
Abstract
Bacground
To assess the contribution of macroprolactin to high serum prolactin levels and their association with thyroid status and thyroid autoimmunity during pregnancy.
Methods
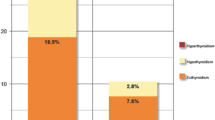
138 pregnant women who suspected of having thyroid dysfunction were studied and divided into three groups according to the thyroid status; group 1; euthyroidism (n 40), group 2; hypothyroidism (n 54), and group 3; hyperthyroid (n 44). Polyethylene glycol (PEG) precipitation method was used for detection of macroprolactin. A percentage recovery of 40 % or less is considered as macroprolactinemia. If macroprolactin was negative, the percentage of monomeric prolactin recovery (monoPRL %) after PEG precipitation was used for comparison between the groups.
Results
Macroprolactinemia was found in two patients (1.4 %) one from hypothyroid and other from euthyroid group. Basal prolactin levels in these patients were 400 and 403 ng/mL respectively. Referring to all patients, there was no correlation between PRL, macroPRL or monoPRL % with thyroid hormone status and also with the serum levels of thyroid antibodies (p > 0.05). A positive correlation was observed between the serum levels of PRL with TSH (p = 0.014 and r = 0.219), while a negative correlation was found with FT4 (p = 0.011 and r = −0.227).
Conclusions
Despite the fact that serum prolactin levels were found to be high during pregnancy, the contribution of macroprolactin was found to be insignificant in our study. Unlike other auto immune diseases, we could not find any relationship between thyroid autoimmunity and PRL, macroPRL or monoPRL %. These results confirmed that measured prolactin was quite homogeneous during pregnancy.
Similar content being viewed by others


Background
Prolactin, a protein hormone, is secreted from the anterior pituitary usually in response to physiological and rarely pathological stimuli. Prolactin concentrations begin to increase after 6 weeks of pregnancy and reach the highest level in late pregnancy to prepare the mammary glands of the breasts for the production of milk [1–3]. It is well known that circulating prolactin is not homogenous and three different forms are defined according to molecular size: monomeric PRL (monoPRL), big PRL (bigPRL), and macroprolactin (macroPRL). Macroprolactin is described as a complex of PRL with immunoglobulin G (IgG) which is related to antiprolactin autoantibodies. This formulation of PRL may cause limited bioactivity, bioavailability and clearance from the glomerulus. Macroprolactinemia is usually asymptomatic, patients with macroprolactinemia do not need further therapy, and pregnancy is possible without any treatment for such hyperprolactinemia [4–6]. Although the gold standard method for detecting macroPRL is gel filtration chromatography, precipitation with polyethylene glycol (PEG) is a widely used screening test. A low PRL recovery, <40 %, after PEG precipitation indicates the presence of macroPRL [7, 8]. In hyperprolactinemic states, the contribution of macroprolactin has been found to be 10 to 25 % of prolactin and macroprolactinemia may be present in about 0.2–3.6 % of the general population [9].
Normal maternal thyroid function is essential for both fetal and maternal health and many physiological alterations occur during pregnancy. Human chorionic gonadotropin (hCG) and estrogen are two pregnancy-related hormones responsible for increased thyroid hormone levels in the blood. Thyroid disorders, particularly those with autoimmune origin, are common in women of reproductive age and both hypo and hyperthyroidism were reported to be associated with poor pregnancy outcome [10–12]. Therefore, different trimester-specific reference ranges were defined to distinguish physiological alterations from pathological states [13–15]. It has been shown that the thyrotropin-releasing hormone (TRH) can stimulate the secretion of prolactin in experimental conditions; however its physiological influence is not so obvious. Hypothyroidism may cause pituitary and thyrotrophic hyperplasia which result in elevated TRH and prolactin release. The high levels of both hormones may return to normal after effective thyroid hormone replacement therapy [16, 17].
Previous studies have shown that prolactin also plays an essential role in metabolism and regulation of the immune system and macroprolactin has been described as the major immune reactive prolactin species in the serum of several subjects before and during pregnancy. The relationship with anti-PRL autoantibodies and autoimmune disorders has been investigated in some studies due to the structure of macroprolactin [18, 19]. Although some case reports have shown interaction between macroprolactinemia and autoimmune thyroid disorders, other studies examining a large number of patients revealed no specific association. It has been shown that only a minority of patients with SLE had higher frequencies of macroprolactinemia [20, 21]. The association of prolactin and macroprolactin with thyroid hormones and thyroid autoantibodies during pregnancy has not been studied before.
