
Abstract
Background
Khat leaves contain the alkaloid cathinone. Research shows that khat might provoke toxicity, mutagenicity, as well as carcinogenicity.
Methods
Two groups were identified as khat abusers and were categorized by abuse time and diagnosis of oral squamous cell carcinoma (OSCC). Here, 41 participants from Group 2 were short-term khat users, and 42 participants were long-term khat users. The control group included 30 healthy individuals.
The coding exons included nine cancer-related genes and were analysed. The histopathological research was conducted with H&E staining along with the TP53 protein expression by implementing immunohistochemical analyses.
Results
Here, 41 short-term khat users carried seven somatic mutations in four out of nine cancer-related genes: 29/41(70.73%) ARID1A, 24/41(58.53%) MLH1, 34/41(82.92%) PIK3CA and 36/41(87.80%) TP53. The 42 long-term khat users incorporated nine somatic mutations in five out of nin ecancer-related genes: 40/42(95.23%) ARID1A, 36/42(85.71%) ARID2, 29/42(69.04%) PIK3CA, 27/42(64.28%) MLH1, and 35/42(83.33%) TP53. Every khat user had somatic mutations related to OSCC affecting the gingiva and the lower lip. TP53 protein expression was confirmed in all immunohistochemical oral tests. Carcinoma was also positive in the histopathological analysis.
Conclusions
Khat is a mutagenic and carcinogenic plant that provoked OSCC among short-term khat users (<15 years of use) and long-term users (>15 years of use).
Similar content being viewed by others

Background
Oral squamous cell carcinoma (OSCC) is one of the most prevalent variations of cancer with high rates of spread in Asia [1,2,3,4]. Some epidemiological researches shows that with gradual reduction of oral cancer’s incidences in general, lethal outcomes related to OSCC have also markedly declined. In fact, this can be explained by improved lifestyle management, new opportunities for timely screening, and general progress of healthcare [5]. The frequency of OSCC is increasing because of risk factors associated with Middle Eastern populations [6]. Indeed, tobacco smoking is increasing in the Middle East [7]. Squamous cell carcinomas represent a wide spectrum of pathologies that can appear in tissues that serve as formal body barriers (oral cavity, oesophagus, lungs, airways, vulva, cervix, urethra, and human skin); they protect people from external environmental effects [8].
Catha Edulis Forsk or simply khat is a natural plant that belongs to the Ceastraceae family. Its leaves and sprouts can be chewed due to its similarity to amphetamines in the context of biology and associated stimulating reactions [9, 10]. Khat use is a cultural tradition and is used in different countries from the Middle East to Eastern Africa especially Saudi Arabia, Yemen, Kenya, and Eritrea. The khat’s leaves are commonly chewed at social venues. Fresh leaves are more prioritized for chewing including swallowing the liquid of the plant. The micro leftovers from the chewed plant typically stay in the mouth’s buccal sulcus in a unidirectional or bipartite position. If the leftovers stay in these positions for several hours, they still produce integral chemical elements [9, 11, 12]. Stimulants such as cathinone and cathine are included in khat’s biology, which explains why chewing the plant influences the user’s cognitive functions and emotional state.
Khat is a typical neurotransmitter that launches parasympathetic activity, thus resulting in the inevitable release of acetylcholine [12]. Research has shown that khat stimulates active release of a stress hormone known as norepinephrine and increasing the user’s alertness and overall vigilance [9, 12, 14]. Like any other neurotransmitter operating through acetylcholine receptors, khat leads to neurological disorders and increases the risk of cancer [12, 13]. Recent studies have demonstrated that nerves from the peripheral group (sympathetic, parasympathetic, and sensory) affect the emergence of tumours and activity of stromal cells, which may trigger the development of diverse physical and haematological pathologies and malignancies [13,14,15,16,17].
The current research examines short-term and long-term outcomes of using khat in male participants diagnosed with and without OSCC. Examination is completed by identifying somatic mutations via analysis of targeted gene panels including sequencing. This study also assessed the histopathological changes and possible immunohistochemical expressions among short-term (2 – 5 years) and long-term (above 5 years) users.
