3 and months follow-up. Serum samples were obtained by centrifugation (1500 × g, 10 min) of the collected blood samples and then kept at -80 °C until the GSH, MDA, TAOS, and TOS parameters were analyzed. Then, they were transferred to the University of Albanian for analyses. Serum concentrations of glutathione (GSH), and malondialdehyde (MDA) were measured by employing a Sciex API 3000 triple quadrupole mass spectrometer as described previously [31]. The concentration of MDA was calculated using an extinction coefficient of MDA–TBA complex, which is 1.56 × 105 M − 1 cm − 1 and the results were expressed as nmol MDA/mg protein. Total glutathione content was measured according to the method described by Beutler et al. [40] using glutathione reduced colorimetric method [42]. Results were expressed as mg/dl. The results were shown as nmol 2HO Eq/mg for TOS, and µmol Trolox Eq/mg for TAOS. The reference range for TOS and TAS were 5.54– 21.38 µmol 2HO Equiv./L, and 1.20– 1.81 mmol Trolox equiv./l, respectively.
Statistical analysis
All the analyses were performed with SPSS for Windows (Version 13.0, SPSS Inc., Chicago, IL, USA). A multivariate analysis of covariance (MANCOVA) was conducted to assess if there were significant differences in the linear combination of TOS, TAOS, GSH, MDA, PPD, CAL, and BOP at baseline and during follow-up between the levels of severity of periodontitis and treatment after controlling for age, smoking status, and sex. Before conducting MANCOVA, Pearson’s correlation was performed between all the dependent variables to test the MANCOVA assumption that the dependent variables would be correlated in the moderate range [33]. A significant pattern of correlation was observed amongst the following dependent variables, suggesting the appropriateness of MANCOVA. Additionally, the Box’s M value of 138.53 was associated with a p-value of 0.008, indicating that the covariance matrices for each group were not statistically significantly different from one another and that the assumption was met based on Huberty and Petoskey’s guidelines [36]. When an effect was significant in MANCOVA, one-way analysis was used to discover which dependent variables had been affected. Statistical testing of the model was performed by the Fisher’s statistical test for analysis of covariance (ANCOVA). This approach evaluated an associated probability (p-value) for each term of the regression model. For a given confidence level (95% in our case), an effect with p-value higher than 0.05 was not considered statistically significant on the output variable [44]. Fixed variables were treatment groups (test, A, or control, B), and degree of severity of periodontitis (moderate or severe). Each participant was included as a random effect. To test for confounders, an a priori set of variables were considered as covariates: age, sex, and smoking status (yes/no) at baseline. Any covariate exerting a change in effect estimate of at least 10% was included in the analysis as a confounder. The only confounder noted was smoking for analysis of oxidant status and was therefore integrated as a confounder in all analyses [45]. Residuals from the outcome variables were reviewed about model assumptions. The assumption of normality was assessed by plotting the quantiles of the model residuals against the quantiles of a Chi-square distribution, and all were normally distributed. Homoscedasticity was evaluated by plotting the residuals against the predicted values. Mauchly’s test was used to assess the assumption of sphericity. Mahalanobis distances were calculated and compared to a χ2 distribution to identify influential points in the residuals. An outlier was defined as any Mahalanobis distance that exceeds 22.46, the 0.999 quantile of a χ2 distribution with 6 degrees of freedom. There were no outliers detected in the model. A correlation matrix was calculated to examine multicollinearity between the dependent variables. The correlation matrix is presented in Appendix 1.
Homogeneity of regression slopes. As shown in Appendix 2, the assumption for homogeneity of regression slopes was assessed by rerunning the MANCOVA, but this time including interaction terms between each independent variable and covariate. If the model with the covariate interaction terms explains significantly more variance than the original MANCOVA model, then there were significant interactions between the covariates and independent variables. The model with covariate-independent variable interactions did not explain significantly more variance for all dependent variables than the original model, F(72, 120) = 0.74, p = .914. This implies that none of the covariates interacted with the independent variables and the assumption of homogeneity of regression slopes was met [46].
