
Abstract
Purpose
The atherogenic index of plasma (AIP) is a novel comprehensive lipid index. We aimed to investigate a possible relationship between AIP index and kidney stones in US adults.
Methods
This cross-sectional study was conducted among adults with complete AIP index and questionnaire records on kidney stones from the National Health and Nutrition Examination Survey (NHANES) spanning from 2007 to 2018. The AIP index served as the exposure variable, defined as the logarithm of the ratio between triglycerides (TG, mmol/L) and high-density lipoprotein cholesterol (HDL-c, mmol/L). Self-reported history of kidney stones was utilized as the outcome variable. The independent relationship between AIP index and the risk of kidney stones was fully assessed.
Results
A total of 14,833 participants were included in this study, with an average AIP index of -0.07 ± 0.01. The proportion of kidney stones progressively increased with higher AIP index tertile intervals (7.33% vs. 9.97% vs. 12.57%, P < 0.001). Furthermore, AIP index was found to be independently associated with the risk of kidney stones after adjusting for confounding factors (OR = 1.32, 95% CI 1.08–1.61, P = 0.006). Restricted cubic spline (RCS) analysis confirmed the robustness of our results. There was no significant interaction observed based on subgroup analysis stratified by age, gender, race, body mass index (BMI, kg/m2), smokers, diabetes, hypertension, and cardiovascular disease (P for interaction > 0.05).
Conclusions
The AIP index may be a potential epidemiological tool to quantify the role of dyslipidemia in the risk of kidney stones in US adults.
Similar content being viewed by others


Introduction
Kidney stones is a prevalent urological disorder formed by the accumulation of inorganic substances (such as crystalline salts) and organic components (such as urinary macromolecules) within the renal parenchyma or pelvicalyceal system [1]. The prevalence and incidence of kidney stones have significantly risen in recent decades, with global estimates ranging from 2 to 20% [2,3,4,5]. Common symptoms of kidney stones include lower back pain, hematuria, frequent urination, urgency to urinate, and dysuria. Kidney stones can cause serious complications such as ureteral blockage, urinary tract infections, and ultimately, end-stage renal failure [6]. Surgical intervention is often required for the treatment of kidney stones, imposing significant financial burdens, and escalating public health concerns [1, 7].
Emerging research suggests that dyslipidemia plays a crucial role in the development of kidney stones, independent of other components of metabolic syndrome such as diabetes and obesity [8,9,10]. Specific alterations in lipid profiles may serve as potential indicators of unique abnormalities in urine physicochemical properties and the risk of stone formation. The AIP index is a newer and more effective lipid marker, introduced by Dobiásová and Frohlich in 2001 [11]. It is calculated as the logarithmic transformation of TG to HDL-c ratio [11]. Unlike TG or HDL-C levels alone, the AIP index combines both TG and HDL-C levels, providing a comprehensive reflection of the ratio as well as the size of lipoprotein particles, making it a more accurate indicator of dyslipidemia pathogenicity and specificity [12, 13]. Previous studies have demonstrated a strong association between AIP index and various diseases, including cardiovascular diseases, diabetes, metabolic syndrome, and non-alcoholic fatty liver disease [14,15,16,17].
However, to our knowledge, there have been no studies exploring the relationship between AIP index and kidney stones. This cross-sectional study utilized data from the NHANES database to investigate the relationship between the AIP index and the risk of kidney stones.
Materials and methods
Data source
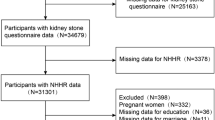
This population-based study utilized data from the NHANES, conducted by the National Center for Health Statistics of the Centers for Disease Control and Prevention [18, 19]. NHANES employed a randomized, stratified, multi-stage survey with nationwide representation. Participants underwent physical examinations, health and nutrition questionnaires, and laboratory assessments. The NHANES study protocol was approved by the Ethics Review Board of the National Center for Health Statistics, and detailed design can be accessed at https://www.cdc.gov/nchs/nhanes/. The current study finally consisted of 14,833 eligible participants, obtained by merging data from the NHANES cycles: 2007–2008, 2009–2010, 2011–2012, 2013–2014, 2015–2016, and 2017–2018 (59,842 participants). All participants were aged 20 years or older, not pregnant, had complete data of AIP index, and provided comprehensive questionnaire records on kidney stones.