Methods
Human participants and ethical compliance
The study was conducted in accordance with the standards of the Deanship of Scientific Research for Princess Nourah Bint Abdulrahman University. The local ethics committee from KACST, Riyadh, Saudi Arabia approved the study (number H-01-R059, IRB LOG number 20-0242). In addition, all patients voluntarily provided written informed consent and released their samples for research purposes.
Respondents and clinical analysis
This study was retrospective research and covered 122 male participants to evaluate short-term (2–5 years) and long-term (above 5 years) outcomes of using khat in male participants diagnosed with and without OSCC between October 2020 - May 2021 in the Surgery & Dental/Maxillofacial Clinics, Histopathology and Biochemistry Laboratories at King Fahad Medical City, Riyadh, KSA. Medical history and reports of all patients were assessed to obtain demographic input and medical parameters.
Exclusion criteria
Exclusion criteria were a long history of smoking (above 10 years), chronic illnesses (for instance, diabetes and/or hypertension), and records of any cancer in family history (except khat usage as a reason).
Inclusion criteria
All patients who used khat before chemotherapy/radiotherapy and the ones diagnosed with OSCC were included in the final list. Their age varied between 51 and 70, and they fit the study’s criteria. In addition, healthy participants were selected for the control group with age ranging from 25 to 35 years old.
Study design and clinical analysis
This study included 113 participants in total were selected for the study and divided into three groups. The first category had 30 persons, i.e., control group with healthy individuals without any khat use. Patients who chewed khat were further distributed by groups based on duration of use and clinical analysis. In the second group, participants with short-term use of khat and OSCC diagnosis were included 41 patients. The third group included participants with long-term use of khat and OSCC diagnosis for a total of 42 patients. Table 1 below describe the study’s groups in detail.
Collection of samples
DNA extraction and blood samples
DNA extraction was performed using fresh peripheral blood samples (before surgery) from all the patients and healthy participants utilizing Qiagen DNA isolation kit (Catalogue Number 69,506, Quigen, Hilden, developed in Germany) according to the manufacturer’s instructions. The DNA samples’ concentration and quality were measured using a NanoDrop Spectrophotometer from Thermo Scientific (United States).
Targeted panel sequencing’s capture
Nine cancer-related genes was analysed: ARID1A, ARID2, TP53, NUMA1, CREBBP, NCOA2, PPP2R1A, MLH1, and PIK3CA. Sixty nanograms of DNA were reinforced by applying three associations of 502 primer pairs with a Ion AmpliSeq Comprehensive Cancer Panel developed by Life Technologies to cover each coding exon over 9 cancer-associated genes. Amplicon ligation used barcoded adaptors provided by Ion Amplicon Library Kit (the manufacturer is Life Technologies). Barcoded catalogues were further combined with sequencing beads by ensuring the prepared PCR emulsion. They were also amplified with a IonChef in compliance with Ion Torrent instructions (developed and provided by Life Technologies). The fragment analyser (AATI) and Qubit (Invitrogen) were selected as choices to define quality and the numerical value of enriched catalogues. The sequencing procedure was conducted using the ion proton sequencer and by applying the Ion PI chip in accordance with the manufacturer’s instructions.
Immunohistochemistry and Histological Analysis
Paraffin-embedded blocks of biopsy fragments were taken from short- and long-term users of khat with OSCC. The specimens were derived during surgical operations and prior to chemotherapy/radiotherapy procedures; 3- to 5-µm sections were made for histopathology and immunohistochemical tests. Furthermore, every block could generate a pair of slides. Eosin and haematoxylin were used. The sections with stains were scanned at increased magnification (20X) to evaluate the histopathological sites of the sections selected. They were then photographed using a photomicroscope. Finally, immunohistochemical tests were completed on the other slide from every block utilizing the TP53 antibody following the protocol [18].
Analysis of statistics
Raw data were generated from the sequencing procedure and was applied to the Hg19 genome of reference implementing the Ion Torrent Suite, Version 4.2. The extent of scope and coverage was defined with a help of the special plugin (Torrent Coverage Analysis). Another plugin (Torrent Variant Caller Version 4.2) was used to identify short insertions/deletions (INDELs) as well as single nucleotide variants (SNVs). Additionally, the special Variant Effect Predictor (VEP) was utilized to comment every item incorporating the library from COSMIC: v.70; dbSNP 138 and 1000 Genomes: phase 1. The items with coverage/scope less than 25 and frequency below 5% were excluded. Moreover, the research used in silico tests via a PolyPhen-2 [19] as well as SIFT [20] to determine whether the selected mutations transform into dangerous or non-harmful outcomes.
