
Abstract
Background
Numerous studies have revealed the role of dietary fatty acids in human health. However, few studies have evaluated dietary fatty acid patterns and their association with metabolic parameters. The current study aimed to explore the association between dietary fatty acid patterns and risk factors for metabolic syndrome (MetS) among overweight and obese adults.
Methods
This cross-sectional study involved 340 participants who were overweight or obese. The study included assessments of body composition and anthropometric measurements. Dietary fatty acid consumption was evaluated using a validated Food Frequency Questionnaire (FFQ) containing 168 items. Additionally, biochemical parameters, including serum total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), fasting serum glucose (FSG), and insulin levels, were measured using enzymatic methods. Fatty acid patterns were determined by principal component analysis (PCA), and the association between these dietary FA patterns and risk factors related to MetS components was assessed using logistic regression.
Results
Factor analysis conducted in this study explored three dietary fatty acid patterns: saturated fatty acids (SFA), polyunsaturated fatty acids (PUFA), and long-chain combined fatty acids (LC-CFA). Those at the highest tertile of the SFA pattern had lower diastolic blood pressure (DBP) (P = 0.03). Low-density lipoprotein cholesterol (LDL) was lower in the second and third tertiles (P ≤ 0.05). Also, higher fasting blood glucose (FBS) was observed in the second and third tertiles (P < 0.05), and the homeostatic model assessment of insulin resistance (HOMA-IR) was higher in the third tertile (P = 0.049). In the PUFA pattern, FBS was lower in the third tertile (P = 0.03). In the LC-CFA pattern, lower TC was achieved in higher tertiles (P = 0.04).
Conclusion
Our findings demonstrated that consuming high and moderate SFA patterns is associated with higher FBS and HOMA-IR. Also, increased consumption of SCFAs is related to lower DPB and LDL. Individuals who consumed more PUFA, especially linoleic acid, had lower FBS. These outcomes might be beneficial in managing MetS and leading to a new field of research.
Similar content being viewed by others

Background
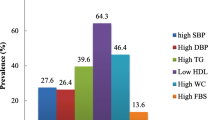
Metabolic syndrome (MetS) is a medical condition characterized by the combination of different metabolic risk factors [1], leading to various complications like obesity [2], cardiovascular disease (CVD) [3], and type 2 diabetes (T2D) [4]. Several organizations, such as the International Diabetes Federation [5], defined MetS as the presence of three or more risk factors, including abdominal obesity, elevated triglyceride (TG) levels, cholesterol imbalances, high blood pressure, and high fasting blood sugar. The increasing prevalence of MetS in developed and developing countries is a global concern [5]. Epidemiological studies show that MetS affects 20–45% of the population and is expected to rise to approximately 53% by 2035 [6]. MetS poses a significant clinical and public health challenge and an economic load on health systems and individuals [7]. Assessing MetS involves measuring indicators like waist circumference (WC), fasting blood glucose (FBG) levels, and TG levels commonly [8, 9]. The findings of multiple studies have validated the link between an unhealthy diet (e.g. diets high in sugars, saturated and trans-fats, low fiber foods, and high-sugar drinks contribute to non-communicable diseases (NCDs) and other health problems [10]) and the presence of MetS features.
On the other hand, adhering to a “healthy” dietary pattern (e.g. diets with appropriate proportions of micronutrients and macronutrients to support energetic and physiologic needs without excess intake [11]) has been shown to reduce MetS risk [12]. Among the nutritional factors, fatty acids, remarkably different types of fats, play a crucial role in developing or preventing MetS [13]. Fatty acids are an important energy source, essential components of membrane lipids, and act as cellular signaling molecules, contributing to MetS etiology [14]. Nevertheless, due to the limitations of studying single nutrients or foods, dietary pattern assessment has emerged as an alternative method for evaluating nutritional exposure in epidemiological research [15]. Analyzing the patterns of fatty acids reveals the interactions between various types of fatty acids and their complex associations with diseases. Combinations of multiple fatty acids may significantly influence MetS risk more than individual fatty acids alone [16]. Therefore, it is crucial to consider the intake of fatty acid patterns. However, the association between combinations of fatty acids and the development of MetS has not been evaluated to date. Thus, the present study aimed to identify specific dietary fatty acid patterns and investigate their relationships with MetS.
Materials and methods
This cross-sectional research included 347 overweight or obese individuals from Tabriz and Tehran, Iran. The study’s procedures and plans were approved and registered by the ethics committee at Tabriz University of Medical Sciences (registration code: IR.TBZMED.REC.1403.041).
Inclusion-exclusion criteria
Two recent projects were previously conducted in Tabriz and Tehran, Iran [17, 18]. Individuals were selected from outpatient clinics through public declaration and the dissemination of posters. The inclusion criteria for this study were individuals aged between 20 and 50 with a BMI between 25 and 40 kg/m2. Individuals with specific conditions, including pregnancy, breastfeeding, menopause, recent bariatric surgery, a history of CVD, cancer, hepatic or renal disease, diabetes mellitus, and taking any drugs and medications that affect weight, were not included in the study. Also, participants on a weight-loss regimen or taking supplements for at least three months before participating in the study were not included.