Exposure and outcome definitions
The AIP index, as an exposure variable, is defined as the logarithm base 10 of the ratio between TG and HDL-c, both measured in mmol/L [20]. The history of kidney stones, which served as the outcome variable, was assessed by posing the question, “Have you or the sample person (SP) ever had a kidney stone?” (ID: KIQ026). Participants who responded “yes” were classified as individuals with kidney stones, whereas those who responded “no” were categorized as individuals without kidney stones. The reliability of self-reported kidney stone history has been established in previous studies [4, 5, 21,22,23,24].
Covariate definitions
Demographic data (age, gender, and race) was obtained. It also included various potential covariates such as annual household income, educational level, physical activity, smokers, diabetes, hypertension, cardiovascular disease, BMI, alanine transaminase (ALT, U/L), aspartate transaminase (AST, U/L), gamma-glutamyl transferase (GGT, U/L), glycohemoglobin, fasting plasma glucose (FPG, mmol/L), total cholesterol (TC, mmol/L), low-density lipoprotein cholesterol (LDL-c, mmol/L), serum creatinine (Scr, μmol/L), serum uric acid (SUA, μmol/L), and the estimated glomerular filtration rate (eGFR, ml/min/1.73 m2). BMI was classified into three categories: < 25, 25–29.9, and ≥ 30 kg/m2, representing normal weight, overweight, and obesity. The eGFR was calculated using the CKD-EPI creatinine equation, considering factors such as age, gender, race, and Scr [25]. Smokers were identified as current and former smokers. Self-reported diabetes and hypertension were also defined, and the presence of cardiovascular disease was determined based on self-reported history of heart attack, stroke, congestive heart failure, coronary artery disease, or angina. Detailed measurement procedures for all variables in this study were publicly available in the NHANES database.
Statistical analysis
All statistical analyses followed Centers for Disease Control and Prevention guidelines, incorporating a complex multistage cluster survey design, and combining fasting subsample weights from six cycles. Continuous variables were reported as mean with standard error (SE), and categorical variables as percentage. Weighted Student’s t-test and chi-squared test were used to compare continuous and categorical variables among multiple groups. Weighted Pearson correlation analysis assessed the association of AIP index with other covariates. Weighted logistic regression models were employed to investigate the associations between TG, HDL-c, TG/HDL, and AIP index and the risk of kidney stones. Three Models were used: Model 1 without covariates adjusted, Model 2 with adjustments for age, gender, and race, and Model 3 with adjustments for multiple covariates including age, gender, race, annual household income, education level, physical activity, smokers, diabetes, hypertension, cardiovascular disease, BMI, ALT, AST, GGT, glycohemoglobin, FPG, TC, LDL, Scr, SUA, and eGFR. RCS analysis was used to further elucidate the correlation between AIP index and the risk of kidney stones. Subgroup analyses were performed based on age (< 60/ ≥ 60 years), gender (female/male), race (white/no white), smokers (ye/no), BMI (normal weight/overweight/obesity), diabetes (yes/no), hypertension (yes/no), and cardiovascular disease (yes/no). The Empower software (http://www.empowerstats.com) and R software (http://www.R-project.org) were used for all statistical analyses. A P value < 0.05 was considered statistically significant.