Pearson’s correlation coefficient was used by SigmaStat software Version 3.5 (Systat Software) for quantitative findings and were interpreted by comparing the standard deviation and mean values. P values < 0.05 were considered to be statistically significant.
Results
Malicious ARID1A, ARID2, CREBBP, NCOA2, NUMA1, PPP2R1A, MLH1, PIK3CA, and TP53 Gene mutations
After completing the clinical trials, nine of 92 respondents were excluded because they did not meet the study criteria. Thus, this study presented 83 participants who chewed khat: 41 participants were short-term khat users, and 42 participants were long-term khat users. All participants had somatic mutations and were diagnosed with OSCC on the gingival and lower lip areas; these conditions contrasted with the control group of 30 healthy participants. Eventually, 7 somatic mutations in four of nine cancer-related genes were identified in the short-term khat users. The incidence of somatic mutations was identified in the following order: 29/41(70.73%) ARID1A, 24/41(58.53%) MLH1, 34/41(82.92%) PIK3CA, and 36/41(87.80%) TP53. In turn, ARID2, NUMA1, CREBBP, NCOA2, and PPP2R1A showed no gene mutations.
On the other hand, nine somatic mutations in five of nine cancer-related genes were identified in the group of long-term khat users. Mutations were identified in the following order: 40/42(95.23%) ARID1A, 36/42(85.71%) ARID2, 29/42(69.04%) PIK3CA, 27/42(64.28%) MLH1, and 35/42(83.33%) TP53. There were no visible mutations in NUMA1, CREBBP, NCOA2, and PPP2R1A relative to the control group.
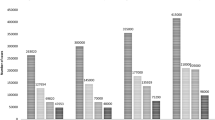
Somatic mutations related to all observable genes are provided in Table 2 for short-term khat users. Outcomes for long-term khat users are listed in Table 3. The incidence of genetic mutations for the two groups are evaluated and presented in Fig. 1. Moreover, there are no mutations in the DNA samples from the control group.

The incidence of genetic mutations for the two groups including short- and long-term khat users diagnosed with OSCC
Histopathology
Histopathological analysis involving photomicrographs based on deriving OSCC paraffin-embedded blocks of biopsy samples from affected gingival and lower lip areas. One of these paraffin-embedded blocks of biopsy samples was taken from a 70-year-old patient who had chewed khat since the age of 33 (e.g., a long-term khat abuser diagnosed with OSCC on the lower lip (Fig. 2). For the histopathological analysis, all the slides were prepared from the paraffin-embedded blocks of biopsy samples from the group of short-term khat users (Fig. 3a and b) as well as from the group of long-term khat users (Fig. 3c and d).

Images of a 70-year-old patient with khat chewing experience since the age of 33 (a long-term khat abuser diagnosed with OSCC on the lower lip) shows exophytic lesions (initiated two months ago). The clinical evaluation revealed the following: red-white exophytic lesion accompanied by dark discoloration, lack of sensation during palpation, history of fever, and no lymph nodes seen. Biopsy analysis revealed verrucous carcinoma on the lower lip

Images of micro-histopathology for H&E samples (with stain) (scale bar: 100 μm). SCC of the oral cavity areas (namely gingival and lower lip) indicates of dissymmetry among squamous cells; black circles are vascular invasion with abnormally sized cells with eminent red nucleoli (showed as yellow circles), pleomorphic big cells (related to yellow arrows), atypical mitotic effects, and some minor nucleoli. Panel a is gingival-related SCC, b is lower lip SCC related to the group of short-term khat users, c is gingival-related SCC, and d is lower lip SCC from the group of long-term khat users
Poorly differentiated cells with occasional histological structures were seen. For instance, there are pathological mitotic effects, certain patterns of proliferation disintegration, necrotic activity, vessels with thin walls, vascular invasion filled with red blood cells as well as pleomorphic cells with changing forms and various sizes of nucleoli. Meanwhile, the histopathological patterns were observed in the gingival and lower lip areas (Fig. 3c and d) from the group of long-term khat users.