Demographics and anthropometric evaluations
We used a questionnaire to collect participants’ sociodemographic data, including age, gender, smoking habits, education level, marital status, employment, medical history, and family size. We calculated the socioeconomic status (SES) score based on this information. Education level was categorized using ordered categorical variables, ranging from illiterate (0) to higher education [5]. Similarly, occupational status was recorded using categories such as housewife, worker, student, freelancer, etc., for females, and without a job, rancher, farmer, worker, etc., for males. Family size was assigned scores of 1, 2, or 3 based on the number of family members. Participants were also given a score of 1 if they did not own a house and 2 if they did. We used bioelectrical impedance analysis (BIA) with the InBody 770 system (InBody Co., Ltd., Seoul, South Korea) specific equipment to assess body composition. Before measurement, participants were requested to avoid: drinking large amounts of water for at least 4 h before the test, dehydration, eating a large meal within 4 h before the test, strenuous exercise for at least 12 h before the test, and alcohol consumption at least 48 h before the test [19].
Height and weight were measured using a wall-mounted stadiometer and a Seca scale (Seca GmbH & Co. KG, Hamburg, Germany). The stadiometer had an accuracy of ± 0.1 cm, while the Seca scale used for weight measurement had an accuracy of ± 0.1 kg. These devices were regularly calibrated to ensure precise and consistent measurements during the study. Hip circumference (HC) was measured at the widest part of the buttocks, and WC was measured at the midpoint between the lowest rib and the hip bone. We also calculated the waist-to-hip ratio (WHR) and body mass index (BMI). A calibrated mercury sphygmomanometer was used to measure blood pressure twice at 15-minute intervals, and the average of the two readings was used for analysis. MetS components were defined based on the criteria provided by the US National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III). The participant’s physical activity levels were assessed using the short form of the International Physical Activity Questionnaire (IPAQ) [20].
Dietary assessment and its reliability and validity
A validated semi-quantitative Food Frequency Questionnaire (FFQ) consisting of 168 questions was employed to gather dietary information from the Iranian population [21] by a trained nutritionist. The nutritionist guided participants through the questionnaire, explaining each item and ensuring that participants understood the questions. All participants signed a written informed consent before participating in the study. Participants maintained diaries in which they recorded the frequency and quantity of each food item consumed daily, weekly, monthly, and yearly. The amount of food consumed was converted into grams per day using standard portion sizes, cooking factors, and edible portions as defined in the Iranian household measures manual [22]. The Nutritionist IV software (N Squared Computing, California, USA) was utilized to analyze daily dietary intakes. Given its reasonable relative validity and reproducibility correlations, this FFQ serves as a reliable tool for evaluating food group consumption and accurately ranking individuals based on their intake levels for each food group. The food items in the FFQ were categorized according to the nutrients they provided, including whole grains, refined grains, potatoes, dairy products, vegetables, fruits, legumes, meats, nuts and seeds, solid fat, liquid oil, tea and coffee, salty snacks, simple sugars, honey and jam, soft drinks, and desserts and snacks. To assess dietary salt consumption, the frequency of adding salt or salty sauce during food preparation or consumption and the frequency of consuming processed foods with a high salt content were considered [23]. Food items from the FFQ were converted into dietary fatty acids using the following formula:
The intake of dietary fatty acids in food of each item = the intake of food of each item (g/d) × the content of dietary fatty acids in the edible part of the food (100 g)/100 g.
The fatty acids and energy content reference is based on the USDA food database [24].
Biochemical evaluation
Blood pressure was measured with standard mercury sphygmomanometer. The measurement was performed twice in one arm and then the average of the two measurements was used. Before measuring blood pressure, participants were required to rest for at least 15 min in a seated position. Participants were asked to avoid any strenuous physical activity and to avoid consuming caffeinated beverages (such as coffee, tea, or energy drinks) for at least 30 min to one hour prior measurement [25]. All participants provided 10 milliliters of fasting venous blood for biochemical analysis. A commercial kit from Pars Azmoon in Tehran, Iran, was used to measure total serum cholesterol (TC), TG, high-density lipoprotein cholesterol (HDL-C), and FBG. Plasma and serum samples were separated by centrifugation at 4,500 rpm for 10 min at 4 degrees Celsius. Aliquots were frozen at -70 degrees Celsius before analysis. The Friedewald Eq. (37) was also used to calculate the low-density lipoprotein cholesterol (LDL-C) portion. Insulin levels in the blood were determined using enzyme-linked immunosorbent assay (ELISA) kits from Bioassay Technology Laboratory, Shanghai Korean Biotech Co., Shanghai, China. The Quantitative Insulin Sensitivity Check Index (QUICKI) and the Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) were calculated by dividing fasting insulin (IU/ml) by 22.5 fasting glucose (mmol/l): 1/ [log insulin (U/mL) + log glucose (mmol/L) during fasting].