In the present study, we aimed to assess the contribution of macroprolactin to high serum prolactin levels and the association of prolactin (PRL) and macroprolactin (macroPRL) levels with thyroid status and thyroid autoimmunity during pregnancy.
Methods
The study, designed as a prospective case series, was conducted between March 2014 and December 2014 in the Sevket Yılmaz Research and Education Hospital, Bursa, Turkey. Data were collected by selecting pregnant women who had undergone a TSH screening and been directed to endocrinology consultation. The study protocol was approved by the local ethics committee. A total of 138 pregnant women suspected of having thyroid dysfunction, and who gave informed consent, were studied in different stages of gestation. All subjects were interviewed regarding reproductive history including miscarriages, preterm deliveries, and neonatal complications. Personal histories of thyroid disorders and thyroid medications were noted. Selected patients were divided into three groups according to the ATA guidelines; Group 1 euthyroid (TSH between 0.1 μIU/L and 2.5 μIU/L), group 2 hypothyroid (TSH ≥ 2.51 μIU/L), and group 3 hyperthyroid (TSH ≤ 0.09 μIU/L). The TPOAb ≥ 35 U/mL was considered to be antibody positive also according to ATA guidelines [15]. History of the following complications during previous pregnancies were considered to be complicated pregnancy; miscarriage, stillbirth, preterm birth, fetal death, postpartum hemorrhage, placental abruption, cardiac dysfunction and maternal heart failure, gestational hypertension, preeclampsia, gestational diabetes, and cesarean sections.
Laboratory investigation
Following an overnight fast, blood samples were acquired in the morning from each subject. Serum was isolated by centrifugation and stored at −80 °C until testing, if needed. The concentrations of serum TSH, FT3 and FT4 were detected by electrochemiluminescence immunoassay diagnostic kit (Advia Centaur XP Siemens, USA). TGAb and TPOAb levels were detected using an electrochemiluminescence immunoassay diagnostic kit (Roche Diagnostics Ltd., Basel, Switzerland). The concentration of serum prolactin was detected by electrochemiluminescence immunoassay diagnostic kit (Immulite 2000, Diagnostic Products Corporation, LA, CA). After centrifugation, the supernatant containing the unprecipitated prolactin is tested for total prolactin level. A concentration of 25 % PEG is added to an aliquot of serum specimen and the PEG-treated sample is incubated for a short period and then centrifuged to precipitate out macroprolactin. The supernatant containing the unprecipitated prolactin is tested for recovery of basal prolactin. The PEG-precipitable PRL (%), which represents the amount of macroprolactin, is calculated as follows: (total PRL-free PRL)/total PRL × 100. PEG-precipitation ratio greater than 60 % (recovery less than 40 %) is used as the cut-off value for the diagnosis of macroprolactinemia. Recovery of less than 40 % after PEG is considered a diagnostic criteria for macroprolactin; recovery values around 40–60 % are considered borderline, and values >60 % rule out macroprolactinemia [22–24]. The unprecipitated percentage of basal prolactin is considered as recovery of monomeric prolactin.
Statistical analysis
Statistical analysis was performed using IBM-SPSS software (version 21.0; SPSS Inc., Chicago, IL, USA). Comparisons between groups were performed using ANOVA for normally distributed variables, and the Mann–Whitney and Kruskal-Wallis tests for non-normal variables. All data are expressed as mean ± standard deviation or percentages, while p value <0.05 was considered statistically significant.
Results
Comparison of patients’ demographics and laboratory parameters between the groups are shown in Table 1.
The number of patients in the euthyroid (n = 40), hypothyroid (n = 54) and hyperthyroid (n = 44) groups and age distributions between the groups (mean age was 29.2 ± 5.6 years in group 1, 29.0 ± 5.1 years in group 2 and 29.3 ± 4.9 years in group 3) were similar (p > 0.05). Although it did not reach statistical significance, the mean number of previous pregnancies was higher in hyperthyroid patients (2.7) than hypothyroid (2.4) and euthyroid (2.2) patients. Rates of complicated pregnancy history were high in all groups (n = 12 (30 %) in group 1, n = 18 (33 %) in group 2 and 14 (34 %) in group 3).