Immunohistochemical findings for protein expression of TP53
Expression of TP53 was investigated using immunohistochemistry analysis, which can be seen in Fig. 4. Immunohistochemistry analysis revealed mainly positive protein expression of staining with TP53 antibody in the oral area (specifically gingival sites) in the short-term khat users. Strong and moderate protein expression for TP53 were identified in the same portion of histological oral areas in the group of long-term khat users. Immune staining was identified in 20% reactions for positive interactions with the special antibodies. This is why they have been interpreted as positive reactions (Fig. 4).

Photomicrographs of immune-stained areas applying TP53 antibody under a specific scale (100 μm). Immunohistochemical slides focused on staining with TP53 antibody. Samples showed a positive status for TP53 proteins among all khat users from the two groups. SCC of the oral cavity areas (gingival sites) was presented as follows: a gingival site SCC among short-term khat users; b gingival site SCC among long-term khat users
In addition, TP53 expression was identified in most oral (gingival sites) areas for both groups. Furthermore, the process of deriving antigens was computed in compliance with the most up-to-date quantitative H-scores for each situation and then by multiplying the values in relation to the following categories: more than 50% (strong), 20–40% (moderate), 1–20% (weak), and 0% (none) (Table 4).
Discussion
In general, oral cancer is seen in 10.5 adults per 100,000. The incidence of oral cancer is higher among males than females. The risks of having oral cancer grow with age [21]. Cancer related to the lips and oral cavity begin from mutations in squamous cells within thin and flat cells of the oral space. As a result, the mutations in squamous cells increase the risk of developing squamous cell carcinomas (SCC). Cancer-affected cells might penetrate into deeper tissues with cancer expansion [22]. The morbidity rates of oral cancer become systematically higher because of people’s vulnerability to various risk factors.6 Moreover, SCC emerges in tissues to ensure the effect of absorbance partition of the toxic/carcinogenic elements between a body and its exterior. These effects are manifested in barrier-related somatic systems including the oral cavity, oesophagus, lungs, airways, cervix, vulva, urethra, and skin [8, 23, 24].
Khat has a variety of constituent compounds and hence chewing khat leads to different health outcomes. In most cases, the person’s gastrointestinal system along with the nervous system become subjected to the plant’s effects [12, 25]. In human anatomy, the nervous system secures autonomic (peripheral) somatic reactions such as constipation, urine retention and some acute cardiovascular issues. In the meantime, the central nervous system is responsible for psychological effects such as elevated alertness, attention, dependence, resistance, and tolerance [12]. Fresh khat leaves contain cathinone—a typical alkaloid that affects the central nervous system [26]. Some research has confirmed toxicity, mutagenicity, carcinogenicity, teratogenicity, and congenital effects from consuming khat, i.e., mammalian cells and animal models [27, 28].
Other studies have reported that long-term use of khat leaves might provoke increased emergence of oral cancer [11, 12]. Moreover, other health complications are also related to khat consumption including oesophageal cancer, insomnia, anorexia, gastric problems, depression, liver disease, and a variety of cardiac problems [28,29,30,31,32]. Studies also suggest that regular khat chewing intensifies blood pressure, increased heart rate, [33, 34] and elevates LDL cholesterol [35,36,37].
This research showed that OSCC develops in participants who used khat. During the study, seven somatic mutations in four of nine cancer-related genes were recorded among short-term users of khat. In addition, nine somatic mutations were identified in the group of long-term khat users in five of nine cancer-related genes. Participants from both groups were diagnosed with OSCC.
There were four common cancer-related genes associated with somatic mutations in two groups of respondents: ARID1A, MLH1, PIK3CA, and TP53. Epidemiological research has shown that mutation processes in the selected genes are attributed to higher risks of OSCC development [38,39,40].