Results
Baseline characteristics of study population
The study finally included 14,833 participants who met the inclusion criteria. Among the entire participant cohort, a total of 1,421 individuals were found to have kidney stones. The average age of the participants was 47.59 ± 0.25 years, and 48.76% of them were male. General characteristics and clinical indicators were compared between the non-kidney stone and kidney stone groups (Table 1). The kidney stone group had higher values in terms of age, male, smokers, diabetes, hypertension, cardiovascular disease, obesity, glycohemoglobin, FPG, TG, Scr, and SUA compared to the non-kidney stone group (P < 0.05). However, the kidney stone group exhibited significant decreases in moderate physical activity, HDL-c, and eGFR (P < 0.05). Significant differences in race distribution were also observed between the groups (P < 0.001). Importantly, the kidney stone group had higher AIP levels than the non-kidney stone group (P < 0.001).
Clinical features of the participants according to the tertiles of AIP index
Participants were divided into three groups based on their AIP index levels: tertile I, tertile II, and tertile III (Table 2). Compared to the tertile I-AIP group, the tertile II-AIP, and tertile III-AIP groups showed significant increases in age, male, annual household income under $20,000, smokers, prevalence of diabetes, hypertension, cardiovascular disease, obesity, ALT, AST, GGT, glycohemoglobin, FPG, TG, TC, LDL-c, Scr, and SUA (P < 0.001). Education level above high school and HDL-c exhibited significant decreases (P < 0.001). Significant differences in race were also observed among the tertile groups (P < 0.001). No differences in moderate physical activity were observed between groups. Importantly, as AIP levels increased, the prevalence of kidney stones showed a gradual increase (7.33% vs. 9.97% vs. 12.57%, P < 0.001).
Correlation of AIP index with clinical parameters
Weighted Pearson correlation analysis revealed significant correlations between the AIP index and various variables (Table 3). Specifically, the AIP index was positively correlated with age, male, race, annual household income under $20,000, smokers, prevalence of diabetes, hypertension, cardiovascular disease, BMI, ALT, AST, GGT, glycohemoglobin, FPG, TG, TC, LDL-c, Scr, and SUA, and kidney stones. On the other hand, the AIP index was negatively correlated with education level above high school, HDL-c, and eGFR. After adjusting for age, gender, and race, except for moderate physical activity, AST, and Scr, the AIP index remained significantly correlated with the other variables.
Associations between the AIP and kidney stones
Table 4 presents the association between the AIP index and the risk of kidney stones. The unadjusted models showed that TG, TG/HDL-c, and AIP index were positively associated with an increased risk of kidney stones (P < 0.001), while HDL-c was negatively associated with the prevalence of kidney stones (P < 0.001). After adjusting for age, gender, and race, these associations remained statistically significant (P < 0.05). Further adjustment for multiple covariates revealed that only HDL-c and AIP index were related to the risk of kidney stones. The results indicated a 32% increased risk of kidney stones per unit increase in AIP index (OR = 1.32, 95% CI 1.08–1.61, P = 0.006). Classification of AIP index into teritles showed that higher AIP teritles levels were associated with a higher prevalence of kidney stones compared to the lowest teritles in the fully adjusted model (P for trend < 0.001). Furthermore, the results of RCS analysis also confirmed a positive correlation between AIP index and kidney stones (Fig. 1), with no significant threshold effect observed (P for nonlinear > 0.05).

RCS results of AIP index and the risk of kidney stones (a no covariates adjusted; b adjusted for age, gender, race, annual household income, education level, physical activity, smokers, diabetes, hypertension, cardiovascular disease, BMI, ALT, AST, GGT, glycohemoglobin, FPG, TC, LDL, Scr, SUA, and eGFR)
Subgroup analyses
Subgroup analyses were performed to investigate the relationship between AIP index and the risk of kidney stones in various population. Subgroups were stratified by various factors, including age (< 60/ ≥ 60 years), gender (female/male), race (white/no white), smokers (yes/no), BMI (normal weight/overweight/obesity), diabetes (yes/no), hypertension (yes/no), and cardiovascular disease (yes/no). Figure 2 illustrates the results of these analyses, which revealed no significant interactions among the subgroups (P for interaction > 0.05). However, there is a trend towards a stronger association between AIP index and kidney stones in individuals with diabetes.

