
Abstract
Background
Although exercise seems to be beneficial for type 2 diabetes mellitus (T2DM) patients, there is limited research elucidating the optimal accessible indices of adiposity and insulin resistance for identifying elderly T2DM patients with poor glycemic control, which could be improved by performing regular exercise.
Methods
A community-based, cross-sectional study was conducted with 918 Chinese elderly individuals with T2DM in Zhejiang. Relevant risk factors for poor glycemic control, as determined using glycated haemoglobin A1c (HbA1c) > 7%, were explored using logistic regression analyses and included body mass index (BMI), waist circumference (WC), waist to height ratio (WHtR), fasting blood glucose (FBG), triglycerides (TGs), total cholesterol (TC), the product of fasting triglycerides and glucose (TyG), visceral adiposity index (VAI), lipid accumulation product (LAP), TyG-BMI, and TyG-WC. Comparisons of the risk factors’ ability to discriminate poor glycemic control as well as their optimal cutoff values were determined using receiver operating characteristic (ROC) analyses, and then the extent of poor glycemic control risk reduction through regular exercise was examined using multivariate logistic regression analyses.
Results
The overall poor glycemic control rate was 49.3%. The factors associated with poor glycemic control included FBG > 3.869, TyG > 8.73, TyG-BMI > 222.45, and TyG-WC > 713.48 in logistic regression analyses. The optimal cutoff points of FBG, TyG, TyG-WC, and TyG-BMI in discriminating poor glycemic control were 7.38, 9.22, 813.33, and 227.77, and their corresponding areas under the ROC curves were 0.864(0.840–0.886), 0.684(0.653–0.714), 0.604(0.571–0.635), and 0.574(0.541–0.606), respectively. Occasional and regular exercise reduced the odds ratios (95% confidence interval) of poor glycemic control to 0.187 (0.063–0.557) and 0.183 (0.059–0.571) for subjects with TyG-WC > 813.33 (p = 0.008), to 0.349 (0.156–0.782) and 0.284 (0.123–0.652) for subjects with TyG > 9.22 (p = 0.011), and to 0.390 (0.175–0.869) and 0.300(0.130–0.688) for subjects with TyG-BMI > 227.77 (p = 0.017), respectively, after adjusting for multiple confounding factors.
Conclusion
Among elderly individuals with T2DM, poor glycemic control risk might be identified using indices calculated from FBG, TG, BMI, and WC measurements, which are indicative of adiposity and insulin resistance. TyG-WC seems to be an accessible and useful indicator to identify which elderly T2DM patients would benefit from performing regular exercise to achieve good glycemic control.
Similar content being viewed by others

Background
Diabetes is one of the top 30 causes of years lived with disability, is affecting the elderly population and is becoming an important health issue in ageing global population [1]. In China, almost 60% of middle-aged and elderly population had prediabetes or diabetes in 2011–2012 [2], which will likely compromise the 33% premature mortality reduction goal between 2013 and 2030 even if all risk factors are attenuated [3]. Furthermore, diabetes-related cost accounts for a great proportion of the overall healthcare costs in China [4]. Therefore, it is necessary to optimize accessible measurements to identify individuals with suboptimal diabetes management to intervene as early as possible in China.
Type 2 diabetes mellitus (T2DM) management achievement could be assessed using integrative control targets, including fasting blood glucose, glycated haemoglobin A1c (HbA1c), blood pressure (BP), and lipid profile [5, 6]. HbA1c tests require sufficient health budget allocation and might not be readily accessible for constant diabetes management, especially in developing countries [7]. Recently, the product of fasting triglycerides and glucose, TyG index, appeared to be a simple and useful estimator of metabolic abnormalities, insulin resistance, T2DM onset and T2DM-related complication risk [8,9,10,11,12]. Alternative convenient indices, based on anthropometric parameters and lipid profile, have also been introduced to determine their association with impaired metabolic function and poor glycemic control in individuals with T2DM [13,14,15]. Despite the overall promising role of TyG, adiposity indices and TyG-adiposity integrated indices in predicting T2DM development and progression risk, their efficiency and optimal cutoff point for discriminating T2DM patients with poor glycemic control remains to be explored, especially for elderly individuals.
Physical activity and exercise have been demonstrated to be beneficial for individuals with T2DM by optimally controlling metabolic risk factors for diabetes management [16, 17]. Exercise-mediated glucose metabolism improvement might be attributed to adiposity and insulin resistance reduction, although the effective strategy of exercise (e.g., to what extent) to regulate glycemic homeostasis in elderly diabetic patients remains largely unknown [18,19,20]. The age-sensitive nature of HbA1c during ageing prompts the need to establish cutoff points of adiposity index for identifying the elderly population with abnormal glucose metabolism and other metabolic risks [21, 22]. Impaired glucose metabolism and the presence of adiposity and dyslipidemia might be related to insulin resistance, which contributes to physical inactivity for elderly individuals living in the community [23]. However, comprehensive knowledge of exercise, glycemic control, adiposity and insulin resistance remains to be established for elderly individuals with T2DM. Therefore, it would be interesting to quantify the effects of exercise frequency on reducing poor glycemic control risk of elderly T2DM patients as stratified by TyG or adiposity indices and to provide additional evidence for selecting exercise strategy to manage T2DM in elderly individuals with suboptimal glycemic control achievement.