Post-hoc. To further examine the effects of the severity of periodontitis and treatments on all dependent variables at baseline and during follow up controlling for age, smoking status, and sex, an analysis of covariance (ANCOVA) was conducted for each dependent variable [47].
A multinomial regression model was conducted and compared to the null model for each pair of categorical covariates and independent variables to assess independence (Appendix 2). There were no significant models for any combination of covariates and independent variables based on an alpha of 0.05, indicating the assumption of independence between covariates and independent variables was met [48]. Categorical variables are summarized using frequencies and percentages. Continuous variables with normal distributions are presented as mean (± standard deviation); continuous variables with non-normal distributions are presented as medians and interquartile ranges. Differences in baseline characteristics among the groups were examined using the Pearson’s chi-square test or Fisher’s exact test for categorical variables and analysis of variance or Kruskal-Wallis test for continuous variables. The primary endpoints were the mean TOS, TAOS, GSH, and MDA at 3, and 6 months, but PPD, CAL, and BOP were also subject to secondary analyses. Likewise, dichotomous outcomes were tested using logistic regression analysis of the effect of the two interventions and their interaction term on the outcome. The significance level was set at P < .05.
Sample size calculation
The power analysis of the study was performed on the primary outcomes TOS and TAOS. To detect a change of 20% between groups with 90% power and α = 0.05, a sample size of 50 patients per group was needed and to account for dropouts 180 patients were recruited. Primary outcomes in this report were TOS and TAOS plasma concentration. Secondary outcomes were periodontal parameters and HbA1c levels.
Results
Out of the 235 patients screened, 180 were enrolled. Two patients were withdrawn from treatment because of cardiomyopathy (1) and pregnancy (1) during the follow-up. Overall, one-hundred-two participants were female (58.8 ± 10.8 years), and 78 (56.9%) were men (54.9 ± 16.5 years). The intervention period lasted for 6 months (8.12 median, ± 13.7 weeks). Baseline characteristics of both trial cohorts were similar. The clinical and biochemical characteristics between groups at baseline are summarized in Table 1.
The main effect for degree of periodontitis’ severity was significant, F(15, 19) = 2.32, p = .043, η2p = 0.65, suggesting the linear combination of each dependent variable was significantly different between the levels of severity of disease after controlling for age, smoking status, and sex. The main effect for treatment was significant, F(15, 19) = 4.73, p < .001, η2p = 0.79, suggesting the linear combination of all dependent variables was significantly different between the levels of treatment after controlling for covariates. The covariates, age and smoking status, were not significantly related to dependent variables at each time point, F(15, 19) = 1.61, p = .163, η2p = 0.56, and F(15, 19) = 0.77, p = .695, η2p = 0.38 respectively. The covariate, sex, was not significantly related to each dependent variable, F(15, 19) = 0.93, p = .551, η2p = 0.42. Table 2 shows the results of the MANCOVA.
The ANCOVA results were insignificant, F(5, 34) = 0.77, p = .575, indicating the differences among the degree of degree of periodontitis’ severity and treatment were insignificant (Table 3). The main effect for degree of periodontitis’ severity was not significant, F(1, 34) = 0.63, p = .435 for TOS at T0, and the main effect for treatment was not significant, respectively F(1, 34) = 0.87, p = .357.