Subgroup analysis results based on age, gender, race, smokers, BMI, diabetes, hypertension, and cardiovascular disease
Discussion
To our knowledge, this is the first population-based study to explore the relationship between AIP index and the risk of kidney stones. Our research indicated that AIP index is associated with the risk of kidney stones in the US population (OR = 1.32, 95% CI 1.08–1.61, P = 0.006). Compared to simple TG, HDL-c, and TG/HDL-c, the AIP index is a promising epidemiological tool that can quantify the role of dyslipidemia in the risk of kidney stones.
Previous studies have shown that serum lipid profiles also affect urinary metabolite profiles and stone composition. Patients with low HDL-c or high TG exhibit significantly increased levels of urinary sodium, oxalate, and uric acid, as well as lower pH values [8, 26]. Additionally, lipid-lowering medications, such as atorvastatin, have been shown to significantly alter urinary citrate, uric acid, and urinary pH levels [27]. Masterson et al. propose that metabolic syndrome may partially explain the impact of dyslipidemia on the formation of kidney stones, as dyslipidemia is one of the diagnostic criteria for metabolic syndrome [28, 29]. Dyslipidemia is also closely associated with insulin resistance. Additionally, elevated levels of AIP index have been suggested as indicative of insulin resistance [30]. Insulin resistance can impair ammonia excretion and increase renal tubular uptake of citrate, contributing to high urinary acidity and reduced citrate levels, respectively, which are major risk factors for uric acid and calcium stone formation [31]. Moreover, evidence suggests that dyslipidemia, which mediates inflammation, is an independent risk factor for increased stone formation [21, 32, 33]. Some scholars also suggest that the accumulation of atherosclerotic plaques may lead to calcification, subsequently eroding into the Bellini collecting ducts, further increasing the likelihood of stone growth [34]. It is evident that dyslipidemia can have a multifactorial impact on the formation of kidney stones.
In this study, we observed a correlation between high TG levels, low HDL-c levels, TG/HDL-c, and AIP index with the formation of kidney stones. However, it is worth noting that, after adjusting for various confounding factors, only HDL-c and AIP index maintained this correlation. Previous studies have shown that AIP index, the logarithmic ratio of TG to HDL-C, not only quantifies lipid metabolism, but also shows significant associations with small dense low-density lipoprotein-cholesterol (sdLDL-C) and glucose metabolism [35, 36]. Other studies have also demonstrated that AIP index is a simple and useful tool for identifying insulin-resistant patients at higher cardiovascular risk, proving more effective than the conventional visceral adiposity index [36, 37]. Therefore, consistent with previous research findings, we also believe that the AIP index, as a novel comprehensive lipid indicator, may have clinical significance that surpasses the impact of individual TG and HDL-c levels and the simple ratio of the two on kidney stone formation [38, 39]. The AIP index is anticipated to serve as a quantifiable marker that connects metabolic syndrome and obesity to the risk of kidney stones. Moreover, the comparative efficacy of the AIP index versus other metabolic indicators, such as the triglyceride-glucose index (TyG), requires further investigation.
This study used a nationally representative sample that adequately represented the various ethnic groups in US adults [24]. However, it is important to recognize the limitations of our study. Firstly, the cross-sectional design used does not allow us to establish a cause-and-effect relationship between the AIP index and the risk of kidney stones. Prospective cohort studies and intervention trials are needed to determine if such a relationship exists. Secondly, although adjustments were made for some common confounding factors in this study, it did not consider the history of diseases like metabolic syndrome and non-alcoholic fatty liver disease, the use of medications such as lipid-lowering drugs that affect lipid levels, or dietary habits including water and meat consumption, which could lead to biased findings. Thirdly, given that our research is an exploratory preliminary analysis of existing data, we were unable to gather detailed information on kidney stones, such as their quantity and composition, which limited further analysis. Lastly, our study was conducted using a sample from the US population, so further research is needed to confirm the generalizability of our findings.