Statistical analysis
The data was examined using SPSS software (IBM SPSS version 26.0) at a significant level of 0.05. Categorical variables were represented as frequency (percentage), while continuous variables were represented as mean [standard deviation (SD)]. The study utilized the USDA food database [24] to classify dietary FAs into 43 types, including 19 saturated fatty acids (SFAs), nine monounsaturated fatty acids (MUFAs), and 15 polyunsaturated fatty acids (PUFAs). Dietary FA patterns were derived through PCA with varimax rotation. The data structure was considered reasonable based on the Kaiser-Meyer-Olkin test (KMO = 0.6) and the Bartlett test of sphericity (P < 0.001). The number of patterns was determined by analyzing the scree plot and eigenvalues, factor interpretability, and total variance. Three patterns were identified, explaining 23.79%, 18.99%, and 14.13% of the total variance. PCA scores were calculated to assess each participant’s dietary fatty acid pattern, with the highest value indicating the compliance level with the respective pattern. The G-power software was utilized to determine the minimum sample size required for the study, considering a correlation coefficient (r) of 0.25, a significance level of 0.05, and a power of 80%, which resulted in a prediction of 315 participants. However, based on previous studies, considering a 10% drop-out rate [26, 27], the final sample size was 347 individuals, with 58.2% male and 41.8% female participants. To compare study parameters in different dietary patterns, the sample was divided into tertiles based on the study power of 80%; accordingly, the dietary fatty acid mean intake for the first, second and third tertiles of each pattern was as follows: first pattern (SFA pattern), 3.9, 6.2 and 12.95; second pattern (PUFA pattern), 1.27, 2.77 and 4.73 and in third pattern (LC-CFA pattern), 1.11, 2.31 and 8.08 respectively.
Analysis of variance (ANOVA) was used to assess the relationship between three dietary pattern groups and MetS components. Additionally, analysis of covariance (ANCOVA) was used to control for the impact of confounding variables, including age, sex, BMI, and total energy intake, on the association. Multinomial logistic regression was employed to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for the presence of cardiometabolic risk factors across the tertiles of patterns 1, 2, and 3. The models used for estimation were as follows: Model I (crude), Model II (adjusted for age and sex), and Model III (adjusted for age, BMI, sex, socioeconomic status, and energy intake). Dietary intake of macronutrients, micronutrients, and food groups are adjusted for dietary energy intake using the residual method.
Results
The fatty acid–factor loadings of the four major factors
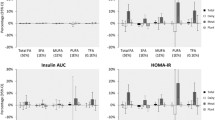
Figure 1 shows the correlation matrix for 43 different fatty acids. We conducted factor analyses on these 43 major fatty acids and found three factors that explained 56.92% of the variation in these variables in the study population. A similar pattern emerged in the cluster analysis, where fatty acids located near each other in the tree exhibited similar loading values (Fig. 1). We extracted three-factor scores for dietary fatty acids to create the fatty acid pattern score is a measure used in this study to quantify individual adherence to specific dietary fatty acid patterns identified through PCA. The fatty acid patterns score is derived from the factor loadings of various fatty acids in a dataset. It represents how much a participant’s dietary intake aligns with a particular pattern. score based on the primary contributors to each pattern (Table 1). Pattern 1 components mainly included 6:00, 8:0, 10:0, 4:0, 18:0, 18:0, 12:0, 16:0, and 14:0, characterized by the SFA pattern. Pattern 2 was characterized by high positive loadings from 18:2:6, 20:3:3, 20:3:9, 22:3:3, 22:6:3, 22:2:6, and 18:3:6, which was called the PUFA pattern. We characterized the third FA pattern as the long-chain combined fatty acids (LC-CFA) with a high factor loading of 20:5:3. 22:0, 12:1, 24:0, 23:0, and 21:0.

Principal components and clusters of 43 fatty acids. (A) The proportion of the total variance of 43 fatty acids is explained by each principal component. (B) Hierarchical cluster tree on the left and the heatmap of fat acid on the right
General demographic and anthropometric features
The general demographic and anthropometric features of study participants are represented in Table 2. As shown, participants in higher tertiles of the SFA pattern were younger than other tertiles (p < 0.001), and the percentage of being single was higher than other tertiles. Also, in a crude model, participants with higher consumption of the SFA pattern had higher weight, height, and WHR (p < 0.001, 0.04, and < 0.001, respectively) that lost their significance level after adjustment for confounders. In the PUFA pattern, individuals in the first tertile had lower SES and educational attainment (p = 0.01 for both variables). Men consumed higher tertiles of the PUFA pattern (p < 0.001). In the crude model of the PUFA pattern, higher height, basal metabolic rate (BMR), and fat-free mass (FFM) were achieved in higher tertiles (p < 0.001, 0.04, and 0.03, respectively). Also, those at the higher tertile of this pattern had significantly lower BMI and HC versus other tertiles (p < 0.001). None of these differences remained significant after adjustment for confounders.
Comparison of biochemical variables
Table 3 compares biochemical variables across different tertiles of SFA, PUFA, and LC-CFA patterns in crude and energy, age, gender, and BMI-adjusted models. In the crude model of the SFA pattern, participants in the lower tertile had higher SBP, DBP, and LDL-C (p = 0.04, < 0.001, and 0.03, respectively). In the adjusted model, DBP and LDL-C differences remained significant (p < 0.001 and 0.05, respectively). Also, in the adjusted model, QUICKI was significantly higher in the lowest tertiles (p = 0.02). In the crude model of the PUFA pattern, participants in the lowest tertile had lower SBP, DBP, and TG concentrations (p < 0.001 for all variables) that lost their significance level after adjustment for confounders. No significant difference was observed in the LC-CFA pattern.