Body weight of the patients in group 3 was lower than patients in the other groups (p < 0.005) and the mean weight was 69.9 ± 13.9 kg in group 1, 68.7 ± 14.5 kg in group 2 and 60.7 ± 11.5 kg in group 3. Blood pressure measurements were not different between the groups. Mean TSH level was 1.04 ± 0.7 μIU/L in group 1, 6.7 ± 10.7 μIU/L in group 2, and 0.02 ± 0.02 μIU/L in group 3. Mean FT4 was 1.13 ± 0.21 ng/dL in group 1, 1.17 ± 0.54 ng/dL in group 2, and 1.7 ± 0.80 ng/dL in group 3. Mean FT3 pg/mL was 2.93 ± 0.331 pg/mL in group 1, 2.78 ± 0.531 pg/mL in group 2, and 4.84 ± 2.04 pg/mL in group 3. As expected, there were significant differences in serum TSH, FT4, and FT3 levels between the groups (p < 0.001). There were significant differences also in terms of thyroid antibodies between the groups (p < 0.001). TPOAb was 189.9 ± 352.6 U/mL in group 1, 563.8 ± 576.5 U/mL in group 2, and 158.8 ± 308.8 U/mL in group 3. TGAb was 71.1 ± 111.51 U/mL in group 1, 164.7 ± 159.0 U/mL in group 2, and 123.7 ± 311.2 U/mL in group 3. Group 2 had significantly higher TPOAb and TGAb levels compared to group 1 and 3 (p < 0.01 and <0.05 respectively). Macroprolactinemia was detected in two patients. One patient was from group 1 and the other patient was from group 2. Basal PRL levels of these patients were 400 and 403 ng/mL respectively. Basal serum PRL levels and percentage of monoPRL recovery after PEG precipitation were similar when the three groups were compared. Percentages of monoPRL recovery after PEG treatment were not different between the groups; 90.6 ± 8.7 % in group 1, 91.5 ± 9.2 % in group 2, and 88.9 ± 10.9 % in group 3.
Correlation analyses of prolactin and monoPRL % with patients’ characteristics and laboratory parameters are summarized in Table 2.
There was a positive correlation (p < 0.001, r =0.532) between PRL with gestational week and a negative correlation (p < 0.05, r = −0.296) with number of pregnancies. Serum prolactin levels were also found positively correlated with serum TSH (p = 0.014 and r = 0.219) and negatively correlated with FT4 (p = 0.011 and r = −0.227). Because of the insufficient number of macroprolactin positive patients, correlation analyses were done between the percentages of monoPRL recovery instead of macroprolactinemia. However, no statistically significant correlation was found between monoPRL % and thyroid hormone levels. Also, there was no correlation between the serum levels of thyroid antibodies with PRL and monoPRL % (p > 0.05). There was a slightly significant negative correlation between PRL and monoPRL % (p = 0.043 and r = −0.181).
The comparisons of data obtained from patients who were divided into two groups according to the presence of TPOAb antibody are also seen in Table 3.
Patients with positive TPOAb had higher serum TSH levels (3.97 ± 9.3 vs. 1.35 ± 0.62 μIU/L) and lower serum FT4 levels (1.28 ± 0.65 vs. 1.46 + 0.62 ng/dL) compared to patients with negative TPOAb and the differences between the groups were significant for both parameters (p = 0.003 and 0.018 respectively). But serum FT3 levels of the groups were similar. In addition, neither prolactin nor monoPRL % levels were different between the patients with positive and negative TPOAb (p > 0.05).
Comparisons of PRL, monoPRL %, and thyroid parameters between patients with and without a history of complicated pregnancy are shown in Table 4.