Conclusion
In a nationally representative study of an adult population in the United States, we uncovered a compelling correlation between the AIP index and a heightened susceptibility to kidney stones.
Availability of data and materials
Data was collected from the NHANES database, which is a publicly accessible and free resource (https://www.cdc.gov/nchs/nhanes/).
References
Peerapen P, Thongboonkerd V. Kidney stone prevention. Adv Nutr. 2023;14(3):555–69. https://doi.org/10.1016/j.advnut.2023.03.002.
Liu H, Ma Y, Shi L. Higher weight-adjusted waist index is associated with increased likelihood of kidney stones. Front Endocrinol (Lausanne). 2023;14:1234440. https://doi.org/10.3389/fendo.2023.1234440.
Thongprayoon C, Krambeck AE, Rule AD. Determining the true burden of kidney stone disease. Nat Rev Nephrol. 2020;16(12):736–46. https://doi.org/10.1038/s41581-020-0320-7.
Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1):160–5. https://doi.org/10.1016/j.eururo.2012.03.052.
Abufaraj M, Xu T, Cao C, Waldhoer T, Seitz C, D’Andrea D, Siyam A, Tarawneh R, Fajkovic H, Schernhammer E, Yang L, Shariat SF. Prevalence and trends in kidney stone among adults in the USA: Analyses of National Health and Nutrition Examination Survey 2007–2018 data. Eur Urol Focus. 2021;7(6):1468–75. https://doi.org/10.1016/j.euf.2020.08.011.
Rule AD, Lieske JC, Pais VM Jr. Management of kidney stones in 2020. JAMA. 2020;323(19):1961–2. https://doi.org/10.1001/jama.2020.0662.
Parmar MS. Kidney stones. BMJ. 2004;328(7453):1420–4. https://doi.org/10.1136/bmj.328.7453.1420.
Torricelli FC, De SK, Gebreselassie S, Li I, Sarkissian C, Monga M. Dyslipidemia and kidney stone risk. J Urol. 2014;191(3):667–72. https://doi.org/10.1016/j.juro.2013.09.022.
Gao M, Liu M, Zhu Z, Chen H. The association of dyslipidemia with kidney stone: result from the NHANES 2007–2020. Int Urol Nephrol. 2023. https://doi.org/10.1007/s11255-023-03784-x.
Hung JA, Li CH, Geng JH, Wu DW, Chen SC. Dyslipidemia increases the risk of incident kidney stone disease in a large Taiwanese population follow-up study. Nutrients. 2022;14(7):1339. https://doi.org/10.3390/nu14071339.
Dobiásová M, Frohlich J. The plasma parameter log (TG/HDL-C) as an atherogenic index: correlation with lipoprotein particle size and esterification rate in apoB-lipoprotein-depleted plasma (FER(HDL)). Clin Biochem. 2001;34(7):583–8. https://doi.org/10.1016/s0009-9120(01)00263-6.
Fernández-Macías JC, Ochoa-Martínez AC, Varela-Silva JA, Pérez-Maldonado IN. Atherogenic index of plasma: novel predictive biomarker for cardiovascular illnesses. Arch Med Res. 2019;50(5):285–94. https://doi.org/10.1016/j.arcmed.2019.08.009.
Yin B, Wu Z, Xia Y, Xiao S, Chen L, Li Y. Non-linear association of atherogenic index of plasma with insulin resistance and type 2 diabetes: a cross-sectional study. Cardiovasc Diabetol. 2023;22(1):157. https://doi.org/10.1186/s12933-023-01886-5.
Li Y, Feng Y, Li S, Ma Y, Lin J, Wan J, Zhao M. The atherogenic index of plasma (AIP) is a predictor for the severity of coronary artery disease. Front Cardiovasc Med. 2023;10:1140215. https://doi.org/10.3389/fcvm.2023.1140215.
Shi Y, Wen M. Sex-specific differences in the effect of the atherogenic index of plasma on prediabetes and diabetes in the NHANES 2011–2018 population. Cardiovasc Diabetol. 2023;22(1):19. https://doi.org/10.1186/s12933-023-01740-8.