Table 3 shows that there were not statistically significant differences between the values of TOS at baseline among the values of degree of periodontitis’ severity and treatment. The main effect for the degree of periodontitis’ severity was not significant, F(1, 34) = 0.10, p = .752, indicating there were no significant differences of TOS at T1 by severity of periodontitis levels. However, there were statistically significant differences for treatment, F(1, 34) = 4.31, p = .045, ηp2 = 0.11, indicating significant differences in TOS at 3 months (T1) by treatment levels. Regarding the TOS levels at 6 months (T2) after treatment, the results of the ANCOVA were not significant, F(5, 34) = 2.31, p = .065, indicating the differences among the degree values of periodontitis’ severity and treatment were not relevant. No statistically significant differences among the degree of periodontitis’ severity and treatment were found for TAOS at T1, with F(1, 34) = 0.60, p = .445, and F(1, 34) = 0.83, p = .369 respectively. Regarding TAOS at 6 months (T2), both groups experienced similar values. Severity of periodontitis did not affect results, F(1, 34) = 0.35, p = .559 by degree of periodontitis’ severity levels. No statistically significant changes were observed in the TOS and TAOS oxidative stress markers in either group (F(1, 34) = 3.45, p = .072). This is consistent with the results regarding MDA and glutathione levels which states that there are not statistically significant differences among groups (p = .086). The results of BOP at T2 were significant, F(5, 33) = 2.80, p = .032 among the values of severity of periodontitis and treatment. The main effect for severity of periodontitis was F(1, 33) = 11.11, p = .002, ηp2 = 0.25, indicating there were significant differences in BOP at T2 by severity of periodontitis levels F(1, 33) = 3.69, p = .063. No significant differences of BOP at T2 by treatment levels were revealed. There were significant differences in CAL at T2 by severity of periodontitis and treatment while controlling for age, smoking status, and sex. The detailed ANCOVA results are reported in Appendix 3.
Discussion
[4, 8, 11, 37] The number of experimental studies on the molecular and physiological basis of the interaction between periodontitis and diabetes has grown considerably in recent years [31,32,33]. It has long been understood that individuals with diabetes are significantly more prone to develop periodontitis than healthy subjects, and vice versa. However, inflammation alone is not enough to stratify the risk for both diseases. Recently, it has been reported that in diabetic patients with periodontitis, oxidative damage could also be dependent on periodontal condition [4, 8, 11]. Periodontitis reflects unsuccessful redox homeostasis through indirect mechanisms which impact the intrinsic antioxidant defence system capacity. The metabolic flux regulation of ROS caused by chronic periodontal inflammation leads to a state of moderately increased levels of intracellular ROS [21, 24]. In line with the theory of the bi-directional relationship between periodontitis and diabetes, many researchers have identified oxidative stress as a key factor contributing to this correlation. A dominant view is that an imbalance between reactive oxygen species (ROS) production and elimination by antioxidant defense mechanisms exerts significant negative pressure. Moreover, chronic periodontal inflammation induces the oxidative burst and is significantly associated with upregulated expression of GSH and MDA levels, markers of oxidative stress [37]. Therefore, it has been alleged that periodontal disease probably contributes to the oxidative stress associated with diabetes and chronic inflammation. Mounting evidence has signaled oxidative stress as a core pathophysiology in the development of complications of diabetes [31]. Indeed, oxidative stress plays a critical role in diabetes, and hyperglycemia decreases enzyme activities of superoxide dismutase (SOD) and glutathione (GSH) synthesis, likely via glycation [17]. The effects of long-term exposure to increased levels of pro-oxidant factors exacerbate the outcomes, by triggering a negative chain reaction which affects processes involving the maintenance of homeostasis, as well as a wide variety of cellular functions (mitochondrial dynamics and function, structural modification of cellular proteins and the alteration of their functions, nuclear and mitochondrial DNA dysfunction, lipids, and proteins damage) [40]. No direct causal link has been established between oxidative stress periodontitis-induced and diabetes, and the exact mechanism remains elusive and is not yet entirely clear [31]. Ozone therapy in diabetes has been widely studied because of the link between diabetic nephropathy and oxidative stress, and it has been anecdotically reported the