In terms of history of complicated pregnancy, there was a slightly significant difference for PRL levels between the groups. Patients without a history of complicated pregnancy had higher prolactin levels than the patients with a history of complicated pregnancy (66.64 ± 65.9 vs. 49.12 ± 66.0 ng/ml; p = 0.026). There were also significant differences in terms of thyroid autoantibodies between the two groups. Patients with a history of complicated pregnancy had higher antibody levels. Serum TPOAb and TGAb levels were 344.7 ± 496.9 U/mL and 169.3 ± 329.2 U/mL in patients with complicated pregnancy, whereas they were 207.7 ± 468.8 U/mL and 89.9 ± 134.7 U/mL in patients without complicated pregnancy.
Discussion
Pregnancy and breastfeeding are the most important periods of long-term physiological increase of prolactin levels. Absence of galactorrhea is mostly related with the high levels of estrogen during pregnancy despite hyperprolactinemia [25]. On the other hand, a probable alternative explanation for the absence of galactorrhea may be heterogeneity of prolactin molecules. It is well known that high-molecular weight isoforms of PRL have low binding affinity to PRL receptors. In addition, it was shown that the relative proportion of little PRL increased in pregnant women as pregnancy progressed [1]. In some studies, the presence of big, big PRL has been reported in a range of 8–38 % of total PRL during pregnancy [26, 27]. However, Hattori et al. [28] has found that the frequency of macroprolactinemia was 2.9 % in women during the third trimester of pregnancy (3 of 105). We found the frequency of macroprolactinemia as 1.4 % in women in the first and second trimester. Unlike the other studies [26, 27], our results were similar to the results of Hattori et al. [28]. The small number of patients with macroprolactinemia suggested that the increase of prolactin is quite homogenous during pregnancy. Interestingly, regardless of thyroid status, patients with macroprolactinemia had the highest PRL levels (400 and 403 ng/mL) compared with other patients. Our results were also similar to Pascoe-Lira et al.’s study. They found that 3.8 % of the pregnant women had significant macroprolactinemia and total PRL concentration was observed higher in those patients. Another probable explanation for the discrepancy of published results may be the detection method which is commonly used for macroprolactin measurement. Although the gold standard method for detecting prolactin homogeneity or macroPRL is gel filtration chromatography, precipitation with polyethylene glycol (PEG) is a widely used, inexpensive, and easy screening test [7, 8, 29]. Therefore, if we were using the latter method, results could have been different. In general, however, this method is not widely used, or available everywhere and recommended if borderline measurement was obtained. In other words, gel filtration chromatography would be necessary if 40-60 % of prolactin recovery was detected after PEG precipitation [30]. Almost all of our patients have shown >90 % persistency from initial levels of monomeric prolactin after PEG precipitation despite the clinical and laboratory differences. These data have supported the strong homogeneity for PRL during pregnancy as well.
It has been shown that there is a strong association between thyroid and prolactin secretion physiologically. Many critical and period-specific changes occur during pregnancy in thyroid and prolactin metabolism. Due to the structural similarity, elevated hCG may increase the synthesis of thyroid hormones and cause TSH suppression. Thus PRL response to TRH may be blunted in hyperthyroid conditions. In contrast, elevated TRH can increase levels of TSH and PRL in patients with hypothyroidism [31, 32]. Autoimmune thyroid disorders are common in women of reproductive age and subclinical hypothyroidism related to chronic autoimmune thyroiditis is the most common thyroid disorder. If the classic reference range (0.4–4.0 μIU/L) of TSH is used in the first trimester of pregnancy, subclinical cases of hypothyroidism may be missed. Gestational transient thyrotoxicosis (GTT) or hCG-mediated transient TSH suppression and Graves Disease (GD) are the most common types of hyperthyroid disease in pregnant women. GTT is generally asymptomatic with mild biochemical hyperthyroidism and may be exacerbated by hyperemesis, while GD is a real thyrotoxic disease and mostly requires anti-thyroid treatment. Both hypo and hyperthyroidism were reported to be associated with poor pregnancy outcome. These outcomes include spontaneous abortions, preterm birth, intrauterine growth restriction, stillbirth, preeclampsia, heart failure, and neurodevelopment deficits in the children [10–12].