This investigation aims to estimate the ability of TyG and other related metabolic risk factors to classify glycemic control status and to determine the appropriate index to discriminate elderly individuals with T2DM who are suitable candidates for regular exercise to improve glycemic control at the community level in Yongkang, Zhejiang, China.
Methods
Study participants
Data for this cross-sectional, observational study were retrieved from a local diabetes management system in Yongkang, Zhejiang, China. Subjects were residents aged ≥60 years and diagnosed with T2DM, and completed survey in March/April 2017. The procedure of this investigation is in accordance with the principles of the Declaration of Helsinki and is approved by the internal ethical review board of Zhejiang Provincial Center for Disease Control and Prevention, followed by acquiring informed consent from all participants.
Parameters and measurements
The measurements of peripheral blood specimens retrieved for this study include circulation lipids profile, fasting blood glucose (FBG), and HbA1c. Circulation lipids profile includes triglycerides (TGs), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C). TGs and TC levels (mmol/L) were determined using glycerol phosphate oxidase-p-aminophenazone assay and cholesterol oxidase-p-aminophenazone assay, respectively, while LDL-C and HDL-C levels (mmol/L) were measured using the clearance method with LDL-C Direct Reagents (Siemens Healthcare Diagnostics Inc) and Direct HDL-C Reagents (Siemens Healthcare Diagnostics Inc) in ARCHITECT c16000 autoanalyzer (Abbott, Shanghai, China). FBG levels (mmol/L) were measured using hexokinase method in ARCHITECT c16000 autoanalyzer (Abbott, Shanghai, China). HbA1c levels (%) were determined using high-performance liquid chromatography method in MQ-2000PT autoanalyzer (Medconn Technology, Shanghai, China).
Complications were recorded and categorized into microvascular, macrovascular, and other comorbidities as previously described [24]. There were 28 subjects with microvascular comorbidities (6 with nephropathy, 6 with retinopathy, and 16 with neuropathy), 70 subjects with macrovascular comorbidities (3 with congestive heart failure, 28 with myocardial infarction, and 39 with stroke), and 1 subject with other complications (hypoglycemia).
The indices collected for the current investigation include anthropometric parameters, questionnaire items, and BP records. The anthropometric parameters consisted of height in centimeters (cm), weight in kilograms (kg), and waist circumference (WC) in cm. In addition, body mass index (BMI) = weight /height2. WC-to-height ratio (WHtR) was determined as WC/height. The questionnaire items from face-to-face interviews included income status (low, medium, high), duration of diabetes (in years), tobacco smoking (yes or no), alcohol drinking (yes or no), anti-diabetic medication (yes or no), medication adherence (poor or good), exercise (no, occasional, regular), and self-reported blood glucose monitoring (yes or no). Good medication adherence referred to taking anti-diabetic medication at the appropriate dose at the time advised by the doctor. Otherwise, poor medication adherence was recorded. Regular exercise referred to exercise performed > 30 min/day and > 3 days/week, indicating that diabetic participants maintained acceptable physical activity. Occasional exercise referred to exercise maintained to some extent but that falls outside of the regular exercise criteria mentioned above. No exercise referred to scarce physical activity and no conscious of effort towards exercise maintenance. BP recordings included diastolic blood pressure (DBP) in mmHg and systolic blood pressure (SBP) in mmHg.
Visceral adiposity index (VAI), lipid accumulation product (LAP), TyG, and TyG-related index was calculated using the following formulae as previously described [13, 25]: VAI male = (WC/(39.68 + (1.88 × BMI))) × (TG/1.03) × (1.31/HDL-C); VAIfemale = (WC/(36.58 + (1.89 × BMI))) × (TG/0.81) × (1.52/HDL-C); LAPmale = (WC − 65) × TG; LAPfemale = (WC − 58) × TG; TyG = Ln(TG × FPG/2); TyG-BMI = TyG × BMI; TyG-WC = TyG × WC.
Definitions of glycemic control target, anthropometric variables, and hypertension
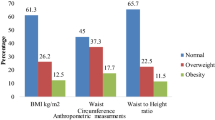
For glycemic control evaluation, HbA1c ≤ 7% is recognized as optimal glycemic control, while HbA1c > 7% is considered as poor glycemic control [26, 27]. HbA1c at 7% is moderate glycemic control target for elderly individuals with T2DM [28]. For anthropometric indices associated with metabolic risk, sex-specific cutoff values of BMI, WC, and WHtR are 24.12 kg/m2, 83.5 cm and 0.51 for males and 23.53 kg/m2, 77.5 cm and 0.49 for females, respectively, as derived from the Chinese elderly population [21]. Furthermore, sex-specific cut-off values of VAI and LAP associated with impaired glucose metabolism are 2.25 and 36.96 for Chinese males and 2.5 and 37.84 for Chinese females, respectively [29]. Hypertension is defined as SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg.
Statistical analysis
Quantitative data are reported as the mean with standard deviation or as the median with the 25th and 75th percentiles and were compared using independent t-tests or Mann-Whitney U tests depending on the normality of variables. Categorical variables were expressed as percentages and compared by Chi-square test or Fisher’s exact test where applicable. Correlation coefficients between two variables were determined using partial correlation analysis. Odds ratio (OR) with 95% confidence interval (CI) was calculated using binary logistic regression analysis to examine the effects of variables on glycemic control. The area under the receiver-operating characteristic (ROC) curve of the indicated variables was calculated with 95% CI, and the optimal cutoff point of variables for predicting poor glycemic control risk was determined according to the best Youden index (sensitivity+specificity-1). All statistical analyses were performed using IBM® SPSS® Statistics software (version 22.0) and MedCalc (version 18.11) and two-sided p value < 0.05 was considered statistically significant.