Zhang X, Zhang X, Li X, Feng J, Chen X. Association of metabolic syndrome with atherogenic index of plasma in an urban Chinese population: a 15-year prospective study. Nutr Metab Cardiovasc Dis. 2019;29(11):1214–9. https://doi.org/10.1016/j.numecd.2019.07.006.
Liu J, Zhou L, An Y, Wang Y, Wang G. The atherogenic index of plasma: a novel factor more closely related to non-alcoholic fatty liver disease than other lipid parameters in adults. Front Nutr. 2022;9:954219. https://doi.org/10.3389/fnut.2022.954219.
Fain JA. NHANES. Diabetes Educ. 2017;43(2):151. https://doi.org/10.1177/0145721717698651.
Akinbami LJ, Chen TC, Davy O, Ogden CL, Fink S, Clark J, Riddles MK, Mohadjer LK. National health and nutrition examination survey, 2017-March 2020 prepandemic file: sample design, estimation, and analytic guidelines. Vital Health Stat. 2022;1(190):1–36.
Onat A, Can G, Kaya H, Hergenç G. “Atherogenic index of plasma” (log10 triglyceride/high-density lipoprotein-cholesterol) predicts high blood pressure, diabetes, and vascular events. J Clin Lipidol. 2010;4(2):89–98. https://doi.org/10.1016/j.jacl.2010.02.005.
Di X, Liu S, Xiang L, Jin X. Association between the systemic immune-inflammation index and kidney stone: a cross-sectional study of NHANES 2007–2018. Front Immunol. 2023;14:1116224. https://doi.org/10.3389/fimmu.2023.1116224.
Wang M, Jian Z, Ma Y, Jin X, Li H, Wang K. Depression increases the risk of kidney stone: results from the National Health and Nutrition Examination Survey 2007–2018 and Mendelian randomization analysis. J Affect Disord. 2022;312:17–21. https://doi.org/10.1016/j.jad.2022.06.008.
Di XP, Gao XS, Xiang LY, Wei X. The association of dietary intake of riboflavin and thiamine with kidney stone: a cross-sectional survey of NHANES 2007–2018. BMC Public Health. 2023;23(1):964. https://doi.org/10.1186/s12889-023-15817-2.
Hill AJ, Basourakos SP, Lewicki P, Wu X, Arenas-Gallo C, Chuang D, Bodner D, Jaeger I, Nevo A, Zell M, Markt SC, Eisner BH, Shoag JE. Incidence of kidney stones in the United States: the continuous national health and nutrition examination survey. J Urol. 2022;207(4):851–6. https://doi.org/10.1097/ju.0000000000002331.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12. https://doi.org/10.7326/0003-4819-150-9-200905050-00006.
Kang HW, Seo SP, Kim WT, Kim YJ, Yun SJ, Lee SC, Kim WJ. Hypertriglyceridemia is associated with increased risk for stone recurrence in patients with urolithiasis. Urology. 2014;84(4):766–71. https://doi.org/10.1016/j.urology.2014.06.013.
Liu CJ, Huang HS. Statins significantly alter urinary stone-related urine biochemistry in calcium kidney stone patients with dyslipidemia. Int J Urol. 2020;27(10):839–44. https://doi.org/10.1111/iju.14312.
Masterson JH, Woo JR, Chang DC, Chi T, L’Esperance JO, Stoller ML, Sur RL. Dyslipidemia is associated with an increased risk of nephrolithiasis. Urolithiasis. 2015;43(1):49–53. https://doi.org/10.1007/s00240-014-0719-3.
Besiroglu H, Otunctemur A, Ozbek E. The metabolic syndrome and urolithiasis: a systematic review and meta-analysis. Ren Fail. 2015;37(1):1–6. https://doi.org/10.3109/0886022x.2014.976133.