effectiveness in reversing the effect of diabetes mellitus [40]. However, ozone therapy includes a wide range of administration methods, and more emphasis has been placed on autohemotherapy and its relevant changes in biological targets [20, 33]. We previously demonstrated the statistically significant effect of ozone therapy on periodontal parameters, but no interesting results were obtained regarding glycaemic control [34]. Then, we focused our trial on oxidant/antioxidant balance, by investigating the impact of gaseous ozone therapy add-on periodontal treatment on the oxidative status of diabetic patients suffering periodontitis. In recent years, the ozone therapy has become a very promising therapeutic agent in dentistry [28, 39]. Ozone’s anti-inflammatory, antimicrobial, and antioxidant properties have been largely recognized. Ozone has ability to stimulate 2,3-diphosphoglycerate that in turn induces an elevation in oxygen supply to the tissues, leading to increased production of enzymes, which act as free radical scavengers and cell wall savers, such as superoxide dismutase, glutathione peroxidase, and catalase determining an increase in the output of prostacyclin, which improves vasodilatation and tissue oxygen supply [31]. In our study, diabetic individuals showed low antioxidant defenses. Our results did not confirm protective effects of ozone on endogenous antioxidant defenses. Periodontal parameters improved significantly in Test group, but no statistically significant differences were revealed among oxidative stress markers. To the best of our knowledge, there is no previous evidence to explore the role of gaseous ozone treatment given adjunctive to non-surgical periodontal therapy on oxidative status of diabetic patients with periodontitis prior to our current study. Sagai and Bocci firstly demonstrated ability of ozone to modulate the metabolic pathway of Nrf2. However, this follow-up study not focused on the oxidative stress outcome [49]. The study conducted by Arana et al. on salivary oxidative stress levels in patients with uncontrolled diabetes demonstrated a strong association between oxidative stress and periodontal disease in diabetic conditions [50]. Some studies have demonstrated the antioxidant effect of ozone application in topical form (subgingival ozone irrigation, topical gaseous ozone application) in delaying the progress of periodontitis reporting mixed results, but periodontal use is still poor investigated. Unfortunately, only one study investigated the effect of periodontal treatment and topical application of ozone on plasma levels of reactive oxygen metabolites in diabetic patients affected by periodontitis [13]. Oxidative status of both groups improved significantly after non-surgical periodontal treatment, and at the 3-month evaluation, periodontal parameters decreased significantly for the ozone group. Previous efforts have led to the identification of effector molecules responsible for regulating the biological protective activity of the ozone in the body, as reviewed by Tricarico and Travagli [51]. The mechanism of ozone-tissue interaction is influenced by many factors including the approach used, the conditions of oxidation, and the physical state of the substrate. The gaseous ozone therapy was used to treat periodontal pockets, and local effects were observed. Because of the limited investigational conditions, we do not know what the direct effects of cell homeostasis would be. Our study has some limitations. First, this study was conducted in a single center with a small sample size; second, TAOS, TOS, GSH, and MDA biomarkers were measured at brief-term. Our data did not point out that periodontitis can negatively affect the oxidative status in diabetes, and the effectiveness of periodontal treatment and ozone to our previous works resulted in pointing to metabolic control. The interindividual and intergroup differences may be explainable by different degrees of oxidative stress among the subjects, with distinct capability of activating the Nrf2-dependent oxidative stress metabolic pathway. The higher level of MDA suggest that oxidative stress was not counterbalanced by sufficient antioxidant defences, despite plasma levels of antioxidants were increased.
Although it is demonstrated that periodontitis has a role in development of diabetes, the studies provide an insufficient explanation about the role ROS play in the mechanism at the cellular level. It is required more thorough research.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
van Winkelhoff AJ, Winkel EG, Vandenbroucke-Grauls CM. Parodontitis: een verborgen chronische infectie [Periodontitis: a hidden chronic infection]. Ned Tijdschr Geneeskd. 2001;145(12):557–63.
Loos BG, Van Dyke TE. The role of inflammation and genetics in periodontal disease. Periodontol 2000. 2020;83(1):26–39.