Results
Among the 918 diabetic subjects recruited here, their mean age, BMI, and WC were 69.40 ± 6.09 years, 24.36 ± 3.08 kg/m2, and 85.06 ± 9.03 cm, respectively. In addition, their mean glucose, HbA1c, TG, TC, LDL, HDL, SBP and DBP levels were 7.76 ± 2.39 mmol/L, 7.35 ± 1.47%, 1.91 ± 1.45 mmol/L, 5.06 ± 1.07 mmol/L, 2.50 ± 0.79 mmol/L, 1.19 ± 0.26 mmol/L, 133.26 ± 13.27 mmHg, and 77.59 ± 7.78 mmHg, respectively. The majority of subjects were diagnosed with T2DM in the last 5 years (43.4%), reached the glycemic control target (HbA1c ≤ 7%) (50.7%), were without complications (89.2%), received anti-diabetic medication (85.3%), were females (57.0%), were non-drinkers (85.7%), and were non-smokers (90.1%), respectively. Additionally, the complication classifications stratified by diabetes duration showed that the microvascular, macrovascular, and other comorbidity percentage was 3% (12/398), 8.3% (33/398), and 0% (0/398) in T2DM subjects diagnosed in the last 5 years; 3.1% (12/381), 8.4% (36/453), and 0.3% (1/381) in T2DM subjects diagnosed in the last 6–10 years; and 2.9% (4/139), 3.6% (5/139), and 0% (0/139) in T2DM subjects diagnosed more than 10 years ago, respectively (p = 0.509).
The characteristics of the 918 diabetic subjects stratified by the HbA1c cutoff point (≤7% vs. > 7%) are shown in Table 1. Median duration of diabetes, FBG, HbA1c, TC, TyG, TyG-BMI, and TyG-WC were significantly higher in subjects with HbA1c > 7% than in the other subjects, and the proportion of individuals with a longer diabetes history (more than 6 years), anti-diabetic medication utilization and exercise deficit was also greater. However, there were no significant differences in age, sex, smoking status, alcohol drinking status, income status, self-blood glucose monitoring, medication adherence, complication classifications, height, weight, WC, BMI, WHtR, TG, LDL-C, HDL-C, VAI, LAP, or BP between subjects with HbA1c > 7% and ≤ 7%.
The correlations between HbA1c and other metabolic risk factors are described in Table 2. HbA1c was significantly positively correlated with FBG (r = 0.765, p < 0.001), TC (r = 0.107, p = 0.009), TG (r = 0.105, p = 0.011), TyG (r = 0.383, p < 0.001), TyG-BMI (r = 0.152, p < 0.001), TyG-WC (r = 0.205, p < 0.001), VAI (r = 0.086, p = 0.037), and LAP (r = 0.084, p = 0.041). However, no significant association between HbA1c and HDL-C, LDL-C, BMI, WC, and WHtR was found.
The potential risk factors associated with HbA1c > 7.0% included TC > 5.71 mmol/L, FBG > 3.869 mmol/L, TyG > 8.73, TyG-BMI > 222.45, and TyG-WC > 713.48 in univariate logistic regression analyses (Table 3, Additional file 1). All these factors were also independently associated with HbA1c > 7.0%, except for TC, according to the results of multivariate logistic regression (Table 3). Moreover, ROC curve analysis showed the value of FBG, TyG, TyG-WC, TyG-BMI, and TC could classify individuals with HbA1c > 7.0%, although their efficiency differed. The AUCs (95% CI) were 0.864 (0.840–0.886) for FBG, 0.684 (0.653–0.714) for TyG, 0.604 (0.571–0.635) for TyG-WC, 0.574 (0.541–0.606) for TyG-BMI, and 0.547 (0.514–0.580) for TC (Table 4).
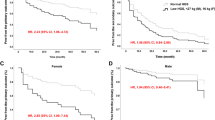
Diabetic subjects with poor glycemic control (HbA1c > 7.0%) were screened using the optimal cutoff value of indices as described in Table 4, followed by exploring the effect of exercise in reducing risk of HbA1c > 7.0%. As shown in Table 5 with Additional file 1, an increase in exercise frequency produced a significant decrease in HbA1c > 7.0% risk for diabetic subjects with TyG > 9.22 (p = 0.011), TyG-WC > 813.33 (p = 0.008), and TyG-BMI > 227.77 (p = 0.017). For instance, among diabetic subjects with TyG-WC > 813.33, their OR (95% CI) of HbA1c > 7.0% risk was reduced to 0.187 (0.063–0.557) for subjects taking occasional exercise and further decreased to 0.183 (0.059–0.571) for subjects performing regular exercise compared to subjects without exercise. However, there was no significant impact of exercise on HbA1c > 7.0% risk reduction for diabetic subjects with FBG > 7.38 or TC > 5.98.