In the present study, due to the complex relationship between thyroid and prolactin metabolism, we tried to examine patients by dividing them into three groups in terms of thyroid status. The second aim of our study was to evaluate prolactin homogeneity in different thyroid disorders during pregnancy. To the best of our knowledge, the present study is the first study which investigated this relationship. Contrary to our expectations, macroprolactin levels did not increase during pregnancy and there were only two patients with macroprolactinemia. All of the remaining patients showed homogeneity in terms of prolactin size. We preferred to use percentage of monoPRL recovery for the other patients to define homogeneity instead of macroprolactinemia for two reasons. Firstly because of the insufficient number of patients with macroprolactinemia and the secondly due to the fact that the definition of macroprolactinemia is already based on percentage of recovered prolactin after PEG precipitation. Nevertheless, there was a small amount of data that can be considered significant. These findings were as follows, a slightly significant positive correlation between TSH and PRL, and a negative correlation between FT4 and PRL. Although there is a known close relationship between thyroid and prolactin metabolism, it was not so clear in the present study. However, the number of marked hypothyroid and hyperthyroid patients was inconsiderable in our study and most of our patients were euthyroid. This can explain why we found serum prolactin levels similar and not enough to confirm our hypothesis.
The other potential issue is the relationship of prolactin with autoimmune processes. It was shown that prolactin has the potential to stimulate the immune system and can also be produced in extra pituitary sites [33, 34]. A large number of autoantibodies are increased in patients with hyperprolactinemia without overt clinical autoimmune disease. These antibodies include antipituitary, antithyroid peroxidase, antithyroglobulin, anti gastric parietal cells, antimicrosomal, and anticardiolipin antibodies [35–38]. In addition, there is an intriguing relationship between macroprolactin and some collagen tissue disorders such as SLE. It is proposed that there is a correlation between disease activity and macroprolactinemia [39, 40]. Initially we investigated this relationship in different thyroid hormone status. We could not find any relationship between thyroid antibodies with either PRL or monoPRL %. Regardless of thyroid status, according to the presence of TPOAb alone, the negative tendency continued. It is well known that antibodies may be high in healthy individuals without apparent thyroid disease [41, 42]. Presence of high number of patients with positive thyroid antibody, 81(58 %) in all groups, can be a reason for statistical uncertainty.
Conclusions
In conclusion; there were no significant contributions of macroprolactin to prolactin levels during pregnancy. The levels of prolactin showed strong homogeneity and no correlation were found with thyroid dysfunction and thyroid autoimmunity at that time. This uncertainty persisted when correlation analyses was done with monoPRL % instead of macroPRL. Ultimately, we could not find any relationship between thyroid hormones and antibodies with prolactin types in terms of molecular size.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
The study protocol was approved by Sevket Yilmaz Research and Education Hospital Ethics Committee. (Number and date: 2014/0501-07.03.2014).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Abbreviations
- DBP:
-
Diastolic blood pressure
- FT3:
-
Free triiodotronin
- FT4:
-
Free tetraiodotronin
- macroPRL:
-
Macroprolactin
- monoPRL %:
-
the percentage of monomeric prolactin recovery after PEG precipitation
- PRL:
-
Prolactin
- PEG:
-
Polyethylene glycol
- SBP:
-
Systolic blood pressure
- TGAb:
-
Thyroglobulin antibody
- TPOAb:
-
Thyroid peroxidase antibody
- TSH:
-
Thyroid stimulating hormone
References
Freeman ME, Kanyicska B, Lerant A, Nagy G. Prolactin: structure, function, and regulation of secretion. Physiol Rev. 2000;80:1523–631.
Molitch ME. Prolactin in Human Reproduction. In: Jerome F Strauss III, Robert Barbieri, editors. Yen & Jaffe’s reproductive endocrinology: physiology. athophysiology and clinical management. 7th Edition. Chapter 3. Philadelphia, USA; 2013. p. 45–65.e11.
Shiu RPC, Friesen HG. Mechanism of action of prolactin in the control of mammary gland function. Annu Rev Physiol. 1980;42:83–96.
Pansini F, Bergamini CM, Malfaccini M, Cocilovo G, Linciano M, Jacobs M, et al. Multiple molecular forms of prolactin during pregnancy in women. J Endocrinol. 1985;106:81–5.
Glezer A, Soares CR, Vieira JG, et al. Human macroprolactin displays low biological activity via its homologous receptor in a new sensitive bioassay. J Clin Endocrinol Metab. 2006;91:1048–55.