In Tables 4 , 5, and 6, we examined the odds of biochemical variables in the second and third tertiles versus the first tertiles of dietary SFA, PUFA, and LC-CFA patterns. In the SFA pattern, those at the highest tertile were more likely to have higher DBP values compared with the reference tertile (P ≤ 0.05). Also, those at the second and third tertiles of the SFA pattern were more likely to have higher FBS values in models II and III (P < 0.05). FBS was higher in the third tertile compared with the first tertile in sex, age, and fully adjusted model models (OR = 1.042; CI = 1.005–1.080; P = 0.02, respectively). In the crude model, being at the third tertile of the SFA pattern was also associated with lower serum total cholesterol levels (p = 0.04), this difference was lost after adjustment for confounders in models II and III. HOMA-IR was significantly higher in the third versus first tertile in the fully adjusted model (OR = 1.200; CI = 0.998–1.444; P = 0.049). LDL was lower in the second tertile than the first tertile in all three models (P < 0.05), whereas in the third tertile, it was only significant in models I and II.
Those in the third tertile of the PUFA pattern (Table 5) were more likely to have higher SBP, DBP, and TG than those in the first tertile (P < 0.001 and 0.01 for all variables in models I and II). Lower HDL was observed in the third tertile versus the first tertile of the PUFA pattern in model I (P = 0.02). Also, lower FBS in the third tertile versus the first tertile of the PUFA pattern in model III was observed (OR = 0.971; CI = 0.945–0.990; P = 0.03). In the LC-CFA pattern (Table 6), TC was lower in the third versus first tertile in the fully adjusted model (OR = 0.987; CI = 0.975–0.999; P = 0.04).
Correlation between dietary fatty acid scores and food groups
Table 7 compares dietary macronutrients and some micronutrients across different tertiles of dietary fatty acid groups. As expected, there was an increase in almost all of the food ingredients in different tertiles of three dietary patterns. The comparison of food groups’ intake across different tertiles of dietary fatty acid patterns is shown in Table 8. Higher tertiles of the PUFA pattern were accompanied by higher intakes of vegetables, dairy, and vegetable fat (P < 0.001, 0.03, respectively). Also, higher LC-CFA tertiles were accompanied by higher intakes of fish, nuts, vegetables, vegetable oil, and eggs (P < 0.001).
Discussion
To the best of our knowledge, this research was the first to examine the relationship between dietary fatty acid patterns and MetS risk factors among people with obesity in Iran. In this cross-sectional study, three main fatty acid patterns were detected, i.e., the SFA pattern, the PUFA pattern, and the LC-CFA pattern. Based on our findings, participants with higher consumption patterns of SFA had higher FBS and HOMA-IR. However, these patients had lower DBP and LDL. Individuals with more PUFA and LC-CFA patterns had lower FBS and TC, respectively.
We observed that individuals who consumed more SFA had higher FBS and HOMA-IR. High HOMA-IR values indicate low insulin sensitivity [28]. There is still ongoing debate regarding the potential of SFAs to contribute to the development of insulin resistance (IR) and diabetes. In an animal study, Denhez et al. reported that SFAs trigger IR in podocytes [29]. A 20-year follow-up of the Finnish and Dutch cohorts by Feskens et al. indicated that consuming a high amount of fat, particularly SFA, increases the risk of developing glucose intolerance [30]. Review studies have shown a positive relationship between dietary SFA intake and IR in humans [31,32,33].
However, Liu et al. investigated the relationship between cancer and nutrition. They found no association between overall SFA intake and the risk of T2D in a Dutch cohort (Netherlands). Instead, the connection may be influenced by specific kinds of saturated fats and dietary origins [34]. An updated systematic review and dose-response meta-analysis of cohort studies conducted by Gaeini et al. showed no significant correlation between the consumption of overall SFA and the risk of developing T2D [35]. Additional research is required to explore the effects of SFA on glucose metabolism. The possible mechanism concerning dietary SFA and IR has also been extensively discussed. SFAs overload adipocytes, which are fat cells, causing an accumulation of diacylglycerol (DAG) [36]. This DAG buildup activates protein kinase C (PKC), desensitizing adipocytes to insulin. PKC further triggers pathways involving IKKβ and c-Jun N-terminal kinase (JNK) [37], leading to serine phosphorylation and degradation of IRS-1 and the release of proinflammatory cytokines [38]. SFAs also result in ceramide accumulation in adipocytes, which can activate IKK and JNK [39]. Additionally, accelerated β-oxidation of SFAs in mitochondria generates excess reactive oxygen species (ROS), all contributing to IR and adipocyte inflammation [40].