Discussion
The good glycemic control rate from 2010 to 2012 was reported to be 32.6% nationally with recent glycemic control improvement in the southern-eastern part of China. However, discrepancies still existed between provinces and the relevant rates ranged from 49.7% in Ningbo, Zhejiang to 58.5% in Xiamen, Fujian [26, 30,31,32]. The updated data reflecting increased awareness and progress of diabetes management at the community level are presented here and indicate acceptable glycemic control and lifestyle, availability of anti-diabetic medication with good adherence, and low incidence of complications at least for elderly individuals with T2DM in 2017 in Yongkang, Zhejiang, China. In addition, poor glycemic control risk could be classified using FBG > 7.38, TyG > 9.22, TyG-WC > 813.33, and TyG-BMI > 227.77 with FBG being the most robust index. Nevertheless, poor glycemic control risk reduction through occasional and regular exercise appears to be much more effective for elderly T2DM patients with TyG-WC > 813.33 compared to the others with TyG > 9.22 and TyG-BMI > 227.77, suggesting that TyG-WC might be an accessible and auxiliary measurement to advice elderly T2DM patients to perform exercise for diabetes management.
Previous cross-sectional studies reported that HbA1c positively correlates with TC, TG, and LDL-C among T2DM patients in Turkey and Saudi Arabia but inversely associates with HDL-C in Saudi Arabian T2DM patients [33, 34]. Baseline HDL-C correlated with insulin resistance, but not with HbA1c, although lower HDL-C suggested a greater and earlier need for glycemic control in T2DM patients from a prospective intervention study in Australia [35]. Positive correlations between HbA1c and TC and TG were also observed, but HbA1c was not associated with LDL-C or HDL-C in Chinese elderly individuals with T2DM in this cross-sectional study. The inconsistent trend of changes between LDL-C and HbA1c were also reported in previous meta-analysis data [36] and elsewhere [37, 38], appearing to be dependent on the presence of lipid-lowering medication and cardiovascular diseases among individuals with T2DM [39].
The association between general/ central obesity measurements (e.g., BMI and WC) and uncontrolled glycemic status differed depending on the ethnic population investigated [15, 40, 41]. Abdominal adiposity, as determined using WHtR, has been demonstrated to be a better obesity indicator for predicting future T2DM risk in a meta-analysis based on prospective studies [42]. Moreover, sex-specific WHtR cutoff point might be helpful for predicting individuals with elevated HbA1c and subjects taking glucose-lowering medication in black South African population [43] and for screening T2DM subjects in Chinese population [44]. Sex-specific cutoff points of WC, BMI, and WHtR for Chinese elderly individuals are available [21], but might not be indicators of predicting poor glycemic control risk for elderly T2DM patients as presented here for the first time. The benefits of incorporation of almonds in a well-balanced healthy diet for improved glycemic and lipid control might be explained by decreased WC and WHtR values, as observed in a 24-week intervention study with 50 Asian Indian T2DM patients [45]. Nevertheless, the modification of diet on the relationship between anthropometric parameter-based adiposity index (e.g., BMI, WC, and WHtR) and glycemic control in the Chinese elderly individuals with T2DM remains to be investigated, which might provide possible evidence to optimize diet choice for diabetes management.
Recently, the anthropometric and lipid measurements-based visceral adiposity parameters (e.g., VAI and LAP) became effective and accessible indicators of insulin resistance in nondiabetic subjects [25] and exhibited promising performance in screening metabolic syndrome among the T2DM population [13], but showed no improved ability to indicate T2DM development [46]. Clinically, glycemic control improvement was evident in T2DM patients after 12 months of liraglutide treatment, which effectively reduced the VAI value [47]. In this filed study, neither VAI nor LAP was a useful tool for evaluating glycemic control in T2DM population regardless of sex, although positive correlations between VAI and LAP and HbA1c existed. Sufficient treatment information was available for patients recruited previously [47], which was not the case for the subjects investigated here due to the unavailability of BP and lipid control-related treatment. Nevertheless, VAI and LAP themselves might reflect lipid profile to some extent, and TC and TG were not independent risk factors for poor glycemic control, as indicated here. Furthermore, BP was further adjusted in our multivariate regression analysis. Sophisticated techniques, which directly measure visceral fat thickness and adipose hypertrophy, have revealed the potential role of adiposity in assessing glucose, lipid and insulin resistance in T2DM patients [48, 49]. Therefore, phenotype-based visceral adiposity measurements (e.g., VAI and LAP) should be simultaneously determined, followed by evaluation of their performance in predicting glycemic control status in individuals with T2DM in future field investigation.
To date, the positive correlation between TyG and TyG-adiposity parameters and the homeostasis model assessment of insulin resistance indicates that these parameters can be employed to recognize insulin resistance and metabolic syndrome in the research field without definitive discussion of these parameters in T2DM primary care guideline for clinical practice [8, 25, 50,51,52]. Previous studies have shown the role of TyG in predicting T2DM development risk among nondiabetic individuals [53] and in evaluating coronary artery stenosis risk among hyperglycemic individuals with poor glycemic control [54]. Nevertheless, TyG seemed to be a less robust predictor of future T2DM risk than FBG but more robust than TG, especially in individuals with impaired fasting glucose [55]. TyG measurement is inexpensive and routinely available and represents a useful tool to assess long term glycemic in T2DM patients with good correlation with HbA1c and insulin resistance [56]. The current finding considered TyG an indicator of poor glycemic control among hyperglycemic individuals, although TyG’s efficiency appeared to be lower than FBG but higher than TG. TyG with adiposity status has been proposed to be a surrogate marker for the early identification of insulin resistance [25] and of prediabetes and diabetes in first-degree relatives of T2DM patients [10]. Incremental increase in both TyG and BMI indicated an increased 8-year cumulative incidence of T2DM but appeared to have no obvious superiority in predicting T2DM risk compared to TyG being used as a forecasting determinant [53]. TyG appeared to discriminate metabolic unhealthy individuals independent of incremental increases in BMI and WC [9]. Neither TyG-BMI nor TyG-WC exhibited improved efficiency in discriminating T2DM patients with poor glycemic control compared to FBG or TyG in this study. Based on the finding mentioned above, FBG might be the most convenient and robust measurement to determine the risk of T2DM development and poor glycemic control, followed by TyG, TyG-WC, and TyG-BMI, respectively.