Chawla R et al. Detection of macroprolactinemia and molecular characterization of prolactin isoforms in blood samples of hyperprolactinemic women. J Med Biochem. 2012;31(1):19–26.
Bell DA, Hoad K, Leong L, et al. A high pressure liquid chromatography method for separation of prolactin forms. Ann Clin Biochem. 2012;49:285–8.
Beltran L, Fahie-Wilson MN, McKenna TJ, et al. Serum total prolactin and monomeric prolactin reference intervals determined by precipitation with polyethylene glycol: evaluation and validation on common immunoassay platforms. Clin Chem. 2008;54:1673–81.
Fahie-Wilson M, Smith TP. Determination of prolactin: the macroprolactin problem. Best Pract Res Clin Endocrinol Metab. 2013;27(5):725–42. doi:10.1016/j.beem.2013.07.002.
Glinoer D. The regulation of thyroid function in pregnancy: pathways of endocrine adaptation from physiology to pathology. Endocr Rev. 1997;18:404–33. doi:10.1210/er.18.3.404.
Chen L, Hu R. Thyroid autoimmunity and miscarriage: a meta analysis. Clin Endocrinol (Oxf). 2011;74:513–9. doi:10.1111/ j.1365-2265.2010.03974.x.
Männistö T, Mendola P, Reddy U, Laughon SK. Thyroid disease and adverse pregnancy outcomes in a contemporary US cohort. J Clin Endocrinol Metab. 2013;98:2725e33.
Stagnaro-Green A, Abalovich M, Alexander E, Azizi F, Mestman J, Negro R, et al. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. 2011;21:1081–125. doi:10.1089/thy.2011.0087.
De Groot L, Abalovich M, Alexander EK, Amino N, Barbour L, Cobin RH, et al. Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012;97:2543–65. doi:10.1210/jc.2011-2803.
Chang DL, Pearce EN. Screening for maternal thyroid dysfunction in pregnancy: a review of the clinical evidence and current guidelines. J Thyroid Res. 2013;2013:851326.
Turankar S, Sonone K, Turankar A. Prolactin and thyroid levels in primary infertility. J Clin Diagn Res. 2013;7(5):794–6.
Binita G, Suprava P, Mainak C, Koner BC, Alpana S. Correlation of prolactin and thyroid hormone concentration with menstrual patterns in infertile women. J Reprod Infertil. 2009;10(3):207–12.
Jara LJ et al. Prolactin and autoimmunity. Clin Rev Allergy Immunol. 2011;40(1):50–9.
Hedi O et al. Prolactin and autoimmunity. Clin Rev Allergy Immunol. 2012;42(2):189–98.
Mario G-C et al. Thyroid disorders, hyperprolactinemia and systemic lupus erythematosus activity. Int J Clin Rheumatol. 2014;9(5):441–7.
Onal ED, Saglam F, Sacikara M, Ersoy R, Cakir B. Thyroid autoimmunity in patients with hyperprolactinemia: an observational study. Arq Bras Endocrinol Metabol. 2014;58(1):48–52.
Kasum M, Oreskovic S, Zec I, Jezek D, Tomic V, Gall V, et al. Macroprolactinemia: new insights in hyperprolactinemia. Biochemiamedica. 2012;22(2):171–9.
Kasum M, Pavičić-Baldani D, Stanić P, Orešković S, Sarić JM, Blajić J, et al. Importance of macroprolactinemia in hyperprolactinemia. Eur J Obstet Gynecol Reprod Biol. 2014;183:28–32.
Hattori N, Ikekubo K, Nakaya Y, et al. Immunoglobulin G subclasses and prolactin (PRL) isoforms in macroprolactinemia due to anti-PRL autoantibodies. J Clin Endocrinol Metabol. 2005;90:3036–44.
Ignacak A et al. Prolactin–not only lactotrophin. A “new” view of the “old” hormone. J Physiol Pharmacol. 2012;63(5):435–43.
Pascoe-Lira D, Duran-Reyes G, Contreras-Hernández I, Manuel-Apolinar L, Blanco-Favela F, Leaños-Miranda A. Frequency of macroprolactinemia due to autoantibodies against prolactin in pregnant women. J Clin Endocrinol Metab. 2001;86:924–9.