Another study finding was that consuming higher and moderate SFA patterns was associated with lower DPB and LDL, respectively. We have proposed the following hypothesis: Short-chain fatty acids (SCFAs) like 6:0, 8:0, and 10:0 have a high load in this pattern, and lower DBP and LDL are probably related to these fatty acids. In the literature, we found consistent results. Review studies have shown that SCFAs can directly regulate blood pressure and LDL [41,42,43,44]. SCFAs can lower blood pressure by binding to receptors like GPR41/GPR43, which activate pathways leading to vasodilation and reduced cAMP levels. SCFAs significantly reduce plasma TC via enhancing fecal excretion of bile acids and upregulating the gene expressions of sterol-regulatory element-binding protein 2 (SREBP2), low-density lipoprotein receptor (LDLR), and cholesterol seven alpha-hydroxylase (CYP7A1) in the liver, which lowers the serum LDL level [45].
This research demonstrated that higher consumption of the PUFA pattern was associated with lower FBS. Linoleic acid (LA) has the highest load in this pattern, followed by 20:3:3 and 20:3:9 fatty acids in the second and third place, respectively. Probably the most significant effects of the PUFA pattern are related to LA. Dietary intake of the PUFA pattern consists of vegetable oil, vegetables, and dairy. A dose-response meta-analysis of cohort studies performed by Hu et al. showed that a collaboration involving 20 studies across ten countries found that biomarker levels of LA were negatively correlated with the development of T2D.
Additionally, consuming PUFA (mostly LA) demonstrated better outcomes in terms of FBS, IR, and insulin secretion when compared to carbohydrates, saturated fats, and even monounsaturated fats (MUFA) in certain aspects [46]. Also, Telle-Hansen et al. concluded that supplementation with a daily dose of 0.42 to 5.2 g of PUFAs for a minimum of eight weeks might serve as a viable alternative therapy for managing T2D [47]. Another fatty acid with a high load in the PUFA pattern is omega-3 fatty acid. Studies have shown conflicting results. Liu et al. performed a meta-analysis of randomized controlled trials, in which the results showed that the addition of omega-3 supplementation has been shown to lower fasting plasma glucose (FPG) levels, reduce inflammatory markers, improve blood lipid metabolism, and alleviate IR in individuals diagnosed with gestational diabetes mellitus (GDM) [48]. Hussein showed that omega-3 supplementation enhanced FBS and increased plasma insulin sensitivity.
Furthermore, omega-3 supplementation improved and reduced glutathione levels in erythrocyte membranes and plasma [49]. Another single-masked randomized clinical trial performed by Chauhan et al. showed that omega-3 fatty acids do not appear to influence fasting and post-meal (postprandial) blood glucose levels or glycosylated hemoglobin (HbA1c) [50]. More studies are needed to investigate the impact of omega-3 fatty acids on glucose metabolism. The possible mechanism is as follows: PUFAs, including omega-3s, primarily impact blood sugar regulation by influencing insulin sensitivity, inflammation, and glucose metabolism [51]. PUFAs, particularly omega-3 fatty acids, and omega-6 fatty acids, specifically LA, enhance insulin sensitivity in cells, making them more responsive to insulin signals, thus facilitating glucose uptake and reducing blood sugar levels. PUFAs also combat inflammation by reducing the production of proinflammatory molecules [47, 52]. They influence gene expression related to glucose metabolism and activate genes involved in glucose uptake and utilization, ultimately improving insulin sensitivity [53]. PUFAs increase the activity of glucose transporters like GLUT4 [54], aiding glucose uptake by cells. They also reduce glucose release from the liver and promote glycogen storage [55].
The other outcome of this study was that higher consumption of the LC-CFA pattern was associated with lower TC. In this pattern, eicosapentaenoic acid (EPA) has the highest load. Dietary intake of this pattern contains fish, nuts, vegetables, vegetable oil, and eggs. These are good sources of EPA and omega-3 [56]. A systematic review and meta-analysis of data from 33 randomized controlled trials found that EPA supplementation reduced TC [57]. A systematic review revealed that in a seven-week study involving healthy men, a daily intake of 3.8 g of EPA decreased TC levels [58]. Mechanistically, most evidence indicates that omega-3 fatty acids tend to decrease the production and release of very low-density lipoprotein (VLDL) particles while simultaneously increasing the removal of TG from both VLDL and chylomicron particles. This effect is achieved by upregulating enzymes like lipoprotein lipase [59].
After adjustment using the residual method, energy-adjusted food groups in pattern 1 showed significant differences between low and high-fat dairy products. As expected, dairy products contain nutrients and bioactive compounds that can have both positive and negative effects on various metabolic parameters [60]. Calcium, magnesium, bioactive peptides, and SCFAs in dairy products can potentially lower DBP and LDL cholesterol levels [43, 60,61,62,63], while the high SFA content can lead to increased FBS and HOMA-IR [64]. Also, in pattern 2, there was a significant increase in high-fat dairy products, but the mean consumption was much lower than in pattern 1. Pattern 2 and 3 food groups were almost all attributed to the higher intake of vegetables. After the residual method adjustment for calorie intake, that was more significant than the others. Predictably, the high consumption of vegetables in these patterns has numerous health benefits, including high fiber, vitamins, minerals, antioxidants, and phytosterols [65]. These nutrients contribute to lower FBS and TC by improving insulin sensitivity, regulating blood sugar, and reducing cholesterol absorption. [66, 67].
