
Abstract
Objective
To evaluate the safety and efficacy of rigid ureteroscopic lithotripsy with a pressure-controlling ureteral access sheath (PC-UAS) for complex steinstrasse.
Methods
Thirty-one consecutive patients (male: 18; female: 13) with steinstrasse were enrolled, six of whom had concurrent kidney stones. The mean cumulative stone size was 2.7 ± 1.3 cm. The patients were treated with rigid ureteroscopic lithotripsy using a PC-UAS. The cavity pressure parameters were set as follows: control value at -15 mmHg to -2 mmHg, warning value at 20 mmHg, and limit value at 30 mmHg. The infusion flow rate was set at 150–200 ml/min. A holmium laser (550 μm) was used to powderize the stone at 2.0–2.5 J/pulse with a frequency of 20–30 pulses/s. Analyses included cavity pressure, operative time, stone-free rates, and complications.
Results
Among the 31 patients, 29 were successfully treated with PC-UAS, with nine requiring adjunctive flexible ureteroscopy for stone migration to the kidney. Two procedures were converted to percutaneous nephrolithotomies due to failure of sheath placement. The cavity pressure of all 29 patients was well-maintained below 20 mmHg, with clear vision. The mean operative time was 48.2 ± 17.7 min. No complications, such as ureteral perforation, mucosal avulsion, or hemorrhage, occurred. Two cases of Clavien-Dindo grade I complications occurred. No major complications (Clavien-Dindo grade II–V) occurred. The mean postoperative hospitalization time was 1.7 days. The stone-free rates 1 day and 1 month after surgery were 93.1% and 96.6%, respectively. One patient with residual stones underwent extracorporeal shockwaves.
Conclusions
Rigid ureteroscopic lithotripsy with PC-UAS can effectively control the cavity pressure, shorten the operation time, and improve the efficiency of broken stones, thus reducing the complication rate.
Similar content being viewed by others


Introduction
Urolithiasis is a disease with high morbidity and recurrence rates, with an increasing annual incidence [1]. With the development of flexible ureteroscopes and holmium lasers, an increasing number of doctors are attempting to use flexible ureteroscopy to treat kidney stones > 2 cm; however, large amounts of crushed stone often need to be slowly excreted after surgery, which also leads to steinstrasse formation. Surgical management of steinstrasses has always been difficult, especially for complex steinstrasses [2]. Percutaneous nephrolithotomy (PCNL), rigid ureteroscopy, and flexible ureteroscopy have been used; however, these are associated with certain risks: PCNL is associated with a high risk of trauma and bleeding; the repeated entry and exit of a rigid ureteroscope into the ureter can easily cause ureteral injuries; and traditional flexible ureteroscopy has low efficiency in stone removal, and has a high risk of complications such as infection and ureteral stenosis [3]. Therefore, researchers have reported the use of a vacuum-assisted ureteral access sheath (UAS) to improve the safety and efficiency of complex steinstrasses [4]. However, cavity pressure monitoring and control are still not possible and require extensive operator experience [5]. Our previous research confirmed that flexible ureteroscopy assisted by a pressure-controlling UAS (PC-UAS) significantly improved safety and efficiency [6].
Therefore, in the present study, we assessed whether rigid ureteroscopic lithotripsy with PC-UAS can achieve favorable results in the treatment of complex steinstrasse syndrome compared with previously published data.
Materials and methods
Platform and PC-UAS
The system consisted of a perfusion and suction platform (Fig. 1) and a PC-UAS (Fig. 2) (PC-UAS, Inventor Technology, Jiangxi, China). The perfusion and suction platform comprised a main control unit, perfusion device, suction device, and pressure feedback device. Users can set the perfusion flow rate, control pressure value, warning pressure value, and limit value on the platform display. The main control unit of the platform adjusts the suction pressure using pressure feedback. The platform offers two modes: automatic (perfusion, suction, pressure monitoring, and pressure feedback control) and simple. It can display the actual suction and cavity pressures in real-time.

Perfusion and suction platform

PC-UAS; 1 pressure channel, 2 suctioning channel, 3 working channel, and 4, pressure measuring hole
The PC-UAS had an inner diameter of 12 Fr, an outer diameter of 14 Fr, and a length of 35 cm. Its transparent material allows for the direct observation of mucosal conditions through the sheath. The cavity pressure is measured using four pressure holes at the tip. The end of the sheath had two connection channels for suction and pressure monitoring. The suction channel can automatically suck out stones and adjust the pressure, whereas the pressure monitoring channel can monitor the cavity pressure.