Ismaiel A, Ciobanu OS, Ismaiel M, Leucuta DC, Popa SL, David L, Ensar D, Al Srouji N, Dumitrascu DL. Atherogenic index of plasma in non-alcoholic fatty liver disease: systematic review and meta-analysis. Biomedicines. 2022;10(9):2101. https://doi.org/10.3390/biomedicines10092101.
Spatola L, Ferraro PM, Gambaro G, Badalamenti S, Dauriz M. Metabolic syndrome and uric acid nephrolithiasis: insulin resistance in focus. Metabolism. 2018;83:225–33. https://doi.org/10.1016/j.metabol.2018.02.008.
Dai Y, Quan J, Xiong L, Luo Y, Yi B. Probiotics improve renal function, glucose, lipids, inflammation and oxidative stress in diabetic kidney disease: a systematic review and meta-analysis. Ren Fail. 2022;44(1):862–80. https://doi.org/10.1080/0886022x.2022.2079522.
Welty FK. How do elevated triglycerides and low HDL-cholesterol affect inflammation and atherothrombosis? Curr Cardiol Rep. 2013;15(9):400. https://doi.org/10.1007/s11886-013-0400-4.
Stoller ML, Meng MV, Abrahams HM, Kane JP. The primary stone event: a new hypothesis involving a vascular etiology. J Urol. 2004;171(5):1920–4. https://doi.org/10.1097/01.ju.0000120291.90839.49.
Qin Z, Zhou K, Li Y, Cheng W, Wang Z, Wang J, Gao F, Yang L, Xu Y, Wu Y, He H, Zhou Y. The atherogenic index of plasma plays an important role in predicting the prognosis of type 2 diabetic subjects undergoing percutaneous coronary intervention: results from an observational cohort study in China. Cardiovasc Diabetol. 2020;19(1):23. https://doi.org/10.1186/s12933-020-0989-8.
Salazar MR, Carbajal HA, Espeche WG, Aizpurúa M, Maciel PM, Reaven GM. Identification of cardiometabolic risk: visceral adiposity index versus triglyceride/HDL cholesterol ratio. Am J Med. 2014;127(2):152–7. https://doi.org/10.1016/j.amjmed.2013.10.012.
Murguía-Romero M, Jiménez-Flores JR, Sigrist-Flores SC, Espinoza-Camacho MA, Jiménez-Morales M, Piña E, Méndez-Cruz AR, Villalobos-Molina R, Reaven GM. Plasma triglyceride/HDL-cholesterol ratio, insulin resistance, and cardiometabolic risk in young adults. J Lipid Res. 2013;54(10):2795–9. https://doi.org/10.1194/jlr.M040584.
Wu TT, Gao Y, Zheng YY, Ma YT, Xie X. Atherogenic index of plasma (AIP): a novel predictive indicator for the coronary artery disease in postmenopausal women. Lipids Health Dis. 2018;17(1):197. https://doi.org/10.1186/s12944-018-0828-z.
Nogay NH. Assessment of the correlation between the atherogenic index of plasma and cardiometabolic risk factors in children and adolescents: might it be superior to the TG/HDL-C ratio? J Pediatr Endocrinol Metab. 2017;30(9):947–55. https://doi.org/10.1515/jpem-2016-0479.
Acknowledgements
We want to acknowledge all participants of this study and the support provided by the Jiangsu University.
Funding
This study was funded by the Suzhou Science and Technology Planning Project (STL2021006).
Author information
Authors and Affiliations
Contributions
Z.W. and B.L. wrote the main manuscript text. L.Z., F.T., and Y.P. prepared figures and tables. S.Z. reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study involving human participants were reviewed and approved by the Ethics Review Board of the National Center for Health Statistics. The patients/participants provided their written informed consent to participate in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Z., Lu, B., Zhang, L. et al. Association between the atherogenic index of plasma and kidney stones: a nationally representative study. BMC Urol 24, 179 (2024). https://doi.org/10.1186/s12894-024-01567-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12894-024-01567-9