The statistically significant effect size that we observed in the current study, shows a relatively small association between the variables examined. However, we do not expect to see substantial effects regarding the effect of food on our variables. Foods and nutrients often exert their influence on the body through subtle, chronic effects that may accumulate over time [68]. Therefore, dietary fatty acid patterns may have small effects on health, but their impact can be significant. even though the effects of dietary fatty acids may seem subtle, their impact on health can be profound.
Certain limitations should be considered when interpreting our findings. Firstly, our study had a cross-sectional design, so we cannot establish a causal relationship between fatty acid patterns and MetS components. We need further research with a prospective design to truly understand the direction of the association between fatty acid patterns and MetS. Secondly, even though we used a validated FFQ to assess dietary and fatty acid intakes, the closed-ended format of the questionnaires may have increased the chances of misclassification [69]. Nevertheless, any misclassifications would likely have a neutral effect on the odds ratios. Lastly, despite our efforts to control various confounding factors in our study, we must partially rule out the potential influence of residual confounders.
In summary, this research investigated the connection between dietary fatty acid patterns and the prevalence of MetS within the Iranian population. The findings of this study revealed that consuming high and moderate SFA patterns is associated with higher FBS and HOMA-IR. Also, increased consumption of SCFAs is related to lower DPB and LDL. Individuals who consumed more PUFA, especially LA, had lower FBS. Further studies are required to confirm our findings, particularly with a prospective design.
Data availability
The datasets generated and analyzed during the current study are not publicly available due to privacy and ethical considerations but can be obtained from the corresponding author upon reasonable request.
References
Sherling DH, Perumareddi P, Hennekens CH. Metabolic syndrome: clinical and policy implications of the new silent killer. J Cardiovasc Pharmacol Therap. 2017;22(4):365–7.
Belladelli F, Montorsi F, Martini A. Metabolic syndrome, obesity and cancer risk. Curr Opin Urol. 2022;32(6):594–7.
He Y, Xu M, Liu Y, Xu Y-J. Association of branched-chain fatty acids with metabolic syndrome: a systematic review and meta-analysis of observational studies. Food & Function; 2023.
Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365(9468):1415–28.
Miao MQ, Han YB, Liu L. Mitophagy in metabolic syndrome. J Clin Hypertens. 2023.
Engin A. The definition and prevalence of obesity and metabolic syndrome. Obes Lipotoxicity. 2017:1–17.
Grundy SM. Drug therapy of the metabolic syndrome: minimizing the emerging crisis in polypharmacy. Nat Rev Drug Discovery. 2006;5(4):295–309.
Cheng TO. Cardiac syndrome X versus metabolic syndrome X. Int J Cardiol. 2007;119(2):137–8.
Fahed G, Aoun L, Bou Zerdan M, et al. Metabolic syndrome: updates on pathophysiology and management in 2021. Int J Mol Sci. 2022;23(2):786.
Jones A, Rådholm K, Neal B. Defining ‘Unhealthy’: A Systematic Analysis of Alignment between the Australian Dietary Guidelines and the Health Star Rating System. Nutrients. 2018;10(4).
Cena H, Calder PC. Defining a healthy Diet: evidence for the role of contemporary dietary patterns in Health and Disease. Nutrients. 2020;12(2).
Suliga E, Kozieł D, Cieśla E, Głuszek S. Association between dietary patterns and metabolic syndrome in individuals with normal weight: a cross-sectional study. Nutr J. 2015;14:1–10.
Silva Figueiredo P, Carla Inada A, Marcelino G, et al. Fatty acids consumption: the role metabolic aspects involved in obesity and its associated disorders. Nutrients. 2017;9(10):1158.
Denisenko YK, Kytikova OY, Novgorodtseva TP et al. Lipid-induced mechanisms of metabolic syndrome. Journal of Obesity. 2020;2020.
Newby P, Tucker KL. Empirically derived eating patterns using factor or cluster analysis: a review. Nutr Rev. 2004;62(5):177–203.
Choi E, Ahn S, Joung H. Association of dietary fatty acid consumption patterns with risk of Hyper-LDL cholesterolemia in Korean adults. Nutrients. 2020;12(5):1412.
Abbasalizad Farhangi M, Vajdi M, Nikniaz L, Nikniaz Z. The interaction between dietary inflammatory index and 6 P21 rs2010963 gene variants in metabolic syndrome. Eating and Weight disorders-studies on Anorexia. Bulimia Obes. 2020;25:1049–60.
Khodarahmi M, Asghari-Jafarabadi M, Abbasalizad Farhangi M. A structural equation modeling approach for the association of a healthy eating index with metabolic syndrome and cardio-metabolic risk factors among obese individuals. PLoS ONE. 2019;14(7):e0219193.
Kyle UG, Bosaeus I, De Lorenzo AD, et al. Bioelectrical impedance analysis–part I: review of principles and methods. Clin Nutr. 2004;23(5):1226–43.
National Cholesterol Education Program. Adult Treatment Panel III (NCEP-ATP III) Criteria for the Metabolic Syndrome (MS) Are Unreliable in Children. 2023.
Mirmiran P, Esfahani FH, Mehrabi Y, et al. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 2010;13(5):654–62.