Patients
We retrospectively analyzed data from consecutive patients with steinstrasse between June 2018 and October 2023 at Ganzhou People’s Hospital. The patient inclusion criteria were age 18–80 years and complex steinstrasse containing ≥ 4 stones or with an aggregate length ≥ 1.5 cm [7]. The exclusion criteria were pregnancy, urinary tract abnormalities, kidney malrotation, and positive urine cultures. Steinstrasse was confirmed by imaging, including urinary tract ultrasonography, intravenous urography, and computed tomography (CT). Stone size was calculated using CT. The study was approved by institutional ethics committee of Ganzhou People’s Hospital(TY-HKY2021-012). All patients provided written informed consent prior to surgery.
Procedural methods
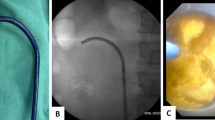
Rigid ureteroscopic lithotripsy was performed under general anesthesia with the patient in the oblique supine lithotomy position [8]. After the rigid ureteroscope was connected to the irrigation tube, the platform mode was switched to the simple irrigation mode, in which the platform operated similarly to a conventional irrigation pump with an irrigation flow of 50 ml/min. Under the guidance of a guidewire, a rigid 7/8.4 Fr ureteroscope (KARL Storz, Tuttlingen, Germany) was used for ureteroscopy. The rigid ureteroscope had an irrigation channel (2.4 Fr) and a working channel (3.4 Fr). After verifying the absence of ureteral stricture, a guidewire was inserted. The 12/14Fr PC-UAS was placed along the guidewire at the distal end of the stone. The pressure-measuring and suction channels of the sheath were connected to the perfusion suction platform (Fig. 3), and the pressure measuring channel was filled with water and zeroed. The perfusion suction platform was set to fully automatic mode, with a perfusion flow rate of 150 ml/min, control pressure of -15 to -2 mmHg, pressure warning value of 20 mmHg, and limit value of 30 mmHg. During the surgery, a 550 μm diameter fiber was used for rigid lithotripsy with a power of 2.0–2.5 J × 20–30HZ. The broken stone particles were automatically sucked out through the gap between the sheath and the scope, while particles larger than the gap but smaller than the sheath diameter were removed by withdrawing the scope. After surgery, a 4.6 Fr double J was routinely placed for 4 weeks. For patients with ureteral stenosis detected during ureteroscopy, the surgery was changed to ordinary ureteroscopy, and the stones were pushed into the kidneys for PCNL. Laparoscopy was performed for middle and lower ureteral stones that could not be pushed.

Pipe connection; 1, pressure measuring tube, 2, working channel, and 3, suctioning tube
After surgery, the patients’ vital signs and blood tests, such as routine blood count, electrolytes, and procalcitonin, were closely monitored. A kidney, ureter, and bladder radiograph (KUB) was performed on postoperative days 1 and 30 to evaluate residual stones. CT scans were performed on patients with X-ray-negative stones. Ultrasonography was performed at 3 months to assess hydronephrosis. Stone-free status was defined as the absence of stone fragments or residual stones < 2mme in CT or < 4 mm on KUB in size. Procedure duration was defined as the time from insertion of the controlled-pressure ureteral suction sheath to the end of the procedure. Surgical complications were graded according to the Clavien-Dindo classification [9].
Results
A total of 31 consecutive patients were included, six of whom had concurrent kidney stones. Among the included patients, 17 had a history of flexible ureteroscopy, seven had a history of PCNL surgery, five had a history of extracorporeal shockwave, and two had no treatment. In 29 cases, a PC-UAS was successfully inserted, of which nine cases were combined with a flexible ureteroscope, three cases had ureteral stones migrated to the kidneys, and two cases were converted to PCNL due to failure of the sheath insertion. The intraoperative pressure was controlled to within 20 mmHg in all 29 cases, with a clear field of view. There were no cases of ureteral perforation, mucosal avulsion, or hemorrhage during the operation. There were no cases of Clavien-Dindo grades II–V complications. One patient with fever and another with nausea and vomiting recovered after symptomatic treatment. The stone-free rates were 93.1% (27/29) and 96.6% (28/29) on 1 day and 1 month postoperatively, respectively ((Table 1; Fig. 4). The double J was removed successfully 1 month postoperatively, and one patient with residual stones was cleared after an extracorporeal shock wave. At the 3-month follow-up, hydronephrosis was reduced compared to the preoperative period, and there was no perinephric fluid or hematoma formation. Calculus composition analysis revealed 16 calcium oxalate calculi, two calcium phosphate calculi, three uric acid calculi, and eight mixed calculi.