Exercise and weight loss may put T2DM into remission if applied early after diagnosis [57]. However, there is a concern that severe metabolic dysregulation could reduce benefit from exercise and exercise tends to exhibit metabolic benefit for T2DM patients with relative stable and good glycemic control [58]. T2DM subjects might suffer from dysmetabolic environment, endothelial, cardiac and peripheral dysfunction, or have insufficient exercise, which are likely attributed to insulin resistance [59]. Insulin resistance might be estimated using adiposity parameters (e.g., BMI, WC) [60, 61] or glucose and lipid-based indices (e.g., TyG) [7, 62]. For T2DM patients with higher level of HbA1c, increased exercise frequency per week seems to be an important approach to achieve favorable health outcome [63]. Among the Chinese elderly individuals with T2DM investigated here, subjects with TyG > 9.22, TyG-WC > 813.33, and TyG-BMI > 227.77 might be much better candidates to perform exercise to reduce poor glycemic control risk, which was not the case for subjects with FBG > 7.38 or TC > 5.98. Central obesity reduction seems to exert primordial function in glycemic control and personal characteristics must be taken into consideration for the choice of the best exercise modality for each elderly T2DM patient [18]. Coincidently, either occasional or regular exercise tended to maximally improve glycemic control, especially for subjects with TyG-WC > 813.33, which appeared to have higher specificity in predicting poor glycemic control compared to TyG > 9.22 or TyG-BMI > 227.77. Accordingly, exercise might be beneficial for glycemic control, especially for elderly T2DM patients with suspicious insulin resistance and adiposity, but not for elders with only elevated FBG or TC. This might be tentatively explained by the fact that exercise could increase insulin sensitivity and reduce resting insulin levels and body fat, thereby changing metabolic adaptions of T2DM patients [17]. Moreover, exercise could also decrease WC, body mass, BMI and the required hypoglycemic drug dose alone with improved glycemic control, which provided great benefits for T2DM patients who are with inadequate glycemic control and are worrying about possible injection therapy (e.g., insulin) as revealed in a recent lifestyle intervention study [64].
There are some limitations in this study. First, multiple risk factors associated with poor glycemic control are identified in this cross-sectional study, but their predictive values for evaluating glycemic control remained unknown. Second, exercise frequency is a categorical variable not an absolute frequency or amount of exercise, providing preliminary information regarding the potential benefit of regular exercise on glycemic control events for certain groups of elderly individuals with T2DM, but no definitive exercise training intensity advice. Third, the findings may or may not be applicable for T2DM patients with unstable conditions because this study recruited residents with T2DM living in the community but not T2DM cases at the hospital. Furthermore, the findings appear to be ethnic-dependent, which should be further tested in other ethnic T2DM populations.
Conclusions
The current data suggest that poor glycemic control risk might be screened using indices derived from FBG, TG, and anthropometric parameters indicative of adiposity and insulin resistance among elderly individuals with T2DM. Among them, TyG-WC seems to be an accessible and useful indicator to identify the most suitable elderly T2DM patients to perform regular exercise to achieve good glycemic control.
Availability of data and materials
The data are within the manuscript.
Abbreviations
- BMI:
-
body mass index
- BP:
-
blood pressure
- CI:
-
confidence interval
- DBP:
-
diastolic blood pressure
- FBG:
-
fasting blood glucose
- HbA1c:
-
glycated haemoglobin A1c
- HDL-C:
-
high-density lipoprotein cholesterol
- LAP:
-
lipid accumulation product
- LDL-C:
-
low-density lipoprotein cholesterol
- ORs:
-
odds ratios
- ROC:
-
receiver-operating characteristic
- SBP:
-
systolic blood pressure
- T2DM:
-
type 2 diabetes mellitus
- TC:
-
total cholesterol
- TG:
-
triglycerides
- TyG:
-
the product of triglycerides and glucose
- VAI:
-
visceral adiposity index
- WC:
-
waist circumference
- WHtR:
-
waist circumference to height ratio
References
GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211–59.
Zhao Y, Crimmins EM, Hu P, Shen Y, Smith JP, Strauss J, et al. Prevalence, diagnosis, and management of diabetes mellitus among older Chinese: results from the China health and retirement longitudinal study. Int J Public Health. 2016;61:347–56.
Li Y, Zeng X, Liu J, Liu Y, Liu S, Yin P, et al. Can China achieve a one-third reduction in premature mortality from non-communicable diseases by 2030? BMC Med. 2017;15(1).
Wu H, Eggleston KN, Zhong J, Hu R, Wang C, Xie K, et al. Direct medical cost of diabetes in rural China using electronic insurance claims data and diabetes management data. J Diabetes Investig. 2019;10:531–8.