Ghaffarpour M, Houshiar-Rad A, Kianfar H. The manual for household measures, cooking yields factors and edible portion of foods. Tehran: Nashre Olume Keshavarzy. 1999;7(213):42–58.
Akhavanfar R, Hojati A, Kahrizi MS, et al. Adherence to lifelines diet score and risk factors of metabolic syndrome among overweight and obese adults: a cross-sectional study. Front Nutr. 2022;9:961468.
FoodData C. 2023.
The rules for measuring. blood pressure – and why they exist 2024 https://www.heart.org/en/news/2024/06/25/the-rules-for-measuring-blood-pressure-and-why-they-exist.
Wang X, Ji X. Sample size estimation in clinical research: from randomized controlled trials to observational studies. Chest. 2020;158(1):S12–20.
KEY, POINTS IN. SAMPLE SIZE WORKSHOP. 2022.
Bonora E, Formentini G, Calcaterra F, et al. HOMA-estimated insulin resistance is an independent predictor of cardiovascular disease in type 2 diabetic subjects: prospective data from the Verona Diabetes complications Study. Diabetes Care. 2002;25(7):1135–41.
Denhez B, Rousseau M, Spino C, et al. Saturated fatty acids induce insulin resistance in podocytes through inhibition of IRS1 via activation of both IKKβ and mTORC1. Sci Rep. 2020;10(1):21628.
Feskens EJ, Virtanen SM, Räsänen L, et al. Dietary factors determining diabetes and impaired glucose tolerance: a 20-year follow-up of the Finnish and Dutch cohorts of the Seven Countries Study. Diabetes Care. 1995;18(8):1104–12.
Calder PC. Functional roles of fatty acids and their effects on human health. J Parenter Enter Nutr. 2015;39:S18–32.
Risérus U. Fatty acids and insulin sensitivity. Curr Opin Clin Nutr Metabolic Care. 2008;11(2):100–5.
Sears B, Perry M. The role of fatty acids in insulin resistance. Lipids Health Dis. 2015;14(1):1–9.
Liu S, van der Schouw YT, Soedamah-Muthu SS, et al. Intake of dietary saturated fatty acids and risk of type 2 diabetes in the European prospective investigation into Cancer and Nutrition-Netherlands cohort: associations by types, sources of fatty acids and substitution by macronutrients. Eur J Nutr. 2019;58:1125–36.
Gaeini Z, Bahadoran Z, Mirmiran P. Saturated fatty acid intake and risk of type 2 diabetes: an updated systematic review and dose–response Meta-analysis of Cohort studies. Adv Nutr. 2022;13(6):2125–35.
Yang A, Mottillo EP. Adipocyte lipolysis: from molecular mechanisms of regulation to disease and therapeutics. Biochem J. 2020;477(5):985–1008.
Lučić I, Truebestein L, Leonard TA. Novel features of DAG-activated PKC isozymes reveal a conserved 3-D architecture. J Mol Biol. 2016;428(1):121–41.
Chen L, Chen R, Wang H, Liang F. Mechanisms linking inflammation to insulin resistance. International journal of endocrinology. 2015;2015.
Hammerschmidt P, Brüning JC. Contribution of specific ceramides to obesity-associated metabolic diseases. Cell Mol Life Sci. 2022;79(8):395.
Han CY. Roles of reactive oxygen species on insulin resistance in adipose tissue. Diabetes Metabolism J. 2016;40(4):272–9.
Wu Y, Xu H, Tu X, Gao Z. The role of short-chain fatty acids of gut microbiota origin in hypertension. Front Microbiol. 2021;12:730809.
Xiong R-G, Zhou D-D, Wu S-X, et al. Health benefits and side effects of short-chain fatty acids. Foods. 2022;11(18):2863.
Xu J, Moore BN, Pluznick JL. Short-chain fatty acid receptors and blood pressure regulation: Council on Hypertension Mid-career Award for Research Excellence 2021. Hypertension. 2022;79(10):2127–37.
Perna M, Hewlings S. Saturated fatty acid chain length and risk of Cardiovascular Disease: a systematic review. Nutrients. 2022;15(1).
Zhao Y, Liu J, Hao W, et al. Structure-specific effects of short-chain fatty acids on plasma cholesterol concentration in male Syrian hamsters. J Agric Food Chem. 2017;65(50):10984–92.
Hu M, Fang Z, Zhang T, Chen Y. Polyunsaturated fatty acid intake and incidence of type 2 diabetes in adults: a dose response meta-analysis of cohort studies. Diabetol Metab Syndr. 2022;14(1):34.
Telle-Hansen VH, Gaundal L, Myhrstad MC. Polyunsaturated fatty acids and glycemic control in type 2 diabetes. Nutrients. 2019;11(5):1067.
Liu W, Gao M, Yang S et al. Effects of omega-3 supplementation on glucose and lipid metabolism in patients with gestational diabetes: a meta-analysis of randomized controlled trials. J Diabetes Complicat. 2023:108451.
Hussein J, Mostafa E, El-Waseef M, et al. Effect of omega-3 fatty acids on erythrocyte membrane in diabetic rats. Macedonian J Med Sci. 2011;4(3):234–9.