Preoperative and postoperative kidney, ureter, and bladder radiograph (KUB)
Discussion
The surgical management of steinstrasse, especially complex steinstrasse, has always been a difficult problem for urologists. Surgical intervention should be initiated as early as possible in patients who have not been drained within 4 weeks of conservative medication, especially in type II or III steinstrasse [7]. Currently, flexible ureteroscopy is the preferred surgical intervention for steinstrasse stenosis, and high cavity pressure of renal often occurs during surgery [10]. When the cavity pressure exceeds 30–35 mmHg, it leads to reflux of the renal pelvic lymph nodes and veins, which causes the absorption of fluids, bacteria, and endotoxins into the bloodstream, leading to fever, systemic inflammatory response syndrome, sepsis complications, and long-term renal impairment [11, 12]. Impairment of renal function owing to elevated pressure has a cumulative effect [13]. In the case of a complex steinstrasse, the efficiency is low, the operative time tends to be long, and the incidence of infection-related complications is high. Therefore, scholars have reported the use of a suctioning UAS to improve the safety and efficiency of complex steinstrasse [4]. However, this method cannot monitor the cavity pressure of, and there is still a risk of high cavity pressure. To resolve the contradiction between irrigation flow and cavity pressure, in 2015, we developed a flexible ureteroscope with automatic pressure control using a PC-UAS, which achieved better results during clinical use [14, 15]. This system intelligently adjusts the suction pressure based on the pressure value collected by the sheath and feeds it back to the main control unit, thereby maintaining the cavity pressure at a set value. If a blockage caused by stone powder or blood clots causes a rapid pressure increase that exceeds the warning pressure value, the platform sounds an alarm. If the cavity pressure exceeds the limit value, the platform automatically stops perfusion to prevent a high cavity pressure [16].
The combined use of a rigid ureteroscope and PC-UAS for complex steinstrasse has the following advantages. First, it can monitor and automatically control pressure, which reduces fluid absorption and infection complications related to high cavity pressures [17]. Secondly, the rigid ureteroscope is easy to operate and can be used with a 550 μm fiber to significantly improve the efficiency of holmium laser lithotripsy. The 150–200 ml/min perfusion flow carried by the rigid ureteroscope reduces the thermal effect, ensures clear vision, and accelerates stone extraction [18]. The system can rapidly and automatically suction stone fragments without a stone basket, thereby reducing postoperative stone residue and stone migration. In this study, there were two cases of postoperative Clavien-Dindo grade I complications and no cases of Clavien-Dindo grade II–V complications. The complication rate was lower than that of control group using vacuum-assisted ureteral access sheath. No cases of ureteral perforation, mucosal avulsion, or hemorrhage were observed. The operation time of 48.2 ± 17.7 min was significantly shorter than that of traditional flexible ureteroscopy or rigid ureteroscopy [19]. However, the operation time was longer than that of rigid ureteroscopy using vacuum-assisted ureteral access sheath. Stone-free rates of 1 day and 30 day is higher than than that of control group. These are most likely attributable to the effective control of cavity pressure at high perfusion flow. This suggests that this technique can effectively control cavity pressure, shorten the operation time, improve lithotripsy efficiency, and reduce the complication rates.
This study has some limitations. It was a retrospective study and the sample size was small. Due to lack of a concurrent control group and the control group was obtained from the published data, we could not determine the difference in safety and efficacy compared with traditional technique. Also, because of the short follow-up time, we were unable to analyze the incidence of ureteral stricture. Finally, we did not check all CT scans during postoperative follow-up, which may lead to bias in stone free rate. In conclusion, this preliminary study confirms that ureteroscopic lithotripsy with PM-UAS is a safe and effective method for treating complex steinstrasse. To address the study limitations, prospective comparative studies are necessary in the future.
Data availability
The data is contained within the manuscript, any missing details will be available from the corresponding author on reasonable request.
Abbreviations
- CT:
-
Computed tomography
- KUB:
-
Kidney, ureter, and bladder radiograph
- PCNL:
-
Percutaneous nephrolithotomy
- PC-UAS:
-
Pressure-controlling ureteral access sheath
- UAS:
-
Ureteral access sheath
References
Zheng G, Mai Z, Xia S, et al. Prevalence of kidney stones in China: an ultrasonography based cross-sectional study. BJU Int. 2017;120(1):109–16. https://doi.org/10.1111/bju.13828.
Parmar K, Manoharan V, Kumar S, et al. Large spontaneous steinstrasse: our experience and management issues in tertiary care centre. Urologia. 2022;89(2):226–30. https://doi.org/10.1177/03915603211001174.
Feng C, Wu Z, Jiang H, et al. Ureteroscopic holmium:YAG laser lithotripsy is effective for ureteral steinstrasse post-SWL. Minim Invasive Ther Allied Technol. 2013;22(5):279–82. https://doi.org/10.3109/13645706.2012.762026.
Wang D, Xu Y, Liu Z, et al. Using vacuum-assisted ureteral access sheath in the treatment of complex steinstrasse. Urolithiasis. 2023;51(1):89. https://doi.org/10.1007/s00240-023-01462-2.