Eeg-Olofsson K, Zethelius B, Gudbjörnsdottir S, Eliasson B, Svensson A, Cederholm J. Considerably decreased risk of cardiovascular disease with combined reductions in HbA1c, blood pressure and blood lipids in type 2 diabetes: report from the Swedish National Diabetes Register. Diab Vasc Dis Res. 2016;13:268–77.
Shi Q, Liu S, Krousel-Wood M, Shao H, Fonseca V, Shi L. Long-term outcomes associated with triple-goal achievement in patients with type 2 diabetes mellitus (T2DM). Diabetes Res Clin Pract. 2018;140:45–54.
Ang SH, Thevarajah M, Alias Y, Khor SM. Current aspects in hemoglobin A1c detection: a review. Clin Chim Acta. 2015;439:202–11.
Khan SH, Sobia F, Niazi NK, Manzoor SM, Fazal N, Ahmad F. Metabolic clustering of risk factors: evaluation of triglyceride-glucose index (TyG index) for evaluation of insulin resistance. Diabetol Metab Syndr. 2018;10:74.
Yu X, Wang L, Zhang W, Ming J, Jia A, Xu S, et al. The fasting triglycerides and glucose (TyG) index is more suitable for the identification of metabolically unhealthy individuals of Chinese adult population: a nationwide study. J Diabetes Investig. 2018. https://doi.org/10.1111/jdi.12975.
Navarro-Gonzalez D, Sanchez-Inigo L, Fernandez-Montero A, Pastrana-Delgado J, Martinez JA. TyG index change is more determinant for forecasting type 2 diabetes onset than weight gain. Medicine (Baltimore). 2016;95:e3646.
Jin JL, Sun D, Cao YX, Guo YL, Wu NQ, Zhu CG, et al. Triglyceride glucose and haemoglobin glycation index for predicting outcomes in diabetes patients with new-onset, stable coronary artery disease: a nested case-control study. Ann Med. 2018:1–11.
Zhang M, Wang B, Liu Y, Sun X, Luo X, Wang C, et al. Cumulative increased risk of incident type 2 diabetes mellitus with increasing triglyceride glucose index in normal-weight people: the rural Chinese cohort study. Cardiovasc Diabetol. 2017;16:30.
Ma CM, Lu N, Wang R, Liu XL, Lu Q, Yin FZ. Three novel obese indicators perform better in monitoring management of metabolic syndrome in type 2 diabetes. Sci Rep. 2017;7:9843.
Li S, Xiao J, Ji L, Weng J, Jia W, Lu J, et al. BMI and waist circumference are associated with impaired glucose metabolism and type 2 diabetes in normal weight Chinese adults. J Diabetes Complicat. 2014;28:470–6.
Bae JP, Lage MJ, Mo D, Nelson DR, Hoogwerf BJ. Obesity and glycemic control in patients with diabetes mellitus: analysis of physician electronic health records in the US from 2009-2011. J Diabetes Complicat. 2016;30:212–20.
Colberg SR, Sigal RJ, Fernhall B, Regensteiner JG, Blissmer BJ, Rubin RR, et al. Exercise and type 2 diabetes: the American College of Sports Medicine and the American Diabetes Association: joint position statement. Diabetes Care. 2010;33:e147–67.
Zanuso S, Sacchetti M, Sundberg CJ, Orlando G, Benvenuti P, Balducci S. Exercise in type 2 diabetes: genetic, metabolic and neuromuscular adaptations. A review of the evidence. Br J Sports Med. 2017;51:1533–8.
Ferriolli E, Pessanha FP, Marchesi JC. Diabetes and exercise in the elderly. Med Sport Sci. 2014;60:122–9.
Rohling M, Herder C, Roden M, Stemper T, Mussig K. Effects of long-term exercise interventions on Glycaemic control in type 1 and type 2 diabetes: a systematic review. Exp Clin Endocrinol Diabetes. 2016;124:487–94.
Motahari-Tabari N, Ahmad SM, Shirzad-E-Ahoodashty M, Yousefi-Abdolmaleki E, Teimourzadeh M. The effect of 8 weeks aerobic exercise on insulin resistance in type 2 diabetes: a randomized clinical trial. Glob J Health Sci. 2014;7:115–21.
Gu Z, Li D, He H, Wang J, Hu X, Zhang P, et al. Body mass index, waist circumference, and waist-to-height ratio for prediction of multiple metabolic risk factors in Chinese elderly population. Sci Rep. 2018;8:385.
Loh TP, Ma S, Heng D, Khoo CM. Age-related changes in the Cardiometabolic profiles in Singapore resident adult population: findings from the National Health Survey 2010. PLoS One. 2016;11:e162102.
Yang CW, Li CI, Li TC, Liu CS, Lin CH, Lin WY, et al. The joint association of insulin sensitivity and physical activity on the skeletal muscle mass and performance in community-dwelling older adults. Exp Gerontol. 2017;95:34–8.
Gordon J, McEwan P, Idris I, Evans M, Puelles J. Treatment choice, medication adherence and glycemic efficacy in people with type 2 diabetes: a UK clinical practice database study. BMJ Open Diabetes Res Care. 2018;6:e512.
Er LK, Wu S, Chou HH, Hsu LA, Teng MS, Sun YC, et al. Triglyceride glucose-body mass index is a simple and clinically useful surrogate marker for insulin resistance in nondiabetic individuals. PLoS One. 2016;11:e149731.