Sczepanik FSC, Grossi ML, Casati M, Goldberg M, Glogauer M, Fine N, et al. Periodontitis is an inflammatory disease of oxidative stress: we should treat it that way. Periodontol 2000. 2020;84(1):45–68.
Chapple IL, Milward MR, Dietrich T. The prevalence of inflammatory periodontitis is negatively associated with serum antioxidant concentrations. J Nutr. 2007;137:657–64.
Wang Y, Andrukhov O, Rausch-Fan X. Oxidative stress and antioxidant system in Periodontitis. Front Physiol. 2017;8:910.
Liu C, Mo L, Niu Y, Li X, Zhou X, Xu X. The role of reactive oxygen species and autophagy in Periodontitis and their potential linkage. Front Physiol. 2017;8:439.
Kalyanaraman B, Darley-Usmar V, Davies KJ, Dennery PA, Forman HJ, Grisham MB, et al. Measuring reactive oxygen and nitrogen species with fluorescent probes: challenges and limitations. Free Radic Biol Med. 2012;52(1):1–6.
Tricarico G, Travagli V. The relationship between ozone and human blood in the course of a Well-Controlled, mild, and transitory oxidative eustress. Antioxid (Basel). 2021;10(12):1946.
Sauer H, Wartenberg M, Hescheler J. Reactive oxygen species as intracellular messengers during cell growth and differentiation. Cell Physiol Biochem. 2001;11(4):173–86.
Forman HJ, Maiorino M, Ursini F. Signaling functions of reactive oxygen species. Biochemistry. 2010;49(5):835–42.
Mittal M, Siddiqui MR, Tran K, Reddy SP, Malik AB. Reactive oxygen species in inflammation and tissue injury. Antioxid Redox Signal. 2014;20(7):1126–67.
Esterbauer H, Schaur RJ, Zollner H. Chemistry and biochemistry of 4-hydroxynonenal, malonaldehyde and related aldehydes. Free Radic Biol Med. 1991;11(1):81–128.
Marconcini S, Giammarinaro E, Cosola S, Oldoini G, Genovesi A, Covani U. Effects of non-surgical Periodontal treatment on reactive oxygen metabolites and Glycemic Control in Diabetic patients with chronic Periodontitis. Antioxid (Basel). 2021;10(7):1056.
Konopka T, Krol K, Kopec W, Gerber H. Total antioxidant status and 8-hydroxy-2′-deoxyguanosine levels in gingival and peripheral blood of periodontitis patients. Arch Immunol Ther Exp (Warsz). 2007;55:417–22.
Fialkow L, Wang Y, Downey GP. Reactive oxygen and nitrogen species as signaling molecules regulating neutrophil function. Free Radic Biol Med. 2007;42:153–64.
Hyslop PA, Hinshaw DB, Halsey WA Jr, Schraufstätter IU, Sauerheber RD, Spragg RG, et al. Mechanisms of oxidant-mediated cell injury. The glycolytic and mitochondrial pathways of ADP phosphorylation are major intracellular targets inactivated by hydrogen peroxide. J Biol Chem. 1988;263(4):1665–75.
Johansen JS, Harris AK, Rychly DJ, Ergul A. Oxidative stress and the use of antioxidants in diabetes: linking basic science to clinical practice. Cardiovasc Diabetol. 2005;4:5.
Chapple IL, Matthews JB. The role of reactive oxygen and antioxidant species in periodontal tissue destruction. Periodontol 2000. 2007;43:160–232.
Almeida M, Han L, Ambrogini E, Weinstein RS, Manolagas SC. Glucocorticoids and tumor necrosis factor α increase oxidative stress and suppress wnt protein signaling in osteoblasts. J Biol Chem. 2011;286(52):44326–35.
Suh Y, Patel S, Kaitlyn R, Gandhi J, Joshi G, Smith NL, et al. Clinical utility of ozone therapy in dental and oral medicine. Med Gas Res. 2019;9(3):163–7.