Tokas T, Skolarikos A, Herrmann TRW, et al. Pressure matters 2: intrarenal pressure ranges during upper-tract endourological procedures. World J Urol. 2019;37(1):133–42. https://doi.org/10.1007/s00345-018-2379-3.
Deng X, Song L, Xie D, et al. Suctioning flexible ureteroscopy with Automatic Control of Renal pelvic pressure. J Endourol B Videourol. 2015;195(6):e782. https://doi.org/10.1089/vid.2015.0036.
Coptcoat MJ, Webb DR, Kellet MJ, et al. The steinstrasse: a legacy of extracorporeal lithotripsy? Eur Urol. 1988;14(2):93–5. https://doi.org/10.1159/000472910.
Peng G, Song L, Xie D, et al. Suctioning flexible ureteroscopic lithotripsy in the oblique supine lithotomy position and supine lithotomy position: a comparative retrospective study. Minerva Urol Nefrol. 2018;70(6):612–6. https://doi.org/10.23736/S0393-2249.18.03144-2.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13. https://doi.org/10.1097/01.sla.0000133083.54934.ae.
Chew BH, Jung HU, Emiliani E, et al. Complication risk of endourological procedures: the role of Intrarenal pressure. Urology. 2023;181:45–7. https://doi.org/10.1016/j.urology.2023.08.011.
Breda A, Angerri O. Retrograde intrarenal surgery for kidney stones larger than 2.5 cm. Curr Opin Urol. 2014;24(2):179–83. https://doi.org/10.1097/MOU.0000000000000030.
Tokas T, Herrmann TRW, Skolarikos A, et al. Pressure matters: intrarenal pressures during normal and pathological conditions, and impact of increased values to renal physiology. World J Urol. 2019;37(1):125–31. https://doi.org/10.1007/s00345-018-2378-4.
Guohua Z, Wen Z, Xun L, et al. The influence of minimally invasive percutaneous nephrolithotomy on renal pelvic pressure in vivo. Surg Laparosc Endosc Percutan Tech. 2007;17(4):307–10. https://doi.org/10.1097/SLE.0b013e31806e61f4.
Deng X, Xie D, Huang X, et al. Suctioning flexible ureteroscopy with Automatic Control of Renal pelvic pressure versus Mini PCNL for the treatment of 2-3-cm kidney stones in patients with a solitary kidney. Urol Int. 2022;106(12):1293–7. https://doi.org/10.1159/000521373.
Deng X, Song L, Xie D, et al. A Novel Flexible Ureteroscopy with Intelligent Control of Renal pelvic pressure: an initial experience of 93 cases. J Endourol. 2016;30(10):1067–72. https://doi.org/10.1089/end.2015.0770.
Zhu X, Song L, Xie D, et al. Animal experimental study to Test Application of Intelligent pressure control device in monitoring and control of renal pelvic pressure during flexible Ureteroscopy. Urology. 2016;91:e24211–15. https://doi.org/10.1016/j.urology.2016.02.022.
Chen YJ, Liu SW, Deng XL, et al. The effect and safety assessment of monitoring ethanol concentration in exhaled breath combined with intelligent control of renal pelvic pressure on the absorption of perfusion fluid during flexible ureteroscopic lithotripsy. Int Urol Nephrol. 2023. https://doi.org/10.1007/s11255-023-03776-x.
Winship B, Wollin D, Carlos E, et al. The rise and fall of high temperatures during Ureteroscopic Holmium laser lithotripsy. J Endourol. 2019;33(10):794–9. https://doi.org/10.1089/end.2019.0084.
Rabbani SM. Treatment of steinstrasse by transureteral lithotripsy. Urol J. 2008;5(2):89–9. https://doi.org/10.22037/UJ.V5I2.52.
Acknowledgements
The authors sincerely thank all the medical workers who contributed to the treatment used in this study. We would like to thank Editage (www.editage.cn) for English language editing.
Funding
This study was funded by the following funds: Ganzhou Science and Technology Innovation Talent Plan of 2019. Ganzhou Science and Technology Bureau Science and technology plan project of 2023.
Author information
Authors and Affiliations
Contributions
DXL and SLM: design; ZYM and YL: Acquisition of data; ZQL and HX: Analysis and interpretation of data; KJ and DXL: Drafting of the manuscript and statistical analysis; ZYM and HX: Critical revision. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by institutional ethics committee of Ganzhou People’s Hospital(TY-HKY2021-012). All patients provided written informed consent prior to surgery.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yuming, Z., Lei, Y., Qiliang, Z. et al. Rigid ureteroscopic lithotripsy with a pressure-controlling ureteral access sheath for complex steinstrasse. BMC Urol 24, 112 (2024). https://doi.org/10.1186/s12894-024-01501-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12894-024-01501-z