Li J, Chattopadhyay K, Xu M, Chen Y, Hu F, Chu J, et al. Glycaemic control in type 2 diabetes patients and its predictors: a retrospective database study at a tertiary care diabetes Centre in Ningbo, China. BMJ Open. 2018;8:e19697.
Yang W, Han P, Min KW, Wang B, Mansfield T, T'Joen C, et al. Efficacy and safety of dapagliflozin in Asian patients with type 2 diabetes after metformin failure: a randomized controlled trial. J Diabetes 2016;8:796–808.
Abbatecola AM, Paolisso G, Sinclair AJ. Treating diabetes mellitus in older and oldest old patients. Curr Pharm Des. 2015;21(13):1665–71.
Wang B, Zhang M, Liu Y, Sun X, Zhang L, Wang C, et al. Utility of three novel insulin resistance-related lipid indices for predicting type 2 diabetes mellitus among people with normal fasting glucose in rural China. J Diabetes. 2018;10:641–52.
Chen R, Ji L, Chen L, Chen L, Cai D, Feng B, et al. Glycemic control rate of T2DM outpatients in China: a multi-center survey. Med Sci Monit. 2015;21:1440–6.
Shan S, Gu L, Lou Q, Ouyang X, Yu Y, Wu H, et al. Evaluation of glycemic control in patients with type 2 diabetes mellitus in Chinese communities: a cross-sectional study. Clin Exp Med. 2017;17:79–84.
Zeng Y, Wu J, Han Y, Chen F, Chen L, Yang S, et al. Educational disparities in the associations between self-monitoring of blood glucose and glycemic control in type 2 diabetes patients in Xiamen. China J Diabetes. 2018;10:715–23.
Ozder A. Lipid profile abnormalities seen in T2DM patients in primary healthcare in Turkey: a cross-sectional study. Lipids Health Dis. 2014;13:183.
Khan HA, Sobki SH, Khan SA. Association between glycaemic control and serum lipids profile in type 2 diabetic patients: HbA1c predicts dyslipidaemia. Clin Exp Med. 2007;7:24–9.
Waldman B, Jenkins AJ, Davis TM, Taskinen MR, Scott R, O'Connell RL, et al. HDL-C and HDL-C/ApoA-I predict long-term progression of glycemia in established type 2 diabetes. Diabetes Care. 2014;37:2351–8.
Silverman J, Krieger J, Kiefer M, Hebert P, Robinson J, Nelson K. The relationship between food insecurity and depression, diabetes distress and medication adherence among low-income patients with poorly-controlled diabetes. J Gen Intern Med. 2015;30:1476–80.
Jalving AC, Gant CM, Binnenmars SH, Soedamah-Muthu SS, Bakker S, Navis G, et al. Glycemic control in the diabetes and lifestyle cohort Twente - a cross-sectional assessment of lifestyle and pharmacological management on Hba1c target achievement. Diabetes Obes Metab. 2018;20:2494–9.
Vazquez LA, Rodriguez A, Salvador J, Ascaso JF, Petto H, Reviriego J. Relationships between obesity, glycemic control, and cardiovascular risk factors: a pooled analysis of cross-sectional data from Spanish patients with type 2 diabetes in the preinsulin stage. BMC Cardiovasc Disord. 2014;14:153.
Hanefeld M, Traylor L, Gao L, Landgraf W. The use of lipid-lowering therapy and effects of antihyperglycaemic therapy on lipids in subjects with type 2 diabetes with or without cardiovascular disease: a pooled analysis of data from eleven randomized trials with insulin glargine 100 U/mL. Cardiovasc Diabetol. 2017;16:66.
Yousefzadeh G, Shokoohi M, Najafipour H. Inadequate control of diabetes and metabolic indices among diabetic patients: a population based study from the Kerman coronary artery disease risk study (KERCADRS). Int J Health Policy Manag. 2015;4:271–7.
Abebe SM, Berhane Y, Worku A, Alemu S, Mesfin N. Level of sustained glycemic control and associated factors among patients with diabetes mellitus in Ethiopia: a hospital-based cross-sectional study. Diabetes Metab Syndr Obes. 2015;8:65–71.
Kodama S, Horikawa C, Fujihara K, Heianza Y, Hirasawa R, Yachi Y, et al. Comparisons of the strength of associations with future type 2 diabetes risk among anthropometric obesity indicators, including waist-to-height ratio: a meta-analysis. Am J Epidemiol. 2012;176:959–69.
Ware LJ, Rennie KL, Kruger HS, Kruger IM, Greeff M, Fourie CM, et al. Evaluation of waist-to-height ratio to predict 5 year cardiometabolic risk in sub-Saharan African adults. Nutr Metab Cardiovasc Dis. 2014;24:900–7.
Xiao X, Liu Y, Sun C, Gang X, Cheng J, Tian S, et al. Evaluation of different obesity indices as predictors of type 2 diabetes mellitus in a Chinese population. J Diabetes. 2015;7:386–92.
Gulati S, Misra A, Pandey RM. Effect of almond supplementation on Glycemia and cardiovascular risk factors in Asian Indians in North India with type 2 diabetes mellitus: a 24-week study. Metab Syndr Relat Disord. 2017;15:98–105.
Kavaric N, Klisic A, Ninic A. Are visceral adiposity index and lipid accumulation product reliable indices for metabolic disturbances in patients with type 2 diabetes mellitus? J Clin Lab Anal. 2018;32(3).