Two landmark mutation processes were identified in ARID1A and MLH1 related to DNA samples of long-term khat users, but a single landmark mutation was recorded in MLH1 taken from short-term khat users. This was arranged by comparing the results to DNA samples from the control group. Another substitution mutation was noticed in ARID2 and was related only to the group of long-term khat users. Noticeably, other studies assumed that systematic mutations in ARID2 contribute to the oral tumorigenesis, which can be triggered by dysregulation of NF-κB signaling [41,42,43] and by active long-term tobacco smoking [44]. Nevertheless, TP53 protein’s expression was positive in all immunohistochemical oral areas, which reflected rates of OSCC development in both groups. Moreover, all affected participants had mutations in TP53 genes—this is one of the most transforming genes in patients with OSCC diagnosis [45–48]. Histopathological tests also revealed poorly differentiated cells with unstable histological structure. This confirms the hypothesis that chewing khat, whether for short or long periods, eventually provoked OSCC.
Implications for behavioural health
The mutagenicity and carcinogenicity effects from using and chewing khat plant have been insufficiently studied in Arabian and Asian cultures especially in short-term and long-term perspectives. The fresh findings derived in this study demonstrated a positive relation between khat use for short and long periods and somatic mutations: These were identified in nine cancer-related genes, thus increasing the risk of developing OSCC. The research shows that khat usage provoked high and systemic mutations in four to five of nine cancer-related genes. This was associated with provoking OSCC in short term khat users who were chewing the plant between 10 and 15 years; the same effect was seen among long-term khat users who were chewing for more than 15 years. In all cases, OSCC was the most prevalent health risk, which underscores the serious health threat of using khat for stimulation.
Availability of data and materials
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
References
Yip TT, Ngan RK, Fong AH, et al. Application of circulating plasma/serum EBV DNA in the clinical management of nasopharyngeal carcinoma. Oral Oncol. 2014;50(6):527–38.
Alqahtani WS, Almufareh NA, Al-Johani HA, et al. Oral and oropharyngeal cancers and possible risk factors across Gulf Cooperation Council countries: a systematic review. World J Oncol. 2020;11(4):173.
Al-Jaber A, Al-Nasser L, El-Metwally A. Epidemiology of oral cancer in Arab countries. Saudi Med J. 2016;37(3):249.
Alqahtani WS, Almufareh NA, Domiaty DM, et al. Epidemiology of cancer in Saudi Arabia thru 2010–2019: a systematic review with constrained meta-analysis. AIMS Public Health. 2020;7(3):679.
Capote-Moreno A, Brabyn P, Muñoz-Guerra MF, et al. Oral squamous cell carcinoma: epidemiological study and risk factor assessment based on a 39-year series. Int J Oral Maxillofac Surg. 2020;49(12):1525–34.
Kujan O, Farah CS, Johnson NW. Oral and oropharyngeal cancer in the Middle East and North Africa: Incidence, mortality, trends, and gaps in public databases as presented to the Global Oral Cancer Forum. Transl Res Oral Oncol. 2017;2:2057178X17698480.
South AP, den Breems NY, Richa T, et al. Mutation signature analysis identifies increased mutation caused by tobacco smoke associated DNA adducts in larynx squamous cell carcinoma compared with oral cavity and oropharynx. Sci Rep. 2019;9(1):1–9.
Campbell JD, Yau C, Bowlby R, et al. Genomic, pathway network, and immunologic features distinguishing squamous carcinomas. Cell Rep. 2018;23(1):194–212.
Al-Mugahed L. Khat chewing in Yemen: turning over a new leaf: Khat chewing is on the rise in Yemen, raising concerns about the health and social consequences. Bull World Health Org. 2008;86(10):741–3.
Al-Hebshi N, Skaug N. Khat (Catha edulis)—an updated review. Add Biol. 2005;10(4):299–307.
Al-Maweri SA, Warnakulasuriya S, Samran A. Khat (Catha edulis) and its oral health effects: an updated review. J Invest Clin Dent. 2018;9(1):e12288.
Alshahrani SA, Almufareh NA, Almarshady B, et al. Effects of Consuming Catha Edulis Forsk (khat) on the Gene Manifestation of CHRM1 and CHRM3 in relation to Salivary Glands, Saliva Flow Rates, pH and Dental Caries in Yemeni Consumers. Open Dent J. 2020;14(1).
Faulkner S, Jobling P, March B, et al. Tumor neurobiology and the war of nerves in cancer. Cancer Discov. 2019;9(6):702–10.
Dasgupta A. Abuse of magic mushroom, peyote cactus, LSD, khat, and volatiles. In Critical issues in alcohol and drugs of abuse testing. Academic Press. 2019: 477–494.