Morgantini C, Natali A, Boldrini B, Imaizumi S, Navab M, Fogelman AM, et al. Anti-inflammatory and antioxidant Properties of HDLs are impaired in type 2 diabetes. Diabetes. 2011;60:2617–23.
Jakus V. The role of free radicals, oxidative stress and antioxidant systems in diabetic vascular disease. Bratisl Lek Listy. 2000;101:541–51.
Jacob S, Ruus P, Hermann R, Tritschler HJ, Maerker E, Renn W, et al. Oral administration of RAC-alpha-lipoic acid modulates insulin sensitivity in patients with type-2 diabetes mellitus: a placebo-controlled pilot trial. Free Radic Biol Med. 1999;27(3–4):309–14.
Preshaw PM, Bissett SM. Periodontitis and diabetes. Br Dent J. 2019;227(7):577–84.
Preshaw PM, Alba AL, Herrera D, Jepsen S, Konstantinidis A, Makrilakis K, Taylor R. Periodontitis and diabetes: a two-way relationship. Diabetologia. 2012;55(1):21–31.
Abbass MM, Korany NS, Salama AH, Dmytryk JJ, Safiejko-Mroczka B. The relationship between receptor for advanced glycation end products expression and the severity of periodontal disease in the gingiva of diabetic and non diabetic periodontitis patients. Archives of Oral Biol. 2012;57:1342–54.
Allen EM, Matthews JB, O’Halloran DJ, Griffiths HR, Chapple IL. Oxidative and inflammatory status in type 2 diabetes patients with periodontitis. J Clin Periodontol. 2011;38:894–901.
Güçlü A, Erken HA, Erken G, Dodurga Y, Yay A, Özçoban Ö, et al. The effects of ozone therapy on caspase pathways, TNF-α, and HIF-1α in diabetic nephropathy. Int Urol Nephrol. 2016;48(3):441–50.
Petrarca C, Viola D. Redox Remodeling by Nutraceuticals for Prevention and Treatment of Acute and chronic inflammation. Antioxidants. 2023;12(1):132.
Fernández-Aparicio Á, Correa-Rodríguez M, Castellano JM, Schmidt-RioValle J, Perona JS, González-Jiménez E. Potential molecular targets of oleanolic acid in insulin resistance and underlying oxidative stress: a systematic review. Antioxidants. 2022;11(8):1517.
Dai S, Tian Z, Zhao D, Liang Y, Liu M, Liu Z, et al. Effects of Coenzyme Q10 supplementation on biomarkers of oxidative stress in adults: a GRADE-Assessed systematic review and updated Meta-analysis of Randomized controlled trials. Antioxidants. 2022;11(7):1360.
Jha JC, Banal C, Chow BS, Cooper ME, Jandeleit-Dahm K. Diabetes and kidney disease: role of oxidative stress. Antioxid Redox Signal. 2016;25(12):657–84.
Rapone B, Ferrara E, Santacroce L, Topi S, Gnoni A, Dipalma G, et al. The gaseous ozone therapy as a promising antiseptic adjuvant of Periodontal Treatment: a Randomized Controlled Clinical Trial. Int J Environ Res Public Health. 2022;19(2):985.
Rapone B, Ferrara E, Corsalini M, Converti I, Grassi FR, Santacroce L, et al. The Effect of Gaseous ozone therapy in conjunction with Periodontal Treatment on Glycated Hemoglobin Level in subjects with type 2 diabetes Mellitus: an unmasked Randomized Controlled Trial. Int J Environ Res Public Health. 2020;17(15):5467.
Touyz RM. Reactive oxygen species and angiotensin II signaling in vascular cells – implications in cardiovascular disease. Braz J Med Biol Res. 2004;37(8):1263–73.
Huberty CJ, Petoskey MD. In: Tinsley HEA, Brown SD, editors. Multivariate analysis of variance and covariance. Handbook of applied multivariate statistics and mathematical modeling. Academic Press; Eds.) 2000. pp. 183–208.