Chauhan S, Kodali H, Noor J, et al. Role of omega-3 fatty acids on lipid profile in diabetic dyslipidaemia: single blind, randomised clinical trial. J Clin Diagn Research: JCDR. 2017;11(3):OC13.
Baynes HW, Mideksa S, Ambachew S. The role of polyunsaturated fatty acids (n-3 PUFAs) on the pancreatic β-cells and insulin action. Adipocyte. 2018;7(2):81–7.
Sinha S, Haque M, Lugova H, Kumar S. The effect of Omega-3 fatty acids on insulin resistance. Life (Basel). 2023;13(6).
Wilcox G. Insulin and insulin resistance. Clin Biochem Rev. 2005;26(2):19–39.
Lovejoy JC. Dietary fatty acids and insulin resistance. Curr Atheroscler Rep. 1999;1(3):215–20.
Merz KE, Thurmond DC. Role of skeletal muscle in insulin resistance and glucose uptake. Compr Physiol. 2020;10(3):785–809.
Ratledge C, Lippmeier C. In: Ahmad MU, editor. Chapter 7 - Microbial production of fatty acids. Fatty Acids: AOCS; 2017. pp. 237–78.
Zhang HJ, Gao X, Guo XF, et al. Effects of dietary eicosapentaenoic acid and docosahexaenoic acid supplementation on metabolic syndrome: a systematic review and meta-analysis of data from 33 randomized controlled trials. Clin Nutr. 2021;40(7):4538–50.
Innes JK, Calder PC. The Differential effects of Eicosapentaenoic Acid and Docosahexaenoic Acid on Cardiometabolic Risk factors: a systematic review. Int J Mol Sci. 2018;19(2).
Brinton EA, Mason RP. Prescription omega-3 fatty acid products containing highly purified eicosapentaenoic acid (EPA). Lipids Health Dis. 2017;16(1):23.
Timon CM, O’Connor A, Bhargava N et al. Dairy Consum Metabolic Health Nutrients. 2020;12(10).
Dickinson HO, Nicolson DJ, Cook JV et al. Calcium supplementation for the management of primary hypertension in adults. Cochrane Database Syst Rev. 2006(2):Cd004639.
Houston M. The role of magnesium in hypertension and cardiovascular disease. J Clin Hypertens (Greenwich). 2011;13(11):843–7.
Marcone S, Belton O, Fitzgerald DJ. Milk-derived bioactive peptides and their health promoting effects: a potential role in atherosclerosis. Br J Clin Pharmacol. 2017;83(1):152–62.
She Y, Wang K, Makarowski A, et al. Effect of High-Fat and low-fat dairy products on cardiometabolic risk factors and Immune function in a low Birthweight Swine Model of Diet-Induced insulin resistance. Front Nutr. 2022;9:923120.
Slavin JL, Lloyd B. Health benefits of fruits and vegetables. Adv Nutr. 2012;3(4):506–16.
Imai S, Fukui M, Kajiyama S. Effect of eating vegetables before carbohydrates on glucose excursions in patients with type 2 diabetes. J Clin Biochem Nutr. 2014;54(1):7–11.
Tang GY, Meng X, Li Y et al. Effects of vegetables on Cardiovascular diseases and related mechanisms. Nutrients. 2017;9(8).
Huang QC, Xu ZR, Han XY, Li WF. Effect of betaine on growth hormone pulsatile secretion and serum metabolites in finishing pigs. J Anim Physiol Anim Nutr (Berl). 2007;91(3–4):85–90.
Freudenheim JL, Johnson NE, Wardrop RL, Misclassification of Nutrient Intake Of Individuals. And Groups Using One-, Two-, Three-, and Seven-Day Food Records1. Am J Epidemiol. 1987;126(4):703–13.
Acknowledgements
The authors wish to thank all the study participants for their sincere collaboration. We also thank the Research Undersecretary of Tabriz University of Medical Sciences for their financial support (Grant number: 72955).
Funding
The present study was financially supported by a grant from Tabriz University of Medical Sciences (Code: IR.TBZMED.REC.1403.041 and grant number: 72955). The funders had no role in hypothesis generation, recruiting, or designing the study.
Author information
Authors and Affiliations
Contributions
All authors approved the final version of the article. RM and MAF contributed to study design, supervision, statistical analysis, and manuscript writing. RM was involved in manuscript writing and revision. MDR was involved in Figure illustrations. MAF and RM performed statistical analysis and was involved in hypothesis generation and figure illustration. FA was involved in data collection, data analysis and revision of article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All subjects provided written informed consent before participating in the study. We confirm that the methods followed the Declaration of Helsinki’s guidelines and regulations. Also, the legal guardians of the illiterate participants provided written informed consent. The study protocol was approved and registered by the ethics committee of Tabriz University of Medical Sciences (registration code: IR.TBZMED.REC.1403.041).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hemami, R.M., Farhangi, M.A., Rouzi, M.D. et al. Dietary fatty acid pattern and its association with metabolic profile among overweight and obese adults. BMC Endocr Disord 24, 141 (2024). https://doi.org/10.1186/s12902-024-01662-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-024-01662-w