Zahalka AH, Frenette PS. Nerves in cancer. Nat Rev Cancer. 2020;23:1–5.
Horvathova L, Mravec B. Effect of the autonomic nervous system on cancer progression depends on the type of tumor: solid are more affected then ascitic tumors. Endocrine Regul. 2016;50(4):215–24.
Kuol N, Stojanovska L, Apostolopoulos V, et al. Crosstalk between cancer and the neuro-immune system. J Neuroimmunol. 2018;315:15–23.
Suliman RS, Algebaly AS, Alqahtani WS. Role of human PTEN and TP53 sequence mutations in the Etiology of Breast Cancer in Saudi Patients. Pak J Biol Sci. 2020;23(3):321–30.
French SW, Lee J, Zhong J, et al. Alcoholic liver disease-Hepatocellular carcinoma transformation. J Gastrointest Oncol. 2012;3(3):174.
Yang J, Trépo E, Nahon P, et al. A 17-beta‐hydroxysteroid dehydrogenase 13 variant protects from hepatocellular carcinoma development in alcoholic liver disease. Hepatology. 2019;70(1):231–40.
Bosetti C, Carioli G, Santucci C, et al. Global trends in oral and pharyngeal cancer incidence and mortality. Int J Cancer. 2020;15(4):1040–9.
Conforti F, Pala L, Giaccone G, De Pas T. Thymic epithelial tumors: from biology to treatment. Cancer Treat Rev. 2020;86:102014.
Warnakulasuriya S, Greenspan JS. Epidemiology of oral and oropharyngeal cancers. WarnakulasuriyaGreenspaneditors Textbook of oral cancer. Berlin: Springer; 2020. p. 5–22.
Jiang X, Wu J, Wang J, et al. Tobacco and oral squamous cell carcinoma: a review of carcinogenic pathways. Tobacco induced diseases. 2019;17.
Al-Motarreb A, Al-Habori M, Broadley KJ. Khat chewing, cardiovascular diseases and other internal medical problems: the current situation and directions for future research. J Ethnopharmacol. 2010;132(3):540–8.
Balint EE, Falkay G, Balint GA. Khat–a controversial plant. Wiener Klinische Wochenschrift. 2009;121(19):604–14.
Pennings EJ, Opperhuizen A, Van Amsterdam JG. Risk assessment of khat use in the Netherlands: a review based on adverse health effects, prevalence, criminal involvement and public order. Regul Toxicol Pharmacol. 2008;52(3):199–207.
Al-Habori M. The potential adverse effects of habitual use of Catha edulis (khat). Expert Opin Drug Saf. 2005;4(6):1145–54.
Wiergowski M, Aszyk J, Kaliszan M, et al. Identification of novel psychoactive substances 25B-NBOMe and 4-CMC in biological material using HPLC-Q-TOF-MS and their quantification in blood using UPLC–MS/MS in case of severe intoxications. J Chromatogr B. 2017;1041:1–0.
Wabe NT. Chemistry, pharmacology, and toxicology of khat (Catha edulis forsk): a review. Addict Health. 2011;3(3–4):137.
Wabe NT, Mohammed MA. What science says about khat (Catha edulis Forsk)? Overview of chemistry, toxicology and pharmacology. J Exp Integrat Med. 2012;2(1):29–37.
Ademe BW, Brimer L, Dalsgaard A, et al. Chemical and microbiological hazards of Khat (Catha edulis) from field to chewing in Ethiopia. GSC Biol Pharm Sci. 2020;11(1):024–35.
Brenneisen R, Fisch HU, Koelbing U, et al. Amphetamine-like effects in humans of the khat alkaloid cathinone. Br J Clin Pharmacol. 1990;30(6):825–8.
Hassan NA, Gunaid AA, Abdo-Rabbo AA, et al. The effect of Qat chewing on blood pressure and heart rate in healthy volunteers. Trop Doctor. 2000;30(2):107–8.
Al-Motarreb A, Briancon S, Al‐Jaber N, et al. Khat chewing is a risk factor for acute myocardial infarction: a case‐control study. Br J Clin Pharmacol. 2005;59(5):574–81.