Steinberg D, Witztum JL. Is the oxidative modification hypothesis relevant to human atherosclerosis? Do the antioxidant trials conducted to date refute the hypothesis? Circulation. 2002;105(17):2107–11.
Burgos-Morón E, Abad-Jiménez Z, Martínez de Marañón A, Iannantuoni F, Escribano-López I, López-Domènech S, et al. Relationship between oxidative stress, ER stress, and inflammation in type 2 diabetes: the battle: continues. J Clin Med. 2019;8:1385.
Molins S, Mayer KU. Coupling between geochemical reactions and multicomponent gas and solute transport in unsaturated media: a reactive transport modeling study. Water Resour Res. 2007;43:W05435.
Beutler E, Duron O, Kelly BM. Improved method for the determination of blood glutathione. J Lab Clin Med. 1963;61:882–90.
Schulz KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials.
Apostolova N, Victor VM. Molecular strategies for targeting antioxidants to mitochondria: therapeutic implications. Antiox Redox Signal. 2015;22:686–729.
Kumar A, Grover V, Satpathy A, Jain A, Grover HS, Khatri M, et al. ISP good clinical practice recommendations for gum care. J Indian Soc Periodontol. 2023;27(1):4–30. https://doi.org/10.4103/jisp.jisp_561_22.
Field A. Discovering statistics using IBM SPSS statistics: north american edition. Sage Publications; 2017.
Kline RB. Principles and practice of structural equation modelling. Guilford Publications; 2005.
Miller GA, Chapman JP. Misunderstanding analysis of covariance. J Abnorm Psychol. 2001;110(1):40.
Newton RR, Rudestam KE. Your statistical consultant. Sage Publications; 2012.
Pituch KA, Stevens JP. Applied multivariate statistics for the social sciences. Routledge Academic; 2015.
Sagai M, Bocci V. Mechanisms of action involved in ozone therapy: is healing induced via a mild oxidative stress? Med Gas Res. 2011;1:29.
Arana C, Moreno-Fernández AM, Gómez-Moreno G, Morales-Portillo C, Serrano-Olmedo I, de la Cuesta Mayor MC, Martín Hernández T. Increased salivary oxidative stress parameters in patients with type 2 diabetes: relation with periodontal disease. Endocrinology: Diabetes Nutr. 2017;64:258–64.
Tricarico G, Rodrigues Orlandin J, Rocchetti V, Ambrosio CE, Travagli V. A critical evaluation of the use of ozone and its derivatives in dentistry. Eur Rev Med Pharmacol Sci. 2020;24(17):9071–93.
Acknowledgements
None.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
“Conceptualization: B.R.Methodology, B.R.Software, B.R. and E.F.Validation, B.R., E.F., E.Q., G.I., P.D., G.M.T., A.S. and F.I.Formal analysis, B.R. and E.F.Investigation, B.R. and G.M.T.Resources, B.R. and E.Q.Data curation, B.R., G.M.T., P.D. and F.I.Writing-original draft preparation, B.R.Writing-review and editing, B.R., E.F. and G.M.T.Visualization, B.R. and G.M.T.Supervision, B.R., A.S. and G.M.T.Project administration B.R., E.Q. and G.M.T.All authors read and approved the final manuscript.“
Corresponding author
Ethics declarations
Competing interests
All other authors have no competing interest.
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the local Ethics Committee of Albania University, Tiran, Albania (Reference Number 2018/224). This study was executed in accordance with the guidelines of the Declaration of Helsinki. All participants provided informed written consent prior to patient enrolment and randomization. The trial is registered with the ISRCTN registry, number ISRCTN17281691.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rapone, B., Ferrara, E., Qorri, E. et al. Research efficacy of gaseous ozone therapy as an adjuvant to periodontal treatment on oxidative stress mediators in patients with type 2 diabetes: a randomized clinical trial. BMC Oral Health 23, 278 (2023). https://doi.org/10.1186/s12903-023-02985-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-02985-1