Russo GT, Labate AM, Giandalia A, Romeo EL, Villari P, Alibrandi A, et al. Twelve-month treatment with Liraglutide ameliorates visceral adiposity index and common cardiovascular risk factors in type 2 diabetes outpatients. J Endocrinol Investig. 2015;38:81–9.
Kim SK, Hur KY, Kim HJ, Shim WS, Ahn CW, Park SW, et al. The increase in abdominal subcutaneous fat depot is an independent factor to determine the glycemic control after rosiglitazone treatment. Eur J Endocrinol. 2007;157:167–74.
Monickaraj F, Gokulakrishnan K, Prabu P, Sathishkumar C, Anjana RM, Rajkumar JS, et al. Convergence of adipocyte hypertrophy, telomere shortening and hypoadiponectinemia in obese subjects and in patients with type 2 diabetes. Clin Biochem. 2012;45:1432–8.
Du T, Yuan G, Zhang M, Zhou X, Sun X, Yu X. Clinical usefulness of lipid ratios, visceral adiposity indicators, and the triglycerides and glucose index as risk markers of insulin resistance. Cardiovasc Diabetol. 2014;13:146.
Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6:299–304.
Aschner P. New IDF clinical practice recommendations for managing type 2 diabetes in primary care. Diabetes Res Clin Pract. 2017;132:169–70.
Navarro-Gonzalez D, Sanchez-Inigo L, Pastrana-Delgado J, Fernandez-Montero A, Martinez JA. Triglyceride-glucose index (TyG index) in comparison with fasting plasma glucose improved diabetes prediction in patients with normal fasting glucose: the vascular-metabolic CUN cohort. Prev Med. 2016;86:99–105.
Lee EY, Yang HK, Lee J, Kang B, Yang Y, Lee SH, et al. Triglyceride glucose index, a marker of insulin resistance, is associated with coronary artery stenosis in asymptomatic subjects with type 2 diabetes. Lipids Health Dis. 2016;15:155.
Zheng S, Shi S, Ren X, Han T, Li Y, Chen Y, et al. Triglyceride glucose-waist circumference, a novel and effective predictor of diabetes in first-degree relatives of type 2 diabetes patients: cross-sectional and prospective cohort study. J Transl Med. 2016;14:260.
Hameed EK. TyG index a promising biomarker for glycemic control in type 2 diabetes mellitus. Diabetes Metab Syndr. 2019;13:560–3.
Ades PA. A lifestyle program of exercise and weight loss is effective in preventing and treating type 2 diabetes mellitus: why are programs not more available. Prev Med. 2015;80:50–2.
Plomgaard P, Weigert C. Do diabetes and obesity affect the metabolic response to exercise? Curr Opin Clin Nutr Metab Care. 2017;20:294–9.
Reusch JE, Bridenstine M, Regensteiner JG. Type 2 diabetes mellitus and exercise impairment. Rev Endocr Metab Disord. 2013;14:77–86.
Kahn HS, Cheng YJ. Comparison of adiposity indicators associated with fasting-state insulinemia, triglyceridemia, and related risk biomarkers in a nationally representative, adult population. Diabetes Res Clin Pract. 2018;136:7–15.
Chen S, Chen Y, Liu X, Li M, Wu B, Li Y, et al. Insulin resistance and metabolic syndrome in normal-weight individuals. Endocrine. 2014;46:496–504.
Unger G, Benozzi SF, Perruzza F, Pennacchiotti GL. Triglycerides and glucose index: a useful indicator of insulin resistance. Endocrinol Nutr. 2014;61:533–40.
Harmer AR, Elkins MR. Amount and frequency of exercise affect glycaemic control more than exercise mode or intensity. Br J Sports Med. 2015;49:1012–4.
Sbroma TE, Pippi R, Reginato E, Aiello C, Buratta L, Mazzeschi C, et al. Intensive lifestyle intervention is particularly advantageous in poorly controlled type 2 diabetes. Nutr Metab Cardiovasc Dis. 2017;27:688–94.
Acknowledgments
Not applicable.
Funding
This work was supported by the Ministry of Science and Technology [grant numbers: 2016YFC0901200, and 2016YFC0901205]; and Science Technology Department of Zhejiang Province [grant number: 2017C33090]. The funding body has no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
Acquisition, analysis of data and writing the manuscript: HTZ; design of the work, analysis, interpretation of data, writing and substantively revising the manuscript: MY; acquisition, interpretation of data and substantively revising the manuscript: HH, QFH, and JP; conception of the work, interpretation of data, substantively revising the manuscript, Funding Acquisition and Supervision: RYH. All authors have read and approved the manuscript.
Authors’ information
Hong-Ting Zhu MD, Min Yu MD, MPH, PhD, Hao Hu MD, Qing-Fang He MPH, Jin Pan MPH, Ru-Ying Hu MD.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The procedure of this investigation, including the form of consent, is in accordance with the principles of the Declaration of Helsinki and approved by internal ethical review board of Zhejiang Provincial Center for Disease Control and Prevention, followed by acquiring written informed consent from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
β and S.E. of parameter corresponding to binary logistic regression results. (DOCX 27 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Zhu, HT., Yu, M., Hu, H. et al. Factors associated with glycemic control in community-dwelling elderly individuals with type 2 diabetes mellitus in Zhejiang, China: a cross-sectional study. BMC Endocr Disord 19, 57 (2019). https://doi.org/10.1186/s12902-019-0384-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-019-0384-1