Jackson RD, Wortsman J, Malarkey WB. Persistence of large molecular weight prolactin secretion during pregnancy in women with macroprolactinemia and its presence in fetal cord blood. J Clin Endocrinol Metab. 1989;68:1046–50.
Hattori N. The frequency of macroprolactinemia in pregnant women and the heterogeneity of its etiologies. J Clin Endocrinol Metab. 1996;81:586–90.
Shimatsu A, Hattori N. Macroprolactinemia: diagnostic, clinical, and pathogenic significance. Clin Dev Immunol. 2012;2012:167132.
Leslie H, Courtney CH, Bell PM, Hadden DR, McCance DR, Ellis PK, et al. Laboratory and clinical experience in 55 patients with macroprolactinemia identified by a simple poly ethylene glycol precipitation method. J Clin Endocrinol Metab. 2001;86(6):2743–6.
Ferrari C, Boghen M, Paracchi A, et al. Thyroid autoimmunity in hyperprolactinemic disorders. Acta Endocrinol. 1983;104:35–41.
Hermite ML, Robyn C, Golstein J, et al. Prolactin and thyrotropin in thyroid diseases: lack of evidence for a physiological role of thyrotropin-releasing hormone in the regulation of prolactin secretion. Horm Metab Res. 1974;16:190–5.
Ben-Jonathan N, Mershon JL, Allen DL, Steimetz RM. Extra pituitary prolactin: distribution, regulation, functions, and clinical aspects. Endocr Rev. 1996;17:639–69.
Shahar S, Boaz M, Orbach H. Prolactin and autoimmunity. Autoimmun Rev. 2012;11(6):A465–70.
Costanza M, Binart N, Steinman L, Pedotti R. Prolactin: a versatile regulator of inflammation and autoimmune pathology. Autoimmun Rev. 2014;14(3):223–30.
Kavanagh-Wright L, Smith TP, Gibney J, et al. Characterization of macroprolactin and assessment of markers of autoimmunity in macroprolactinaemic patients. Clin Endocrinol (Oxf). 2009;70:599–605.
Ishibashi M, Kuzuya N, Sawada S, Kitamura K, Kamoi K, Yamazi T. Anti-thyroid antibodies in patients with hyperprolactinemia. Endocrinol Jpn. 1991;38:517–22.
Vera-Lastra O, Jara LJ, Espinoza LR. Prolactin and autoimmunity. Autoimmun Rev. 2002;1:360–4.
Leanos-Miranda A, Pascoe-Lira D, Chavez-Rueda KA, et al. Antiprolactin autoantibodies in systemic lupus erythematosus: frequency and correlation with prolactinemia and disease activity. J Rheumatol. 2001;28:1546–53.
Kramer CK, Tourinho TF, de Castro WP, Oliveria MD. Association between systemic lupus erythematosus, rheumatoid arthritis, hyperprolactinemia, and thyroid autoantibodies. Arch Med Res. 2005;36:54–8.
Liu H, Shan Z, Li C, Mao J, Xie X, Wang W, et al. Maternal subclinical hypothyroidism. Thyroid autoimmunity and the risk of miscarriage: a prospective cohort study. Thyroid. 2014;24(11):1642–9.
Krassas GE, Poppe K, Glinoer D. Thyroid function and human reproductive health. Endocr Rev. 2010;31(5):702–55.
Acknowledgements
We thank Fatma Kara who provided acquisition of data.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector. Routine examinations are taken from the patient's file, while macroprolactin measurement fee was covered by the corresponding author.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no conflict of interest. No payment has been made to any of authors due to all researchers working in the same hospital and collaborated voluntary.
Authors’ contributions
MG designed the study and wrote the manuscript. SC contributed to patient selection and performed the statistical analysis. SK participated in its design and helped to draft the manuscript. EV carried out the laboratory studies. ABH and GK participated in coordination of study and contributed to patient selection. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Guclu, M., Cander, S., Kiyici, S. et al. Serum macroprolactin levels in pregnancy and association with thyroid autoimmunity. BMC Endocr Disord 15, 31 (2015). https://doi.org/10.1186/s12902-015-0025-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-015-0025-2