Al-Sharafi BA, Gunaid AA. Effect of habitual khat chewing on glycemic control, body mass index, and age at diagnosis of diabetes in patients with type 2 diabetes mellitus in Yemen. Clin Med Insights: Endocrinol Diabetes. 2015;8:CMED-S26045.
Hassan NA, Gunaid AA, Murray Lyon IM. Khat [Catha edulis]: health aspects of khat chewing. EMHJ-Eastern Mediterranean Health J. 2007;13(3):706–18.
Lui VW, Hedberg ML, Li H, Vangara BS, et al. Frequent mutation of the PI3K pathway in head and neck cancer defines predictive biomarkers. Cancer Disc. 2013;3(7):761–9.
Galot R, van Marcke C, Helaers R, et al. Liquid biopsy for mutational profiling of locoregional recurrent and/or metastatic head and neck squamous cell carcinoma. Oral Oncol. 2020;104:104631.
Husain N, Neyaz A. Molecular Diagnostics in Head and Neck Squamous Cell Carcinoma. In Molecular Diagnostics in Cancer Patients 2019 (pp. 165–185). Springer, Singapore.
Su SC, Lin CW, Liu YF, et al. Exome sequencing of oral squamous cell carcinoma reveals molecular subgroups and novel therapeutic opportunities. Theranostics. 2017;7(5):1088.
Ma X, Sheng S, Wu J, et al. LncRNAs as an intermediate in HPV16 promoting myeloid-derived suppressor cell recruitment of head and neck squamous cell carcinoma. Oncotarget. 2017;8(26):42061.
Er TK, Wang YY, Chen CC, et al. Molecular characterization of oral squamous cell carcinoma using targeted next-generation sequencing. Oral Diseases. 2015;21(7):872–8.
Liu H, Zhao H. Prognosis related miRNAs, DNA methylation, and epigenetic interactions in lung adenocarcinoma. Neoplasma. 2019;66(3):487–93.
Abrahao AC, Bonelli BV, Nunes FD, et al. Immunohistochemical expression of p53, p16 and hTERT in oral squamous cell carcinoma and potentially malignant disorders. Braz Oral Res. 2011;25:34–41.
Renzi A, De Bonis P, Morandi L, et al. Prevalence of p53 dysregulations in feline oral squamous cell carcinoma and non-neoplastic oral mucosa. Plos one. 2019;14(4):e0215621.
Su W, Sun S, Wang F, et al. Circular RNA hsa_circ_0055538 regulates the malignant biological behavior of oral squamous cell carcinoma through the p53/Bcl-2/caspase signaling pathway. J Transl Med. 2019;17(1):1–2.
Yao Y, Zhou WY, He RX. Down-regulation of JMJD5 suppresses metastasis and induces apoptosis in oral squamous cell carcinoma by regulating p53/NF-κB pathway. Biomed Pharmacother. 2019;109:1994–2004.
Acknowledgements
Not applicable.
Funding
This research was funded by the Deanship of Scientific Research at Princess Nourah Bint Abdulrahman University through the Fast-track Research Funding Program.
Author information
Authors and Affiliations
Contributions
SAA Methodology, Software Data curation, Writing-Reviewing and Editing. W.S.A. Carried out the design of the study, Conceptualization, Methodology, Performed the statistical analysis, Software Data curation, Visualization, Investigation, Writing- Original draft and submitted the paper as a corresponding author. N.A.A. Investigation, Software Data curation, Writing-Reviewing and Editing. D.M.D. Methodology, Visualization, Investigation, Software Data curation, Writing-Reviewing and Editing. G.I.A. Visualization, Investigation, Software Data curation, Writing-Reviewing and Editing. F.A.S. Methodology, Visualization, Investigation, Software Data curation, Writing-Reviewing and Editing. F.A.A. Software Data curation, Writing-Reviewing and Editing. M.A.A. Methodology, Investigation, Writing-Reviewing and Editing. T.M.A. Methodology, Investigation, Software Data curation, Writing-Reviewing and Editing. B.A.A. Methodology, Investigation, Writing-Reviewing and Editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alshahrani, S.A., Al-Qahtani, W.S., Almufareh, N.A. et al. Oral cancer among Khat users: finding evidence from DNA analysis of nine cancer-related gene mutations. BMC Oral Health 21, 626 (2021). https://doi.org/10.1186/s12903-021-01981-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-021-01981-7